










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores
Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282versão On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.32 no.1 Santo André jan./abr. 2022
https://doi.org/10.36311/jhgd.v32.12617
ORIGINAL ARTICLE
doi: 10.36311/jhgd.v32.12617
Vaccine coverage and measles incidence in Northern Brazil
Carolina Miranda ParraI; Mariane Albuquerque Lima RibeiroII, III; Italla Maria Pinheiro BezerraIV; Maura Regina RibeiroII, III; Luiz Carlos de AbreuI, II, III
IPrograma de Pós-Graduação em Ciências da Saúde na Amazônia Ocidental, Universidade Federal do Acre, Rio Branco, AC, Brasil
IIPrograma de Pós-Graduação em Ciências da Saúde, Centro Universitário Saúde ABC, Santo André, São Paulo, SP, Brasil
IIILaboratório de Delineamento de Estudo e Escrita Científica, Centro Universitário Saúde ABC, Santo André, São Paulo, SP, Brasil
IVPesquisador da Escola Superior de Ciências de Santa Casa de Misericórdia de Vitória, ES - Brazil
ABSTRACT
INTRODUCTION: measles is an immunopreventable viral disease, acute exanthematous and extremely transmissible. Infection occurs directly, from person to person, through respiratory secretions. The measles vaccine is low-cost and effective, but measles still affects around 40 million people worldwide and is responsible for at least 800,000 deaths, mainly in developing countries
OBJECTIVE: to analyze vaccination coverage and measles incidence in Northern Brazil
METHODS: this is an ecological study. Secondary data were used regarding vaccination coverage of the viral double, viral triple and viral tetra and incidence of measles in residents in the States of the Northern Region, Brazil, from 2010 to 2018
RESULTS: confirmed measles cases in 2010 to 2018 in the Northern region of Brazil it registered 10,249, were reported in Amazonas (95.65%), Roraima (3.53%), Pará (0.80%) and Rondônia (0.02%). Outbreaks of measles cases in the Northern Region were reported in 2018, the highest incidence rate was in Amazonas with 237.7. Vaccination coverage in the North Region varied between the lowest rate in 2013 with 56.88% and the highest vaccination coverage achieved in 2010, with 104.02%
CONCLUSION: it was possible to observe a reduction in vaccination coverage during the study period, not reaching the percentage recommended by the Ministry of Health and increasing the incidence of measles in the Northern Region of Brazil and these indicators are important to determine the strategies to be carried out by the National Program for Immunization and Epidemiological Surveillance
Keywords: Vaccination coverage. Measles. Incidence.
Authors summary
Why was this study done?
In view of the alarming growth of measles cases in Brazil, especially in the northern region of the country, this study was carried out in order to analyze the vaccination coverage and incidence of measles in the northern region of Brazil.
What did the researchers do and find?
A study was carried out with secondary data regarding the double, triple and tetra viral vaccination coverage and incidence of measles in residents in the state of the Northern Region, Brazil, from 2010 to 2018. The results were based on epidemiological bulletins, Sistema de Informação de Imunização and Sistema de Informação de Internação Hospitalar. There was a reduction in vaccination coverage, which in the study period does not reach the percentage recommended by the Ministry of Health and the increase in the incidence of measles in the Northern Region of Brazil, and these indicators are important to determine the strategies to be carried out by the National Program for Immunization and Epidemiological Surveillance.
What do these findings mean?
With the increase in measles cases in the North of Brazil and a decrease in the percentage of vaccination coverage recommended by the Ministry of Health, the need for health strategies and campaigns for vaccination coverage to reach the recommendation is evident, and should be carried out frequently and with emphasis on not having new measles cases and especially the non-occurrence of death from an immunopreventible disease. These indicators are important to determine the strategies to be carried out by the National Program for Immunization and Epidemiological Surveillance.
INTRODUCTION
Measles is an immunopreventable, acute exanthematous viral disease, extremely transmissible, caused by viruses of the Paramyxoviridae family of the genus Morbillivirus1. The infection occurs directly, from person to person, through respiratory secretions, and the virus can remain active for up to two hours in the air or on surfaces2.
