










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores
Compartilhar

 Permalink
PermalinkCuadernos de neuropsicología
versão On-line ISSN 0718-4123
Cuad. neuropsicol. vol.6 no.1 Santiago 2012
https://doi.org/10.7714/cnps/6.1.201
ORIGINAL PAPERS
DOI: 10.7714/cnps/6.1.201
Rheumatoid Arthritis - Neuropsychology, Depression and Anxiety. A case - control study -120 Portuguese Female subjects.
Artrite Reumatóide – Neuropsicologia, Depressão e Ansiedade. Estudo de Caso-Controlo – 120 mulheres portuguesas.
Artritis Reumatoide - Neuropsicología, Depresión y Ansiedad. Un estudio de caso – control, con 120 mujeres Portuguesas.
Luis Alberto Coelho Rebelo Maia1
ABSTRACT
Objectives: Impact of Rheumatoid Arthritis in cognitive functions has not been well acknowledged in Portugal. With this original article we intended to elucidate this problem in this specific country. Methods: We measured the results of 60 Rheumatoid Arthritis female patients (study group), comparing every patient in a case control paired plan (years in school and age), with control subjects (n = 60, in a total of 120 subjects). All participants were evaluated with Paced Auditory Selective Attention Test, Word List Generation Test, Luria Nebraska Neuropsychological Battery, a Portuguese depressive screening test (IACLIDE), STAI (anxiety trace and trait test) and the Mini Mental state examination. Results: The outcomes demonstrate, for the first conclusive time in Portuguese patients, the occurrence of main deficits in terms of cognitive functioning (measured by a variety of neuropsychological tests), and depressive and anxiety symptomatology. Conclusion: This article asset the need to pay attention in psychoeducational, psychotherapeutic and cognitive stimulation, and reinforcement of neuropsychological intervention in these types of patients.
Keywords: Neuropsychology, inflammatory / rheumatic diseases; depression, anxiety; Paced Auditory Selective Attention Test, Word List Generation Test, Luria Nebraska Neuropsychological Battery, a Portuguese depressive screening test (IACLIDE), STAI (anxiety trace and trait test) and the Mini Mental state examination; exploratory study.
RESUMO
Objectivos: O impacto da artrite reumatóide nas funções cognitivas não tem sido bem reconhecido em Portugal. Com este artigo original pretendemos elucidar este problema neste país específico. Métodos: Avaliámos os resultados de 60 pacientes femininos com artrite reumatóide (grupo de estudo), comparando cada paciente num estudo de caso-controle, emparelhando os sujeitos com Artrite Reumatóide (60 sujeitos) com 60 pacientes Artrite Reumatóide, nas variáveis anos de escolaridade e idade (a variável género era uma constante = feminino). Todos os participantes foram avaliados com o Teste de Atenção Auditiva Selectiva (PASAT), teste de geração de lista de palavras, Bateria Neuropsicológica de Luria Nebraska, um teste português de despistagem de sintomatologia depressiva (IACLIDE), um teste de rastreamento de traços de ansiedade - STAI) e um teste de exame de Estado Mental. Resultados: Os resultados demonstram, pela primeira vez de forma conclusivo em pacientes portugueses, a ocorrência de défices principais em termos do funcionamento cognitivo (avaliado por uma variedade de testes neuropsicológicos) e semiologia de depressão e ansiedade. Conclusão: Este artigo consolida a necessidade de prestar atenção a uma abordagem psico-educativa, estimulação psicoterapêutica e cognitiva e reforço da intervenção neuropsicológica nestes tipos de pacientes.
Palavras-chaves: Neuropsychology, inflammatory / rheumatic diseases; depression, anxiety; Paced Auditory Selective Attention Test, Word List Generation Test, Luria Nebraska Neuropsychological Battery, a Portuguese depressive screening test (IACLIDE), STAI (anxiety trace and trait test) and the Mini Mental state examination; exploratory study.
