










Serviços Personalizados
Journal

artigo
 Português (pdf)
Português (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores
Compartilhar

 Permalink
PermalinkPsicologia: teoria e prática
versão impressa ISSN 1516-3687
Psicol. teor. prat. v.9 n.1 São Paulo jun. 2007
CONFERÊNCIA
Conference on Neuroscience Lectured the Cognitive Neurosciences Institute of London, May of 2007
Miguel Angel Alvarez González
School of Psychology of Havana University, Cuba
Neurocognition Laboratory, Ins titute of Neurology
Dear colleagues,
I have been granted the honour, probably not worthy of it, to give this conference in the Cognitive Neuroscience Institute, thank you to the invitation as a visiting fellow at the British Society of Psychology. I will, therefore, try to live up to their expectations and take this opportunity to share with you the search for a pressing problem which affects the quality of life in children and elders.
My scientific interests have evolved from psychoneuroendocrine research in the eighties, up to the present time where I am focused on the link between basic research in neuroscience and its applications to the welfare of the community.
When I was young, even though the issues were apparently challenging, it was fun to adjust equations which could describe the relationships between hormones and psychological processes because I could control the variables. To obtain original results and publish them in top rank journals was a controllable task. Now I will present you three research problems as models for discussion.
The massive cognitive screening for children in some countries in Latin America, a privilege given to me as consultant for the Pan Am Health Organization.
The work of my small laboratory in the national program for prevention of mental retardation by early diagnosis of congenital hypothyroidism, and finally screening of early markers of initial stages of dementia en elderly people.
In these three fields I have felt the overwhelming responsibility to dictate accurate criteria that could have direct social implications. The greatest limitation in fulfilling my social role lies in the lack of cognitive diagnostic tools to help diagnose and act, prompt-ly and efficiently. These missing tools will be the core of this presentation. It is easy to understand that I am trying to recruit young scientists.
Scientific problems have different levels of complexity. The human genome or the global warming are good examples of problems which are characterized by the highest level of complexity. On the opposite end we find the trivial or low complexity problems such as a good number of graduate theses. The first ones require great scientific group or institutional efforts and the need of significant financial resources. They are general-ly managed or conducted by great personalities of the science. While the latter depend mostly on personal effort and small amounts of money
Nevertheless, medium complexity problems are limited in time, aimed to well defined questions and carried out by researchers in their top efficiency level such as PhD projects. If these projects are well designed, their results add up and are able to push science forward to critical points producing significant changes in the known paradigms of science.
The medium complexity level problem which is the topic of our discussion today, has to do with how to apply the knowledge we have acquired about the brain function through mass intervention diagnosis of cognitive disorders at the community level. In other words, it is about outside the boundaries of clinical or laboratory research. Let us analyse this phenomena regarding the work of international and government agencies. Their community projects for sustainable development such as drinkable water, fight against pollution, health promotion campaigns and general or specific health preven-tion campaigns.
However, rarely do health or government or NGO’s policies, take into account the progress which have been made by the neurosciences in general and the knowledge attained by psychology regarding the brain function. This gap between public policies and the academic world dismisses the mutual benefits that could be found, if both established a productive communication between these two areas (ALVAREZ; SAFOR-CADA, 2006; JENKINS, 2003; SAFORCADA, 1999).
Perhaps the cause of this gap is the lack of resolved medium complexity level prob-lems, hich would help stimulate mental health and quality of life.
The partial solution to this problem would enable us to:
• Diagnose early stages of cognitive disorders potentially disabling or negatively affecting quality of life.
• Prevent the onset of the disorders or be able to act upon them at an early stage.
• To monitor the effect on the brain of intervention campaigns.
At the community level one should apply almost all our efforts and resources to two target groups; early childhood and elderly subjects. This problem has two aspects to be taken into account. One, the direct social benefit gained and the other the scientific research.
