










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores
Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282versão On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.30 no.2 São Paulo maio/ago. 2020
https://doi.org/10.7322/jhgd.v30.10381
ORIGINAL
Effects of inspiratory muscle training and breathing exercises in children with asthma: a systematic review
Tayná CastilhoI; Bianca Dana Horongozo ItaborahyI; Andreza HoepersII; Joyce Nolasco de BritoII; Ana Carolina da S. AlmeidaI; Camila Isabel Santos SchivinskiIII
IMestre em Fisioterapia pela Universidade do Estado de Santa Catarina (UDESC)
IIGraduada em Fisioterapia pela Universidade do Estado de Santa Catarina (UDESC)
IIIDoutora em Saúde da Criança e do Adolescente pela Faculdade de Ciências Médicas da UNICAMP. Professora dos cursos de graduação e pós-graduação em Fisioterapia pela UDESC
ABSTRACT
INTRODUCTION: Asthma is characterized by a narrowing and inflammation of the bronchi, with symptoms of dyspnea, fatigue and exercise limitation. Physical therapy includes inspiratory muscle training and breathing exercises, given that an increase in inspiratory muscle strength and resistance can improve the symptoms of the disease
OBJECTIVE: To describe the effects of inspiratory muscle training (IMT) and breathing exercises in children with asthma
METHODS: This is a systematic review of the literature using the Cochrane, PubMed Scopus e Web of Science databases. The following descriptors were used: asthma, inspiratory muscle training, breathing exercises and child in Portuguese, English and Spanish. Two independent evaluators screened studies that used breathing exercises and IMT in children with asthma
RESULTS: Of a total of 312 titles, eight studies were included, of which six are randomized clinical trials and two are observational studies All the studies included breathing exercises, with the objective of adjusting breathing patterns and pulmonary ventilation, reducing pulmonary hyperinflation, bronchospasm and sensation of dyspnea. However, as these exercises were not performed solely, the effects of this intervention could not be verified. Two studies performed IMT and showed an increase in maximal respiratory pressure
CONCLUSION: Breathing exercises are widely used in clinical practice as part of the management of asthma in children; however it is not possible to measure the effects in this population. IMT seems to improve inspiratory and expiratory muscle strength, but its indication in the pediatric population is not a standard procedure
Keywords: asthma, breathing exercise, child.
Authors summary
Why was this study done?
This study was designed to gather information about the effects of the IMT and breathing exercises in the pediatric population diagnosed with asthma. The importance and benefits of these interventions in adults are already known, and although they are widely used in pediatric clinical practice, the effects are not yet clear.
What did the researchers do and find?
A systematic review was carried out, as this type of study is at the top of the pyramid of scientific evidence, in order to identify the studies that used these interventions ( IMT and breathing exercise). However, only eight studies were included, which presented a variety of intervention methods and protocols, with associated application of techniques, making it difficult to generalize the results and to identify the effects of IMT respiratory exercises.
What do these findings mean?
There is a lack of evidence in scientific literature about the efects and possible benefits of IMT and breathing exercises in children with asthma. These interventions deserve further investigation, since they are quite widespread in clinical practice.
INTRODUCTION
The Global Initiative for Asthma defines asthma as a heterogeneous disease characterized by chronic inflammation of the airways, with a history of respiratory symptoms, such as wheezing, dyspnea, chest tightness, cough and variable airflow limitation1. Currently, it affects people of different age groups and is the most common chronic disease among children1,2.
According to the World Health Organization, approximately 235 million people worldwide suffer from asthma3, and in Brazil Barreto et al.4 found a high prevalence of asthma symptoms among schoolchildren. There is a progressive increase in all age groups5 and in deaths at home, with asthma being responsible for 5-10% of these cases6. Asthma is therefore considered a public health problem and a major concern to governmental authorities and healthcare professionals globally6.
The disease is triggered by multiple allergenic and non-allergenic stimuli, such as infectious, emotional and hormonal factors, food, gastroesophageal reflux, as well as hypersensitivity reactions to drugs and chemicals. Among school children, physical exercise is the most frequently cited precipitating factor7,8, and this may also be a limiting factor9 in patients with the disease, given the presence of dyspnea due to respiratory and peripheral muscle weakness10,11. As a consequence, asthma can lead to fatigue and irritability and reduce tolerance to physical exercise and patients may suffer from side effects associated with the use of asthma medication11. When exercise deprivation occurs, it is possible to note underdeveloped musculature, lack of motor coordination and exercise tolerance10,11. However, there is evidence of benefits provided by physical activities, especially combined with breathing exercises; and it is therefore indicated as a non-pharmacological treatment option as well as physiotherapy12.