RESUMEN
Objetivos: El presente estudio pretende registrar el nivel de impacto en las funciones cognitivas de la Artritis Reumatoide (AR) en una muestra de pacientes portugueses. Métodos: En un estudio de caso-control, se comparan los resultados de 60 pacientes femeninos con artritis reumatoide (grupo de estudio) y un grupo de mujeres de similar edad y escolaridad como grupo control. Todas las participantes fueron evaluadas con pruebas de atención selectiva rítmica auditiva, prueba de generación de lista de palabra, batería neuropsico- lógica de Luria Nebraska, una prueba portuguesa de valoración de síntomas depresivos (IACLIDE), el STAI (prueba valoración de ansiedad) y el Mini Mental Test. Resultados: el resultado de una variada serie de pruebas neuropsicológicas logra entregar evidencia, por primera vez de forma concluyente en pacientes portugueses, sobre los principales déficits en términos de funcionamiento cognitivo y su manifestación, junto con sintomatología depresiva y de ansiedad en pacientes con AR. Conclusión: Este artículo busca llamar la atención, desde una perspectiva psicoeducativa, sobre la importancia de un apoyo activo en la implementación de estimulación cognitiva, intervención psicoterapéutica y refuerzo de la intervención neuropsicológica en pacientes con Artritis Reumatoide.
Palabras claves: Neuropsicologia; artritis reumatoide; depresion; ansiedad; Test auditivo de atención selectiva; batería neuropsicológica Luria Nebraska; Portuguese depressive screening test (IACLIDE).
Introduction
Subsequently to the first unpublished report of Rheumatoid Arthritis (RA), for Landré-Beauvais, in 1800 [1], the information about this illness increased intensely.
Hippocrates named it as gout, and after 1800 RA happening to be seen as a specific etiological unit. In general RA is considered a progressive and disabling auto-immune disease [2], causing strong physical, emotional and financial complications [3]. RA is characterized by inflammation of the lining at the joints, and this can improve long term damage, chronic pain, limitations in daily life activity [4], and familiar and emotional stress [5]. It is estimated that in USA exists around 1 in 108 or 0.92% (2.5 million patients in USA) [6], and nearly ninety seven thousand http://www.wrongdiagnosis.com/travel-health/portugal.htm in Portugal.
With the knowledge brought with time, patients and clinicians started to be conscious with other kind of symptoms that apparently affected RA patients in a very marked way: chronic fatigue [7], psychiatric illnesses [8], with main occurrence of Depression and Anxiety [9-13]. Progressively, a cognitive and neuropsychological deficit pattern in RA has been reported in numerous studies in the latest years of clinical investigation [14, 44, 45].
Methodology
We assessed 120 subjects (60 rheumatoid subjects and 60 control subjects, paired by age more or less 3 years, and years in School, more or less 3 years). The intervention group was collected in different centers (institutions) for specific care in Rheumatic patients, in the Center/Littoral Region of Portugal. Control subjects were selected by statistical convenience method. Subects of Study Group (RA patients) were introduced following the criterias for RA, from Aletaha, Neogi, Silman, Funovits, Felson & Bingham, et al. (2010) [46]. In the control group we only considered subjects without any certified rheumatic disorders.
Statistical data homogeneity where guaranteed with the utilization of Kolgomorov Sminrov and by this, we used parametric statistical methods.
Short description of tests
Paced Auditory Serial Addition Test (PASAT) is a measure of cognitive function, developed by Gronwall in 1977 [15], which expressly assess acoustic information processing swiftness and plasticity, as well as computation ability. The patient as to execute serial summation of numbers (61 items and 60 calculations) that are given in a CD voice support, in a rate of 2 or 3 seconds. The results could vary in a range of 0 to 60. Scores lower than percentile 5, considering normal population for Portuguese normative data is usually considered to be in the compromised range.
The Word List Generation procedure access the ability to produce and access semantic knowledge, through the process of naming words of a particular category or starting with a particular letter [16]. Is expected that the subject could be able to present, as a minimum, 10 items (names of vegetables, animals and words that starts with the letter P). A result indicating less than 10 items in considered very poor, considering Portuguese test adaptation.