The incubation period can last up to eleven days and the disease can last from three to four days, presenting a clinical picture of high fever, coryza, serumucosa, conjunctivitis with photophobia, dry cough. In addition, Koplik patches may appear, which are white dots located on the oral mucosa. Around the fourth day of the disease onset, the reddish maculopapular rash begins, starting with the face, retroauricular and cervical regions1,3.
Most measles deaths occur from complications associated with the disease. They are more common in children under the age of five or in adults over the age of 30. These complications include blindness, severe diarrhea, severe respiratory and auditory system infections, even encephalitis3. Measles has an important cause of hospitalization, morbidity and mortality in childhood, and may be related to the degree of socioeconomic development of those infected4.
Measles is still common in many developing countries. About 95% of deaths from measles occur in low-income countries and where there is a weak health infrastructure3. According to the World Health Organization (WHO), an estimated 36.5 million cases and 1.5 million deaths from measles occur worldwide each year1.
Comprised of live attenuated virus (with low pathogenicity), the measles vaccine was introduced in Brazil during the years 1967 and 1968, becoming a nationally mandatory notification disease5,6, however, it was used in a discontinuous way until 19737.
In 1973, the National Immunization Program (PNI) was created, which aimed to implement immunization actions across the country. In 1980, a vaccination campaign was carried out in places with low vaccination coverage. Until 1990, measles was considered an endemic disease, with some peaks every 2, 3 years, having its biggest epidemic in 1986. In 1992, Brazil instituted the National Measles Elimination Plan (1992), with the goal of eliminating measles by the year 2000, reaching 96.7% of vaccination coverage7.
Brazil received the measles eradication certificate from the Pan American Health Organization in 2016. However, the outbreak that occurred in the north of the country in 2018 highlighted the need for continuous surveillance to control this pathology1.
In 2018, Brazil faced the reintroduction of the measles virus and outbreaks were detected in at least 11 Brazilian states. According to the Ministry of Health, this outbreak is related to imports, because in a viral characterization, the D8 genotype was identified, identical to that circulating in Venezuela in an outbreak that the country suffered in 20178. The North region was the most affected due to low vaccination coverage.
Thus, the objective of this work is to analyze the vaccination coverage and the incidence of measles in the Northern Region of Brazil in the period from 2010 to 2018, therefore, this study is justified by the importance of evaluating the epidemiological profile and vaccination status of measles in North region, since this region has the largest number of measles cases in Brazil.
METHODS
Study Design
This is an ecological study. Secondary data referring to vaccination coverage of the double, triple and tetra viral measles incidence in residents in the states of the Northern Region, Brazil, from 2010 to 2018.
Study Location and Period
Data were collected according to place of residence. The collection took place through the data available at the Department of Informatics of the Unified Health System (DATASUS - http://datasus.saude.gov.br/), National Immunization Program (PNI), Hospital Information System (SIH) and through the Ministry's portal of Health through epidemiological measles bulletins (http://www.saude.gov.br/saude-de-az/sarampo-situacao-epidemiologica). Secondary data corresponded to the period from January 1, 2010 to December 31, 2018. Data were collected from the seven states in the Northern region of Brazil: Amazonas (AM); Roraima (RR); Amapá; Pará (PA); Tocantins (TO); Rondônia (RO); Acre (AC).
Study Population and Eligibility Criteria
New measles cases were counted from the confirmed ones caused by Measles, occurred and notified Hospital Information System (SIH) and epidemiological bulletins according to the age group established by the World Health Organization (WHO).
Data from the Notifiable Diseases Information System (SINAN) were not used, since the last update of measles information was in 2014 and for this reason, it was decided to use confirmed measles cases by epidemiological bulletins. Knowing that these data can be changed, the study used the last bulletin with the number 37, of 03/19/2019.
For the construction of the incidence rate, data were collected from the population residing in the states of the Northern Region, Brazil from the 2010 and 2018 censuses and from inter-census projections for the other years (from 2010, to 2018), according to information provided by DATASUS.
All new measles cases from 2010 to 2018 were included, considering Chapter I (Some infectious and parasitic diseases), according to the 10th Review of the International Classification of Diseases (ICD-10) at: B05.0 - Measles complicated by encephalitis, B05.1 - Measles complicated by meningitis, B05.2 - Measles complicated by pneumonia, B05.3 - Measles complicated by otitis media, B05.4 - Measles with intestinal complications, B05.8 - Measles with other complications and B05.9 - Measles without complications.
