










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Curriculum ScienTI
Curriculum ScienTIIndicadores
Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282versão On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.30 no.2 São Paulo maio/ago. 2020
https://doi.org/10.7322/jhgd.v30.10383
ORIGINAL
Self- Reported morbidity in adults: population survey in Rio Branco, Brazil, 2007 - 2008
Polyana Caroline de Lima BezerraI; Simone Perufo OpitzI; Rosalina Jorge KoifmanII; Gina Torres Rego MonteiroII; Pascoal de Torres MunizI
IUniversidade Federal do Acre, Programa de Saúde Coletiva
IIEscola Nacional de Saúde Pública, Fundação Oswaldo Cruz, Programa de Saúde Pública e Meio Ambiente
ABSTRACT
INTRODUCTION: Epidemiological data allow to know the needs of the communities and can provide subsidies for planning and actions in the health services, hence, it is necessary to investigate illness and chronic non-communicable diseases in the population of interest
OBJECTIVE: The objectives of this study are to describe and verify the association between the most prevalent self-reported morbidities in adults regarding the characteristics: socioeconomic, demographic and lifestyle
METHODS: This is a population-based survey conducted with adults (≥18 years of age), living in Rio Branco, Acre State, Brazil, during the period 2007/2008. The sample consisted of 1516 individuals, from a probabilistic sampling in two stages of a draw
RESULTS: The most prevalent self-reported morbidity was spine/back disease with a percentage of 30.8%, followed by hypertension (28.3%), malaria (28.3%) and depression (18.7%). Regarding socioeconomic and demographic aspects, the most prevalent characteristics were: female gender and low level of formal education, with statistical significance. As for life habits, the most common characteristics with statistical significance were: smoking and physical inactivity
CONCLUSION: In view of the scarcity of studies of this nature in the North region of Brazil, and especially in the State of Acre, the results regarding the most prevalent self-reported morbidities in the adult population of Rio Branco are of fundamental importance, to alert researchers and health professionals. This contributes to a better adaptation and/or implementation of public strategies for promotion, protection and health assistance
Keywords: morbidity surveys, health profile, epidemiology.
Authors summary
Why was this study done?
The motivation for carrying out the study was due to the scarcity of scientific publications to identify the most prevalent self-reported morbidities in the adult population in the Acre State, Western Brazilian Amazon, and especially in the State of Acre. Its results are of fundamental importance for researchers, managers and health professionals to know the needs of the communities and contribute to a better adaptation or implementation of public health strategies of promotion, protection and care.
What did the researchers do and find?
They conducted a population survey with adults living in Rio Branco, Acre, Brazil. The sample consisted of 1,516 individuals, through a probabilistic sampling in two stages of the draw. They found that the most prevalent self-reported morbidity was spine/back disease with a percentage of 30.8%, followed by hypertension (28.3%), malaria (28.3%) and depression (18.7%).The most relevant health determinants for the prevalence of these morbidities were the next socioeconomic and demographic aspects: female gender, older age and less education. As for life habits, the characteristics with statistical significance were: smoking and physical inactivity.
What do these findings mean?
The identification of the factors associated with the self- reported diseases in the investigated population, it highlights the possibility of implementing measures to control and prevent health risks, which take into account the social determinants of the health in the region, as well as the promotion of healthy lifestyle.
INTRODUCTION
It is observed that Brazil follows the global trend of demographic, epidemiological and nutritional transition, which has led to new demands on health services. All countries must be prepared to face the consequences of demographic change. This situation requires health promotion, disease prevention and community intervention, as well as the adoption of health management strategies and requires a strong information system to enable the management of its services1,2.
For a long period of time, in the absence of morbidity information systems and due to the predominant epidemiological profile of communicable diseases, the assessment of the health status of the populations was based on mortality data. The ability to measure health with the mortality indicator has always been precarious, but especially with the reduction of mortality rates, increased survival and increased prevalence of chronic diseases, this limitation started to require statistics on morbidity and its effects on health3-5.
It is important to consider that Brazil is undergoing an expressive demographic transition caused mainly by the fall in fertility that started in the mid 1960s and widespread in all Brazilian regions and social strata. The Brazilian average dropped from 6.3 children per woman in 1960 to 2.0 in 2005. The increase in longevity and the reduction in infant mortality also contribute to this change in the demographic pattern, in addition to determinants such as intense urbanization and changing the economic role of women. Therefore, there is an intense growth of diseases with age, since the increase in the population's survival is concurrent with the increment in the burden of morbidities3,5.
In this sense, health surveys are important, as they cover a wide spectrum of health problems, allowing the results to be correlated with the living conditions of the populations, and making it possible to know the distribution of risk factors and people's perception of their health condition6.
Information on the prevalence of disease is commonly collected through population surveys. Although the method is relatively inexpensive and efficient, as opposed to physical examinations, the validity of the information collected is often questioned7. However, in several countries the investigation of chronic diseases has shown that the information obtained on their prevalence is in good agreement when compared to medical records or clinical examinations, especially in relation to cardiovascular diseases and diabetes7,8,9,10.
Thus, the objective of this study is to estimate the prevalence of self-reported morbidities and their association with socioeconomic, demographic and lifestyle characteristics in adults living in Rio Branco, West Amazonia, Brazil.
METHODS
This is a cross-sectional population-based study, consisting of individuals aged 18 or over, living in the municipality of Rio Branco, in the State of Acre between 2007 and 2008. This study is part of the Health and Nutrition research in Children and Adults in the municipality of Rio Branco, Acre (Saúde e Nutrição em Crianças e Adultos no Município de Rio Branco, Acre), carried out by the Federal University of Acre in partnership with the Health Surveillance Secretariat of the Ministry of Health, the State Health Secretariat of Acre and the Municipal Health Secretariat of the Municipality of Rio Branco.
