










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores
Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282versão On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.31 no.2 Santo André maio/ago. 2021
https://doi.org/10.36311/jhgd.v31.12224
ORIGINAL ARTICLE
Children with autistic spectrum disorder: perception and experience of families
Patricia Poleto MonholI; Juliana Maria Bello JastrowI; Yasmin Neves SoaresI; Nathalya das Candeias Pastore CunhaI; Micael Colodette PianissolaI; Larissa Zuqui RibeiroI; Jaçamar Aldenora dos SantosII; Italla Maria Pinheiro BezerraI
IEscola Superior de Ciências da Santa Casa de Misericórdia de Vitória (EMESCAM), Vitória - Espírito Santo, Brazil
IIUniversidade Federal do Acre. Centro Universitário FMABC; Laboratório de Escrita Científica da Escola Superior de Ciências da Santa Casa de Misericórdia de Vitória (EMESCAM), Vitória - Espírito Santo, Brazil
ABSTRACT
INTRODUCTION: Autistic Spectrum Disorder (ASD) is part of neurodevelopmental disorders, which are behavioral and cognitive. These symptoms appear according to the child's development, however, most of the time, they present themselves before the age of three, and they may evolve to greater intensities or not
OBJECTIVE: To analyze the experience of families with children with Autistic Spectrum Disorder
METHODS: Exploratory study with a qualitative approach carried out at the Associação de Pais e Amigos dos Excepcionais (Association of Parents and Friends of the Exceptional/APAE). 46 families and 10 professionals participated in the study. For the analysis of the results, the technique of content analysis proposed by Bardin was used. The research project for this study was approved by the Ethics Committee for Research with Human Beings under opinion No. 3172.942 on February 27, 2019
RESULTS: It was evident that the family is an important instrument for the care of children with ASD and, for this reason, it should be seen in an integrated and not fragmented way in care, thus revealing the need to promote actions that take care of the caregiver and not just of the child itself, because as seen, every process that goes from birth to diagnosis and treatment of the child requires changes that can also bring harm to the health of the family
CONCLUSION: The experience of families of children with ASD goes through phases of acceptance and adaptation and depends on the interaction and assistance of professionals so that they can, despite life changes, perceive them as important in promoting the child's life from the motor and cognitive interaction with society
Keywords: autistic spectrum disorder, family, professionals.
Authors summary
Why was this study done?
The present study was carried out in order to analyze the experience of families with children with Autistic Spectrum Disorder.
What did the researchers do and find?
Exploratory study with a qualitative approach, carried out at the Associação de Pais e Amigos dos Excepcionais (Association of Parents and Friends of the Exceptional/APAE), in the state of Espírito Santo, Brazil. This study showed that the family is an important instrument for the care of children with ASD and, for this reason, it should be seen in an integrated and not fragmented way in care, thus revealing the need to promote actions that take care of the caregiver and not only of the child itself. As seen, every process that goes from birth to diagnosis and treatment of the child requires changes that can also harm the health of the family.
What do these findings mean?
The experience of families of children with ASD goes through phases of acceptance and adaptation, and that depends on the interaction and assistance of professionals so that they can, despite life changes, perceive them as important in promoting the child's life, from the motor and cognitive development to interact with society.
INTRODUCTION
The ASD - Autism Spectrum Disorder - is part of the neurodevelopmental disorders, which are of behavioral and cognitive nature and that arise during the child's development period, thus involving relevant difficulties in performing motor, intellectual and social functions1.
ASD is characterized by persistent deficits in the ability to initiate and sustain reciprocal social interaction and social communication and by a series of restricted, repetitive, and inflexible patterns of behavior and interests. The onset of the disorder occurs during the developmental period, typically in infancy, most of them appearing before the age of three. However, the symptoms manifest themselves according to development and may appear later. Deficits are severe to cause damage in personal, family, social, educational, occupational, or other important areas of functioning1.
The etiology of ASD is still unknown, and what has been evaluated is that around 20% of patients diagnosed with Fragile X syndrome have symptoms that meet the diagnosis of ASD. Other genetic syndromes, gene mutations, and chromosomal alterations without an identified cause were recognized. There is a characteristic related to the effects of intellectual disability, in which 10% to 30% of patients with these syndromes have comorbidity with ASD2.
The first signs of ASD often involve delays in language development without social interaction, unusual ways of communicating, and strange patterns of play. According to these changes, parents start to worry and pay attention to the limitations that are being observed. The manifestations, in general, are characterized by: Difficulties in interacting, social communication in various contexts; imagination; skills; interpretations; great deficit of learning social rules and developing them and maintaining and understanding relationships3.
A study released by the CDC (Center of Diseases Control and Prevention), an agency linked to the US government, reveals that one child in every 100 is born with ASD. The data reveal an increase in the number of autism cases worldwide. A few years ago, the estimate was one case for every 500 children. Thus, it is estimated that in Brazil, there are two million people with autism, and what makes the issue more serious is prejudice and lack of proper treatment4.