Direct social benefit is very easily explained because these two groups are the most vulnerable in the function of the nervous system. This vulnerability occurs because neurodevelopment and neurodegeneration are both processes that can be altered very easily and also because humans at those stages in life are dependant to a great extent of outside helpers.
Neurodevelopment is the result of a multifactoral process which arises and expresses itself in human interaction with the environment, being intrauterus life, childhood and puberty the most important vital cycles. It is calculated that probably almost a 19% of children are at risk of having at least one aspect of neurodevelopment potentially com-promised. Diseases of the intellect and neurodevelopment can manifest itself ranging from catastrophic forms such as the acute mentally retarded to the sub clinical cognitive deficiencies. One should keep in mind that these developments are not something that will always achieve its maximum result spontaneously. The great potential we find in intelligence and learning in children and adolescents is a very fragile resource that should be protected, cultivated and helped to develop in as much as we should assign the greatest value to this raw material, the human component of a country.
1. The most frequent risk factors, which compromise cerebral development in early life stages, are:
a) Genetic vulnerabilities and exceedingly pernicious intrauterine influences. b) Adverse neo and peri natal circumstances. c) How the child adapts and certain char-acteristics of his character (temperament). d) Inadequate parental care and family problems. e) Inappropriate social context and the type of stability found in the community. f) Inadequate nutrition. g) Infectious or chronic diseases. h) Low sen-sory or affective stimulation.
The increase of life population expectancy increases the probability that focal cerebral deficits or neurodegenerative alterations occur. Therefore the number of none diagnosed persons with primary cognitive deficiencies increases every day.
Regardless of these unavoidable factors, an early active detection in the community or group – elderly people will enable the possibility to take actions on the type of treat-ment and family education necessary before this pathological conditions compromise the normal personal, family and social group functions.
Risk factors of cognitive deterioration in this target group are:
a) Genetic vulnerabilities. b) Social isolation. c) Inter recurrent health problems compromising the nervous system and a non-diagnosed malnutrition.
However we can still find another advantage for science studying these extreme groups, and that is a methodological one. As long as the genesis or the deterioration of a cognitive process is being studied, we will obtain information not only of the structure in its self but also have an evolutionary perspective. Somehow they are models that help us deduce or understand the essential properties.
In spite of the importance these problems have for psychology, it is easy to find a place to apply and execute projects like that. However, when opportunities arise to develop these projects, we face big instrumental and theoretical limitations that make it difficult for us to approach and deter the social impact that would justify the invested resources.
Barriers or obstacles that hinder the assimilation of cognitive Neuroscience (applied) social practice
These failures originate at least from three obstacles that make hard to link the basic neurosciences with community actions. These obstacles are of a cultural, methodologi-cal and neurobiological nature.
I will try to explain these aspects by listing the difficulties we have encountered in the last few years while trying to implement specific projects.
1. The neurobiological obstacle is related to the lack of correspondence between diagnostic procedures and its molecular and neural basis.
2. The methodological barrier stands for the lack of mass evaluation procedures with high specificity and sensibility.
3. The cultural refers, up to a great extent, to the use of procedures of evaluation that are applied out of the cultural context where they were conceived.
Lack of correspondence between Psychological tests and the Neurobiological Foundation
This is a small summary of the scopes that have been screened in mass Latin American studies.
Table 1. Brief summary of the scopes that have been screened in mass Latin American studies
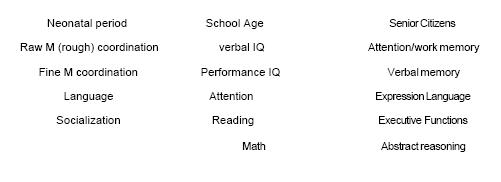
The tests used were the WPPSI, WISC, Gesell, Bayley and Brunet Lezine scales well as computerized scales for dyslexia and dyscalculia, Weschler memory scale, WSCT, CPT and Raven progressive matrixes.
One should ask oneself if these scales were used because they were the ones at hand for clinical use and extrapolated for mass screening. How can we be sure that the choice of these test are not influenced by existing commercial procedures that allow normative criteria and credibility to the peer reviewers?