The sampling design used was by clusters with two stages of drawing. The primary sample unit was the census sector defined by the Brazilian Institute of Geography and Statistics (IBGE)11 2000 Demographic Census. Out of 2450 census sectors, 35 (31 urban and 4 rural) were drawn and in each of them 25 households were randomly selected, based on the map prepared by the 2006 National Household Sample Survey (PNAD).
Every one of adults living in the same household were interviewed, which meant that the sample had a structure by sex and age similar to the population of the municipality. Excluding losses and refusals, 1,514 individuals, living in 850 households participated.
The design, sampling and other methodological aspects of this study, were described in more detail by Lino et al.12 and Bezerra et al.13.
The data from the population survey were entered twice and validated using the Epi Info Windows 6.04 program, and for statistical analysis, the software Stata v.10, module svy was used, taking into account the sample design and the necessary weightings. The prevalences were estimated and the gross and adjusted prevalence ratios were estimated using Poisson regression with the respective 95% confidence intervals. To estimate the adjusted prevalence ratios, possible confounding variables were included in the model.
The questionnaire was structured based on the Household Survey of the National Cancer Institute (2002-2005) and the Risk and Protection Factors Surveillance Survey for Chronic Diseases by Telephone Survey (VIGITEL) of 2006. It consists of closed, semi-open and open questions, and constituted of modules organized by thematic sets, and contemplated the following variables of interest: demographic (sex, age group, race/color), socioeconomic (marital status, education, occupational situation, family income), aspects related to life habits (physical activity, smoking, alcohol consumption, healthy eating habits) and self-reported health ( perception and morbidities), in addition to the measurement of weight and height, allowing the calculation of body mass index (BMI).
Self-perceived health was characterized on four levels: "excellent", "good", "regular" and "bad". The "don't know" stratum was considered a loss (n=2). For the analysis of unsatisfactory health perception, a dichotomous variable was created, based on the variable "health perception", where the categories of unsatisfactory health perception (combining the regular and bad strata) and satisfactory perception (combining excellent and good) were classified.
The age group was structured in five ranges: 18 to 29; 30 to 39; 40 to 49, 50 to 59 and 60 years or older. The self-declared race/color was dichotomized in black and/or brown and not black and/or brown. The variable education was divided into four categories: zero; 1 to 7 years; 8 to 10; 11 or more years of formal instruction. Information on occupational activities was grouped into with and without occupation. The marital status was dichotomized into with and without a partner. Four categories of family income were defined: zero; <1 to <3; 3 to <5; 5 or more minimum wages, considering the minimum official wage of R$465.00.
As for the variables of life habits, smoking was represented by the dichotomous variable, being considered as smokers individuals who were so called at the time of the interview and those who had previously smoked. Alcohol consumption was classified according to the interviewee's affirmation or denial.
For the practice of physical activity, a dichotomous variable was created with reference to the classification of the World Health Organization (WHO) on the practice of physical leisure and occupational physical activity. Occupational physical activity was considered when the individual answered "yes" to at least one of the questions: "In your work, do you walk a lot?"; "In your work, do you carry weight or do other heavy activity?"; "Do you usually walk or cycle from home to work?"; "do you usually have help with cleaning?"; "Who gets the heaviest part of the cleaning?" The practice of leisure-time physical activity, on the other hand, was classified according to the interviewee's statement when answering whether they do any type of physical exercise. Therefore, the dichotomous variable "Physical activity practice" was created considering the responses of the two variables mentioned above.
To assess eating habits, a "healthy eating index" was created based on Figueiredo et al.14. In the questionnaire, the variables related to food were collected using a scale of frequency of food consumption (1 to 2 days a week; 3 to 4 days a week; 5 to 6 days a week; every day; almost never or never). These were transformed into dichotomous: usual consumption ("every day"/"1 to 6 days a week") and unusual consumption ("almost never"/"never").
The variables contained in the questionnaire were classified as markers of healthy food consumption (fish, beans, fruits, cooked vegetables, vegetable fat, raw salad) and markers of less healthy food consumption (whole milk, red meat with fat, chicken with skin, soda). These variables were dichotomized into usual consumption yes or no and coded as "0" for yes and "1" for no, in the variables markers of healthy food consumption and "0" for no and "1" for yes in the variables markers of food consumption less healthy. The total sum of these variables is equal to 10. The value "3" was defined as the cutoff point, where we consider the score from 0 to 3: healthier eating habits and from 4 to 10, less healthy. Thus, it was constructed the dichotomous variable healthy eating (yes/no).
The Body Mass Index was categorized according to the WHO score: Underweight: <18.5; Eutrophic: 18.5 to 24.9; Overweight: 25 to 29.9 and Obesity: ≥3015.
The categorical variable "number of self-reported morbidities" was constructed from the response of a list of 18 morbidities. Composes the following tracks: none; 1-3; 4-6; 7-9 and 10 or more. Therefore, in the same way, the dichotomous variable "presence of morbidity" (yes/no) was created.
This study follows the recommendations of Resolution Nº. 196/96, of the National Health Council of the Ministry of Health in force at the time of data collection, as well as the request for authorization to the participants through the Informed Consent Form. The research project was submitted and approved by the Research Ethics Committee of the Federal University of Acre, Protocol 2307.001150/2007-22.
RESULTS
The total sample consisted of 55.9% women (n = 863) and 44.1% men (n = 653). The overall average age was 38.8 years (95% CI 37.1-40.5), women with an average of 39.0; 95% CI 37.4-40, 6 and men with an average of 38.5; 95% CI 36.4- 40.7.
When analyzing the age by groups, women showed a higher percentage than men in all strata, ranging from 52.9% in individuals aged 18 to 29 years to 69.9% in those aged 40 to 49 years.
The majority of the population (84.2%) declared themselves as black or brown, only 9 people self-reported yellow race/color and none as indigenous.