The new diagnostic criteria for ASD are divided into two domains: Repetitive behaviors, with at least three deficits in social communication, or two restricted symptoms, such as ADHD, depressive disorders, anxiety disorders, and bipolar disorder are among the most common conditions with the disorder and impairment of social communication, restricted interests. Elimination or proper identification of these concurrent neuropsychiatric conditions is important to confirm the diagnosis5.
The acceptance of the ASD diagnosis is very difficult for the family, especially for the parents, due to the lack of knowledge about the Disorder, so it is necessary to understand the importance of professionals so that they contribute to the reception and support, and that the necessary clarifications are carried out by the part of health professionals, or any professional who works in the place so that pain and anguish are reduced, and acceptance happens more easily6.
When ASD is discovered, families have the greatest difficulty in dealing with the impairment in communication, with the lack of understanding in the child's speech, which causes accentuated maternal frustration and anguish. Some factors influence the families' adaptation, such as lack of social support, unpreparedness in preschool services, little access and difficulties to health services, difficulty in identifying positive aspects, lack of family interaction, and problems related to the disease, in addition, in most cases, they dedicate themselves fully to their day with the child, so they cannot work outside the home or have any other activity, offering all the necessary care7.
Thus, it is important to work with families whose children are diagnosed with ASD to assess the impacts that the disease has on their lives. From this perspective, this work aims to analyze the experience of families with children with Autistic Spectrum Disorder.
METHODS
Study design
This is descriptive research developed from a qualitative approach.
Period and location of study
The survey was conducted in the state of Espírito Santo, Brazil, against the backdrop of the Associação de País e Amigos dos Excepcionais (Association of Country and Friends of the Exceptional/APAE) in the municipality of Cariacica from March to May 2019. It is a non-profit institution that provides assistance to quality care for people with intellectual and multiple disabilities and Autistic Spectrum Disorder. It works with prevention, diagnosis, rehabilitation, learning, and inclusion in the labor market, aiming at social inclusion. As a condition, the association requires that individuals undergo screening, in which they will be evaluated and referred to the necessary services8.
Study Population and Inclusion Criteria
Families with children with Autistic Spectrum Disorder and professionals working at APAE participated in this study. Regarding the families, the inclusion criterion was that they were part of the Associação de País e Amigos dos Excepcionais (Association of Parents and Friends and Exceptional People/APAE) and were over 18 years of age. In this association, there are around 129 families who have children with ASD. The sample was randomly made according to the criteria and the time of data collection.
47 families were approached, and there was one refusal. The other families could not participate in the study due to time compatibility, thus totaling 46 participants in the family group.
As for the study professionals, the inclusion criterion was that they had worked in the research setting for at least six months. There are 15 professionals in this association, namely: six teachers, two occupational therapists, a psychologist, two caregivers, two speech therapists, a principal, and a pedagogue. Of these, there were three refusals; two professionals scheduled more on the day could not attend, totaling 10 respondents from the group of professionals.
Data collection
Data collection with families with children with Autistic Spectrum Disorder was carried out in a waiting room and with professionals in private rooms. A semi-structured interview aimed at families and professionals was used.
For the interviews, a voice recorder was used, and then they were transcribed. Most lasted from three to 20 minutes, and a field notebook was used for notes throughout the research.
Data analysis
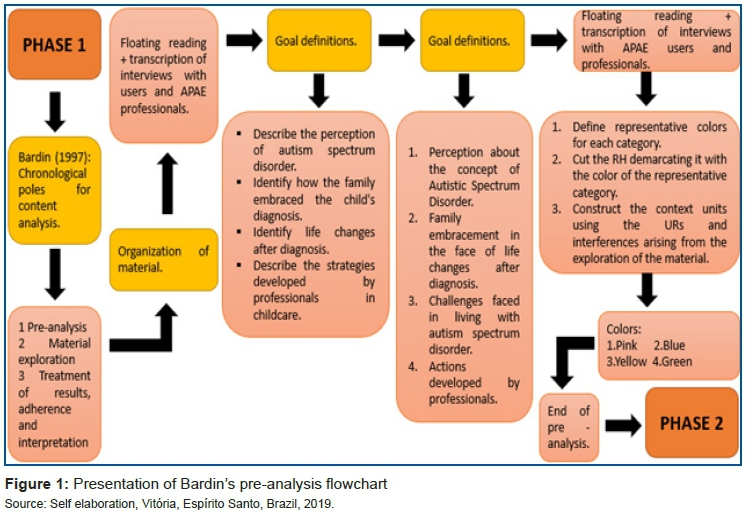
The interviews were initially organized and analyzed according to the technique of Bardin (2010)9, which is divided into three stages:
● Pre-analysis: phase of the organization itself, in which it is possible to choose the documents that will be submitted for analysis for the initial systematization of ideas, formulation of hypotheses, and objectives for the final interpretation. At this stage, the floating reading and constitution of the CORPUS were performed.
● Material exploration: characterized in coding, decomposition, and enumeration, considering the previously formulated rules.
● Treatment of results and interpretation: the raw results are treated in a way that they are meaningful and valid for further inferences.