The treatment of asthma includes respiratory physiotherapy, which consists of resources and techniques taught and applied to the patient to allow removal of secretion from airways, alleviate the sensation of respiratory discomfort, improve respiratory muscle strength and function, and promote cardiorespiratory conditioning13. In addition, they can prevent deformities and postural changes influenced by inadequate breathing.
Along these lines, several respiratory physiotherapy programs including inspiratory muscle training (IMT) and breathing exercises were the objects of study in patients with asthma as complementary therapies to drug treatment10. These programs are widely used in clinical practice, but do not follow a standard protocol regarding frequency, duration and application of their resources.
Thus, the present study is justified by the need to collect information from the scientific literature on the application of these physiotherapy approaches. It aims to describe the effects of 1) inspiratory muscle training and 2) breathing exercises in children with asthma through a systematic literature review.
METHODS
This is a systematic review of the literature, which was based on the recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)14.
Search Strategy
At first, the literature search started with the definition of the guiding question, using the PICO framework: What are the effects of inspiratory muscle training and breathing exercises on children with asthma? Next, the search proceeded with descriptors using the DeCS system (Health Sciences Descriptors) in Portuguese, English and Spanish. Three blocks with descriptors were selected using the following keywords: asthma, inspiratory muscle training, breathing exercises and children. Boolean operators AND and OR were also used for combination of terms.
The electronic search was conducted in February 2019, using the Cochrane, PubMed, Scopus and Web of Science databases.
Selection Criteria
For this systematic review, randomized clinical trials or observational cross-sectional studies that answered the guiding question were included. They included children and adolescents up to 15 years old diagnosed with asthma, who underwent physical therapy intervention, namely IMT or breathing exercises. The date of publication was not an inclusion criterion for the selection of the articles; and only publications in English and Portuguese were considered. The following articles were excluded: case studies and case series, review articles and studies with populations with syndromes, cognitive deficits and associated neurological deficits.
Study Selection and Methodological Evaluation