Data Collection
The data were extracted from the file transfer service provided by the Department of Informatics of the Unified Health System (DATASUS) (website: http://datasus.saude.gov.br/), which started with the systematic registration of data from Vital Statistics - Mortality and Live Births and Epidemiological and Morbidity - Hospital Morbidity of SUS (SIH/SUS) and Diseases and Notifiable Diseases (from 2007 onwards (SINAN)), Health Care - Immunization (since 1994) of the National Health Program Immunization (PNI) and measles epidemiological bulletins. With the advances in the control of infectious diseases, the analysis of the sanitary situation started to incorporate other dimensions of the health status, including epidemiological and morbidity information, which were obtained through measles hospitalizations.
To consult the data, the TABNET and TABWIN programs were used. These tabulators were developed to perform quick tabs on files. Data were collected by two independent researchers to identify possible discrepancies.
Data Analysis
Descriptive statistics was used to characterize and summarize the data set. The frequencies were expressed by absolute and relative measures. For analytical statistical analysis, linear regression was performed using the GRAPH PRISMA 6.0 program, estimating the slope (β) and the respective probability (p), the determination coefficient (r2), considering a significance level of 5%.
To build the incidence rate, data were collected from the population residing in the states of the Northern Region, Brazil, from the 2010 and 2018 censuses and from inter-census projections for the remaining years (from 2010, to 2018), according to information provided by DATASUS.
Ethical and Legal Aspects of the Research
The present study involved only the description and analysis of secondary data: population-obtained by the general population census and deaths-collected from the Information System. All of these information sources are in the public domain. Information that is not freely accessible was not collected. In particular, no personally identifiable information was obtained for this study.
According to Resolution nº 510/2016, of April 7, 2016, of the National Health Council, it was not registered or evaluated by the CEP/CONEP system, as publicly available information was used.
RESULTS
Of the total of confirmed measles cases in 2010 to 2018, the northern region of Brazil registered 10,249. The following states were notified: Amazonas (95.65%), Roraima (3.53%), Pará (0.80%) and Rondônia (0.02). Of the outbreaks of measles cases in the North Region reported in 2018, the highest incidence rate was in Amazonas with 237.7 (Table 1).
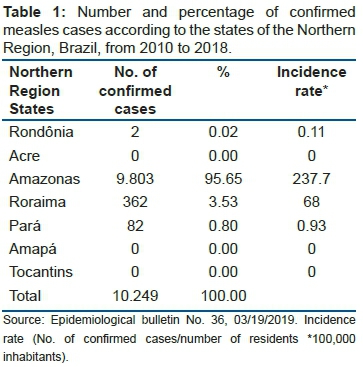
Of the total of 10,249 confirmed measles cases from 2010 to 2018, only 03 cases were reported in 2010 in the state of Pará and 01 cases in Roraima in 2015 and the rest were exclusively in 2018. In 2018, cases measles were higher in the State of Amazonas (9.803), followed by Roraima (361). In the States of Acre, Amapá and Tocantins, measles cases from 2010 to 2018 were not confirmed, as shown in Table 2.
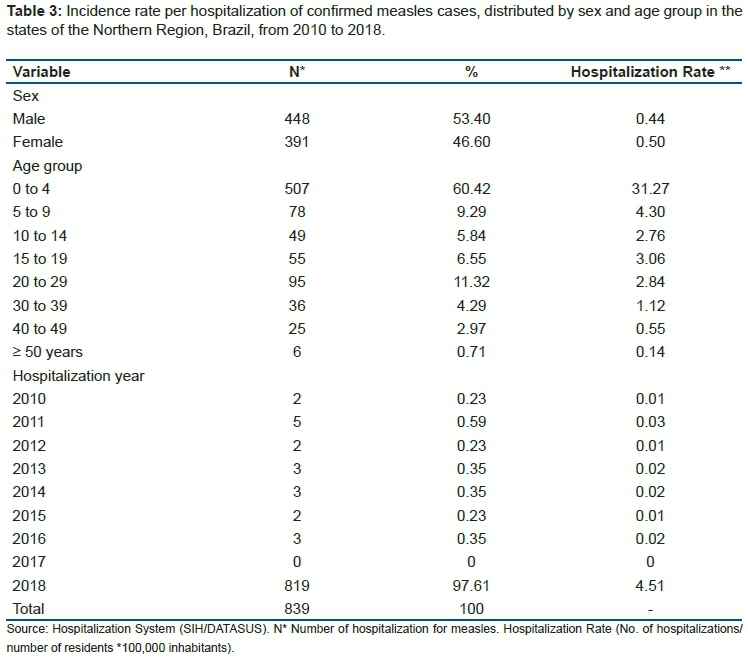
The largest number of people affected was male (53.4%) and 46.6% female. The greatest number of people affected by age group was from 0 to 4 years (60.42%).