First step of the analysis: Pre-analysis
The first step is the pre-analysis, which is related to the (re)definition of the objectives for the construction of the defined thematic categories and the rules used in the codification of the units9.
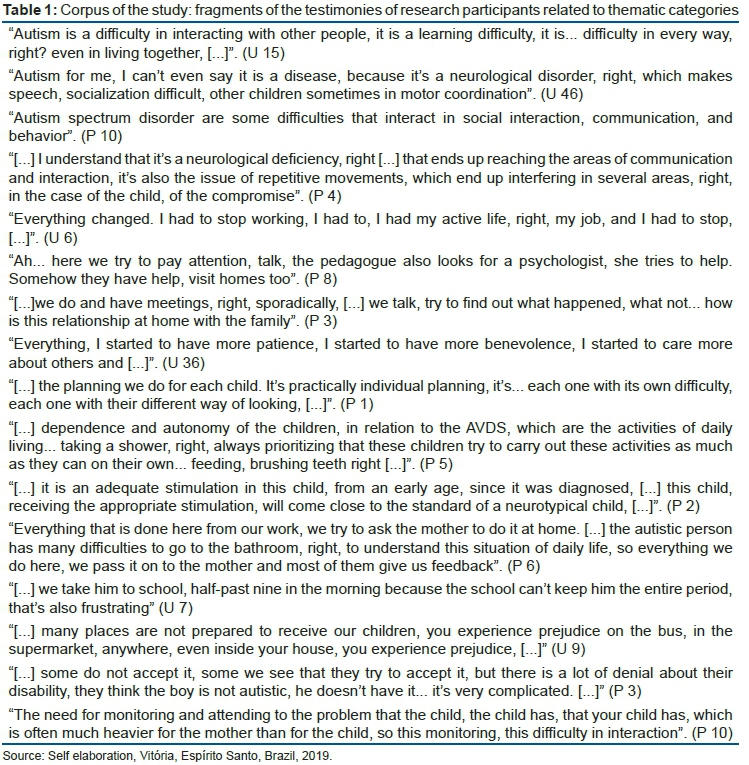
Preparation of the CORPUS of the study
Initially, the interview material was transcribed in full, with all the questions from the interview script for users and professionals, organized in a document in the Microsoft Word program, following the questions related to the initial objectives proposed in the study.
After floating reading, the material was organized, in the Microsoft Word version, according to the thematic pre-categories following the script of the interview.
Participants were identified with the code (U) for users, which would be families and; (P) for professionals, followed by a number that corresponds to the order in which the interviews were transcribed.
Thus, following the steps of Bardin9, after floating reading, with the elaboration of hypotheses and objectives, the register units were identified. After defining the objectives and thematic categories of the study, the rules for coding the Registration Units (UR) and Context Units (UC) were defined, with the colors being defined: pink, blue, yellow, and green for the pre-categories 1, 2, 3, 4, respectively.
Second phase of Content Analysis
The next step was the exploration of the content analysis material according to Bardin9. Thus, from the previously defined rules, the application of the rules was started, according to the process shown in figure 02.
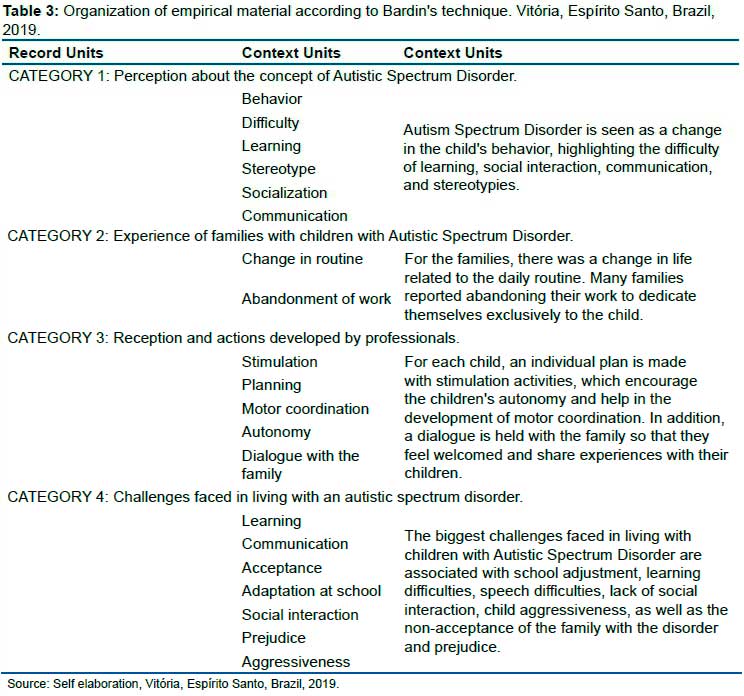
Once the pre-analysis step was implemented, the encodings were operationalized, being identified as record units and, later, as context units. These were found in the speeches through words, which were grouped according to their similarities and identified meanings.