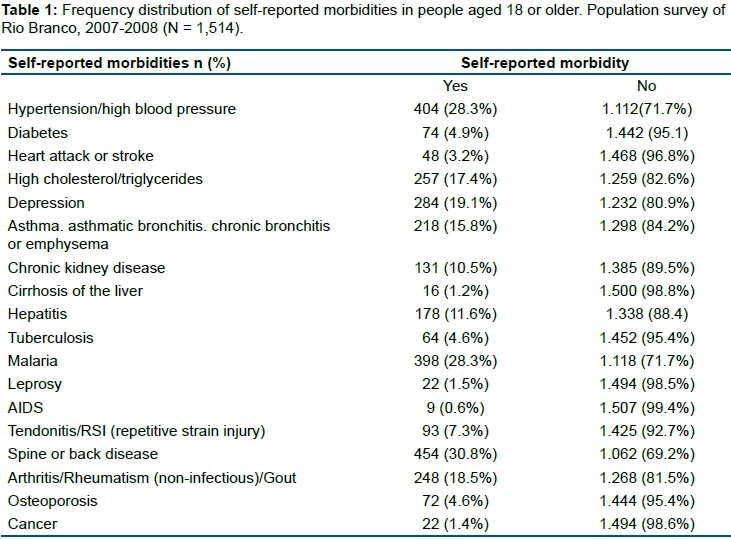
Most of the participants ( 1,149 - 76.7%) reported having at least one of the 18 morbidities surveyed. These were characterized, predominantly by being women (n = 672, 56.7%), with a mean age of 41.4 years (95% CI 39.5 - 43.3), of self-declared brown race/color (77.8%), with incomplete elementary school (61.8%), average monthly income of R $ 743.08 (95% CI 517.4 - 968.7) and having a partner (59.1%).
As for risk behaviors, this population was characterized by not having a healthy diet (78.4%), being inactive (72.3%), being overweight/obese (49.7%), not drinking alcohol (73.6%) and not being a smoker/ or never smoked (54.4%).
The most revealed morbidities were: spine/back disease (30.8%), hypertension/high blood pressure (28.3%), malaria (28.3%) and depression (19%). (Table 1).
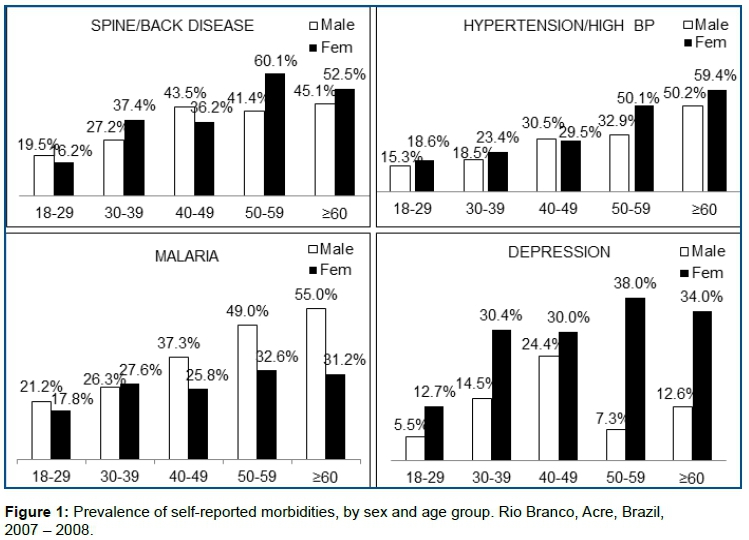
Except in cases of malaria, women and the elderly were the majority with one of these morbidities. Women were predominant in most of age groups (Figure 1).
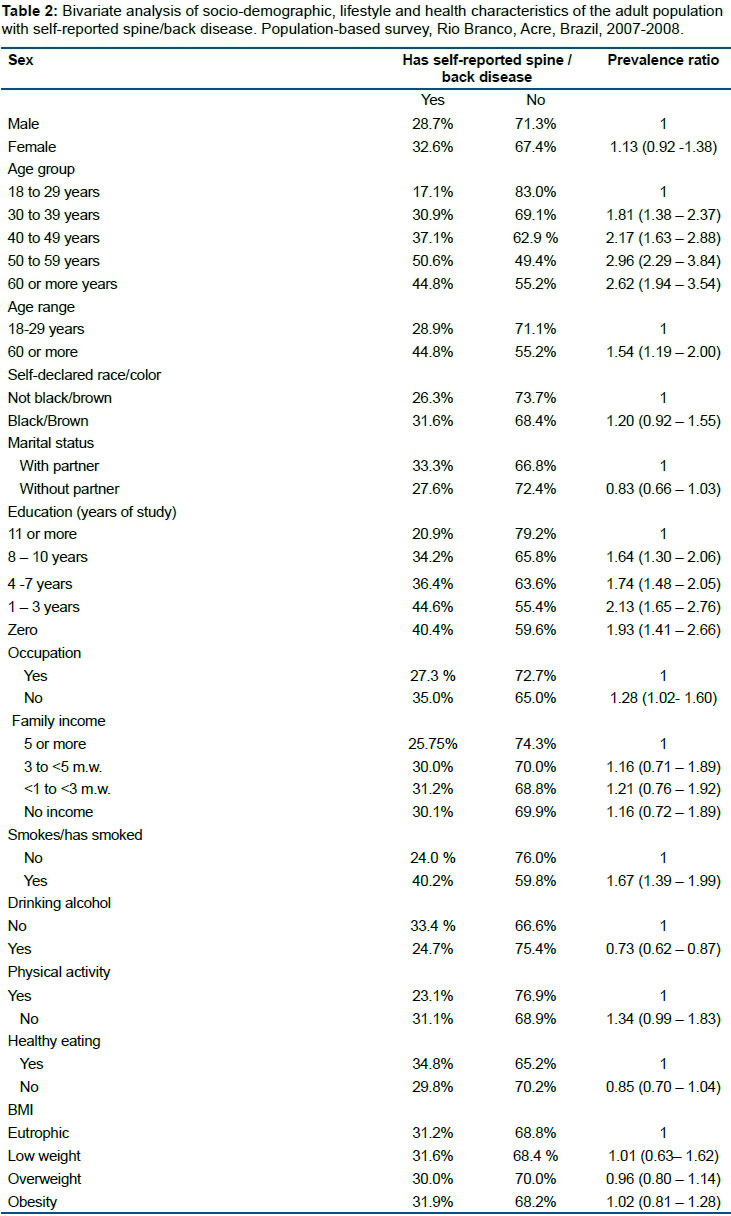
Spine/back disease was 1.54 times higher in the elderly than in the group of people aged 18 to 59 years, with statistical significance. This association increased with age (Table 2). Occupation, smoking and education also showed a positive association with the report of spine/back disease, showing a reduction in the prevalence ratio, when there is an increase in the number of years studied, even in the model adjusted for different variables (Table 3).