Mini Mental State Examination was developed by Folstein et al. [17], as a brief test used to screen cognitive impairment. In the Portuguese version [18], the test as 30 items and the results of this test could range from 0 (severe cognitive deterioration), to 30 (no signal of cognitive deterioration).
Luria Nebraska Neuropsychological Battery (LNNB), allow study and analyze neuropsychological performance of control and patient subjects, both genders, adults (aged 18-65) from different academic levels. The principal neuropsychological functions assessed were Motor Functions, Rhythm Functions, Tactile Functions, Visual Functions, Receptive Speech Functions, Expressive Speech Functions, Writing Functions, Reading Functions, Arithmetic Functions, Memory Functions and Intellectual Processes Functions [19, 20]. The test is composed by more than 740 different items / tasks, with different ways of correction. For each subject (and in each scale) we have to calculate a value ("Critical Value") considering the age and years in school. This Critical Value will serve, individually, to identify if the subject is above or not a T note of normality (results lower than T = 60 represents normality, considering Portuguese test adaptations).
The State-Trait Anxiety Inventory (STAI) was conceptualized as a study instrument to explore anxiety in adults [47, 21]. The test is composed by two scales (trait and state). Each scale is composed by 20 items that should represent the way the subject is feeling in the moment of test administration. Using a 4 points range for each item, the results in the test varies from 20 to 80. Higher results represent higher levels of anxiety in both scales (State and Trait see Portuguese validation in Silva, D. (2003) (48).
IALCIDE Is a test adapted to Portuguese population to assess Depressive Symptoms [22]. The test is composed by 21 items that should represent the way the subject is feeling in the moment of test administration (using a five point range 0-4). Results may vary from 0 to 84. Results lower than 20 represent normality. Then, the level of depression indicators increases as the sum of items provides a higher result. For instance a result of 25 could represent light indication of depression, but a result of 75 represents securely a strong indication of Severe Depression.
Results
In Table I we can see that the mean age for control subjects are 40,94, with a standard deviation of 10,25, and the mean for years in School are 10,89, with a standard deviation of 4,15. Regarding to intervention group (patients), the mean age is 41,03, with a standard deviation of 9,60 and the mean for years in School are 10,10, with a standard deviation of 4,00. None of this differences are statistically significant (Age: t = -1,019; ρ =, 310; Years in school: t = 1,825; ρ =, 081).
In Table II we can see that the mean results in PASAT test for control subjects are 30,62, with a standard deviation of 10,81, and the mean for intervention group is 17,73, with a standard deviation of 8,82, being this difference statistically significant (t = 10,003; ρ = ,021). We also verify that the mean results in WLG for control subjects is 17,71, with a standard deviation of 3,31, and the mean for intervention group is 9,07, with a standard deviation of 3,18, being this difference statistically significant (t = 14,600; ρ = ,034). Finally, in Table II we verify that the mean results in MMSE for control subjects is 28,84, with a standard deviation of 1,50, and the mean for intervention group is 27,89, with a standard deviation of 2,59, being this difference statistically significant (t = 2,398; ρ = ,025).
In Table III we can see that the mean results in STAI (anxiety) test for control subjects are 42,13, with a standard deviation of 6,10, and the mean for intervention group is 57,80, with a standard deviation of 8,79, being this difference statistically significant (df = -11,871;ρ = ,012). Regarding to depressive symptomatology (IACLIDE Test) we can see that the mean results for control subjects were 11,20, with a standard deviation of 11,09, and the mean results for intervention group were 21,02, with a standard deviation of 9,09, being this difference statistically significant (t = -4,915; ρ = ,013).