The majority of tests or psychological procedures used at the present moment belong to the period before neuroimages existed; therefore they were designed without taking into account the brain areas that contribute to the hypothetical neural basis of the eval-uating processes. In other words, they were constructed based on introspective or empir-ical models and ad hoc we have tried to infer their material basis (substrates).
Therefore, sensitivity and specificity are low in these procedures with regards to the brain’s functional topography.
Is in this branch of the neurosciences – where we definitely find an important gap between – basic and applied knowledge. Neurodevelopment evaluation of children’s intellect has made little progress since the works of Gesell, Brunet-Lezine, Terman, Weschler and other scientists. The vital need for empirical evaluations produced tests, which as a result of their use, became essential when results had to be published.
Generally the so called neurodevelopment tests have a great number of rough or fine psychomotricity indicators but very few regarding specific cognitive aspects. This could indicates that one is measuring totally different domains and as such with a very low predictive value.
Conclusion
We do not have at our disposal reliable and predictive mental mass evaluation instruments for the first two years of life. They are focused on psychomotricity. Does it mean that we do not think during the first year of life, but mainly move?
But one thing is true, how much more could we improve our neurodevelopment evaluation if we were capable of a design criterion applicable to field work evaluations, for example, which could explore short term memory? Would we really find a solution for the problem if we only added cognitive mental items to the neurodevelopment tests? The answer is not straightforward.
In 2004, I worked as a PHO/WHO consultant in Tarija, a Bolivian region. Children under the age of two were given a nutritional supplement which included Iron, Zinc and Folic Acid. Researchers wanted to evaluate the impact this nutritional supplement had on the neurodevelopment of these children. On the other hand, my task was to organize a training workshop for psychologists and teachers in neurodevelopment conventional evaluation techniques such as Bayley and Brunet-Lezine. Afterwards, we would evaluate pre and post treatment results in order to measure the impact of the nutritional spark. The workshop attendees unanimously expressed that based on their experience with severe anaemic children (less the 8) – never seen in the UK or in my country – the effects of an effective treatment was easily seen as it produced a flourishing of the social emo-tional response. Language and psychomotricity were expressed much later. Therefore, the tests we had were not capable of measuring the most important psychobiological change that occurred. So we needed to design instruments which could explore matu-ration responses and also be able to take into account memory and emotional aspects in nursing babies (PANDYA; YETERIAN, 2001).
A parallel problem arose when we started to discuss if the ethnic group we wanted to evaluate, the Aymaras, expressed their emotions not in the same way as the culture we the consultants came from. Perhaps we were strangers that tried to impose our own criteria.
Then we realized that we did not have suitable instruments based on neurobiologi-cal data so as to allow us to check the anaemia response hypothesis. Fortunately, we were able to come up with the best possible social scientific solution. The workshop attendees started the worked on the design of scales which, in their opinion, best cap- tured the changes. This task is still inconclusive. Based on this experience, at present we are working with the Madrid’s Autonomous University in a psychobiological study – identifying short memory items in nursing babies and differentiating their emotions through their face expressions.
In regards to IQ evaluation of school age children, the best we are able to do is to use tests from other cultural contexts adapted and with norms for the country one works in. However in all cases, these instruments are variations of procedures which were created in another time when the brain was seen as a black box and therefore does not reflect its neural maturation expressions, just simply items which have been validated by prac-tice. Therefore they have low sensitivity and specificity regarding brain functions.
At present, with the development of cognitive neurosciences, automated methods are been developed which let us explore with a high level of sensitivity and specificity, cog-nitive processes related to reading or arithmetic calculation, just to mention the two most directly related to academic performance in school age children.