In Table 3, it can be seen that the largest number of people affected was male (53.4%) and 46.6% female. The greatest number of people affected by age group was from 0 to 4 years (60.42%).
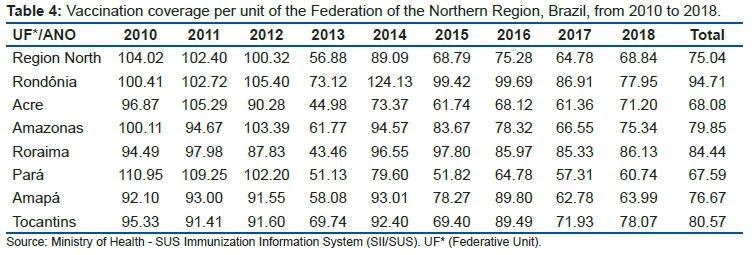
As for vaccination coverage, the North Region had the lowest rate in 2013, with 56.88%, and the highest vaccination coverage achieved in 2010, with 104.02%. In 2017 and 2018, vaccination coverage of 64.78% and 68.84% was obtained, respectively. The state that obtained the highest vaccination coverage, between the years 2010 to 2018, was Rondônia, with around 94.71%. The one that reached the lowest vaccination coverage was in the states of Acre and Pará (Table 4). In 2013, the lowest vaccination coverage recorded in the period from 2010 to 2018 was obtained (56.88%).
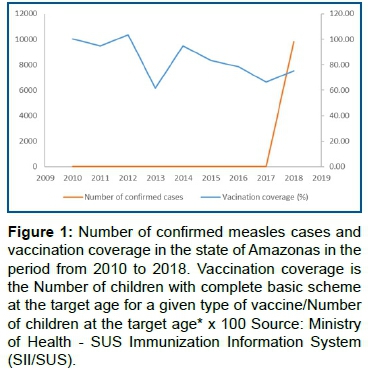
In Amazonas, there was a reduction in vaccination coverage in 2017, but in 2018 the number of confirmed measles cases increased with the notification of 9.803 together with an increase in vaccination coverage, with coverage always being below what is recommended by the Ministry Health (Figure 1).
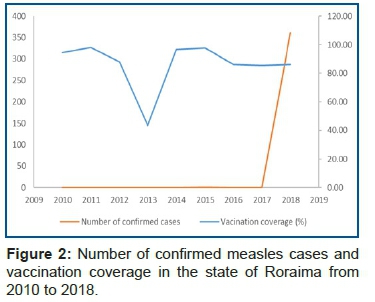
In figure 2, vaccination coverage dropped sharply in 2013 in the state of Roraima, but in the year 2016 to 2018 it remains stable and, in the period of 2018, there was a measles outbreak with 361 reported cases.
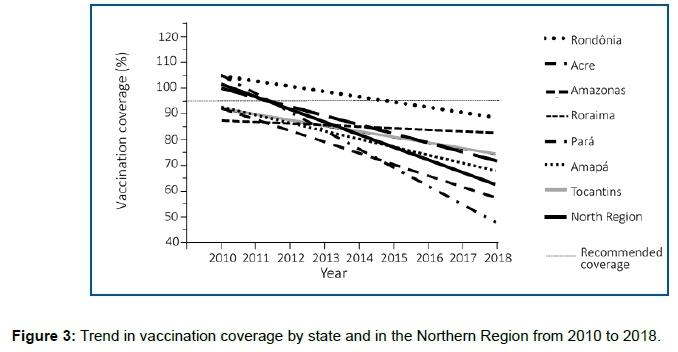
The average vaccination coverage in the years analyzed in the states of the Northern Region was 75.04%. In figure 3, it is shown that all states in the North region did not reach the goal recommended by the Ministry of Health and there is also a tendency to reduce vaccination coverage. The state of Pará (p-value <0.001) and the North Region (p-value <0.023) were statistically significant.