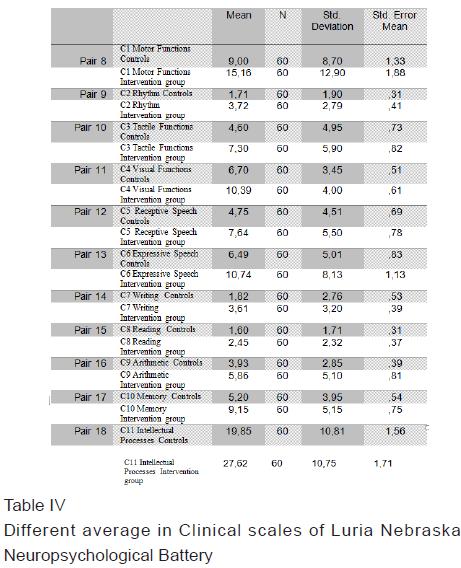
In Table IV we can see the mean results in all Clinical Scales of Luria Nebraska Neuropsychological Battery (LNNB). In the Motor Functions C1 Scale the Control subjects presents a mean punctuation of 9,00 with a standard deviation of 8,70, and the mean for intervention group is 15,16 with a standard deviation of 12,90, being this difference statistically significant (df= -3,212; ρ = ,002).
In Rhythm Functions C2 Scale the Control subjects presents a mean punctuation of 1,71 with a standard deviation of 1,90, and the mean for intervention group is 3,72 with a standard deviation of 2,79, being this difference statistically significant (df = -3,722; ρ = ,011).
In Tactile Functions C3 Scale the Control subjects presents a mean punctuation of 4,60 with a standard deviation of 4,95, and the mean for intervention group is 7,30 with a standard deviation of 5,90, being this difference statistically significant (df= -2,600; ρ = ,012).
In Visual Functions C4 Scale the Control subjects presents a mean punctuation of 6,70 with a standard deviation of 3,45, and the mean for intervention group is 10,39 with a standard deviation of 4,00, being this difference statistically significant (df= -4,520; ρ = ,019). In Receptive Speech Functions C5 Scale, the Control subjects presents a mean punctuation of 4,75 with a standard deviation of 4,51, and the mean for intervention group is 7,64 with a standard deviation of 5,50, being this difference statistically significant (df= -3,043; ρ = ,003).
In Expressive Speech Functions C6 Scale, the control subjects presents a mean punctuation of 6,49 with a standard deviation of 5,01, and the mean for intervention group is 10,74 with a standard deviation of 8,13, being this difference statistically significant (df= -3,692; ρ = ,005).
In Writing Functions C7 Scale the control subjects presents a mean punctuation of 1,82 with a standard deviation of 2,76, and the mean for intervention group is 3,61 with a standard deviation of 3,20, being this difference statistically significant (df = -2,968; ρ = ,023).
In Reading Functions C8 Scale, the control subjects presents a mean punctuation of 1,60 with a standard deviation of 1,71, and the mean for intervention group is 2,45 with a standard deviation of 2,32. This difference is not statistically significant (df = -2,627; ρ = ,087).
In Arithmetic Functions C9 Scale the control subjects presents a mean punctuation of 3,93 with a standard deviation of 2,85, and the mean for intervention group is 5,86 with a standard deviation of 5,10, being this difference statistically significant (df = -2,006; ρ = ,031).
In Memory Functions C10 Scale the control subjects presents a mean punctuation of 5,20 with a standard deviation of 3,95, and the mean for intervention group is 9,15 with a standard deviation of 5,15, being this difference statistically significant (df= -3,842; ρ = ,027).
In Intellectual Processes Functions C11 Scale, the control subjects presents a mean punctuation of 19,85 with a standard deviation of 10,81, and the mean for intervention group is 27,62 with a standard deviation of 10,75, being this difference statistically significant (df = -4,215; ρ = ,022).
Discussion
In this article we intended to evaluate a particular set of subjects with Rheumatoid Arthritis (RA), in a case control study, compared with normative subjects. We corroborated, in this very original Portuguese study that in the preponderance of the assessed constructs, intervention group (RA) presented poorest results than paired control subjects, bearing in mind statistical significance, in the majority of measures of cognitive, depressive and anxiety symptomatology
Due to a paired strategy, we can see that the mean age for control subjects doesn't differ from patient's mean age, as well as for the years in school. This guarantee to us that the verified differences presented in the several test utilized should not be attributed to differences in age, academic level and gender (this last variable was a constant).