Let us analyze a specific situation. We have in Cuba a nationwide thyroid screening program for the early detection of congenital hypothyroidism (ALVAREZ; GÓMEZ; GONZÁLEZ; YERO; MARTÍNEZ; GESÉN; TORRES; FUMERO, 2004; ALVAREZ; CARVAJAL; RENÓN; PÉREZ; OLIVARES; RODRÍGUEZ; ALVAREZ, 2004). As we all know, mental retardation due to cretinism is prevented in children with congenital hypothyroidism, when they are treated early on and this assures them a normal life. We do a neurocognitive follow up for each child with CH from their first month of life until they are 15 years old. Nevertheless, the cerebellum is particularly sensitive to thyroid hormone deficits in the critical periods of development, so one can expect the presence of subtle cognitive deficits related to these brain areas. We assess them since school age with a computerized battery for exploring attention and other cognitive domains at risk. One of the modules of this battery is aimed to subtle cerebellar deficits. It tries to evaluate the stages of cognitive processes development where the cerebellum and frontal regions are involved. We used the so call tunnel effect, described by Gestalt, at the beginning of the 20th century. After having demonstrated that this test had good discriminative power between children with cere-bellar problems and healthy ones, we included it as a current measure for efficacy or early treatment.
So now based on these examples we are facing a conflict: due to the increasing specificity needed to detect specific disabilities in field evaluations, should we develop spe-cific tests which are able to grasp the neurobiological expression of the disorder, but at the same time have little ecological value in other contexts?
Let us observe the extreme group, the elderly.
On the elderly other type of problems arise:
a) Not well defined variables in relation to diagnosis, nutrition, previous health factors, life style and educational, occupational and sociocultural opportunities.
b) Differentiation between the normal aging in the cognitive process and those associated to diseases such as Alzheimer Disease, vascular brain ictus and any other condi-tions potentially aggressive to the brain. For example, subclinical hypothyroidism may mimic depression in elderly people.
Classical neuropsychology is efficient in the diagnosis of brain problem. However, an examination using the Luria method takes at least an hour and, on the other hand, a simple screening test as the Folstein’s MMES is so simple that it almost gives no information. What could be done in the communities? We need simple and strong cognitive predictors of neurodegeneration.
At present an emerging goal is the search for early predictor instruments of demen-tia due to the ageing of the population. In this field, the need to combine cognitive measures with neural and molecular ones is capital, because this is a problem that over-whelms psychology as a discipline. Then we face a problem, we have not practical tools for assessing the decay of a particular brain area when it is getting older, but we do have strong biological markers of this process. We are close to combining these data.
We encounter this problem in a longitudinal study we are carrying out between the University of Havana and Madrid’s Autonomous University in relation to early on set dementia markers in people over 65 years old with mild cognitive impairment (early stage of dementia). Subjects are selected from the community and are assessed in three do-mains: cognition, neuroimaging and molecular profile. We hope then that as soon the study is finished, changes in the cognitive variables will parallel molecular and neural changes in the brain. If this hypothesis is true, we will have some hard cognitive indica-tors. Currently, we are at the programming stage for a specific test battery, which will measure verbal and figural memory.
But the blood brain barrier imposes to neurobiochemestry a severe limitation when trying to determine substances related to the brain function. Molecular blood concen-trations, which potentially inhibit or stimulate cognitive processes, are not easily detected in the brain. Recently some non invasive techniques such as the enzyme activity, as marker of brain damage indicator. Among the enzymes studied are SOD and GT, Neuronal spe-cific enolase and S100 B protein. With the neurological imagines we have included the use of optic coherence tomography that shows spectacularly the optic nerve’s state as a direct indicator of neurological degeneration.
The conclusion of this study is that for practical and pressing needs at community work level, we still must parallel behavioral, molecular and images because we do not have simple indexes of prediction of damage.
Can functional neuroimages solve this problem ?
• Little conceptual agreement about the meaning of the cognitive tasks and the neural modules activated by them. This is an epistemological problem.
• Diversity of interpretations is a methodological problem.
• And the subtractive method itself (passive period compared with the active task is a theoretical and conceptual problem).
• Without a mind model we have the same risk rich people had with a XVI century curiosity cabinet; collecting and showing objects without grasping the theoretical psychobiological links among them.