DISCUSSION
Over the years analyzed in this study (from 2010 to 2017), only 4 cases of measles were recorded for the North region, however, in 2018 there were 10.245 cases. In 2018, measles cases were highest in the State of Amazonas with 9.803 cases followed by Roraima with 361 reported cases. With regard to the average vaccination coverage in the years analyzed in the states of the Northern Region was 75.04% and in the years 2017 and 2018, vaccination coverage of 64.78% and 68.84% was obtained, respectively.
Brazil has been suffering from the increase in measles cases. 2018 was considered the period with measles outbreak, mainly in the North region. It is noted that this outbreak happened years after Brazil received the certificate of measles-free area. Some factors may be associated with the low vaccination coverage found in some years, such as, for example, anti-vaccination movements, the availability of vaccines in extreme regions and the lack of awareness among the population about the importance of vaccination in children. Another factor that may be influencing is the difficulty encountered by health technicians in the immunization data platform9.
In outbreaks reported before 2013, both sexes were affected, with a predominance of males10,11 corroborating this work, which also registered the highest occurrence of confirmed cases in males. Similar was also found in Ceará (northeast region) in 2013, which registered an epidemic with 1.052 confirmed measles cases, 13 years after having its last confirmed case. The high incidence of measles in males has also been demonstrated12.
Report nº. 37 of the Ministry of Health in 2016 informs that Brazil received the certificate of elimination of the circulation of the measles virus by the World Health Organization (WHO)8. According to Report nº. 28 of the Ministry of Health 2018 before certification, the last measles cases in Brazil were recorded in 2015, in outbreaks in the States of Ceará (211 cases), São Paulo (2 cases) and Roraima (1 case) and associated with the Ceará outbreak13.
The outbreak of the disease may be associated with anti-vaccination movements. These are old, but offer danger to populations around the world14. In 1998, an article was published in the The Lancet journal that related the mercury present in the triple viral vaccine with autism, but later that article was retracted and the author responded criminally. Anti-vaccines are still supported by this article and researcher. This movement was mentioned in the report of the World Health Organization, that talks about the ten biggest risks to global health. However, this movement has been growing and gaining strength worldwide, including in Brazil15. These movements question the effectiveness of vaccination, the benefit of the pharmaceutical industry. They also talk about the possible problems or reactions that can result after the vaccine, for religious reasons, among other reasons14.
The northern region of Brazil shows measles growth, having one of the highest records in relation to the last four years. Of the 7 states in the region, three are in a state of alert and emergency in Public Health, contributing to the loss of the certification of eradication due to confirmed cases16, and such data corroborates with the present study.
According to the Ministry of Health, the northern region is the location of the highest concentration of the virus with the same viral characteristic, the D8 genotype, circulating in Venezuela8. The states with the highest percentage of measles occurrence in the Northern region border and serve as refuges for immigrants, such as Venezuelans, Bolivians, Haitians, among others, thus possibly interfering in the spread of measles.
According to the Epidemiological Bulletin nº. 37, the state of Roraima received many immigrants from Venezuela, who were housed in shelters, homes, rented houses and public squares. In view of this, greater vigilance is needed in places bordering countries that are not rigorous in vaccinating the population8.
The states of the North region with the highest incidence of measles was Amazonas, Roraima and Pará, and the least number of cases is Rondônia, whereas the states of Acre, Amapá and Tocantins had no records of the disease in 2018, maintaining vaccine control without the risk outbreak16.
According to Leite et al. (2019), the State of the Northern Region that showed the lowest rate of vaccination coverage was Roraima17.
There was a decrease in vaccination coverage in 2013 in all states in the Northern region in this study. This fact may be associated with the expansion of the Basic Child Vaccination Calendar with the introduction of the tetra viral vaccine to replace the triple viral vaccine for children aged 15 months18. According to Chaves et al. (2020)19, in 2013 the vaccination of the triple viral (D1) in 12-month-old children remained with good vaccine coverage, however, there was a drop in the North region in the vaccination of D2 and tetra viral (recently introduced)20. Even if D1 is performed, D2 or viral tetra is extremely important, since by failing to complete the doses for complete immunization, individuals remain susceptible, thus, they can maintain the circulation of the virus19.
