










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores
Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282versão On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.31 no.2 Santo André maio/ago. 2021
https://doi.org/10.36311/jhgd.v31.10185
ORIGINAL ARTICLE
Effects of a multi-professional approach on anthropometric variables and food profile of overweight or obese adolescents
Fabiano Mendes de OliveiraI, II, III; Déborah Cristina de Souza MarquesI, II, III; Andressa Alves CoelhoI, III; Marilene Ghiraldi de Souza MarquesI, III; Cynthia Gobbi Alves AraújoI, III; Braulio Henrique Magnani BrancoI, II, III
IUniversidade Cesumar (Unicesumar), Maringá, Paraná, Brasil;
IIPrograma de Pós-Graduação em Promoção da Saúde da Unicesumar, Maringá, Paraná, Brasil;
IIIGrupo de Pesquisa em Educação Física, Fisioterapia, Esporte, Nutrição e Desempenho (GEFFEND/Unicesumar), Maringá, Paraná, Brasil
ABSTRACT
INTRODUCTION: Investigating the of overweight or obese adolescents' nutritional quality is substantial to guide healthy eating strategies
OBJECTIVE: To assess the effects of a multi-professional approach on anthropometric parameters, body composition, and the level of food processing in adolescents
METHODS: Twelve overweight/obese male adolescents between 13-17 years old participated in a series of 12-week multi-professional interventions led by physical education, nutrition, and psychology professionals. The participants were assessed before the intervention as well as at 6 and 12 weeks. Anthropometric assessments were performed, including body weight, stature, and body mass index; body composition, with fat mass (FM), body fat (%BF), skeletal muscle mass, and resting metabolic rate (RMR), and by filling in a three-day food record, to assess the ingested foods by its level of processing: fresh, minimally processed, processed, and ultra-processed
RESULTS: No differences were observed in anthropometric parameters performed at different stages (p>0.05). Reductions in FM and %BF and increases in SMM and RMR (p<0.05) were identified after, the 12-week intervention. There was an increase in the consumption of natural foods/g and increased the caloric consumption of processed foods/kcal after 12-week of intervention (p<0.05
CONCLUSION: The model resulted in a decrease in fat mass and body fat percentage, an in skeletal muscle mass, resting metabolic rate, natural foods/g, and processed foods/kcal
Keywords: adolescent health, food consumption, health promotion, physical activity.
Authors summary
Why was this study done?
This study was conducted to verify the responses of a multi-professional intervention on anthropometric, body composition, and food profile in adolescents with overweight or obesity. The replies between eventual changes in food profile may help health professionals to conduct nutritional guidance to promote health and quality of life in adolescents with overweight or obesity
What did the researchers do and find?
It was observed an improvement in skeletal muscle mass, resting metabolic rate, as well as the consumption of fresh foods/g and processed food/kcal after the intervention period. Besides, it was verified a reduction of fat mass and body fat percentage after 12-week of intervention.
What do these findings mean?
These findings may direct strategies to combat obesity in adolescents and promote positive food consumption changes after nutritional counseling, physical activity, and psychological counseling.
INTRODUCTION
The prevalence of overweight and obese people has increased dramatically, with the latter being considered a worldwide pandemic1. The increase in this chronic non-communicable disease (NCD) is linked to declining levels of physical activity (PA) and increased consumption of processed foods2. Dietary transition refers to consuming foods with high energy density and low nutritional value, which are contributing causes of overweight, obesity, and NCDs3. As a result, the evidence presented above shows a relationship between lower levels of PA and elevated consumption of industrialized foods (processed and ultra-processed foods) that are associated to overweight and especially obesity.
In this context, overweight is conceptualized as the accumulation of above-normal amounts of fat, resulting in damage to health4. According to the Family Budget Survey conducted by the Brazilian Institute of Geography and Statistics (IBGE)5, one in three adolescents is overweight. In 2015, the IBGE conducted a National School Health Survey, which indicated an increase in the consumption of ultra-processed foods, such as soft drinks, sausages, and cookies, in addition to a reduction in the consumption of fresh and minimally processed foods, such as vegetables, fruits, grains, and milk6. In this sense, the prevalence of overweight and obesity in teenagers is alarming, and health promotion strategies (improving PA, nutritional, and psychological counseling) are indispensable to promote healthy longevity.
The increase in the consumption of processed foods in school children's dietary profile is directly related to the development of obesity, metabolic syndrome, and nutritional deficiency, which are very common in children and adolescents7. The reversal of these bad habits requires a multi-disciplinary approach and motivational interventions8. In response to this epidemiological problem, physical activity associated with dietary re-education has been used to treat overweight/obesity cases. It improves body composition components, namely body fat reduction, and improves Skeletal Muscle Mass (SMM) during multi-professional interventions (12-weeks)8,9.