The articles were screened by two independent evaluators, who performed the search in the databases. At first, they read the titles and selected potential articles for further analysis of the abstracts. After screening the abstracts, the evaluators listed the articles that met previously established criteria to be read in full. Disagreements regarding the selection of studies were resolved through discussion between the evaluators. The methodological quality of the selected studies was also assessed using the PEDro scale15.
RESULTS
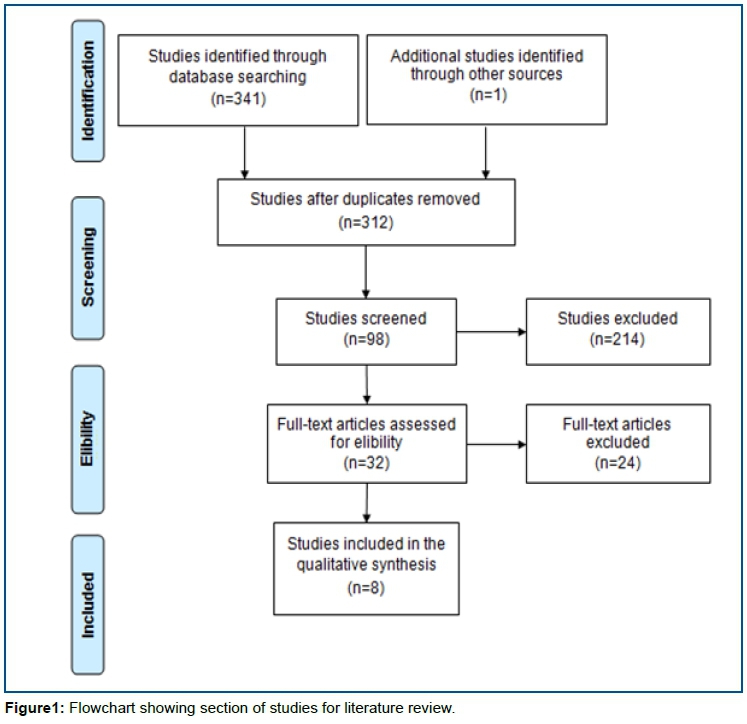
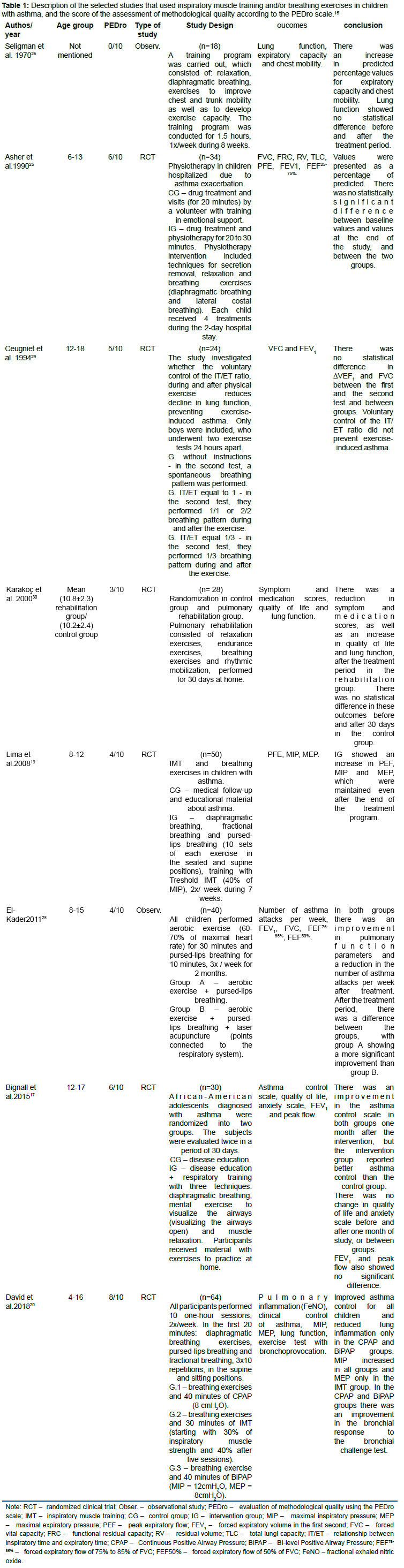
The search in the databases identified 342 articles, and after excluding the duplicates, 312 titles were read. The abstracts of 98 studies were read, of which 32 were considered eligible for full analysis of the article. Of the eligible articles, only eight were included in the present review (Figure 1), for a total sample size of 288 children with asthma. Of the total studies included, six are randomized controlled trials and two are observational studies. The methodological quality was evaluated using the PEDro scale, as shown in table 1.
There was great variability in the physical therapy intervention protocols used in patients with asthma, but all studies included breathing exercises and only two studies reported inspiratory muscle training. About five studies compared intervention groups with control groups; two studies divided the sample into groups that received intervention, without a control group; and one study applied the intervention protocol to all participants. The main outcome under investigation was lung function, specifically spirometry parameters. These data are summarized in table 1.
DISCUSSION
Inspiratory muscle training (IMT)
Pulmonary hyperinflation is a pathophysiological manifestation commonly observed in respiratory diseases that lead to airway obstruction. It causes the lowering of the diaphragmatic dome, which becomes a mechanical disadvantage, thus leading to weakness of the respiratory muscles16,17. Therefore, it is of utmost importance to maintain adequate respiratory muscle strength in individuals with asthma.
Training of respiratory muscles, more specifically of inspiratory muscles, is recommended as part of the pulmonary rehabilitation program and its use is well-established in some conditions such as chronic obstructive pulmonary disease (COPD)18. However, a standard protocol is not available for individuals with asthma, especially for the pediatric population.
In the present review, two studies included IMT in children with asthma19,20. Both performed a similar intervention protocol, in which the participants used the Threshold IMT device (© Philips Respironics) at loads of 30% to 40% of the maximal inspiratory pressure during 25 to 30 minutes. There was an increase in the values for maximal inspiratory pressure (MIP) and maximal expiratory pressure (MEP). Detailed information about the intervention protocol is shown in table 1.