The data obtained in this study corroborate the study carried out by Chaves (2020)19, in which the vaccination coverage trend has dropped sharply between the years 2013 to 2015, remaining so until February 202019. Still according to the work by Chaves (2020)19, the data obtained are predominant in both children and adults, which shows that vaccination at all ages is important for reducing the spread of the virus.
According to the Ministry of Health, some reasons may explain the reduction in vaccination coverage over the years in all regions of Brazil and especially in the North, reasons that stand out: diseases that are not common or that have disappeared, parents who have the perception that there is no need to vaccinate; ignorance of the vaccination schedule and mandatory vaccines; fear of the vaccine causing some side effect in the child; the fear that the number of immunizers will overload the immune system; socioeconomic conditions; the availability to go to the vaccination posts and even the family's link to the posts9.
Herrera-Benavente et al. (2018)20 demonstrated the evolution of measles incidence in Latin America from 1980 to September 21, 2018, and that from 2011, the number of cases increased each year, as well as highlighted countries with greater numbers of measles cases, comprising Canada, the United States of North America, Brazil and the Bolivarian Republic of Venezuela20.
According to the Special Bulletin published by the Ministry of Health, with regard to immunization, in recent years, the coverage of the triple viral vaccine in Brazil has shown a decrease21, similar to this study.
The age group of children aged 0 to 4 years was the most affected by the outbreak in 2018, thus, the Ministry of Health intensified vaccination campaigns with an emphasis mainly on children under five22, as it is more frequent in this age group3. In this way, they launched the "D Day" of national mobilization against measles, where the goal was to vaccinate all children regardless of vaccination status, with the aim of increasing the recommended vaccination coverage and reducing measles cases.
Some actions in 2018 were carried out by the Ministry of Health with the objective of interrupting the transmission of the measles virus, such as: a) Acquisition of approximately 49.8 million doses of triple viral vaccine; b) Carrying out a "vaccination block" in suspected cases and in strategic locations; c) Intensive vaccination campaigns in places where the highest number of cases occurred; d) Rapid monitoring of post-campaign coverage9.
According to Epidemiological Bulletin Special No. 2019, in all vaccination actions carried out in 2018, approximately 22 million doses of measles vaccine were administered21.
In order to interrupt the circulation of the virus, the Ministry of Health develops some recommendations: a) Maintain high and homogeneous vaccine coverage of the triple and viral tetra; b) In positive measles areas, carry out sweeping and vaccination intensification; c) Systemic evaluation of vaccination coverage; d) Conduct the vaccination of groups considered at risk; e) Perform retrospective searches for patients with measles triad in silent municipalities; f) Reinforce the field investigation teams; g) Perform blocking within 72 hours of suspected cases; h) Produce a wide media campaign; i) Establish strategies for implementing rapid response actions in the face of new imported cases; j) Plan vaccination strategies in environments where crowds occur (airports, churches, schools).
Thus, it is evident the need for health strategies and campaigns so that vaccination coverage reaches what is recommended by the Ministry of Health, and should be carried out frequently and with emphasis so that new cases of measles do not arise and, mainly, the non-occurrence of death by an immunopreventable disease.
CONCLUSION
It was found that, during the study period, the reduction in vaccination coverage in all the years analyzed did not reach the percentage recommended by the Ministry of Health, as well as an increase in the incidence of measles in the Northern Region of Brazil in 2018 was evidenced. Hospitalization rate was higher in 2018, the year that the last measles outbreak occurred. These indicators are important to determine the strategies to be carried out by the National Program for Immunization and Epidemiological Surveillance.
Authors' Contributions:
conceptualization, C.M.P.; M.A.L.R., L.C.A.; methodology, C.M.P.; M.A.L.R., L.C.A.; data collection, C.M.P.; M.A.L.R.; data analysis, C.M.P.; M.A.L.R., L.C.A.; formal analysis, C.M.P.; M.A.L.R., L.C.A.; investigation, C.M.P.; M.A.L.R., L.C.A.; writing - preparing the original draft, C.M.P.; M.A.L.R., L.C.A.; writing - proofreading and editing, C.M.P.; M.A.L.R., L.C.A.; financing acquisition, L.C.A. All authors read and agreed with the published version of the manuscript.