We are behind the schedule of the big neuroscience, even though we have good technology. In the fabric of knowledge we are mending the results from of psychology and biology but the sewing is not precise and the boundaries are rough and imprecise. (ALVAREZ; TRAPAGA, 2005)
Maybe the problem lies in that we do not posses a mind model that satisfies our cur-rent knowledge of brain function. Our psychological construct does not correspond satis-factorily with the areas of the brain.
Massive screening problem
Available cognitive evaluation procedures originate from two mayor sources: clinical and experimental neuropsychology. Even though the approach is different in its purpose and logistic, both have something in common as to what has to be done, in a given peri-od of time with the individual subject, as determined by the researcher or the clinical psychologist.
Every individual psychometric evaluation is a small experimental situation and presumes that the evaluator is a specialist that has a deep basic understanding, which ena-bles him to find the way between the procedures’ standardization and the individual relationship that arises with the evaluee. On the other hand, the period of evaluation does not seem to raise any problem, as it is expected that the evaluation should not be limited by narrow margins of time, which could influence the quality of the results.
Therefore, clinical or scientific evaluators are highly qualified experts in their area and their role is not to be used as a group exposed to great time pressure, but as some-one who can show its expertise when giving a diagnosis.
Massive community or risk group evaluations should be done in short periods of time. Therefore, when evaluating brain functions in communities or population groups, the problems encountered cannot be solved by traditional methods used by clinical neuropsychology, because using clinical individual neuropsychology would raise the cost significantly and because they are designed to evaluate gross clinical neurocognitive problems and not subtle changes in cognitive or maturation aspects.
Therefore, procedures used in evaluation should meet the following requirements: a) Fast application, b) Ease to interpret, c) Be reliable and valid.
This can be accomplished by the use of computerized tests by trained local personnel for the evaluation.
Computerized tests are a good alternative, if they respond to the conceptual and cor-rect methodological requirements such as:
• 1. Design of user-friendly software that expresses in a suitable way the theoretical and technical cognitive function. 2. Should meet reliable chronometric criteria. 3. Up to a degree, can be administered simultaneously to a group of subjects. 4. Not sub-ject to variations as a result of using different evaluators or the same one over time. 5. Data gathering should be done by trained personnel. 6. Evaluation should be precise and immediate. 7. Results should be processed immediately.
This refers to the possibility of transferring some of the evaluation’s responsibilities to lay members of the community. This aspect is of the utmost importance. Community interventions by definition handle a great quantity of data and evaluations, which are impossible to be manage by the primary level specialized personnel. If low sensitivity and specificity procedures are carried out at the beginning, to initially sort out presumed cases, this task can be done satisfactorily by lay trained community members.
Cultural frontiers
Cultural frontiers are probably the biggest methodological challenge much more than the former two mentioned before.
Community related intervention evaluation is never done in a cultural vacuum. To prevent deceases and promote good health education requires that we work focus on with trying to change subjective believes, values and habits of certain specific behaviors related to the health process. These changes must come about within the sociocultural context. That is why it is so important how the community perceives the evaluation pro-cedures and its effects and they have adapted ecologically to their context. Therefore, diagnostic interventions are inoperable and insufficient if they do not take into account the most appropriate theoretical approach to health psychology, within the cultural framework of the community.
Evaluation-intervention projects are made inside urban scientific institutions, and frequently, those procedures presuppose that the people who are to be evaluated share their same conditions, habits and have a similar culture as the researchers. If the work is to be done in a rural setting, or even a marginal urban one, our research will be influ-enced by sub cultural factors (in the anthropological sense) and invalidate the evalua-tion or give us information that will be impossible to interpret correctly.
The cultural influence can be analyzed from two different perspectives: relationship between evaluator-evaluee and as a response modulator of the evaluee’s answer. Let us see some examples of these two influences.
1. Relationship evaluator-evaluee
The majority of psychometric tests assume that tested subjects respond to the occidental \ totally inadequate to them. In some contexts this high competitive attitude could be an expression of bad manners, so the subject could even delay his answers so as not to seem rude to the evaluator, even though he knows that it is an incorrect answer.