Concerning to differences in anxiety and depression, endorsing prior studies, our intervention group presents more incidence of these type of symptomatology, being considered as two concurrent pathologies that produce strong deficits in daily life tasks, as well as in quality of life of RA intervention group (23-38).
Regarding to neuropsychological outcomes, our data are in accordance with numerous studies that shows that RA intervention group presents a strong deficit in attention and executive functions when measured with these types of tests (39, 50, 51).Other researchers reported similar deficits in intervention group with RA on tasks requiring differentiation of similar letter and pattern comparison tests of information processing speed in connection with upper levels of pain and depression (40).
According to previous global studies, in this original study of RA Portuguese clinical group, strong neuropsychological deficits were found. In astudyrealized to describe the incidence of cognitive impairment in patients with RA, 40 patients with RA and 40 healthy controls was assessed, the major inferences was that cognitive impairment was not associated to clinical and treatment types or disability once it appears as an independent deficit (not correlated with the well-known relation among RA, Depression and Anxiety disorders) [41].
Another recent study using the Automated Neuropsychological Assessment Metrics (ANAM) shows that RA patients, when compared with hale and hearty matched controls, presents 61% of RA patients with more deficits in neuropsychological clinical capacities [42].
Conclusion
This study, settles, in a very controlled way, what Portuguese Rheumatologists already know, as reported by official websites of Portuguese Rheumatologists [43]. RA induces strong deficits not only in somatic experiences, emotional and cognitive deficits but also in Neuropsychological reality.
This is part of the firsts Portuguese Studies with RA patients demonstrating strong deficits in Neuropsychological dimensions of daily life [44, 45, 46], (as well as the already known relation with depressive and anxiety constructs), namely poorest speed in solution problems, daily locomotion, pain related deficits, inattention, depression, forgetfulness, tiredness, etc.
Consequently, this article assets the need to pay attention in psychoeducational, psychotherapeutic and cognitive stimulation as well as neuropsychological intervention in these types of patients.
Acknowledgements and Conflicts of Interest
The author is grateful to the participants and reports no potential conflicts of interest.
References
[1]. Kaiser, H. (2004). Landré-Beauvais (1772-1840) The actual first description of rheumatoid arthritis. Zeitschrift für Rheumatologie. 63(5, October), 430-435. [ Links ]
[2]. National Rheumatoid Arthritis Society (2011). (Available from: http://www.gencat.net/ics/professionals/protocols/nanda. [ Links ]pdf).
[3]. Markenson, J.A. (1991). Worldwide trends in the socioeconomic impact and long-term prognosis of rheumatoid arthritis. Seminars in Arthritis and Rheumatism. 21, [ Links ] 4-12.
[4]. Arthritis Analysis (http://www.arthritisanalysis.com/category/symptoms/last (available from) 8 March 2008). [ Links ]
[5]. Lam, M., Lehman, A.J., Puterman, E. & DeLongis, A. (2009). Spouse depression and disease course among persons with rheumatoid arthritis. Arthritis Care Research. 61(8, August), 1011-1017. [ Links ]
[6]. Statistics by Country for RA. (2011). (http://www.wrongdiagnosis.com/r/rheumatoid_arthritis/stats-country.htm/last acessed 15 January 2011). [ Links ]
[7]. Stebbings, S., Herbison, P., Doyle, T.C.H, Treharne, G.J & Highton, J. (2010). A comparison of fatigue correlates in rheumatoid arthritis and osteoarthritis: disparity in associations with disability, anxiety and sleep disturbance. British Journal of Rheumatology. 49(2), 361-367. [ Links ]
[8]. Lisitsyna, T.A., Veltishchev, D.U., Seravina, O.F., Kovalevskaya, O.B., Zeltyn, A.E., Fofanova,, Y.S,. & Nasonov, E.L. (2009). Prevalence of Psychiatric Disorders in Rheumatoid Arthritis Patients. Presentation OP-0227, EULAR 2009, Copenhagen, 2009 June 12. [ Links ]
[9]. Dirik, G. & Karanci, A.N. (2010). Psychological distress in rheumatoid arthritis patients: an evaluation within the conservation of resources theory. Psychology & Health. 25(5, June). 617-632. [ Links ]
[10]. El-Miedany, Y. (2002). Is anxiety a more common disorder than depression in rheumatoid arthritis? Joint Bone Spine. 69(3), 300-306. [ Links ]
[11]. Kojima, M., Kojima, T., Suzuki, S., Oguchi, T., Oba, M., Tsuchiya, H., Sugiura, F., Kanayama, Y., Furukawa, T.A., Tokudome, S. & Ishiguro, N. (2009). Depression, inflammation, and pain in patients with rheumatoid arthritis. Arthritis Care & Research. 61(8), 1018-1024. [ Links ]
[12]. Parker, J.C. & Wright, G.E. (1995). The implications of depression for pain and disability in rheumatoid arthritis. Arthritis & Rheumatism. 8, 279–283.
