










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores
Compartilhar

 Permalink
PermalinkPsicologia: teoria e prática
versão impressa ISSN 1516-3687
Psicol. teor. prat. vol.20 no.2 São Paulo maio/ago. 2018
https://doi.org/10.5935/1980-6906/psicologia.v20n2p79-92
ARTICLES
PSYCHOLOGICAL ASSESSMENT
Relationship between substance use and quality of life in a community sample of adults
El consumo de sustancias y la calidad de vida
Luiz Felipe Ayres BernardesI; Nelson Hauck FilhoII; Ana Paula Porto NoronhaIII
ISan Francisco University, USF, SP, Brazil
IISan Francisco University, USF, SP, Brazil
IIISan Francisco University, USF, SP, Brazil
ABSTRACT
Chronic substance use and abuse may associate with the occurrence of several negative events that affect people's quality of life. In this study, we investigated the relationship between the use of substance types and the distinct domains of quality of life as assessed by the WHOQOL-bref. Participants were 105 Brazilian adults from a community sample (mean age = 23.91, SD = .51; 57.14% women). Results revealed that impairments in quality of life were detected only for use of cocaine and anxiolytic drugs; unexpectedly, there was a tendency toward positive relationships between the use of stimulant substances and quality of life. Prevalence rates of moderate use of tobacco, alcohol and marijuana were very high. Findings are discussed considering earlier studies and the possibility of an idiosyncratic composition of the sample employed in the study.
Keywords: drugs; psychopathology; well-being; health; psychological evaluation.
RESUMEN
El uso crónico de sustancias y abuso asociado con la ocurrencia de eventos de la vida que tienen un impacto en la calidad de vida de las personas. En el presente estudio, se emplearon modelos multivariados en un intento de investigar la contribución individual de cada sustancia en la explicación de los distintos dominios de la calidad de vida evaluada por el WHOQOL-BREF. Los participantes fueron 105 adultos brasileños (edad = 23.91, SD = 0,51 significar; las mujeres 57,14%). Los resultados revelaron que las deficiencias en la calidad de vida se asocian únicamente con el uso de la cocaína y las drogas ansiolíticas. Prevalencia del consumo moderado de tabaco, alcohol y marihuana fueron marcadamente más alta que se informó anteriormente. Los resultados se discuten a la luz de los estudios previos y la posibilidad de una composición peculiar de la muestra empleada en el estúdio.
Palabras clave: drogas; psicopatología; salud y bienestar; salud; evaluación de la psicología.
Introduction
Psychoactive substances somehow alter the user's state of consciousness (Seibel, 2010). Continued use and abuse of these substances are related to the occurrence of various events in people's lives, such as health impairments and involvement in accidents (Baylen & Rosenberg, 2006; Gramenzi et al., 2006; Van Dyke & Fillmore, 2015; Waziry, Jawad, Ballout, Al Akel, & Akl, 2016; Zador, Krawchuk, & Voas, 2000), psychopathological conditions (Davis, Uezato, Newell, & Frazier, 2008; Klimas, Neary, McNicholas, Meagher, & Cullen, 2014; Sher & Trull, 2002), interpersonal violence (Choenni, Hammink, & van de Mheen, 2015; Shorey, Stuart, & Cornelius, 2011) and social, labor, and academic impairments (Galea, Nandi, & Vlahov, 2004). Because of the negative effects in various areas of life, substance use can impact people's overall quality of life (QoL), that is, people's integrated assessment of their goals, values, resources, and experiences (Machado & Bandeira, 2012; Orley & Kuyken, 1993). QoL is a subjective and multidimensional construct, which involves individuals' perception of their concerns, expectations and patterns (The Whoqol Group, 1998). In this research, the relationship between substance use and different domains of quality of life is explored in a sample of Brazilian adults.
There is ample evidence linking substance use to reduced QoL (Zubaran & Foresti, 2009). More specifically, the state-of-the-art literature reveals that substance use is associated with declines in a wide range of QoL domains, including physical, social, psychological, labor, academic and financial functioning (Rudolf & Watts, 2009). In some cases, damage may occur in specific domains. In the case of alcohol, negative consequences of chronic use include debilitating diseases (Gramenzi et al., 2006), as well as losses in the individual's social network (Martins, Ribeiro, Baracho, Feital, & Ribeiro, 2012). As for other substances, the damage may be more diffuse. To give an example, the constant use of crack/cocaine seems to impact several domains of QoL (Narvaez et al., 2015). In addition, cocaine users seem to experience lesser satisfaction with life compared to those who use other types of substances (Havassy & Arns, 1998). In short, there are differences in the harm caused by the use of each substance, and generalizations to all types of users are impossible (Rudolf & Watts, 2009).