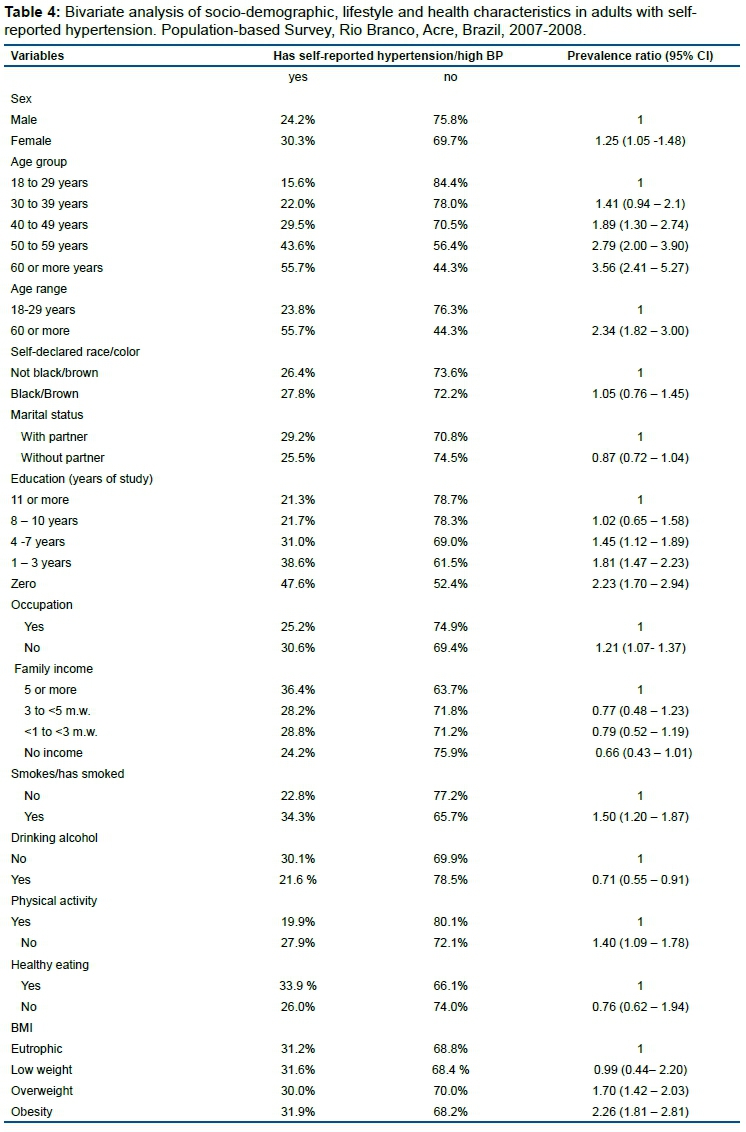
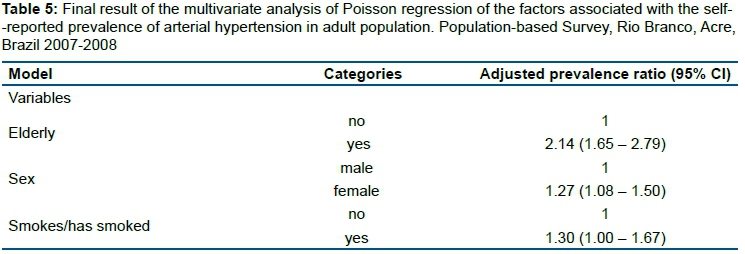
The prevalence of arterial hypertension was higher for elderly people, with obesity, low educational level, who smoke/ had smoked, inactive individuals, female and without occupation. It is noted that, although the prevalence ratio after adjustment for potentially confounding variables decreased, age remained the factor with the highest risk ratio for the report of arterial hypertension (Tables 4 and 5).