Acknowledgments:
We thank Acre State Secretariat of Health (SESACRE), Acre - Brazil, the Federal University of Acre (UFAC), Acre - Brazil and the Santo ABC University Center (FMABC) Santo André, São Paulo - Brazil, for the opportunity to develop Masters, Doctors and Researchers training in health, through Agreement 007/2015 - SESACRE/UFAC/FMABC) and all researchers, undergraduate, masters and doctorates students of the Laboratory of Study Design and Scientific Writing of the ABC University Center (FMABC) and thus made it possible to develop research and science in the Western Amazon, Brazil. Pró-Reitoria de Pesquisa e Pós-Graduação da Universidade Federal do Acre (UFAC). Laboratório da Delineamento de Estudo e Escrita Científica do Centro Universitário Saúde ABC, Santo André, São Paulo.
Conflicts of Interest:
Nothing to declare.
REFERENCES
1.Organização Pan-Americana de Saúde. Folha informativa - Sarampo. OPAS. 2019. Disponível em: https://www.paho.org/bra/index.php?option=com_content&view=article&id=5633:folha-informativa-sarampo&Itemid=1060. Acesso em: 13/10/2019. [ Links ]
2.Almeida, DS. Estabelecimento de material de referência para a determinação da potência da vacina sarampo, caxumba e rubéola (atenuada) pelo fabricante nacional (Bio-Manguinhos). 2014. Instituto Nacional de Controle de Qualidade em Saúde, Fundação Oswaldo Cruz, Rio de Janeiro. Dissertação (Mestrado Profissional em Vigilância Sanitária) -, 121 f. Disponível em https://www.arca.fiocruz.br/handle/icict/9904. [ Links ]
3.Quadros CA, Izurieta H, Carrasco P, Brana M, Tambini G. Progress in measles eradication in the Americas region. Infect Dis. 2003. v. 187, p. S102-110. [doi: 10.1086/368032] [ Links ]
4.Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Guia de Vigilância Epidemiológica. Departamento de Vigilância Epidemiológica. [internet]. Coordenação-geral de Desenvolvimento da Epidemiologia em Serviços. 2017. 2ª edição. Brasília. p. 113-128, 2017.4. Disponível: https://bvsms.saude.gov.br/bvs/publicacoes/guia_vigilancia_saude_3ed.pdf [ Links ]
5.Risi JB Jr. Control of Measles in Brazil. Review of Infectious Diseases. 1983. Chicago. v. 5, no. 3. [doi 10.1093/clinids/5.3.583]. [ Links ]
6.Silva LP. Erradicação do sarampo: uma possibilidade real? Revisão crítica da teoria e das estratégias de eliminação. 1993. Dissertação de mestrado da Escola Nacional de Saúde Pública- Rio de Janeiro. 200 p. Disponível: http://bases.bireme.br/cgi-bin/wxislind.exe/iah/online/?IsisScript=iah/iah.xis&src=google&base=LILACS&lang=p&nextAction=lnk&exprSearch=115669&indexSearch=ID. [ Links ]
7.Mello JN.; et al. Panorama atual do sarampo no mundo: Risco de surtos nos grandes eventos no Brasil. J. Bras. Med. 2014 v. 102, n. 1, p. 33-40. [doi http://dx.doi.org/10.5123/S0104-16731997000100002]. [ Links ]
8.Brasil, Ministério Da Saúde. Informe nº 37. 19 DE MARÇO 2019. Situação do Sarampo no Brasil.2018-2019. [internet]. Disponível: https://portalarquivos2.saude.gov.br/images/pdf/2019/marco/19/Informe-Sarampo-n37-19mar19aed.pdf [ Links ]
9.Zorzetto R. As razões da queda na vacinação. Revista Pesquisa Fapesp. 2018. n. 270, p. 19-24. [internet]. Disponível em: https://revistapesquisa.fapesp.br/as-razoes-da-queda-na-vacinacao/. [ Links ]
10.Costa MCN, Mota E, Nascimento EMR. Estudo Epidemiológico do sarampo em Salvador - 1985. Rev. Baiana Saúde pública. 1988v.15, n.1, p.32-46. [ Links ]