Lima et al.19 also identified improvement of respiratory symptoms, activities of daily living, as well as reduction in the frequency of asthma attacks and use of medications in the intervention group. However, David et al. 20 did not observe clinical changes in the participants of the group who underwent IMT, and who were assessed with the Asthma Control Questionnaire (ACQ6).
In a systematic review on inspiratory muscle training in adults with asthma conducted by Silva et al.16 five randomized clinical trials with varied intervention protocols were included, with a load of 40% to 60% of MIP, which is greater than the load reported by Lima et al.19 and David et al.20. A meta-analysis was carried out, which was in favor of increasing MIP during IMT. Additionally, other outcomes were analyzed, such as MEP, lung function, asthma symptoms and use of medication; but the results of the studies were controversial.
Breathing exercises
The indication of breathing exercises is a strategy that is part of the management of asthma, which has been recommended as an adjunctive treatment for adults with uncontrolled asthma21 and the pediatric population. These exercises aim to maintain an adequate breathing pattern and pulmonary ventilation as well as to reduce pulmonary hyperinflation, bronchospasm and sensation of dyspnea10,22,23.
In the most severe cases of asthmatic attacks with bronchospasm and subsequent limitation of expiratory flow, the implementation of breathing exercises to favor expiration has been discussed12,24. To our knowledge, Asher et al.25 published the only study with breathing exercises in children who were hospitalized due to asthma exacerbation. However, no differences in lung function were observed before and after the intervention period and between the control and intervention groups. This outcome may be explained by the fact that the physical therapy intervention involves other physiotherapy resources, including techniques for secretion removal and muscle relaxation, in addition to breathing exercises, which were applied according to the needs of each patient.
Among different types of breathing exercises, diaphragmatic breathing was the most used technique in the studies in this review19,20,25-27. Other exercises were pursed-lips breathing19,20,28 fractional breathing,19,20 voluntary control of inspiratory and expiratory time (IT/ET)29 and lateral costal breathing25 the latter did not include its form of application.
As previously mentioned, breathing exercises still do not have a standard protocol regarding frequency, duration and specific exercise for asthma. In the present review, only the studies conducted by Lima et al.19 and David et al.20 described the frequency and duration of each exercise, and yet Karakoç et al.30 did not describe which breathing exercises were used and how they were applied.
The studies included in this review did not use breathing exercises solely: they were one element of a more complex intervention protocol, including aerobic exercises, muscle relaxation, disease education, among other interventions. Therefore, the real effects of each resource or technique of the respiratory physiotherapy could not be identified and isolated. Nonetheless, it can be noted that breathing exercises are well-established techniques for the management of asthma in children and their importance has been recognized in the scientific community.
In the case of the pediatric population, breathing exercises should be associated with games and playful activities31. Notably, McCaully24 had already described playful breathing exercises for children with asthma, especially through fun blowing games. However, none of the studies in the current review described the use of breathing exercises in a playful manner.
Although IMT and breathing exercises are widely used in patients with asthma, there is still insufficient scientific evidence on these physiotherapy approaches, especially in children. Thus, further studies are needed to identify the effects and benefits of these interventions among children with asthma.
CONCLUSION
It has been shown that IMT in children with asthma can improve the strength of inspiratory and expiratory muscle. But, the clinical improvement after treatment is still uncertain given the dearth of scientific literature about this intervention in the pediatric population.
Breathing exercises are widely used, both in clinical practice and in the scientific environment, and they are well-established techniques for the management of asthma. However, in this review, none of the studies used breathing exercises solely and a standardized protocol could not be identified; therefore, their effects on children with asthma cannot yet be measured.