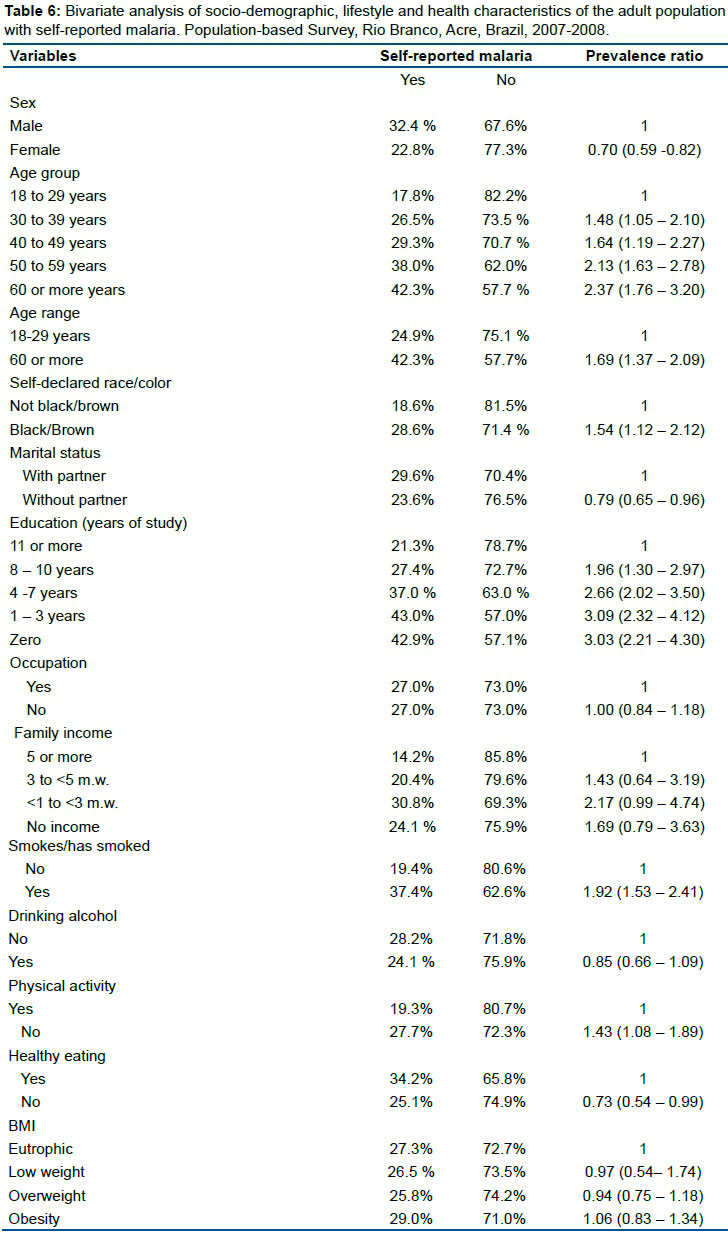
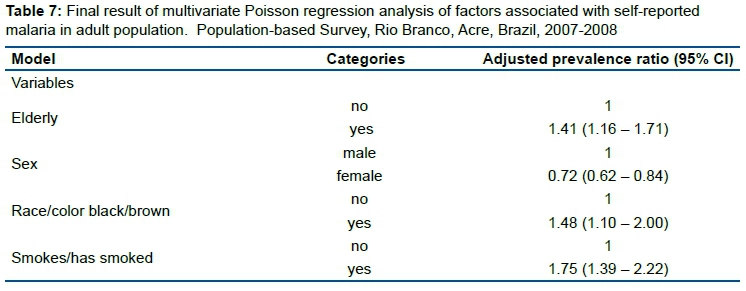
The proportion of malaria was significantly higher for people with low instruction level, older than 50 years, who smoke/had smoked and self-declared black or brown race/color. Although it has shown great risk previously, when adjusted for age, sex, race/color, black/brown color and smoking, the variable of educational level has lost its statistical significance (Tables 6 and 7).
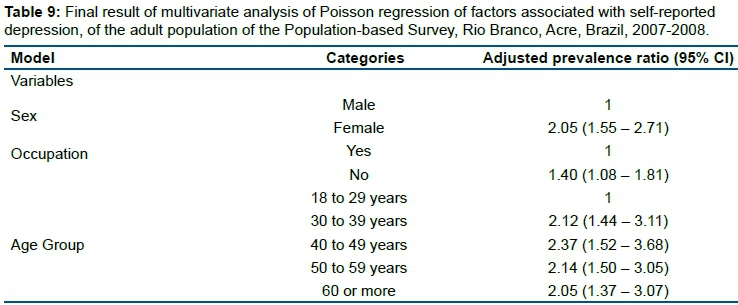
The prevalence of depression was significantly higher for older females and without work activity (Table 8). After control analysis of potentially confounding variables, the prevalence ratios related to demographic and occupation factors, remained statistically significant (Tables 8 and 9).
DISCUSSION
The 1,516 adults investigated were characterized, predominantly by women, with a median age of 38.8 years, of self-declared brown race/color, with both low educational and income level, having a partner and with work activity.
The study identified the epidemiological profile of self-reported morbidities in the population of Rio Branco, Acre, Brazil. The significant inequalities of magnitude in the prevalence of selected diseases are in agreement with other national and international population surveys, suggesting that Rio Branco follows the trend in global patterns of illness, observed in the mid-twentieth century with emphasis on the predominance of chronic diseases, a reflection of an accelerated process of industrialization-urbanization that influenced population, cultural and health dynamics16,17.
At the same time that it follows national trends with regard to the proportion of self-reported morbidities, the capital of the state of Acre reveals its own characteristics, since the third most self-reported morbidity is a parasitic disease typical of the Northern region. The socioeconomic and environmental conditions of the Amazon territory favor the proliferation of Plasmodium vectors, increasing the exposure of its inhabitants to the etiological agent of malaria, which makes the occurrence of the disease in Brazil almost exclusive to this geographical area, with a record of 99.8 % of the total number of cases17.
In population surveys, the prevalence of some chronic diseases tends to be underestimated, such as arterial hypertension and diabetes mellitus, as they require prior medical diagnosis. Self-assessed conditions, such as low back pain and depression, may have an overestimated prevalence. This is justified, if it is considered that the knowledge/diagnosis of the diseases and the perception of signs and symptoms depend on the social disparities of the populations17. However, several authors have discussed the validity of the prevalence of morbidities in population-based surveys3,17-19.
In summary, diseases that require medical/laboratory monitoring tend to be better informed. The recognition of diseases depends on the social use of the body, individual capacities, access and quality of health services. The use of the morbidity check list, face-to-face interview and self-referral technique ensure greater accuracy of the survey data. It is worth noting that, in the present study, these questions were taken into account both for data collection and analysis.
In a cross-sectional study carried out in Taiwan, between July 1992 and June 1993, to verify the concordance between the clinical status report and the prevalence of selected self-reported chronic diseases common among the elderly. An interview and clinical evaluation was applied to a sample of 228 people aged 65 and over to estimate the prevalence of heart disease, high blood pressure and diabetes20. The results showed that the self-declaration of diabetes obtained greater sensitivity (66.7%) and specificity (95.2%). The self-report of heart disease was the least sensitive with 20.5%, while reports of arterial hypertension were the least specific with 82.8%. The multivariate analysis showed that age, education and the amount of self-reported diseases influenced the accuracy of the indicated data. However, this information suggests that estimates of high blood pressure and diabetes morbidity would not necessarily be a problem. On the other hand, the prevalence of heart disease would be underestimated9.