In the coding process, one of the steps proposed by Bardin10 is an enumeration, with the choice of counting rules that make it possible to better define the URs and UCs, according to the object of the study, based on a counting that is done using criteria pre-established by the researcher. In this study, the following rule was used:
Simple Frequency (FS): corresponds to the frequency of appearance of the words or themes. The more these are repeated, the more meaning the expression or sense has, as shown in table 2. Thus, the record units were defined by counting the simple frequency, and the context units were built, which provide better interpretation for the analysis, as shown in table 3.
Third phase of content analysis: Treatment of results
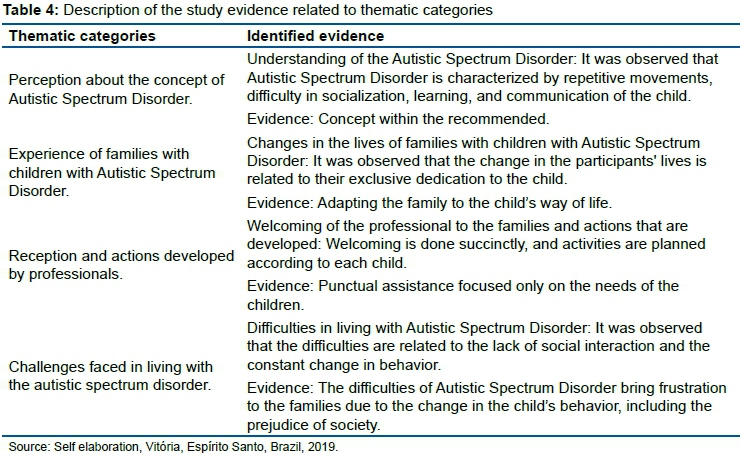
The last moment corresponding to the study method was the treatment of the results already categorized and organized in the URs and UCs, for the preparation of evidence and the construction of the framework with them by thematic category.
For each thematic category, the Evidence of the study that guided the discussions were described, which are presented in the results chapter, seeking to understand the meanings of the experience of family and professionals with Autistic Spectrum Disorder.
Ethical aspects
The project complied with the main ethical and legal requirements, obeying the formal requirements set out in Resolution 466/12 of the National Health Council/Ministry of Health10, which provides for research involving human beings, being approved by the ethics committee under the number: 3,172,942.
RESULTS
Characterization of participants
Forty-six users were interviewed, 42 females (91%) and four males (9%), aged between 25 and 55 years. Regarding the level of education, four users (9%) did not complete elementary school, and 42 (91%) completed high school. With regard to marital status, 23 are married (50%), 19 are single (41%), three divorced (7%), and one widower (2%).
Regarding professionals, 10 professionals who are part of the Autism Center of APAE were interviewed. All are female (100%), aged between 25 and 60. It is composed of five teachers, an occupational therapist, a caregiver, a principal, a pedagogue, and a psychologist. Experience related to the length of experience at APAE: between six months to two years, three professionals; three to four years, three professionals; over four years, four professionals.
Category analysis
The results of the study were identified from the evidence, with the treatment of data categorized in the URs and UCs and organized in table 4.
In Category I - Perception about the concept of Autistic Spectrum Disorder, the evidence on the understanding of the Autistic Spectrum Disorder is presented. In Category II - Experience of families with children with Autistic Spectrum Disorder, evidence of the experience of families is presented, showing the main changes in life after diagnosis. In Category III - Welcoming and actions developed by professionals, evidence of welcoming the family and educational actions that are developed at APAE and taught to the family to develop with them are presented. In Category IV - Challenges faced in living with Autistic Spectrum Disorder, evidence is presented on the main difficulties reported by families with children with Autistic Spectrum Disorder.
It was evident that the concept of ASD is known by families according to what is stated in studies and that the disorder brings changes in life, making families have an exclusive dedication to their children, abandoning some dreams and expectations. These changes lead to difficulties in relation to the lack of social interaction and the constant change in behavior, and they suffer some frustrations due to society's prejudice.
In addition, it was evident that the professionals perform care in a succinct manner and that the main focus of the professionals' actions is linked only to the children, with no more precise attention being paid to the families. The activities carried out are in accordance with each specificity of the child.
DISCUSSION
It was evident that the family's experience in the situation of Autistic Spectrum Disorder (ASD) permeates common situations that are characteristic of the disorder, which implied changes in the family's life as a whole. It is noteworthy that the perception of the disorder within a concept advocated in the literature, which is stated by repetitive movements, difficulty in socialization, learning, and communication of the child, characteristics made the family adapt to the child's way of life.
On the other hand, when seeking professional assistance, it was evidenced that the reception is done in a more punctual way, and the activities are planned according to each child. Thus there seems to be almost or no action aimed at the family as a whole, and yes, specific actions focused only on the child. In this bias, it is highlighted that every process of adaptation to the family, it goes through difficulties, bringing some frustration due to the change in the child's behavior, including the prejudice of society.
Thus, in relation to the perception of the family about the Disorder, there is a concept aimed at changing behavior, communication, and socialization. In line with what Santo and Ivanildo (2011)11 discuss, ASD is a disorder that affects the person's ability to communicate, establish relationships and respond appropriately to the environment around them.