[13]. VanDyke, M.M., Parker, J.C., Smarr, K.L., Hewett, J.E., Johnson, G.E., Slaughter, J.R. & Walker, S.E Anxiety in rheumatoid arthritis. Arthritis and Rheumatism. 51;(15 June) 2004: 408-412. [ Links ]
[14]. Appenzeller, S., Bertolo, M.B. & Costallat, L.T. Cognitive impairment in rheumatoid arthritis. Methods and Findings in Experimental and Clinical Pharmacology. 26;(5) 2004: 339-343 [ Links ]
[15]. Gronwall, D.M.A. Paced auditory serial-addition task: A measure of recovery from concussion. Perceptual and Motor Skills. 44; 1977: 367-373. [ Links ]
[16]. Ravdin L.D., Katzen, H.L., Agrawal, P. & Relkin, NR Verbal fluency in mildly depressed older adults: Comparisons between letter and semantic word list generation and age-stratified normative data, The Clinical Neuropsychologist. 17;(2) 2003: 195-202. [ Links ]
[17]. Folstein, M.F., Folstein, S.E. & Mchugh, P.R. Mini-Mental State: a practical method for grading the cognitive state of patients for the clinician. Journal of Psychiatry Research. 12; 1975: 189-198. [ Links ]
[18]. Guerreiro, M., Silva, A.P. & Botelho, M.A. Adaptação à população portuguesa na tradução do "Mini Mental State Examination" (MMSE). Revista Portuguesa de Neurologia. 1; 1994:9-10. [ Links ]
[19]. Golden, C.J., Hammeke, T.A. & Purisch, A.D. Manual for the Luria-Nebraska Neuropsychological Battery: Forms I and II. Los Angeles, Western Psychological Services. [ Links ] 1985.
[20]. Maia, L.A., Loureiro, M.J., Silva, C.F., Vaz-Patto, M.A., Loureiro, M., Correia, C., et al. Bateria de Avaliação Neuropsicológica de Luria Nebraska - A sua introdução em Portugal - Descrição do Instrumento e dois estudos de caso. Psiquiatria Clínica. 24;(2) 2003: 91-106. [ Links ]
[21]. Spielberger, C.D., Gorsuch, R.L. & Lushene. R.E. Manual for the State-Trait Anxiety Inventory. Palo Alto, CA: Consulting Psychologists Press. 1970. [ Links ]
[22]. Serra, Adriano Vaz. Iaclide. Inventário de Avaliação Clínica da Depressão. Provas Psicológicas em Portugal. Braga, Apport. 1995: 181-191. [ Links ]
(23). Abdel-Nasser, A.M., Abd El-Azim, S., Taal, E., El-Badawy, S.A., Rasker, J.J. & Valkenburg, H.A. Depression and depressive symptoms in rheumatoid arthritis patients: an analysis of their occurrence and determinants. British Journal of Rheumatology. 37; 1998: 391-397. [ Links ]
[24]. Bartolini, M., Candela, M., Brugni, M., Catena, L., Mari, F., Pomponio G, et al. Are behavior and motor performances of rheumatoid arthritis patients influenced by subclinical cognitive impairments? A clinical and neuroimaging study. Clinical and Experimental Rheumatology. 20; 2002: 491-497. [ Links ]
[25]. Belza, B.L. Comparison of self-reported fatigue in rheumatoid arthritis and controls. Journal of Rheumatology. 22; 1995: 639-643. [ Links ]
[26]. Brown, S.C., Glass, J.M. & Park, D.C. The relationship of pain and depression to cognitive function in rheumatoid arthritis patients. Pain. 96; 2002: 279–284.