In Brazil, a population-based study of simple random sampling (n = 970) with residents of the city of Bambuí, in the state of Minas Gerais, aged 18 years or older, which proposed to determine the validity of self-reported arterial hypertension and its determinants, revealed 72% sensitivity and 86% specificity. These results show that self-reported information is an appropriate indicator of the prevalence of arterial hypertension21.
In a study by Mendoza-Sassi et al.22, the researchers warn of the differences in reported morbidity between men and women, noting that there are differences between genders in morbidity, but with diversity in magnitude according to the type of morbidity measure used. However, in general, reports are more intensified in women than in men. This excess can be explained by variations in behavior in the search for health care (perception and/or information about health problems) between women and men.
When comparing our findings with the 2003 National Household Sample Survey (PNAD), it was observed that, in our study, the prevalence of individuals who reported having at least one morbidity (76.7%), was more than twice that what was presented by the national population (29.9%)23.
The most prevalent self-reported morbidities of our study are similar to those pointed out in the study that used data from PNAD/2003. Among the 12 diseases investigated, the most prevalent in Brazil, considering all age groups, were spine or back disease, arterial hypertension, arthritis, depression, asthma and heart disease. In the survey conducted in the state of São Paulo with individuals aged 20 years or older, the most prevalent morbidities were: migraine (21.8%), allergy (20.4%), arterial hypertension (20%), depression (17.7 %) and spine disease (17.6%)24.
Another population-based survey, carried out in Belo Horizonte, Minas Gearis, Brazil21, showed arterial hypertension as the most prevalent morbidity (18%) of the sample composed of adults, followed by spine disease, affecting 11.9%. In our findings, the most common morbidity was spine disease/back pain, with a proportion three times higher (30.8%) than that found in the population of Belo Horizonte. Our prevalence of depression (19%) was also higher than that of the capital of Minas Gerais (8.8%).
Comparing with data from the National Health Interview Survey (NHIS), it was observed that, regarding chronic conditions, the results presented in our survey are similar to those of the United States in 200815. Among adults 18 years of age or older, the two morbidities most reported were exactly the same ones found in our data: "back pain" (26%) and arterial hypertension (21%).
Socioeconomic and demographic factors were the ones most at risk for the diseases studied, when compared to factors of life habit and health.
According to Szwarcwald et al.25, the investigation of social determinants in the measures of referred morbidity deserve greater attention and needs to consider data such as those presented in our study, to guarantee the continuity of similar investigations that allow testing hypotheses concerning the influence of the effects of social disparity in the quality of life and health situation of the populations.
After adjusting different models for self-reported morbidities, it is observed that, in the studied sample, the variables with the highest association with the report of spine/back disease were, respectively, low educational level, advanced age and being female.
In Rio Branco, the greatest disparities in the occurrence of morbidities due to education were observed in the adjusted prevalence of malaria (PR 2.58; CI 1.81 - 3.69), followed by spine/back disease (PR 1.71; CI 1.14 - 2.58) following the lowest level of education (zero) when compared to the highest level (11 years or more). National data regarding education, the morbidities that had the highest prevalence ratio were heart disease (3.29), arthritis/rheumatism (3.22), diabetes (3.23), chronic renal failure (2.94) and arterial hypertension (2.90)23.
The prevalence of hypertension in Rio Branco estimated in the study "Surveillance of Risk Factors for Chronic Diseases by Telephone Survey" (VIGITEL), carried out in 2011, with 5,000 adults distributed in the capitals of the 26 Brazilian states and in the Federal District (at least 200 in each capital) was lower (22.7%) than that found in our study (28.3%). Such difference can be attributed to the population survey methodology by telephone, which limits the information to those individuals who have a landline26.
It is warned that there are at least 600 million hypertensive patients in the world. It is estimated that this disease causes the death of 7.1 million people, equivalent to 13% of the total deaths27. Hypertension has great relevance for health impairment, since, according to the health information system of the Epidemiological Surveillance of the State of Acre (unpublished data), in 2008, among the four self-reported morbidities analyzed, it had the highest number of hospital admissions in the National Health System (SUS) , being separately responsible for 198 admissions. However, it is known that arterial hypertension is a strong risk factor for other health problems, therefore it is evident the great impact that its high prevalence causes in the use in health services.
In our sample, the variable with the highest adjusted risk ratio for arterial hypertension was age (60 years or more), followed by the female. The "Household survey on risk behaviors and referred morbidity of illness and non-communicable diseases", carried out with 23,442 individuals aged 15 years and older, distributed in 15 Brazilian capitals and the Federal District between 2002 and 2003, using a sample design similar current study, revealed that the proportion of hypertensive patients in Brazil ranged between 11.22% and 14.77% in the group aged 30 to 39 years and from 42.57 % to 52.14% in individuals aged 60 and older28.
A population-based study, carried out in Campinas, São Paulo, Brazil which evaluated the prevalence of arterial hypertension in 426 elderly people, showed a percentage of 51.8% of referred hypertension, 46.4% in men and 55.9% in women29.
The high prevalence of malaria reveals the regional geographic specificity of the municipality of Rio Branco, as well as the social factors involved in this epidemiological picture. Malaria is endemic throughout the Brazilian Amazon, which encompasses the northern region and part of the states of Maranhão (Northeast) and Mato Grosso (Midwest). The high malaria endemic in the Amazon is linked to changes in extractive economic activities, which generate internal migrations and disordered rural settlements. The increase in malaria cases is mainly due to an intense and disorganized occupation of the peripheral areas of large cities17.