Let me show you an example of what is a myth regarding the best possible scenario for an evaluation.
A psychologist from the Andean “altiplano” region tried to evaluate oculomotricity and attention to children who lived in regions with endemic goiter, which had been given an iodine salt supplement. The psychologist, who lived in the city, picked a version of Porteus labyrinths. This test consists of a labyrinth drawing through which a mouse must find a piece of cheese at the other end. All the children that had been given the test got cero or near cero points in their evaluation before and after having taken the iodized salt.
All the village children obtained results which were in the lowest rank, as if the whole population had a severe mental handicap coordinating their movements.
He was so surprised with the results that he consulted with a rural schoolteacher of the same region. This man explained to him that the analogous idea of a mouse search-ing for food in this particular cultural setting was inadmissible because the children did not want to assume the mouse as a symbolic role. The mouse was a much-hated animal as it ate the community grain reserves. But as their shyness before a stranger could not permit them, based on their Aymara cultural values, to be impolite they would never say no to the test. The results were not good. The problem was solved by changing the mouse and cheese for a “llama” and pasture. Results then showed as expected, normal curves with a mean value placed towards the right, after having taken the iodine salt supplement.
2. Culture as the evaluee’s modulated response
History repeats… By the late XIX century and the beginnings of the XX, interest for trans cultural cognitive studies increased. Positivism’s influence in psychology probably was responsible for this.
Many research studies were carried out on the influence of “culture in the mind”, within a trans cultural framework. Their aim was to find out how cultural variables influ-enced basic psychological functions such as perception or sensation, which, up to that time were considered “universal” and potentially reducible as physiological substrates.
Cole (1999), in his great book Psicología cultural [Cultural psychology], referrers to one of the first studies ever done, in 1895, about the relationship between perceptive processes and culture. This took place during an expedition to the southeast coast of what was known then as British New Guinea on the islands on the Torres Strait. The expert on experimental psychological methods was W. H. Rivers who wanted to examine the veracity about the statement “savages and semi civilized races manifest a superior grade of acuteness in their senses as opposed to the ones found in Europeans ”
One of the most relevant results found by Rivers was in an experiment to evaluate visual acuteness of a group of inhabitants from the Torres Strait, most of them fisher-men. The results indicated that the subjects understood what was asked of them; their precision decreased regularly the same way the targets became smaller or the distance from the target increased. (Their visual acuteness was 2.1:1.)
To control the influence that their main activity, fishing in The Torres’s Strait, could have on the results, the experiment was repeated with fishermen from an island in the North Sea. The valid sample was taken from the Isle of Heligoland (off the coast of Ger-many). Visual acuteness found in the European subjects was 1.77:1. It was slightly inferior to the “primitives,” but not much.
The comparative study revealed that visual acuteness of the “savages and semi civi -lized races” was not outstandingly superior to those found in the normal European. These results suggested that elementary psychological processes, and presumably universal, were not susceptible to cultural variations. On the other hand, the use of cultural conventions would influence processes that depend on them (for example, when the stimulus are complex materials).
The interpretations of the study’s results, the differences and similarities, and later on others, stimulated controversial interpretations by classics of psychology like Titchnner.
Recently, one of my lab students did a trans cultural study about sustained attention processes (Posner’s vigilance) in two different cultural contexts; Santa Cruz de la Sierra, Bolivia and Havana, Cuba. Both cities are similar in size, at same sea and economic level. 50 children of each city were studied age range between 6 and 12 years.
A computerized version of the CPT (Continuous Performance Test) paradigm was used with simple and complex variations (go no go). Exposition time and stimulus concealment was 500 milliseconds on both situations. 700-letter form stimulus was presented.
No significant differences were found between the Bolivian and Cuban children’s performance in the General Attention or in the other elements that are part of it, that is, number of correct answers, non-expected Answers and Omissions. On the other hand, significant differences were observed in relation to reaction time. In the Bolivian sample the superior mean value of time reaction is found for both samples. This indicates that the Bolivian children reacted slower than the Cuban children when placed before the target stimulus in the Simple sustained Attention Test.