However, Branco et al.8,9 pointed out that 12-week interdisciplinary interventions in adolescents did not promote changes in total caloric intake after the nutritional education period. Nevertheless, in the two aforementioned articles, the authors performed only a quantitative analysis. Qualitative research was not conducted to verify possible changes in the level of food processing (fresh, minimally processed, processed, and ultra-processed food). A qualitative analysis could provide in-depth information about the changes in health education and awareness among adolescents, which may help nutritionists and health professionals to develop clinical conduct.
In this sense, nutritional counseling is an essential tool for health literacy8,9. To aid the study of nutrition, Monteiro et al.10 suggested the classification of foods according to the level of processing. The first category labeled was fresh foods obtained from plants or animals whose composition did not change after leaving nature, including greens and fruits. The second group included minimally processed foods, which underwent minor changes between the farm and the table, such as grinding, cleaning, freezing, or vacuum storage. The third category included processed foods. These included foods to which salt, sugar, or fat are added in the manufacturing process to increase their durability and palatability, including cheese, yogurt, and canned food. The fourth group was the ultra-processed foods, which has passed through different processing stages, with the addition of industrial additives to the composition, including ice cream, chocolates, cookies, and candies11. Therefore, nutritional counseling based on classification Monteiro et al. 10 could help health professionals promote nutritional health among adolescents.
Nowadays, it is easy to acquire food products ready to consume due to the practicality, accessibility, and preparation time. These foods have been allocated a lot of space in the markets and adolescents' daily lives12. As mentioned, processed foods and, above all, ultra-processed foods are nutritionally inadequate and have high energy density11. It is also noteworthy that ultra-processed foods have high palatability, which may increase the consumption of less healthy foods by children and adolescents, who are easily influenced by the lack of natural discernment of their age group13. Thus, considering the aspects mentioned above in this introduction, the nutritional approach focusing on health education could improve their quality of life.
Therefore, the objective was to assess the effects of a multi-professional approach on anthropometric parameters, body composition, and the level of food processing in adolescents. As a hypothesis, we believe that that the adolescents will improve the components of body composition and improve the food' quality after the intervention period.
METHODS
Experimental design
This study is a clinical study with follow-up. The evaluations were carried out before the start, at 6 weeks, and after 12 weeks of the multi-professional intervention.
Participants
Public announcements through radio, television, and the internet (social media) about the study were made inviting participants to register for the study, in Maringa, Parana, Brazil. At the end of registration, a meeting was held with the adolescents' parents or guardians with a detailed explanation of the study's objectives. Those applicants meeting the following criteria were accepted for inclusion: (1) male adolescents, overweight or obese within the cut-offs established by Cole and Lobstein14; (2) between 13 and 17 years old; (3) available to participate twice a week in the theoretical and practical classes of dietary re-education and group psychotherapy once a week; (4) available to perform physical exercises three times a week; and (5) being a student in the municipal or state education. The following criteria were grounds for exclusion: (1) participation in other structured projects focusing on losing weight and behavioral changes outside of school; (2) orthopedic injuries, cardiovascular diseases, or cognitive impairment that compromised understanding of the theoretical and practical classes; (3) following any diet or food plan outside the research project; (4) use of medications that prevented or enhanced weight loss; and (5) participation in less than 75% of the multi-professional sessions over the 12-week intervention.
The adolescents were asked to sign the assent form and the parents or guardians to sign the informed consent form. The research project was approved by the local research and ethics committee under number 2.505.200/2018 and registered in the Brazilian Clinical Trials Registry (RBR45ywtg). The researchers affirm that Resolution 466/2012 of the Ministry of Health and the Declaration of Helsinki were thoroughly followed during this study.
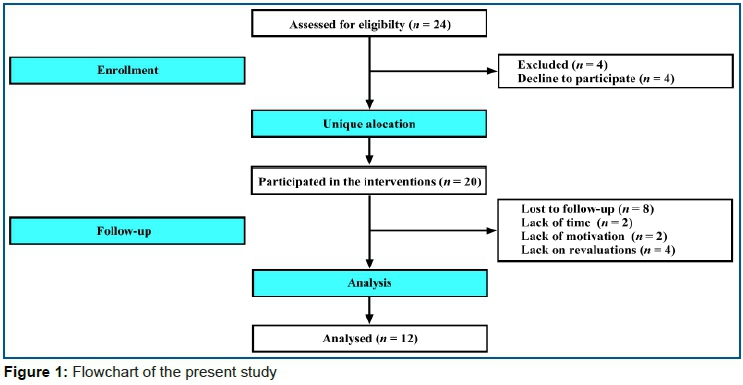
The sample calculation indicated that nine adolescents would be necessary to detect α = 0.05 and β = 80%, based on previous studies8,9. We recruited 20 adolescents who were eligible for this study. However, eight of them did not complete the 12-week intervention or gave up on the process, as shown in the flowchart below. The drop-outs were related to lack of time, lack of motivation, and missed evaluations at 12-weeks post-intervention, as presented in figure 1.