The connection between substance use and quality of life has increasingly been taken into account in the current perspectives of health assessment and intervention. Quality of life has been focused both on the evaluation of chemical dependence (Zubaran & Foresti, 2009) and on its treatment (Laudet, 2011). Increases in quality of life have been considered criteria to characterize the success of an intervention in the area (Pasareanu, Opsal, Vederhus, Kristensen, & Clausen, 2015). This justifies the proposal of detailed investigations, which seek to understand in greater depth the relationship between the use of specific substances and the different impaired or unaltered domains of QoL. Regarding the relevance, studies of this nature can provide useful information for decision making in health interventions, permitting more effective resource allocation.
One of the problems related to studying substance use and QOL is the fact that part of the individuals consumes various substances (Conway et al., 2013). Due to the collinearity between the use of different substances, the association between the use of any substance and a domain of quality of life can be skewed without statistical control of the overlapping of the variables in relation to the other substances. Thus, a strategy to better understand the specific relationship between each substance and the domains of QL is through multivariate models that control the shared variance among the use of the various substances. This partial relationship with QoL, beyond the bivariate relationships usually reported, may help to better specify the unique damage associated with each substance.
The aim of this study is to investigate to what extent the use of various legal and illegal substances impacts the dimensions of QoL as assessed by means of the WHO-QOL-bref. We sought to understand the partial contribution of each substance to the explanation of QoL by controlling for the effect of the use of other drugs. This permits a more specific understanding of the possible impact of substance use on different dimensions of people's QoL. Secondarily, we also aimed to investigate the prevalence rates of light, moderate and heavy use of nine different substances in the sample.
Method
Participants
The participants were 105 adults between 18 and 55 years old (mean = 23.91 years, SD = 0.51, 57.14% women), who answered the questionnaire online. It is a non-probabilistic convenience sample of individuals from the Brazilian general population, considering that the link to participate in the research was published on a social network (Facebook). The most prevalent level of education was Incomplete Higher Education (58.10%), while the modal income category was superior to R$ 8,000.00 (33.33%). Regarding ethnicity, 88.57% of the participants declared themselves white, 9.52% brown, 0.95% black and 0.95% yellow.
Instruments
Alcohol, Smoking and Substance Involvement Screening Test (ASSIST; Henrique, De Micheli, Lacerda, Lacerda, & Formigoni, 2004; The ASSIST Group, 2002). Used to detect abuse or dependence on alcohol, cigarettes and other psychoactive substances, it contains eight questions on the use of nine classes of psychoactive substances: tobacco, alcohol, marijuana, cocaine, stimulants, sedatives, inhalants, hallucinogens and opiates. The questions address use in life (question 1), use in the past three months (question 2), craving (question 3), problems related to use (question 4), concern about the use by people close to the user 5), impaired performance of expected tasks (question 6), unsuccessful attempts to cease or reduce use (question 7), use of injectable substances (question 8). In all seven first questions, the individual should indicate a score for each substance, being a "yes" or "no" answer to the first and final questions and frequency responses on a Likert scale for the other questions (e.g. "never" , "1 or 2 times", "monthly", "weekly", "daily or almost every day"). In this sample, the internal consistency of the instrument based on the alpha coefficient was 0.88, when considering the total number of items.
The World Health Organization (WHO) recommends some cut-off points in the instrument, which can be used to screen for possible disorders. In the case of the alcohol, scores of 0 to 10 are classified as abstemious or low-risk use, 11 to 26 points as moderate use, and 27 or more points as heavy use. For the other substances, the WHO suggests classifying scores from 0 to 3 as abstemious or low-risk use, from 4 to 26 for moderate use, and 27 or more as heavy use.
Quality of life assessment questionnaire - short version (WHOQO-bref; The WHOQOL Group, 1998). It is a self-reported instrument, containing 26 items that evaluate the general (2 items) and specific (24 items) aspects of people's quality of life. The specific items are distributed in four domains: physical, psychological, social relationships and environment. All items are scored on a Likert scale from 1 to 5 points. In this study, the internal consistency of the WHOQOL-bref was assessed using the alpha coefficient, with 0.84 for the total scale, 0.73 for the physical domain, 0.76 for the psychological, 0.80 for social relationships and 0.77 for the environment.
Procedures
The project received approval from the Research Ethics Committee of the University of São Francisco. The data collection was done using the resource Google Docs, which permitted the creation of an online questionnaire in which the tools were made available for application. The link was posted on a social network (Facebook) on the primary author's main page and remained available for 15 days. The text that preceded the link informed the academic nature of the research and its authorization by the Research Ethics Committee, in addition to its voluntary nature. Upon access, a Free and Informed Consent Form was displayed for each participant, describing the objectives and nature of the study. The participants only had access to the research instruments after confirming that they were 18 years of age or older and agreed to consent term.