11.Lanini S, Capobianchi MR, Pure V, Filia A, Manso Mdel, Karki T, Nicoletti L, Magurano F, Derrough T, Severi E, Bongigli S, Lauria Fn, Ippolito G, Vellucci L, Pompa MG. The Central Task Force For The Meascle Outbreak. Measles outbreak on a cruise ship in the western Mediterranean, February 2014, preliminary report. Eurosurveillance. 2014. v.19, p.1-5. Disponível em https://www.eurosurveillance.org/content/10.2807/1560-7917.ES2014.19.10.20735. [ Links ]
12.Lemos, DRQ. Epidemia de sarampo no Ceará no período pós-eliminação nas Américas: enfrentamento, resposta coordenada e avaliação de risco para reintrodução do vírus. 2014. Dissertação (Doutorado) Programa de Pós-Graduação em Saúde Coletiva do Centro de Ciências da Saúde da Universidade Estadual do Ceará. Fortaleza - Ceará, 204 f. [ Links ]
13.Brasil, Ministério da Saúde. Informe nº 28. 22 DE OUTUBROS DE 2018. Situação do Sarampo no Brasil - 2018. [internet]. Disponível em: https://portalarquivos2.saude.gov.br/images/pdf/2018/outubro/24/informe-sarampo-28-23out18.pdf [ Links ]
14.Sato, APS. Qual a importância da hesitação vacinal na queda das coberturas vacinais no Brasil? Rev Saude Pública. 2018. v 52, p 52-96. [ Links ]
15.Sociedade Brasileira de Medicina Tropical. Movimento antivacina é uma das dez ameaças para a saúde mundial. 11 de abril de 2019. SBMT. [internet] disponível em: https://www.sbmt.org.br/portal/anti-vaccinemovement-is-one-of-the-ten-threats-to-global-health/. Acesso em 23 de outubro de 2019. [ Links ]
16. Silvério SMR, Milagres, BS. Perfil Epidemiológico do Sarampo na Região Norte Brasileira no ano de 2018. Centro Universitário de Brasília- UniCEUB. 2019. Faculdade de Ciências da Educação e Saúde, Curso de Graduação em Biomedicina. Disponível em: https://repositorio.uniceub.br/jspui/handle/prefix/13646 [ Links ]
17.Leite FSLS, Ramalho MIL, Sousa MNA. Evolução do Sarampo no Estado de Roraima e a Atual Situação Vacinal no Brasil. C&D-Revista Eletrônica da FAINOR, 2019. Vitória da Conquista. v.12, n.1, p.129-140. [doi 10.11602/1984-4271.2019.12.1.8] [ Links ]
18.Brasil. Ministério da Saúde. Manual de normas e procedimentos para vacinação. Ministério da Saúde. 2014. Brasília. [internet]. Disponível em: https://bvsms.saude.gov.br/bvs/publicacoes/manual_procedimentos_vacinacao.pdf. [ Links ]
19.Chaves ECR, Trindade JKN, Andrade FFB, Mendonça MHR. Avaliação da cobertura vacinal do sarampo no período de 2013-2019 e sua relação com a reemergência no Brasil. Revista Eletrônica Acervo Saúde. 2020 Vol.Sup., n.38, p. 1-16. [doi https://doi.org/10.25248/reas.e1982.2020] [ Links ]
20.Herrera-Benavente IF, Santos AHM, Rodríguez-Barragán e Comas-García A, Ochoa-Pérez UR. Estado actual del sarampión Comportamiento en Latinoamérica. Revista Latinoamericana de Infectología Pediátrica. 2018. v. 31, n.4, p. 140-148. [ Links ]
21.Brasil, Ministério da Saúde. Secretaria de Vigilância em Saúde. Informe Número Especial. Vigilância em Saúde no Brasil 2003-2019. 2019, v 50, p 66-67. [internet]. Disponível em: https://portalarquivos2.saude.gov.br/images/pdf/2019/setembro/25/boletim-especial-21ago19-web.pdf [ Links ]
22.Brasil, Ministério da Saúde. Informe nº 28. 22 DE OUTUBROS DE 2018. Situação do Sarampo no Brasil - 2018. [internet]. Disponível em https://portalarquivos2.saude.gov.br/images/pdf/2018/outubro/24/informe-sarampo-28-23out18.pdf. [ Links ]
 Correspondence:
Correspondence:
Carolina Miranda Parra
carolinaparrabio@gmail.com
Manuscript received: november 2020
Manuscript accepted: march 2021
Version of record online: january 2022


{kind=link}
{kind=link}
{kind=link}
{kind=link}