ASD mainly compromises the child's development and is a behavioral syndrome of various etiologies. The qualitative impairments that define these conditions represent a marked deviation from the individual's level of development or mental age. In general, changes manifest themselves in the first years of life, varying in degree and intensity of manifestations12,13.
Individuals affected with ASD also present impairments in verbal and non-verbal communication and repetitive use of the word. In addition, he has delayed language comprehension and an inability to understand metaphors. It is a consensus of the authors in the field to state that individuals with this disorder have restricted behaviors and interests, adopt a permanent routine, present restriction in an area of interest may brusquely insist on something, and also may present posture abnormalities14.
According to these concepts, family interaction is extremely important for a child diagnosed with ASD, as it constitutes an individual's first relational context. For this reason, it has an important influence on the determination of human behavior and on the formation of its personality15. That is, personal relationships in the childhood context require that the child be understood as a subject inserted in a social and family environment, in constant interaction with the environment16.
In this context, when approached about how the family now lives with the child with ASD, it was noticed that despite a series of adaptations for living with the child, this family has been seeking to understand processes and experience them in order to bring about improvements to child development.
However, the analysis of the testimonies shows that women had to give up their daily activities to dedicate themselves exclusively to the child, results that confirm with Santiago (2016)17 when reporting that families have just lost their own history and started to live the history of the child as a priority. Thus, educating a child with ASD is hard work, even more so because they often have to put aside their wishes, dreams, and plans to fully dedicate themselves to the child.
In this context, the developmental impairments shown by children can have several implications for family dynamics, such as physical and mental overload that happens due to the tasks of daily life to the possibility of developing adaptability and resilience. These issues can interfere in aspects of personal, family, social, and work life18-19.
Children with ASD face deficits in relation to common tasks, which is the developmental stage, as the characteristics of a child with ASD affect physical and mental conditions, increasing the demand for care and dependence on the family. From this perspective, according to the evidence, the family is faced with the challenge of adjusting their plans and future expectations to the limitations of the condition, in addition to the need to adapt to the intense dedication and provision of care to the specific needs of the child.
According to Fávero and Santos (2005)20, job abandonment and some difficulties in pursuing a professional career in families with children who have ASD are common, as these families need to meet the child's needs and do not have time to develop something for them for an over-care account.
Furthermore, it is seen that women are the main ones responsible for directly caring for the child with ASD. For this reason, they develop high levels of stress due to the overload of demands for excessive care for their children, causing harm to their physical and psychological health. In addition, the lack of parenteral support generates a feeling of insecurity, negatively influencing women's expectations21.
Thus, it is clear in the study that there is a lack of support from family members to support the family, to assist with the burden of day-to-day care with their child, to have someone to share the moments and difficulties, to have a place to take their children for a walk, but not suffer from different looks. Thus, it would be an alternative to change this suffering, making the experience of this family lighter.
Due to the changes in life that happen with the family, it is important for a relationship between family and child to promote better development and quality of life; it is necessary to have the support of health professionals or related areas so that they can best serve the child's needs and your own needs.
In this scenario, the TEA entails changes that point out that the entire daily life of families is focused on the child. This dedication brings physical and emotional overload, both with the general care of the child, as well as with all other tasks of the day, such as taking care of the house, attention to other members of the family, and even your job. All schedules and routines are modified in order to provide the necessary support and care for the TEA. For the child, the difficulties in social relationships can cause problems that reflect on the family's daily life, as they start to live according to their demands and permanent dependence22.
The results are in line with the study by Zanatta et al. (2014)23, in which it was seen that families suffer from being totally attached to their children and that they need attention, to be listened to and comforted, that the look should not only be for the child with ASD. For this reason, it is necessary to have support and mediation during this trajectory, from the closest people and especially from professional assistance to help this family in the overload.
In this sense, it was evident in this study that the role of professionals who care for children in a specialized association such as APAE is important in facing this new family life, and these professionals are responsible for the care that generates improvement in the motor, cognitive and social development of that child. However, at the same time that these welcoming actions aimed at meeting these needs were perceived, few strategies were seen that could meet the family's needs, as well as people who, from then on, begin to undergo important life changes.
Thus, the inter-family comprehensiveness of health actions is a determining factor for the quality of interpersonal relationships because, in addition to considering only the individual's disease, comprehensive care involves looking at the person in order to understand in a broader way the life context. Thus, the concern goes beyond looking at the biological, assuming the commitment to meet their multiple needs16.
When parents plan to have a child, or even when an unexpected pregnancy happens, the family believes that the child will come into the world in a healthy and perfect way. In the mind of no family, it will be born with any limitation. When this long-awaited child starts to have aggressive behaviors, difficulty in socializing, and takes time to speak and repeats movements, facing this new reality causes frustration to the dreams that were idealized by the family, the scene changes, and the reality is unknown, a new family organization is needed23.
According to the analysis of the interviews, professionals and family reported that actions are carried out with activities related to Activities of Daily Living (ADL), which corroborates Araújo et al. (2018)24 when they state that social interaction with children, professionals, or the family itself, can be stimulated for them to develop and this involvement can happen through activities and games developed together. Such activities are able to develop in the child possibilities of behavior changes related to ADL in which children are encouraged to eat and drink liquids, use the bathroom, do hand hygiene, put on and tie shoes, put on their clothing independently, thus stimulating the autonomy of this child.