[27]. Dicckens, C., McGowan, L., Clark-Carter, D. & Creed, F. Depression in rheumatoid arthritis: a systematic review of the literature with meta-analysis. Psychosomatic Medicine. 64; 2002: 52-60. [ Links ]
[28] Dick, B., Eccleston, C. & Crombez, G. Attentional functioning in fibromyalgia, rheumatoid arthritis and musculoskeletal pain patients. Arthritis Rheumatoid. 47; 2002: 639-644. [ Links ]
[29]. Dickens, C. & Creed, F. The burden of depression in patients with rheumatoid arthritis. Rheumatology. 40; 2001: 1327-1330. [ Links ]
[30]. Hawley, D.J. & Wolfe, F. Anxiety and depression in patients with RA: a prospective study of 400 patients. Journal of Rheumatology. 15; 1998: 932–941.
[31]. Isik, A., Koca, S.S., Ozturk, A. & Mermi, O. Anxiety and depression in patients with rheumatoid arthritis. Clinical Rheumatology. 26;(6) 2007: 872-878. [ Links ]
[32]. Botequio Mella, L.F., Bértolo, M.B. & Dalgalarrondo, P. Depressive symptoms in rheumatoid arthritis patients . Revista Brasileira de Psiquiatria. 32;(3, Sept.) 2010: 257-263. [ Links ]
[33]. Park, D.C., Glass, J.M., Minear, M. & Crofford, L.J. Cognitive function in fibromyalgia patients. Arthritis Rheumatoid. 44; 2001: 2125-2133. [ Links ]
[34]. Pincus, T., Griffith, J., Pearce, S. & Insberg, D. Prevalence of self- reported depression in patients with rheumatoid arthritis. British Journal of Rheumatology. 35; 1996: 879-883. [ Links ]
[35]. Söderlin, M.K., Hakala, M.eminen, P. Anxiety and depression in a community-based rheumatoid arthritis population. Scandinavian Journal of Rheumatology. 29;(3) 2000: 177-183. [ Links ]
[36]. Stoltz, C.M., Baime, M.J. & Yaffe, K. Depression in the patient with rheumatologic disease. Rheumathic Disease Clinic of North America. 25; 1999: 687-702. [ Links ]
[37]. VanDyke, M.M., Parker, J.C., Smarr, K.L., Hewett, J.E., Johnson, G.E., Slaughter, J.R. & Walker, S.E. Anxiety in rheumatoid arthritis. Arthritis and Rheumatism. 51;(3) 2004: 408-412. [ Links ]
[38]. Velasquez, X., Pizarro, C., Pizarro, P. & Massardo, L. La depresión en artritis reumatoídea. Reumatología 18;(2) 2002: 49-52. [ Links ]
[39]. Dick, B., Eccleston, C. & Crombez, G. Attentional functioning in fibromyalgia, rheumatoid arthritis, and musculoskeletal pain patients. Arthritis Care & Research. 47; 2002: 639–644.
[40]. Brown, S.C., Glass, J.M. & Park, D.C. The relationship of pain and depression to cognitive function in rheumatoid arthritis patients. Pain. 96; 2002: 279–284.