According to the Malaria Epidemiological Surveillance Information System (SIVEP - Malária), in 2008, 74.4% (166) of the cases notified in Rio Branco came from the rural area of the municipality30. It is common in the capital of Acre that residents of the urban area spend weekends, holidays and vacations in places known in the region as "colony", "branch" and "rubber tree", which were precisely the locations identified with the highest number of reported cases.
Compared to 2007 data, 2008 presented 28 new locations with malaria records. These areas were responsible for 40 notifications of that year, with 28 cases located in the rural area and 12 in the urban area. Such observations suggest that these cases may be connected with the advance of housing in the peripheral areas of the municipality.
Regarding depression, after adjusted analysis, demographic and occupation factors maintained statistical significance and the highest prevalence ratio. This information is similar to that found at national level in the PNAD- 200323 data, where it was found that depression is much more frequent among women. Possible causes include hormonal peculiarities, social and cultural factors. Another aspect that requires attention is the fact that women seek more medical and psychological assistance, which can increase the prevalence statistics31,32.
It is interesting to note that, in our study, individuals with work activity were more affected by depression compared to people without occupation (PR 1.40; CI 1.08 - 1.81). This fact demands attention to the need for a multidimensional look at health problems. Occupation would be directly related to depression and this fact signals the necessity for further research and strategies on the theme of occupational health.
The most prevalent self-reported morbidities were spine/back disease, hypertension, malaria and depression, respectively.
The eminent majority of morbidities have a higher proportion in the adult female population, of self-declared race/color black or brown, with a partner, without occupation and with few years of formal instruction and low level of family income.
One of the limitations of the present study is that, in the cross-sectional design, there is the possibility of reverse causality, which can occur when the apparent exposure is a consequence of the outcome. This aspect may explain the lack of association between arterial hypertension and spine/back pain with eating habits, and, with the practice of physical activity.
On the other hand, it is worth mentioning that this population-based survey is a pioneering study in Rio Branco. A differential of this study is the identification of socioeconomic factors as those that most presented a risk associated with the diseases reported, when they are compared to those related to life and health habits.
CONCLUSION
In light of the findings, measures to control and prevent health risks are necessary to implement policies that take into account social determinants of health, as well as the promotion of healthy life. The scientific community, together with the other health professionals involved, especially in the management field, must be attentive to this information, which allows greater discussions about the influence of people's precarious living conditions on the health of Rio Branco residents.
REFERENCES
1.Maia FOM, Duarte YAO, Lebrão ML. Análise dos óbitos em idosos no estudo SABE. Rev Esc Enferm USP. 2006;40(4):540-7. DOI: https://doi.org/10.1590/S0080-62342006000400013 [ Links ]
2.World Health Organization (WHO). Towards Policy for Health and Ageing. The challenge for health care system. [cited 2020 Jun 11] Available from: https://www.who.int/mip/2003/other_documents/en/E%20AAE%20Towards%20Policy%20for%20Health%20and%20Ageing.pdf?ua=1 [ Links ]
3.Barros MBA. Inquéritos domiciliares de saúde: potencialidades e desafios. Rev Bras Epidemiol. 2008;11(suppl 1):6-19. DOI: https://doi.org/10.1590/S1415-790X2008000500002 [ Links ]
4.Laurenti R, Jorge MHPM, Gotlieb SLD. A confiabilidade dos dados de mortalidade e morbidade por doenças crônicas não-transmissíveis. Ciênc Saúde Coletiva. 2004;9(4):909-20. DOI: https://doi.org/10.1590/S1413-81232004000400012 [ Links ]
5.Rede Integral de Informação para Saúde (RIPSA). Informe de Situação e Tendências: Demografia e saúde. Brasília: Organização Pan-Americana de Saúde, 2009. [ Links ]
6.Waldman EA, Novaes HMD, Albuquerque MFM, Latorre MRDO, Ribeiro MCSA, Vasconcellos M, et al. Inquéritos populacionais: aspectos metodológicos, operacionais e éticos. Rev Bras Epidemiol. 2008;11(supp 1):168-79. DOI: https://doi.org/10.1590/S1415-790X2008000500018 [ Links ]
7.Molenaar EA, Van Ameijden EJC, Grobbee DE, Numans ME. Comparison of routine care self-reported and biometrical data on hypertension and diabetes: results of the Utrecht Health Project. Eur J Public Health. 2007;17(2):199-205. DOI: https://doi.org/10.1093/eurpub/ckl113 [ Links ]
8.Molarius A, Staffan J. Self-rated health, chronic diseases, and symptoms mong middle-aged and elderly men and women. J Clin Epidemiol. 2002;55(4):364-70. DOI: https://doi.org/10.1016/S0895-4356(01)00491-7 [ Links ]
9.Wu SC, Li CY, Ke DS. The agreement between self-reporting and clinical diagnosis for selected medical conditions among elderly in Taiwan. Public Health. 2000;114(2):137-42. DOI: https://doi.org/10.1016/s0033-3506(00)00323-1 [ Links ]