Medical history
Before the beginning of the study, the following procedures were performed by a medical team: (a) pulmonary auscultation, (b) cardiac auscultation, and (c) family history disease. All participants completed the International Physical Activity Questionnaire (IPAQ) adapted for adolescents15.
Anthropometry and body composition
To measure stature, a standard stadiometer (Sanny, Standard, São Paulo, Brazil) was used. The measure was standardized as follows: (a) the adolescent was asked to keep heels and knees together, arms loose and positioned along the body with the palms facing the thighs, legs erect, shoulders relaxed, and head aligned to the Frankfurt plane (looking toward the horizon, straight at eye level); (b) the heels, calf (optional), the buttocks, the shoulder blades and the back of the head should, when possible, by comma vertical surface of the stadiometer16.
To assess body composition, adolescents were instructed to follow the following standardization: (1) fasting for at least 4h; (2) no alcohol consumed in the previous 48h; (3) no diuretic substances used in the last 24h; (4) absence of ingestion of products with caffeine over the previous 12h; (5) no moderate or high-intensity exercises performed in the last 24h; (6) evacuating and urinating before the test; (7) no metallic objects used during the bioimpedance test; (8) wearing light clothing; (9) performing the assessment at a temperature between 20ºC and 24ºC17. After completing the procedures, the adolescents had their body composition measured via tetrapolar bioimpedance of eight tactile points, using InBody 570® (InBody, Seoul, South Korea). The variables used were: body weight, stature, body mass index (BMI), fat mass (FM), body fat (%BF), skeletal muscle mass (SMM), and resting metabolic rate (RMR).
Food record
To obtain information about the participants' eating habits, a three-day non-consecutive food record was applied. Participants were instructed to register all food and drink consumed during the day, together with portions or quantities. The adolescents were asked to complete the forms on two non-consecutive days of the week and one weekend day8,9.
To estimate the portion of food, the participants counted on the help of traditional home measures used in their respective daily routines18. Participants were also instructed to note in detail: how the food was prepared, the ingredients, the food brand, and whether the type of food was diet, light, or normal19. All records were calculated using Avanutri software (Avanutri Equipamentos de Avaliação, Três Rios, Rio de Janeiro, Brazil) by a nutritionist. Subsequently, foods were classified by the level of processing: fresh, minimally processed, processed, or ultra-processed10, in which the grams and calories of those foods were calculated.
Physical exercise protocols
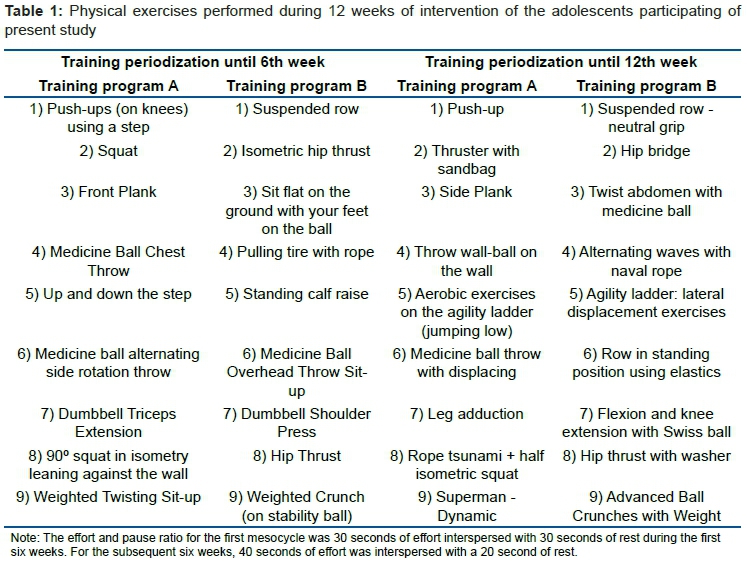
Resistance exercises were performed three times a week for 12-weeks, with an approximate duration of 75-min per training session. The circuit method was used with an emphasis on large muscle groups. The sessions were divided into training sessions A and B, which were performed alternately. The effort: pause ratio for the first mesocycle was 30 seconds of effort interspersed with 30 seconds of rest during the first six weeks. For the subsequent six weeks, 40 seconds of effort was interspersed with 20 seconds of rest. During the execution of the exercises, the repetitions were not counted. It was only requested that the concentric and eccentric phases last one time each. The choice of "functional exercises" was based on Boyle20. Table 1 shows the exercises performed over the 12 weeks of the intervention.