In the results obtained, the professionals reported that they use as a methodology in APAE the Treatment in Education for Autism and Children with Communication Related Disabilities (TEACCH), which according to Mello (2007)25 is one of the most used teaching methods in Brazil to assist children with TEA. This method helps in the following aspects: motor coordination skills, classification, object perception, the introduction of letters and numbers and symbols, memorization exercises, reading, writing, and performing mathematical operations, enhancing the characteristics of the methodological principles aimed at learning the student. It is an approach that responds to the needs of members, using the best approaches and methods.
From this perspective, the reception of professionals who are involved with this family is relevant. However, welcoming does not presume a specific professional, and anyone can perform; it is a way of dialoguing, listening, and responding that welcome and help, listening to their requests and assuming the service a posture capable of welcoming and providing care, guiding the best to be done with a relationship of trust26.
Given the difficulties faced by these individuals and consequently the limitations that the disease brings to their families, the monitoring of the APAE professional, as well as the common activities of daily life, motor coordination are important stimulations. In addition, it is necessary to be comprehensive in the care, not just looking at the child with ASD, but to do it in a way that the family, the mother, is included, since they are the ones who play the biggest role. It is through the construction of a bond of trust with these professionals that care becomes more effective and light27.
Developing good professional-patient relationships reduces anxiety and improves understanding. Using the strengths of the ASD patient instead of scoring their weaknesses can increase the professional's control of the situation. Many have poor motor coordination and may not be able to perform basic tasks performed by professionals, even when they give their best28.
Finally, it was observed that there are challenges that need to be faced by the family and even by professionals who directly or indirectly interfere with the child's life, difficulties that are related to the lack of social interaction and the constant change in behavior, implying even in society's prejudice towards children.
It appears that the difficulties in dealing with situations that bring concerns are constituted by some elements. Among them are the various forms of prejudice that this child will suffer at school, on the street, and even among members of the family. The process of acceptance in many cases is gradually constituted, from the denial of the diagnosis to the frustration of having a child with limitations, until reaching the acceptance of this disorder29.
In this context, prejudice is defined as a set of negative beliefs, attitudes, and behaviors attributed to members of certain social groups30. When talking about ASD, society's view is a factor that influences the family, dealing with people's discomfort, discrimination, looks in a different way is pointed out as an offense to the child and felt by the mother as if it were her. It is precise because of this circumstance that the fragility of the child in society is perceived, and thus the families also feel fragile31.
In view of the aspects addressed by the child with ASD, it is understood that there are difficulties and challenges in the areas of social interaction, communication, and behavior that are closely articulated in human development. In this model, the school is seen as a space that favors this child to develop these areas due to the fact of being with other children and the importance of the professional who favors the children's abilities32.
In this regard, it is important to highlight the provisions of articles 1 and 27 of Law No. 13,146 of July 6, 2015, the Lei Brasileira de Inclusão da Pessoa com Deficiência (Brazilian Law for the Inclusion of People with Disabilities)33, on the subject:
Art. 1º. The Brazilian Law of Inclusion of Persons with Disabilities (Statute of Persons with Disabilities) is instituted, aimed at ensuring and promoting, under identical conditions, the exercise of fundamental rights and freedoms by persons with disabilities, aiming at their social inclusion and citizenship.
Art. 27. Education is a right of people with disabilities, guaranteed inclusive educational system at all levels and lifelong learning, in order to achieve the maximum possible development of their physical, sensory, intellectual, and social talents and abilities, according to their characteristics, interests, and learning needs. Single paragraph. It is the duty of the State, the family, the school community, and society to ensure quality education to people with disabilities, keeping them safe from all forms of violence, negligence, and discrimination.
Based on the foregoing, the existence of the aforementioned law aims at the effectiveness of inclusive education, as can be seen from the literalness of art. 28, item XI:
Art. 28. Public authorities are responsible for ensuring, creating, developing, implementing, encouraging, monitoring, and evaluating: (...) XI. "Training and providing teachers for specialized educational services, translators and interpreters of Libras, interpreting guides and support professionals".
These professionals act as regulatory agents ensuring access to education for people with ASD and other disabilities. However, it does not ensure that educators know how to help them in their educational process. However, this phenomenon is faced with the precarious reality of the educator in the way of conducting the educational process so that the right to have an education is satisfactorily fulfilled34. In other words, the educator needs to be prepared to help the child with a disability. Its main objective is to teach them and encourage the formation of knowledge, and it is necessary to give them confidence so that this child feels welcomed by this professional.
Thus, it is clear that the family of children with ASD, as a result of the change in life after the child's birth and diagnosis, goes through difficulties such as prejudice, aggressiveness, lack of adaptation in schools and, therefore, it generates frustration on the part of the family as for the child. However, it was clear that despite these challenges, after the adaptation and acceptance of the family, the importance of the family for this child is emphasized, as well as the relevance of the professional in stimulating and welcoming both.