REFERENCES
1.Global Initiative for Asthma. Global strategy for asthma manegement and prevention, 2018. [cited 2018 Sep 22] Available from: https://ginasthma.org/wp-content/uploads/2019/01/2018-GINA.pdf [ Links ]
2.Solé D, Melo KC, Camelo-Nunes IC, Freitas LS, Britto M, Rosário NA, et al. Changes in the prevalence of asthma and allergic diseases among Brazilian schoolchildren (13-14 years old): Comparison between ISAAC Phases One and Three. J Trop Pediatr. 2007;53(1):13-21. DOI: https://doi.org/10.1093/tropej/fml044 [ Links ]
3.World Health Organization (WHO). Asthma [online]. [cited 2018 Sep 22] Available from: http://www.who.int/news-room/fact-sheets/detail/asthma [ Links ]
4.Barreto ML, Ribeiro-Silva RC, Malta DC, Andreazzi MA, Cruz AA. Prevalence of asthma symptoms among adolescents in Brazil: national adolescent school-based health survery (PeNSE 2012). Rev Bras Epidemiol. 2014;17(Suppl 1):106-15. DOI: https://doi.org/10.1590/1809-4503201400050009 [ Links ]
5.IV Diretizes Brasileiras para o Manejo da Asma. J Bras Pneumol. 2006;32(Suppl 7):447-74. DOI: https://doi.org/10.1590/S1806-37132006001100002 [ Links ]
6.Sociedade Brasileira de Pneumologia e Tisiologia (SBPT). Diretrizes da Sociedade Brasileira de Pneumologia e Tisiologia para o Manejo da Asma. J. Bras Pneumol. 2012;38 (Suppl 1):S1-46. [ Links ]
7.Athanazio R. Airway disease: similarities and differences between asthma, COPD and bronchiectasis. Clinics (São Paulo. 2012;67(11):1335-43 DOI: http://dx.doi.org/10.6061/clinics/2012(11)19 [ Links ]
8.Mascarenhas JMO, Silva RCR, Assis AMO, Pinto EJ, Conceição JS, Barreto ML. Symptoms of asthma and associated factors in adolescents from Salvador, Bahia. Rev Bras Epidemiol. 2016;19(1):181-93. DOI: http://doi.org/10.1590/1980-5497201600010016 [ Links ]
9.Robles-Ribeiro PG, Ribeiro M, Lianza S. Relationship between peak expiratory flow rare and shoulders posture in healthy individuals and moderate to severe asthmatic patients. J Asthma. 2005;42(9):783-6. DOI: http://doi.org/10.1080/02770900500308411 [ Links ]
10. Macêdo TMF, Freitas DA, Chaves GSS, Holloway EA, Mendonça KMPP. Breathing exercises for children with asthma. Cochrane Database Syst Rev. 2016;4(4):CD011017. DOI: http://doi.org/10.1002/14651858.CD011017.pub2 [ Links ]
11.Ruas G, Urquizo WEC, Abdalla GK, Abrahão DPS, Cardoso FAG, Pinheiro PS, et al. Relationship of muscle strength with activies of daily living and quality of life in individuals with chronic obstructive pulmonary disease. Fisioter Mov. 2016;29(1):79-86. DOI: http://dx.doi.org/10.1590/0103-5150.029.001.AO08 [ Links ]
12.Bruurs ML, van der Giessen LJ, Moed H. The effectiveness of physiotherapy in patients with asthma: a systematic review of the literature. Respir Med. 2013;107(4):483-94. DOI: http://dx.doi.org/10.1016/j.rmed.2012.12.017 [ Links ]
13.Silva KCL, Andrade TCQ, Pessoa MF, Andrade AC. Posicionamento corporal alterando a força muscular respiratória e o grau de obstrução em crianças asmáticas. Fisiot Mov. 2012;25(3):533-40. DOI: http://dx.doi.org/10.1590/S0103-51502012000300009 [ Links ]
14.Galvão TF, Pansani TSA, Harrad D. Principais itens para relatar Revisões sistemáticas e Meta-análises: A recomendação PRISMA. Epidemiol Serv Saúde., 2015;24(2):335-42. DOI: https://doi.org/10.5123/S1679-49742015000200017 [ Links ]
15.Maher, CG, Sherrington C, Herbert RD, Moseley AM, Elkins M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys Ther. 2003;83(8):713-21. DOI: https://doi.org/10.1093/ptj/83.8.713 [ Links ]
16.Silva IS, Fregonezi GAF, Dias FAL, Ribeiro CTD, Guerra RO, Ferreira GMH. Inspiratory muscle training for asthma. Cochrane Database Syst Rev. 2013;(9):CD003792. DOI: https://doi.org/10.1002/14651858.CD003792.pub2 [ Links ]