Nutritional counseling classes
The central theme proposed for adolescents was to comprehend the following aspects of nutrition: the food pyramid, the classification of food, the energy value of food, the relevance of macro- and micronutrients for health, the interpretation of food labels, the types of diets, eating disorders, the kinds of food recommended for pre- and post-PA, the levels of food processing, nutrition and health, and preparing healthy food in the kitchen. The nutrition lessons lasted an average of 60-min, twice a week, and were carried out in groups according to the proposal established by Branco et al.8,9.
Group psychotherapy classes
The psychology team's intervention followed the cognitive-behavioral approach and addressed these objectives: anxiety control, eating mindfully, dealing with emotions, promoting healthy eating habits, improving self-esteem, acceptance of the body itself, encouraging the practice of PA outside of school, and the interventions carried out in the higher education institution and themes brought up by the research volunteers. Each group psychotherapy session lasted 60-min, happened once a week, and was based on the proposal of Branco et al.8,9.
Statistical analysis
The Shapiro-Wilk test was used to test the normality of the data. Data are presented as mean and standard deviation. As pointed out in previous sections, measurements were made at three stages: before the intervention started, then at 6-weeks into the intervention, and at 12-weeks (end of the intervention). Therefore, a one-way analysis of variance with repeated measures was used, with the Bonferroni test as a post-hoc test if a significant difference was found between the different intervals. Cohen's d was calculated using Rhea21. A significance level of 5% was established. All statistical analyses were performed using Statistica 12.0 software (TIBCO, Palo Alto, CA, USA).
RESULTS
No significant differences were observed in PA's level via the IPAQ (p>0.05) after the intervention period. The unique difference observed was related to PA during the days of interventions. However, the increase in PA on Mondays, Wednesdays, and Fridays was expected since the adolescents were in the interventions.
Figure 2 shows the anthropometric responses of the adolescents participating in the present study.
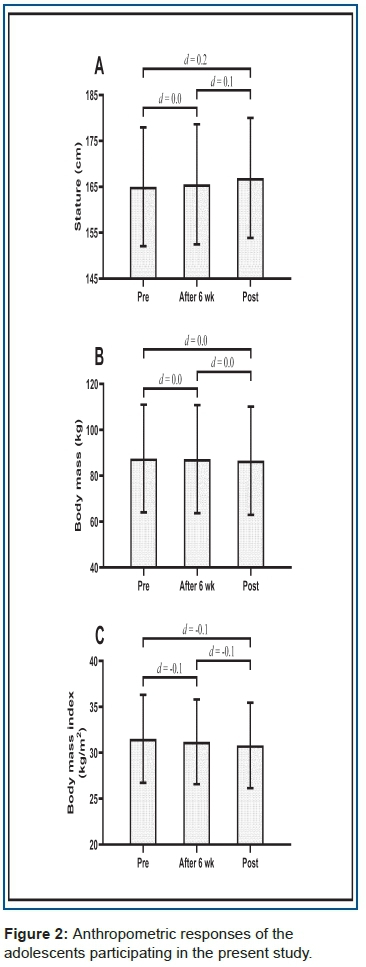
Anthropometric values did not present significant differences among the stature, body mass, and BMI during the 12-week intervention (p>0.05).
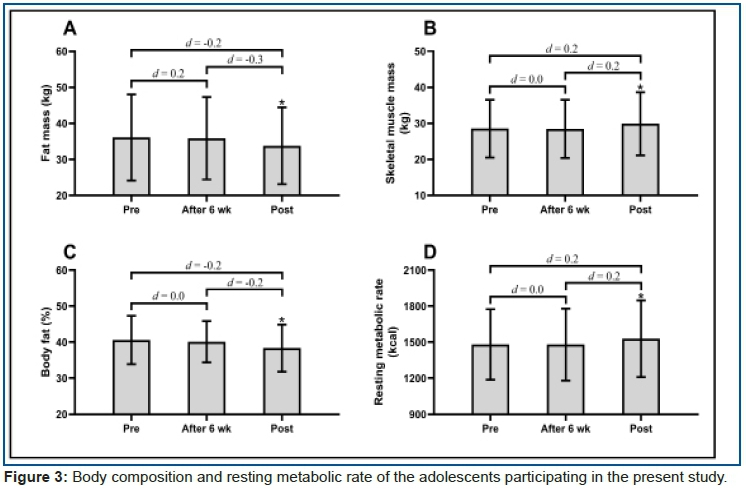
Figure 3 shows the parameters of body composition and RMR of the adolescents participating in the present study.
Body composition values showed significant differences (p<0.05), with lower values for FM and %BF and higher values for SMM and RMR after the 12-week intervention.