Taking into account that a measure used for central processes is reaction time, the results we found suggest that the increase in the answer’s latency which, differentiates Bolivian and Cuban children in our study, indicates variability in the way both groups process information.
In the Simple Sustained Attention Test, the task solution, the optimum one, includes the use of strategies that depend mostly on the knowledge the subject has of letters and colors. This knowledge is very much influenced by the educational experience, there-fore, cultural difficulties in coding and letter recognition might increase the task’s com-plexity and produce an increase in the attention aspect were required for the solution of the test.
Even though this might not affect the correct test’s performance (General Attention Index), it would prolong the target stimulus discrimination time between other stimulus that are similar and increase the reaction time. Based on these results the influence of educational variables that are very specific of a socio-cultural context, on the basic psychophysical measures (TR), are of great value when analyzing the mental processes involved in the information gathering process and answer elaboration. More specific, these results, which are impossible to interpret through nutritional deficit factors (iodine or caloric), or for that matter, sub culturalization, can only be explained because the Cuban educational system has a slight advantage regarding letter decoding.
So, not even a simple paradigm as the CPT is, which directly shows neural central processes, is independent of a subtle cultural context.
A last example of cultural influence; those of nutritional behaviors
Psychologists from the Iguaçu province on the Argentinean north, in a field research, wanted to study what effect environmental contaminants had on cognitive processes in school children. The research design got complicated because in some schools children are permitted to drink during class, “mate” a stimulant beverage very common in that country. As a result, it was impossible to cohort the groups as to general variables be-cause this beverage is very much part of the group’s culture and would interfere in the attention process results interpretation.
Therefore, we must transfer, assimilate, adapt and create specific methodologies when implementing projects so that the measurement procedures are valid, trustworthy and contextualized based on the specific ecological, cultural and socioeconomic characteris-tics of the community where the intervention is going to take place.
Diagnostic and intervention procedures should be designed locally and with partici-pation from some of the community members but most important they should take into account each group’s idiosyncrasy so that all the actions taken will be accepted and not be rejected as an imposition. At the same time, minimum generalization conditions to similar communities must be insured.
However there is still a reasonable doubt. As we are able to contextualize evaluations for local conditions, we will work with subjects who are evaluated in accordance to their context so we will not have the comparison perspective regarding which place would they have in relationship to other human groups economically or materially less favored. Would not it be then a paternalistic approach when we say “normal within its context”, knowing that they will obtain worse results if we compare them to the ones in our context? The answer to this is neither neurobiological nor methodological. It is open to discussion.
What to do after assessment?
The media creates the illusion that the brain’s plasticity is such a wonderful characteristic that it allows us to act with a high efficiency rate. As we all know plasticity expresses its best on the first years of our lives, so this period offers a window of oppor-tunity to intervene through corrective actions or stimulate its development. Because of this, in altered or obstructed child neurodevelopment, the concept “window of oppor-tunity” is a key factor in relation to diagnostics, prognosis and intervention.
An ethical question lies among other things in up to what level can we estimate the possibility of rehabilitating a function? Creating false hopes is against being honest as a scientist and as a human being. Nevertheless, plasticity’s possibilities are yet unknown because the genetic transcription function is influenced so much by external factors that one should not venture to establish a limit for its prognosis.
Doing a correct prognostic evaluation is not seen as a scientific problem itself and it is left on the hands of the author’s intervention, his skepticism or optimism. Cultural and historic trends defend an almost infinite horizon of rehab possibilities while others, more conservatives, center their position in how to handle the limitations that arise as a life style. A consensus criterion does not exist.
Regenerative versus chemical interventions
The growing interest in the use of cholinesterase inhibitors as cognitive enhancers, offer us useful models for study, even though it might not be the panacea. This involves molecular agents tailored for specific problems. The possibility of interaction between behavioral and chemical procedures is promising. In my opinion it is obstaculized by prejudiced views on what is a natural or an artificial intervention. I think those considerations are based on arguments which are not scientific so this is not a good place for its discussion.