10.Theme-Filha M, Szwarcwald MC, Souza Júnior PRB. Medidas de morbidade referida e inter-relações com dimensões de saúde. Rev Saúde Pública. 2008; 42(1):73-81. DOI: http://dx.doi.org/10.1590/S0034-89102008000100010 [ Links ]
11.Instituto Brasileiro de Geografia e Estatística (IBGE). Censo Demográfico de 2000.[internet]. [cited 2020 Jun 11] Available from: https://www.ibge.gov.br/estatisticas/sociais/educacao/9663-censo-demografico-2000.html?edicao=9771&t=sobre [ Links ]
12.Lino MZR, Muniz PT, Siqueira KS. Prevalência e fatores associados ao excesso de peso em adultos: inquérito populacional em Rio Branco, Acre, Brasil, 2007-2008. Cad Saúde Pública. 2011;27(4):797-810. DOI: http://dx.doi.org/10.1590/S0102-311X2011000400019 [ Links ]
13.Bezerra PCL, Opitz SP, Koifman RJ, Muniz PT. Percepção de saúde e fatores associados em adultos: inquérito populacional em Rio Branco, Acre, Brasil, 2007-2008. Cad Saúde Pública. 2011;27(12):2441-51. DOI: http://dx.doi.org/10.1590/S0102-311X2011001200015 [ Links ]
14.Figueiredo ICR, Jaime PC, Monteiro CA. Fatores associados ao consumo de frutas, legumes e verduras em adultos da cidade de São Paulo. Rev Saúde Pública. 2008;45(5):777-85. DOI: http://dx.doi.org/10.1590/S0034-89102008005000049 [ Links ]
15.World Health Organization (WHO). Obesity: preventing and managing the global epidemic. Geneva: WHO, 2000. [ Links ]
16.Pleis JR, Lucas JW, Ward BW. Summary Health Statistics for U.S. Adults: National Health Interview Survey, 2008. Vital Health Stat. 2009;10(242):1-157. [ Links ]
17.Oliveira-Ferreira J, Lacerda MVG, Brasil P, Ladislau JLB, Tauil PL, Daniel-Ribeiro CT. Malaria in Brazil: an overview. Malar J. 2010;9:115. DOI: http://dx.doi.org/10.1186/1475-2875-9-115 [ Links ]
18.Viacava F. Informações em saúde: a importância dos inquéritos populacionais. Ciênc Saúde Coletiva. 2002;7(4):607-21. DOI: https://doi.org/10.1590/S1413-81232002000400002 [ Links ]
19.Knight M, Stewart-Browm S, Fletcher L. Estimating health needs: the impact of a cheaklist of conditions and quality of life measurement on health information derived from community surveys. J Public Halth Med. 2001;23(3):179-86. DOI: https://doi.org/10.1093/pubmed/23.3.179 [ Links ]
20.Simpson CF, Boyd CM, Carlson MC, Griswold ME, Guralnik JM, et al. Agreement between self-report of disease diagnoses and medical record validation in disable older women: factors that modify agreement. J Am Geritric Soc. 2004;52(1):123-7. DOI: https://doi.org/10.1111/j.1532-5415.2004.52021.x [ Links ]
21.Lima-Costa MF, Peixoto SV, Firmo JOA. Validade da hipertensão arterial auto-referida e seus determinantes (projeto Bambuí). Rev Saúde Pública. 2004;38(5): 637-42. https://doi.org/10.1590/S0034-89102004000500004 [ Links ]
22.Mendoza-Sassi R, Béria JU. Gender differences in self-reported morbidity: evidence from a population-based study in southern Brazil. Cad Saúde Pública. 2007;23(2):341-6. DOI: https://doi.org/10.1590/S0102-311X2007000200010 [ Links ]
23.Barros MBA, César CLG, Carandina L, Torre GD. Desigualdades sociais na prevalência de doenças crônicas no Brasil, PNAD-2003. Ciênc Saúde Coletiva. 2006;11(4):911-26. DOI: https://doi.org/10.1590/S1413-81232006000400014 [ Links ]
24.Cesar CLG, Carandina L, Alves MCGP, Barros MBA, Goldbaum M. Saúde e condição de vida em São Paulo. Inquérito multicêntrico de saúde no Estado de São Paulo- ISA-SP. São Paulo: FSP/USP, 2005. [ Links ]
25.Szwarcwald CL, Damacena GN. Amostras complexas em inquéritos populacionais: planejamento e implicações na análise estatística dos dados. Rev Bras Epidemiol. 2008;11(Suppl.1):38-45. DOI: https://doi.org/10.1590/S1415-790X2008000500004 [ Links ]
26.Malta DC, Iser BPM, Claro RM, Moura L, Bernal RTI, Nascimento AF, et al. Prevalência de fatores de risco e proteção para doenças crônicas não transmissíveis em adultos: estudo transversal, Brasil, 2011. Epidemiol Serv Saúde. 2013;22(3):423-34. DOI: https://doi.org/10.5123/S1679-49742013000300007 [ Links ]
27.Lawes CMM, Hoorn SV, Rodgers A, International Society of Hypertension. Global burden of blood pressure-related disease, 2001. Lancet. 371(9623):1513-8. DOI: https://doi.org/10.1016/S0140-6736(08)60655-8 [ Links ]
28.Pereira JC, Barreto SM, Passos VMA. Perfil de risco cardiovascular e autoavaliação da saúde no Brasil: estudo de base populacional. Rev Panam Salud Pública. 2009; 25(6):491-8. [ Links ]
29.Zaitune MPA, Barros MBA, César CLG, Carandina L, Goldbaum M. Hipertensão arterial em idosos: prevalência, fatores associados e práticas de controle no Município de Campinas, São Paulo, Brasil. Cad Saúde Pública. 2006; 22(2):285-94. DOI: https://doi.org/10.1590/S0102-311X2006000200006 [ Links ]
30.30. Brasil. Ministério da Saúde. SIVEP-Malária. Sistema de informação de vigilância epidemiológica: Notificação de casos. Secretaria de Vigilância em Saúde. Secretaria Estadual de Saúde do Acre. Rio Branco: 2008. [ Links ]
31.Szwarcwald CL, Viacava F, Vasconcellos MTL, Leal MC, Azevedo LO, Queiroz RSB, et al. Pesquisa Mundial de Saúde 2003: o Brasil em números. Rio de Janeiro: RADIS/FIOCRUZ, 2004; p.14-33. [ Links ]
32.Pires CGS, Mussi FC. Crenças em saúde para o controle de hipertensão arterial. Ciênc Saúde Coletiva. 2008;13(Supl. 2):2257-67. DOI: https://doi.org/10.1590/S1413-81232008000900030 [ Links ]
 Correspondence:
Correspondence:
polyana_caroline@yahoo.com.br
Manuscript received: September 2019
Manuscript accepted: January 2020
Version of record online: May 2020


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}