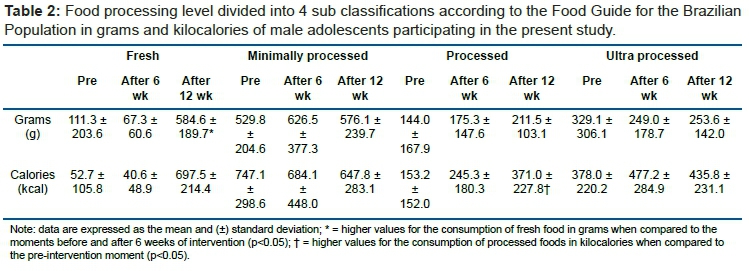
Table 2 shows the food processing level divided into four sub-classifications according to the Food Guide for the Brazilian Population in grams and kilocalories of male adolescents participating in the present study.
Consumption of fresh food in grams showed significant improvement after 12-week when compared to pre - and after 6-week post-intervention (p<0.05). The processed food showed higher values after 12-week compared to the pre-intervention period (p<0.05).
DISCUSSION
Considering that the present study aimed to investigate the effects of a multi-professional approach on the anthropometric variables, body composition, and dietary profile of overweight or obese adolescents, the main results identified were:
(1) reduction of FM and %BF;
(2) increase in SMM and RMR;
(3) increased consumption in grams of fresh food;
(4) increased caloric consumption of processed foods.
However, no significant differences were found in body weight, stature, BMI, or consumption of minimally processed and ultra-processed foods. Thus, our hypothesis was partially confirmed.
Previous evidence has indicated that body weight and BMI are not good predictors for analyzing the effects of a program focused on obesity combat8,9. This is because resistance training stimulates an increase in SMM. Consequently, if there occurs a reduction in FM and an increase in SMM, there will be no differences in the participants' BMI. Therefore, BMI can be considered as an indicator of little importance for assessing any changes induced by a physical exercise program and dietary re-education.
The participants performed physical exercises for an average of 225-min per week, distributed over three days/week. A study by Donnelly pointed out that incorporating ~150 to 250-min of PA/wk promotes an energy expenditure between 1200 and 2000 kcal.22 Wishnofsky suggests that 1 kg of %FM is equivalent to 7,700 kcal23. In contrast, according to Pietrobelli, the referred equivalent is not a magic number and can range from 7,188 to 7,700 kcal, influenced by sex, age, and biological individuality24. Therefore, the reduction of ~2 kg of FM is closely related to the increase in the level of PA among adolescents since no significant caloric consumption reductions were identified during the intervention period.
Previous evidence indicates that the increase in SMM in adolescents depends on the optimal volume and intensity of resistance training8,9. In this sense, 12 weeks of intervention may or may not provide an increase in SMM. The answers regarding the gain of SMM depend on the type of physical exercise performed. Coffey and Howley indicated that concurrent training tends to decrease muscle hypertrophy stimulus when compared to resistance training25. Thus, the recommendation to provide benefits associated with resistance and aerobic exercise is around 6-24 hours of passive rest between the different stimuli26.
The Physical Activity Guidelines for Americans27 recommends the performance of PA seven days a week, lasting ≥ 60 min. In future studies, new interventions of the following type can be tested.
1. Face-to-face sessions with trainers five times per week
2. Semi-face sessions (hybrid classes) three times per week with supervision from physical education professionals, and three more sessions per week via distance prescription with the periodization of exercises with the use of technology.
This may contribute to the increase in the practice of PA among adolescents. Another point that deserves to be emphasized is the participation of parents and family in the process of combating obesity in adolescents. Therefore, Costa et al.28 suggested that the adherence and integration of the multi-professional team, parents or guardians, and adolescents are essential for a treatment program's success. However, the present study did not include any interventions with parents or guardians. It is possible that this is a reason for the high drop-out rate in the study, with 50% of the sample giving up over the weeks. However, the drop-out appears to be a pattern during lifestyle proposals in different age groups. Therefore, motivational interventions could be tested in obesity management to promote better adherence.
RMR showed a slight increase after the intervention period. McClave and Snider indicate that 1 kg of SMM corresponds to a total energy expenditure of 13/kcal/kg/day29. Therefore, the increase in the identified RMR has a low relationship with the rise in SMM. Thus, it is believed that the differences found are mainly due to the increase in the level of PA30 over the 12-week intervention. Given this, the increase in RMR is related to the rise in the level of PA in unstructured activities and the physical exercise program that was carried out during the intervention31. In addition, regular and systematic physical exercise promotes metabolic adaptations that elevate adaptive thermogenesis to promote increased glycolytic and oxidative enzymes' increased efficiency, contributing to the oxidation of free fatty acids in SMM32.