17.Rossi A, Aisanov Z, Avdeev S, Di Maria G, Donner CF, Izquierdo JL, et al. Mechanisms, assessment and therapeutic implications of lung hyperinflation in COPD. Respir Med. 2015;109(7):785-802. DOI: https://doi.org/10.1016/j.rmed.2015.03.010 [ Links ]
18.Spruit MA, Singh SJ, Garvey C, ZuWallack R, Nici L, Rochester C, et al. An official American Thoracic Society/European Respiratory Society statement: key concepts and advances in pulmonary rehabilitation. Am J Respir Crit Care Med. 2013;188(8):e13-64. DOI: https://doi.org/10.1164/rccm.201309-1634ST [ Links ]
19.Lima EVNCL, Lima WL, Nobre A, Santos AM, Briito LMO, Costa MRSR. Treinamento muscular inspiratório e exercícios respiratórios em crianças asmáticas. J Bras Pneumol. 2008;34(8):552-8. DOI: https://doi.org/10.1590/S1806-37132008000800003 [ Links ]
20.David MMC, Gomes ELFD, Mello MC, Costa D. Noninvasive ventilation and respiratory physical therapy reduce exercise-induced bronchospasm and pulmonary inflammation in children with asthma: randomized clinical trial. Ther Adv Respir Dis. 2018;12:1753466618777723. DOI: https://doi.org/10.1177/1753466618777723 [ Links ]
21.Bott J, Blumenthal S, Buxton M, Ellum S, Falconer C, Garrod R, et al. Guidelines for the physiotherapy management of the adult, medical, spontaneously breathing patient. Thorax. 2009;64(Suppl 1):1-51. DOI: http://dx.doi.org/10.1136/thx.2008.110726 [ Links ]
22.Bruton A, Lewith GT. The Buteyko breathing technique for asthma: a review. Complement Ther Med. 2005;13(1):41-6. DOI: https://doi.org/10.1016/j.ctim.2005.01.003 [ Links ]
23.Burgess J, Ekanayake B, Lowe A, Dunt D, Thien F, Dhamarge SC. Systematic review of the effectiveness of breathing retraining in asthma management. Expert Rev Respir Med. 2011;5(6):789-807. DOI: https://doi.org/10.1586/ers.11.69 [ Links ]
24.McCaully HE. Breathing exercises as play for asthmatic children. Am J Matern Child Nurs. 1980;5(5):340-4. [ Links ]
25.Asher MI, Douglas C, Airy M, Andrews D, Trenholme A. Effects of chest physical therapy on lung function in children recovering from acute severe asthma. Pediatr Pulmonol. 1990;9(3):146-51. DOI: https://doi.org/10.1002/ppul.1950090305 [ Links ]
26.Seligman T, Randel HO, Stevens JJ. Conditioning program for children with asthma. Phys Ther. 1970;50(5):641-50. DOI: https://doi.org/10.1093/ptj/50.5.641 [ Links ]
27.Bignall WJR, Luberto CM, Cornette AF, Haj-Hamed M, Cotton S. Breathing retraining for African-American adolescents with asthma: a pilot study of a school-based randomized controlled trial, J Asthma. 2015;52(9):889-96. DOI: https://doi.org/10.3109/02770903.2015.1033724 [ Links ]
28.El-Kader SMA. Laser acupuncture therapy combined with aerobic exercise training and pursed lips breathing in treatment of asthmatic children: A comparison of two treatment protocols. Eur J Gen Med. 2011;8(3):200-6. DOI: https://doi.org/10.29333/ejgm/82731 [ Links ]
29.Ceugniet F, Cauchefer F, Gallego J. Do voluntary changes in inspiratory-expiratory ratio prevent exercise-induced asthma? Biofeedback Self Regul. 1994;19(2):181-8. DOI: https://doi.org/10.1007/BF01776490 [ Links ]
30.Karakoç GB, Yilmaz M, Sur S, Altintas DU, Sarpel T, Kendirli SG. The effects of daily pulmonary rehabilitation program at home on childhood asthma. Allergol Immunopathol. 2000;28(1):12-4. [ Links ]
31.Schenkel IC, Garcia JM, Berretta MSK, Silva MEM, Schivinski CIS. Therapeutic play as technique supporting to physiotherapeutic treatment in children with respiratory disorders. Psicol Teor Prat. 2013;15(1):130-44. [ Links ]
 Correspondence:
Correspondence:
cacaiss@yahoo.com.br
Manuscript received: September 2019
Manuscript accepted: January 2020
Version of record online: May 2020


{kind=link}
{kind=link}