These mind theories must relay on the continuously increasing and changing body of information contributed by neurobiology, social sciences, and information handling procedures related to the brain function.
We have to consider another aspect and that is as these interactions are reciprocal, there is always the possibility to apply biological criteria to psychology and social sciences. The danger does not lie in that psychology as a profession loose its power because this argument, even though to stimulate emotions is totally irrelevant for the develop-ment of science.
To reduce this gap the so-called hard sciences must be ready to assimilate and handle the soft data of psychology and other human knowledge. These two must aspire to improve their methods and offer higher quality and generalization results so as to gene-rate information, which might serve as an orientation in relation to brain function.
Be able to count with neurodevelopment evaluation instruments, for children younger than 5 years old, which posses a high degree of sensitivity and specificity. Children in school age have a greater trustworthy behavioral repertoire to evaluate, so we have bet-ter psychometric or neurological procedures for them. But the paradox lies in the fact that we have lost the best years of the brain’s plasticity to achieve effective interventions.
Ending this talk, I would like to mention three important tasks for our work that can only be accomplished by a strong collaboration between the academic world and applied research.
1. Development of methods for cognitive assessment in children under the age of 5 years, with a high degree of sensitivity and specificity.
2. Production of scientific information in relation to the process by which certain fac-tors such as the emotional response, interfere with brain development and/or children’s cognitive performance.
3. Develop research and action methodologies, related to neurodevelopment, which are contextualized in different cultural communities, with ecological value and a certain amount of trans culturalization.
Are we prepared academically? Universities have the answer.
Referências
ALVAREZ, R. R.; GÓMEZ, F. B.; GONZÁLEZ, M. A. A.; YERO, J. L. F.; MARTÍNEZ, F. C.; GESÉN, C. P.; TORRES, A. O.; FUMERO, R. A. Pronóstico de la cognición en el hipotiroidismo congénito tratado precozmente. Hipótesis del doble efecto. Revista de Neurologia, Habana, v. 38, n. 6, p. 513-517, mayo/ago. 2004.
ALVAREZ, M. A.; CARVAJAL, F., RENÓN, A.; PÉREZ, C.; OLIVARES, A.; RODRÍGUEZ, G.; ALVAREZ, V. Differential effect of fetal, neonatal and treatment variables on neurodevelopment in infants with congenital hypothyroidism. Hormone Research, v. 61, n. 1, p. 17-20, Mar. 2004.
ALVAREZ, M. A.; TRAPAGA M. Principios de neurociencias para psicólogos. Buenos Aires: Paidós, 2005.
ALVAREZ, M. A; SAFORCADA, E. El papel de la psicología en la evaluación del impacto de ciertas políticas públicas de salud. In: LELLIS, M. (Ed.). Psicología y políticas públicas de salud. Buenos Aires: Paidós, 2006. p. 187-225.
COLE, Michael. Psicología cultural. Madrid: Morata, 1999.
SAFORCADA, E. Psicología sanitária: análisis crítico de los sistemas de atención de salud. Buenos Aires: Paidós, 1999.
JENKINS, C. D. Building better health. Washington: Pan American Health Organi-zation, 2003.
PANDYA, D. N.; YETERIAN, E. H. The anatomical substrates of emotional behaviour: the role of cerebral cortex. In: BOLLER, F. ; GRAFMAN, J. (Ed.). Handbook of neuropsycholo-gy: emotional behavior and its disorders. 2. ed. Amsterdam: Elsevier, 2001. v. 5.
 Correspondence
Correspondence
Miguel Angel Alvarez González
Facultad de Psicologia Universidad de
La Habana Calle Mazon y San Rafael
Habana, Cuba
e-mail: exxxpadero@yahoo.com
Tramitação
Recebido em fevereiro de 2007
Aceito em abril de 2007