Recent evidence has reinforced the need to reduce ultra-processed food consumption to combat obesity in adolescents28. Among the recommendations, we stressed on the decrease in the consumption of ultra-processed and processed foods, increased consumption of fruits and vegetables, and encouraged family meals33. Therefore, the increase in consumption of fresh foods/g identified in the present study can be considered beneficial, as they are related to the promotion and recovery of health conditions in different NCDs. In line with the author mentioned above, Steele et al.34 suggested that the increase in the consumption of fresh foods and minimally processed foods may help the weight loss process because they are relatively healthier and have lower energy density.
Another point observed after the intervention period was the increase in consumption of processed foods. However, it cannot be said that this result is negative, given that a qualitative analysis of food eaten has not been performed. Standard foods such as cheese, yogurt, jelly, homemade bread, French bread, and canned tuna are classified as processed foods10. It is also worth noting that the foods described above are part of the regular Brazilian diet (middle-class people consume most of the foods listed sometimes people with lower purchasing power tend to eat high-calorie and nutritionally deficient foods). Additionally, knowing the complexity of achieving a change in eating habits and the need to adopt the right strategies so that this process becomes more effective, more prolonged action focusing on adolescents' nutritional education is indispensable.
Because of the minor changes in body composition, dietary profile, and absence of differences in anthropometric values of the adolescents investigated, interventions with ≥ 12 weeks in length are recommended, in line with our American Guide to Obesity Management35. Furthermore, it is emphasized that the absence of a control group in the present study is justified because it is not recommended to prevent people with serious health problems from not participating in interventions that aim to improve parameters related to the fight against obesity36. A prior study has also suggested that behavioral interventions have been recommended for obesity treatment35; in view of this, previous studies with similar designs have presented success in parameters related to obesity treatment with adolescents with the same length of interventions in the multi-professional approach8,9. Accordingly, it is indispensable to inform that obesity treatment can be carried out during aging. Health promotion lifestyle changes are important for overall health and longevity.
One limitation of the study was its high drop-out rate of 50%. When we intend to treat humans and the objective is to change behavior aspects, several difficulties can occur. Behavioral interventions in the adolescent group need to be include parents. When behavioral changes are conducted with people who do not wish to change their behavior, changes in their nutritional behavior, PA stimulus, and mental health are unlikely to occur. Thus, prior to intervening, their receptivity for intervention and readiness for change must be taken into account37. Finally, as future directions, we emphasize the need to involve parents in behavioral intervention programs in scientific research and clinical practice to maintain adherence and promote healthy habits in the family.
CONCLUSION
It was concluded that 12-week multi-professional interventions can reduce FM and %BF, as well as increase, SMM, RMR, and the consumption of fresh foods. Another point that could be highlighted is the 50% rate of drop-out during the interventions.
Author Contributions
FMO, DCSM, AAC, MGSM, CGAA and BHMB contributed to the study's conception and design. FMO, DCSM and AAC organized the database. BHMB performed the statistical analysis. FMO, DCSM, AAC and BHMB wrote the first draft of the manuscript. FMO, CGAA and BHMB wrote the sections of the manuscript. All authors contributed to the manuscript and approved the final version.
Funding
This research was financed by ICETI - Cesumar Institute of Science, Technology, and Innovation and Fundação Araucária, via call notice "CP 20/18: Young Researchers - PPP".
Acknowledgments
The authors thank everyone who participated directly or indirectly in the development of this study.
Conflicts of Interest
The authors declare no conflict of interest.