It is noteworthy that the family is an important instrument for the care of children with ASD and, for this reason, it should be seen in an integrated and not fragmented way in care, thus revealing the need to promote actions that take care of the caregiver and not only of the child itself, because, as seen, every process that goes from birth to diagnosis and treatment of the child requires changes that can also bring harm to the family's health.
CONCLUSION
The experience of the family of children with Autistic Spectrum Disorder goes through phases of acceptance and adaptation and depends on the interaction and assistance of professionals so that they can, despite life changes, perceive them as important in promoting the child's life from motor development and the interaction with social cognitive.
REFERENCES
1.Organização Mundial de Saúde; CID-11 Classificação Internacional de Doenças [Internet]. [place unknown]; 2018 [cited 2019 Jun 11]. Available from: https://icd.who.int/browse11/l-m/en#/http://id.who.int/icd/entity/120443468. [ Links ]
2.Zanolla TA, Fock RA, Perrone E, Garcia AC, Perez ABA, Brunoni D. Causas genéticas, epigênicas e, ambientais do transtorno do espectro autista. Cadernos de Pós-graduação em Distúrbios do Desenvolvimento. 2015;15(2). Available from: https://www.mackenzie.br/fileadmin/ARQUIVOS/Public/6-pos-graduacao/upm-higienopolis/mestrado-doutorado/disturbios_desenvolvimento/2015/cadernos/2/CAUSAS_GENE__TICAS__EPIGENE__TICAS_E_AMBIENTAIS_DO_TRANSTORNO_DO_ESPECTRO_AUTISTA_.pdf. [ Links ]
3.Brasil. Manual diagnóstico e estatístico de transtornos mentais. Brasília; 2015. [ Links ]
4.Número de pessoas com autismo aumenta em todo o Brasil. Apae Brasil [Internet]. Brasília; 2017. Disponível em: https://apaebrasil.org.br/noticia/numero-de-pessoas-com-autismo-aumenta-em-todo-o-brasil. [ Links ]
5.Sharma SR, Gonda X, Tarazi FI. Autism spectrum disorder classification, diagnosis and therapy. Pharmacology & Therapeutics. 2018; 185: 1-170. DOI: 10.1016 / j.pharmthera.2018.05.007 [ Links ]
6.Pinto RNM, Torquato IMB, Collet N, Reichert APDS, Souza Neto VLD, Saraiva AM. Autismo infantil: impacto do diagnóstico e repercussões nas relações familiares. Revista Gaúcha de Enfermagem. 2016;37(3). DOI: http://dx.doi.org/10.1590/1983-1447.2016.03.61572 [ Links ]
7.Meimes MA, Saldanha HC, Bosa CA. Adaptação materna ao transtorno do espectro autismo: relações entre crenças, sentimentos e fatores psicossociais. Psico, Porto Alegre. 2015; 46(4). https://dx.doi.org/10.15448/1980-8623.2015.4.18480 [ Links ]
8.Brasil. Federação nacional das APAES [Internet]. Brasília, DF; 2017 [cited 2019 Jun 11]. Available from: http://www.ineedce.com/coursereview.aspx?url=2037%2FPDF%2F1103cei_aut.pdf&scid=14486. [ Links ]
9.Bardin L. Análise de conteúdo. 70. Ed. Lisboa; 1977. [ Links ]
10.Conselho Nacional de Saúde. Resolução nº 466/12 [Internet]. Brasília, DF; 2012 [cited 2019 Jun 11]. Available from: http://conselho.saude.gov.br/resolucoes/2012/reso466.pdf. [ Links ]
11.Santos J, Ivanildo F. Educação Especial: Inclusão escolar da criança autista. São Paulo: Editora All Print; 2011. [ Links ]
12.Siluk ACP. Atendimento Educacional Especializado: contribuições para a prática pedagógica. Santa Maria; 2012. 287 p. [ Links ]
13.Dornelles C. Manual Diagnóstico e Estatístico de Transtornos Mentais. 4. ed. Porto Alegre; 2002. [ Links ]
14.Garcia PM, Mosquera CFF. Causas Neurológicas Do Autismo. O Mosaico - Revista de Pesquisa em Artes da Faculdade de Artes do Paraná. 2011; 5. Available from: http://periodicos.unespar.edu.br/index.php/mosaico/article/viewFile/19/pdf. [ Links ]
15.Andrade AA. Teodoro MLM. Família e Autismo: Uma Revisão da Literatura. Contextos Clínicos. 2012; 5 (2):133-142. DOI: 10.4013/ctc.2012.52.07 [ Links ]
16.Furtado MCDC, Silva LCT, Mello DF, Lima RAG, Petri MD, Rosário MM. A integralidade da assistência à criança na percepção do aluno de graduação em enfermagem. Revista Brasileira de Enfermagem. 2012;65(1): 56-64. DOI: https://doi.org/10.1590/S0034-71672012000100008 [ Links ]