[41]. Appenzeller, S., Bertolo, M.B. & Costallat, L.T. Cognitive impairment in rheumatoid arthritis. Methods Find Exp Clin Pharmacol. 26;(5) 2004: 339. [ Links ]
[42]. Hanly, J.G., Omisade, A., Su, L., Farewell, V. & Fisk, J.D. Assessment of cognitive function in systemic lupus erythematosus, rheumatoid arthritis, and multiple sclerosis by computerized neuropsychological tests. Arthritis and Rheumatism. 62;(5, May) 2010: 1478-1486. [ Links ]
[43].Instituto Português de Reumatologia (2010) Artrite reumatóide – Números. http://www.pdr.pt/Noticias/Mais-de-metade-das-pessoas-com-artrite-reumatoide-sofrem-de-depressao.aspx, available at March, 17th, 2011.
[44] Hanly, J.G. & Fisk, J.D. (2011). Connective tissue diseases: Diagnosis of cognitive impairment in adult and pediatric SLE. Nature Reviews Rheumatology. 7(October), 564-565. [ Links ]
[45] Shin, S.Y., Katz, P. P., Wallhagen, M.I. & Julian, L.J. (2011). Cognitive Impairment in Persons with Rheumatoid Arthritis. Arthritis & Rheumatism, Volume 63, November 2011 Abstract Supplement. Abstracts of the American College of Rheumatology/Association of Rheumatology Health Professionals. Annual Scientific Meeting Chicago, Illinois November 4-9. [ Links ]
[46] Aletaha, D., Neogi, T., Silman, A.J., Funovits, J., Felson, D.T. & Bingham, C.O. Rheumatoid Arthritis Classification Criteria. An American College of Rheumatology/European League Against Rheumatism Collaborative Initiative. Arthritis & Rheumatism. 62(9, September) 2569–2581.
[47] Silva, D. (2003). O inventário de Estado-Traço de Ansiedade (STAI). Avaliação Psicológica: Instrumentos validados para a população portuguesa. Ed M Gonçalves. M Simões, L Almeida, C Machado. Quarteto Editora. Coimbra 2003. [ Links ]
[48] Silva, D. (2003). O inventário de Estado-Traço de Ansiedade (STAI). Avaliação Psicológica: Instrumentos validados para a população portuguesa. Ed M Gonçalves. M Simões, L Almeida, C Machado. Quarteto Editora. Coimbra 2003.
[49] Mulligan, K., Newman, SP., Taal, E., Hazes, M., Rasker, J.J. & OMERACT 7 Special Interest Group. (2005). The design and evaluation of psychoeducational/self-management interventions. The Journal of Rheumatology. 32(12, December), 2470-2474. [ Links ]
[50] Appenzeller, S., Bertolo, M.B. & Costallat, L.T. (2004). Cognitive impairment in rheumatoid arthritis. Methods Findings in Experimental Clinical Pharmacology. 26(5, June), 339-343. [ Links ]
[51] Hanly, J,G,, Omisade, A. & Su L. (2010). Cognitive function in systemic lupus erythematosus, rheumatoid arthritis and multiple sclerosis assessed by computerized neuropsychological tests. Arthritis Rheumathoid. Available in http://www.nhiondemand.com/hsjarticle.aspx?id=767, 08, January, 2011. [ Links ]
[52] Plasqui, G. (2007). The role of physical activity in rheumatoid arthritis. Physiology & Behavior. 2(23, May), 270 - 275. [ Links ]
[53] Oku, E.A., Pinheiro, G.R.C. & Araújo, PMP. (2009). Hand functional assessment in patients with rheumatoid arthritis. Revista Fisioterapia em Movimento Curitiba. 22, (2, April/June), 221-228. [ Links ]
[54] Katz, P.P. & Yelin, E.H. (Life activities of persons with rheumatoid arthritis with and without depressive symptoms. Arthritis & Rheumatism. 7(2, June), 69 – 77.
1 Auxiliar Professor of Neuropsychology and Clinical & Assessment approaches at Psychology & Education Department, Beira Interior University, Covilhã, Portugal. lmaia@ubi.pt