REFERENCES
1.Elvsaas IKO, Giske L, Fure B, Juvet LK. Multicomponent Lifestyle Interventions for Treating Overweight and Obesity in Children and Adolescents: A Systematic Review and Meta-Analyses. J Obes. 2017; 2017: 5021902. DOI: https://doi.org/10.1155/2017/5021902 [ Links ]
2.Martin A, Booth JN, Laird Y, Sproule J, Reilly JJ, Saunders DH, et al. Physical activity, diet and other behavioural interventions for improving cognition and school achievement in children and adolescents with obesity or overweight. Cochrane Database Syst Rev Phys. 2018. DOI: https://doi.org/10.1002/14651858.CD009728.pub3 [ Links ]
3.de Oliveira ASD, Moreira NF, de Moraes AB de V, Pereira RA, De Veiga GV. Co-occurrence of behavioral risk factors for chronic non-communicable diseases in adolescents: Prevalence and associated factors. Rev Nutr. 2017; 30(6): 747-58. DOI: https://doi.org/10.1590/1678-98652017000600007 [ Links ]
4.World Health Organization (WHO). Obesity: Preventing and managing the global epidemic: report of a WHO consultation. Geneva, Switzerland; 2000. [ Links ]
5.Instituto Brasileiro de Geografia e Estatística (IBGE). Pesquisas de orçamentos familiares 2008-2009: Antropometria e Estado Nutricional de Crianças, Adolescentes e Adultos no Brasil. Rio de Janeiro: IBGE; 2010. [ Links ]
6.Instituto Brasileiro de Geografia e Estatística (IBGE). Pesquisa nacional de saúde do escolar: 2015. Rio de Janeiro: IBGE; 2016. [ Links ]
7.Souza AM, Barufaldi LA, Abreu GA, Giannini DT, Oliveira CL, Santos MM, et al. ERICA: intake of macro and micronutrients of Brazilian adolescents. Rev. Saúde Pública. 2016; 50(1): 1-15. DOI: https://doi.org/10.1590/S01518-8787.2016050006698 [ Links ]
8.Branco BHM, Carvalho IZ, de Oliveira HG, Fanhani AP, dos Santos MCM, de Oliveira LP, et al. Effects of 2 Types of Resistance Training Models on Obese Adolescentsʼ Body Composition, Cardiometabolic Risk, and Physical Fitness. J Strength Cond Res. 2020; 34 (9): 2672-2682. DOI: https://10.1519/jsc.0000000000002877 [ Links ]
9.Branco BHM, Valladares D, de Oliveira FM, Carvalho IZ, Marques DC, Coelho AA, et al. Effects of the Order of Physical Exercises on Body Composition, Physical Fitness, and Cardiometabolic Risk in Adolescents Participating in an Interdisciplinary Program Focusing on the Treatment of Obesity. Front Physiol 2019; 10: 1013. DOI: https://10.3389/fphys.2019.01013 [ Links ]
10.Monteiro CA, Levy RB, Claro RM, Castro IRR de, Cannon G. A new classification of foods based on the extent and purpose of their processing. Cad Saúde Pública. 2010; 26(11): 2039-49. DOI: https://doi.org/10.1590/S0102-311X2010001100005 [ Links ]
11.Svisco E, Shanks CB, Ahmed S, Bark K. Variation of adolescent snack food choices and preferences along a continuum of processing levels: The case of apples. Foods. 2019; 8(2): 50. DOI: 10.3390/foods8020050 [ Links ]
12.Enes CC, Camargo CM de, Justino MIC. Ultra-processed food consumption and obesity in adolescents. Rev Nutr. 2019; 32: e180170. DOI: https://doi.org/10.1590/1678-9865201932e180170 [ Links ]
13.Machado PP, Claro RM, Canella DS, Sarti FM, Levy RB. Price and convenience: The influence of supermarkets on consumption of ultra-processed foods and beverages in Brazil. Appetite. 2017; 116: 381-388. DOI: http://doi.org/10.1016/j.appet.2017.05.027 [ Links ]
14.Cole TJ, Lobstein T. Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatr Obes. 2012; 7(4): 284-94. DOI: https://doi.org/10.1111/j.2047-6310.2012.00064.x [ Links ]
15.Guedes DP, Lopes CC, Guedes JERP. Reproducibility and validity of the International Physical Activity Questionnaire in adolescents. Rev Bras Med do Esporte. 2005; 11(2): 151-8. DOI: https://doi.org/10.1590/S1517-86922005000200011 [ Links ]
16.Norgan NG. A Review of: "Anthropometric Standardization Reference Manual". Edited by Lohman TG, Roche AF and Martorell R. (Champaign, IL.: Human Kinetics Books, 1988). Ergonomics. 1988; 30(10): 1493-1494. DOI: https://doi.org/10.1080/00140138808966796 [ Links ]
17.Guedes DP. Procedimentos clínicos utilizados para análise da composição corporal. Rev Bras Cineantropometria e Desempenho Hum. 2013; 15(1): 113-29. DOI: https://doi.org/10.5007/1980-0037.2013v15n1p113 [ Links ]
18.Pinheiro ABV, Lacerda EM de A, Benzecry EH, Gomes MC da S, Costa VM. Tabela para avaliação de consumo alimentar em medidas caseiras. 5 ed. São Paulo: Atheneu; 2008. [ Links ]