17.Maia Filho ALM, Amanda LANMN, Nogueira L, Silva KCO, Santiago RF. A importância da família no cuidado da criança autista/the importance of the family in the care of autist children. Saúde em Foco. 2016;3(1): 66-83. Available from: http://www4.unifsa.com.br/revista/index.php/saudeemfoco/article/view/719. [ Links ]
18.Martins T, Ribeiro JP, Garret C. Estudo de validação do Questionário de avaliação da sobrecarga para cuidadores informais. Psicologia, Saúde & Doenças. 2003; 4(1): 131-148. Available from: https://sigarra.up.pt/fpceup/pt/pub_geral.pub_view?pi_pub_base_id=83237. [ Links ]
19.Ghanizadeh A, Alishahi MJ, Ashkani H. Helping families for caring children with autistic spectrum disorders. Arch Iran Med. 2009;12(5): 478-482. Available from: https://pubmed.ncbi.nlm.nih.gov/19722770/. [ Links ]
20.Fávero M, Santos M. Autismo infantil e estresse familiar: uma revisão sistemática da literatura. Psicologia: reflexão e crítica. 2005: 18(3): 358-369. DOI: https://doi.org/10.1590/S0102-79722005000300010 [ Links ]
21.Schmidt C, Bosa C. Estresse e auto-eficácia em mães de pessoas com autismo. Arq. bras. Psicol..2007; 59(2): 179-191. Available from: http://pepsic.bvsalud.org/scielo.php?script=sci_arttext&pid=S1809-52672007000200008. [ Links ]
22.Minatel MM,Matsukura TS. Famílias de crianças e adolescentes com autismo: cotidiano e realidade de cuidados em diferentes etapas do desenvolvimento. Revista de Terapia Ocupacional da Universidade de São Paulo. 2014; 25(2): 126-134. DOI: https://doi.org/10.11606/issn.2238-6149.v25i2p126-134 [ Links ]
23.Zanatta EA, Menegazzo, E, Guimarães AN, Ferraz L, da Motta, MDGC. Cotidiano de famílias que convivem com o autismo infantil. Revista Baiana de Enfermagem. 2014;28(3). DOI: http://dx.doi.org/10.18471/rbe.v28i3.10451 [ Links ]
24.Silva SED, Santos AL, Sousa YM, Cunha NMF, Costa JL, Araújo JS. A família, o cuidar e o desenvolvimento da criança autista. Journal of Health & Biological Science.2018;6(3): 334-341. DOI: http://dx.doi.org/10.12662/2317-3076jhbs.v6i2.1782.p334-341.2018 [ Links ]
25.Mello AMSR. Autismo: guia prático. 5. ed. Brasília; 2007. [ Links ]
26.Núcleo Técnico da Política Nacional de Humanização. Acolhimento nas práticas de produção de saúde [Internet]. Brasília, DF; 2009 [cited 2019 Jun 11]. Available from: https://bvsms.saude.gov.br/bvs/publicacoes/acolhimento_praticas_producao_saude.pdf [ Links ]
27.Campos CC, Haddad AS. Transtornos de comportamento e tratamento odontológico. In: Haddad AS. Odontologia para pacientes com necessidades especiais. 2017. p. 229-239. [ Links ]
28.Palma AM, Raposa KA. Building Bridges: Dental Care for Patients with Autism [Internet]. [place unknown]; 2011 [cited 2019 Jun 11]. Available from: http://www.ineedce.com/coursereview.aspx?url=2037%2FPDF%2F1103cei_aut.pdf&scid=14486. [ Links ]
29.Monte LCP, Pinto AA. Família e autismo: Psicodinâmica Familiar diante do Transtorno e Desenvolvimento Global na Infância. Estação Científica, Juiz de Fora. 2015; 14:1-16. Available from: https://portal.estacio.br/docs%5Crevista_estacao_cientifica/02-14.pdf [ Links ]
30.Silva SG. Preconceito no Brasil Contemporâneo. Psicologia Ciência e Profissão.2003; 23(2): 2-5. DOI: https://doi.org/10.1590/S1414-98932003000200002 [ Links ]
31.Cezar PK, Smeha LN. Repercussões do autismo no subsistema fraterno na perspectiva de irmãos adultos. Estud psicol. 2016; 33(1):51-60. DOI: https://doi.org/10.1590/1982-02752016000100006 [ Links ]
32.Lemos ELMD, Salomão NMR, Ramos NCS. A. Inclusão de crianças autistas: um estudo sobre interações sociais no contexto escolar. Revista Brasileira de Educação Especial. 2014; 20(1). DOI: https://doi.org/10.1590/S1413-65382014000100009 [ Links ]
33.Brasil. Lei nº 13.146 de 06 de julho de 2015. Lei Brasileira de Inclusão da Pessoa com Deficiência (Estatuto da Pessoa com Deficiência). Diário Oficial da União. 6 de jul de 2015. [ Links ]
34.Selau B.;Hammes,LJ. Educação inclusiva e educação para a paz: relações possíveis. São Luiz: EDUFMA; 2009. [ Links ]
 Correspondence:
Correspondence:
Jaçamar Aldenora dos Santos
jacamar.santos@ufac.br
Manuscript received: April 2021
Manuscript accepted: May 2021
Version of record online: July 2021


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}