19.Fisberg RM, Marchioni DML, Colucci ACA. Avaliação do consumo alimentar e da ingestão de nutrientes na prática clínica. Arq Bras Endocrinol Metabol. 2009; 53(5): 617-24. DOI: https://doi.org/10.1590/S0004-27302009000500014 [ Links ]
20.Boyle M. O Novo Modelo de Treinamento Funcional de Michael Boyle. 2a ed. Porto Alegre: Artmed; 2018. [ Links ]
21.Rhea MR. Determining the Magnitude of Treatment Effects in Strength Training Research Through the Use of the Effect Size. J Strength Cond Res. 2004; 18(4): 918-20. DOI: http://doi:10.1519/14403.1 [ Links ]
22.Donnelly JE, Blair SN, Jakicic JM, Manore MM, Rankin JW, Smith BK. American College of Sports Medicine Position Stand. Appropriate physical activity intervention strategies for weight loss and prevention of weight regain for adults. Med Sci Sports Exerc. 2009; 41(2): 459-71. DOI: https://doi:10.1519/14403.1 [ Links ]
23.Wishnofsky M. Caloric Equivalents of Gained or Lost Weight. Am J Clin Nutr. 1958; 6(5): 542-6. DOI: https://doi:10.1093/ajcn/6.5.542 [ Links ]
24.Pietrobelli A, Allison DB, Heshka S, Heo M, Wang ZM, Bertkau A, et al. Sexual dimorphism in the energy content of weight change. Int J Obes. 2002; 26(10): 1339-48. DOI: https://doi:10.1038/sj.ijo.0802065 [ Links ]
25.Coffey VG, Hawley JA. Concurrent exercise training: do opposites distract? J Physiol. 2017; 595(9): 2883-96. DOI: https://doi:10.1113/JP272270 [ Links ]
26.Murach KA, Bagley JR. Skeletal Muscle Hypertrophy with Concurrent Exercise Training: Contrary Evidence for an Interference Effect. Sport Med. 2016;46(8):1029-39. DOI: https://doi:10.1007/s40279-016-0496-y [ Links ]
27.For Powell KE, King AC, Buchner DM, Campbell WW, DiPietro L, Erickson KI, et al. The Scientific Foundation for the Physical Activity Guidelines for Americans, 2ª Edition. J Phys Act Heal. 2019; 16(1):1-11. [ Links ]
28.Costa CS, Del-Ponte B, Assunção MCF, Santos IS. Consumption of ultra-processed foods and body fat during childhood and adolescence: A systematic review. Public Health Nutr. 2018; 21(1): 148-59. DOI: https://doi:10.1017/S1368980017001331 [ Links ]
29.McClave SA, Snider HL. Dissecting the energy needs of the body. Curr Opin Clin Nutr Metab Care. 2001; 4(2): 143-7. DOI: https://doi:10.1097/00075197-200103000-00011 [ Links ]
30.Byrne NM, Hills AP. How much exercise should be promoted to raise total daily energy expenditure and improve health? Obes Rev. 2018; 19: 14-23. DOI: https://doi:10.1111/obr.12788 [ Links ]
31.Westerterp KR. Exercise, energy expenditure and energy balance, as measured with doubly labelled water. Proc Nutr Soc. 2018; 77(1): 4-10. DOI: https://doi:10.1017/S0029665117001148 [ Links ]
32.Müller MJ, Enderle J, Bosy-Westphal A. Changes in Energy Expenditure with Weight Gain and Weight Loss in Humans. Curr Obes Rep. 2016; 5(4): 413-23. DOI: https://doi:10.1007/s13679-016-0237-4 [ Links ]
33.Cardel MI, Jastreboff AM, Kelly AS. Treatment of Adolescent Obesity in 2020. JAMA. 2019; 322(17): 1707-08. DOI: https://doi:10.1001/jama.2019.14725 [ Links ]
34.Steele EM, Baraldi LG, Da Costa Louzada ML, Moubarac JC, Mozaffarian D, Monteiro CA. Ultra-processed foods and added sugars in the US diet: Evidence from a nationally representative cross-sectional study. BMJ Open. 2016; 6(3): 1-8. DOI: https://doi:10.1136/bmjopen-2015-009892 [ Links ]
35.Jensen MD, Ryan DH, Apovian CM, Ard JD, Comuzzie AG, Donato KA, et al. 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults: A report of the American College of Cardiology/American Heart Association Task Force On Practice Guidelines And The Obesity Society. J Am Coll Cardiol. 2014; 63(25): 2985-3023. DOI: https://doi.org/10.1016/j.jacc.2013.11.004 [ Links ]
36.Hecksteden A, Faude O, Meyer T, Donath L. How to construct, conduct and analyze an exercise training study? Front Physiol. 2018; 9: 1-15. DOI: https://doi:10.3389/fphys.2018.01007 [ Links ]
37.Toral N, Slater B. Abordagem do modelo transteórico no comportamento alimentar. Cien Saude Colet. 2007; 12(6): 1641-50. DOI: https://doi.org/10.1590/S1413-81232007000600025 [ Links ]
 Correspondence:
Correspondence:
Braulio Henrique Magnani Branco
braulio.branco@unicesumar.edu.br
Manuscript received: November 2020
Manuscript accepted: February 2021
Version of record online: July 2021


{kind=link}
{kind=link}
{kind=link}
{kind=link}