Data analysis
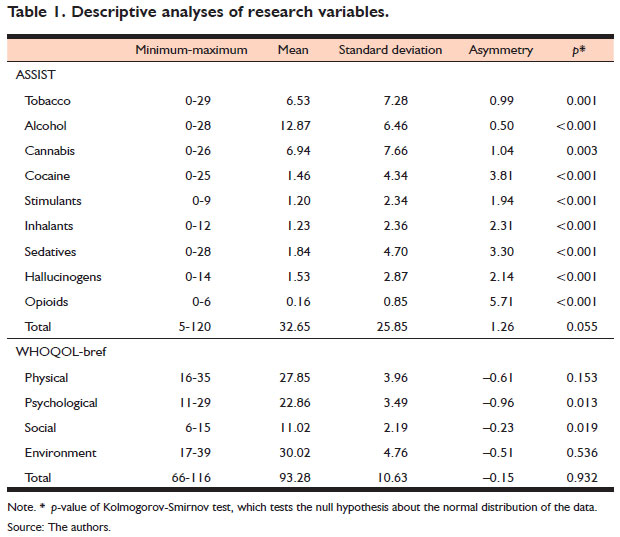
Descriptive statistics (mean, frequency, standard deviation) were used in the description of the data. The normality assumption of the data was investigated using the Kolmogorov-Smirnov test, which revealed significant deviations from normality in some of the variables, as presented below, in Table 1. Based on this result, robust analysis strategies were employed to minimize bias in the parametric estimates of the models (Erceg-Hurn & Mirosevich, 2008). The linear relationship between the research variables was investigated using two approaches: bivariate and multivariate. For the first case, Spearman's rho ordinal coefficient was used to quantify the strength of association between the variables. For the second case, multivariate linear regressions were used in combination with the bootstrap method to predict the QoL dimensions based on the nine subscales of the ASSIST (tobacco, alcohol, cannabis, cocaine, stimulants, sedatives, inhalants, hallucinogens and opioids). Resampling tends to produce better approximations of the theoretical distribution of the statistical tests (F and t) used in the multivariate regression analysis (Erceg-Hurn & Mirosevich, 2008) are based on. In view of the small sample size (n = 109), possible deviations from normality and a large number of predictors in each model (nine), we decided to relate the adjusted R2 coefficient in order to quantify the explained variance in each dependent variable. This coefficient tends to be less biased in small samples. The analyses were developed in IBM SPSS 20.
Results
The descriptive analysis of the variables is presented in Table 1. The sample specifically presented a trend towards lower scores in the subscales of the ASSIST (positive asymmetry), and a trend towards high scores in the dimensions of the WHOQOL-bref (negative asymmetry). The substances in the ASSIST that demonstrated greater variation (standard deviation) in the endorsed scores were cannabis, tobacco and alcohol, in decreasing order.
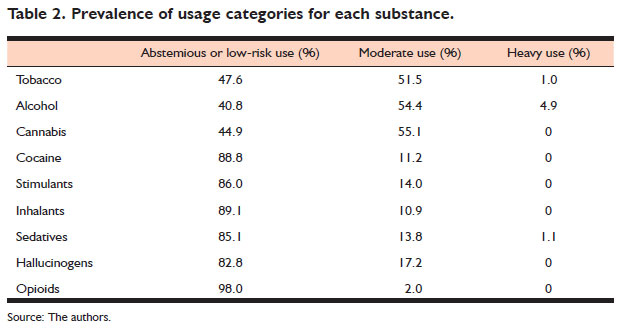
Next, a more detailed analysis of the ASSIST variables was developed, aiming to investigate the prevalence rates of abstemious or low-risk use, moderate use or heavy use for each substance. The findings have been displayed in Table 2. As noticed, the most reported substances were tobacco, alcohol and cannabis, with very similar prevalence rates in the three categories (except because there was no case of heavy cannabis use). For the other substances, most cases were classified in the abstemious or low-risk use category, some cases (between 2 and 17.2%) in the moderate use category, and no case (except for hypnotic drugs, with one case), in the heavy use category.
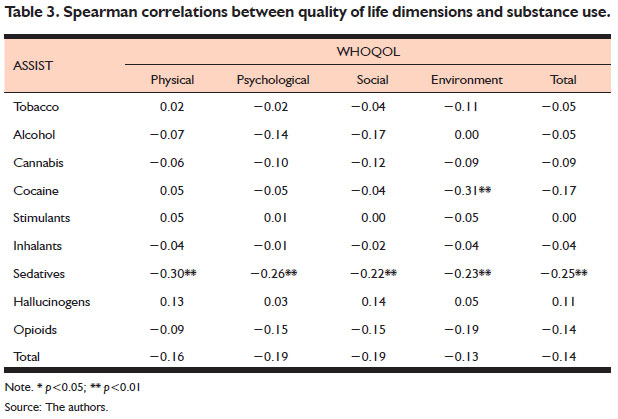
The next step was the bivariate assessment of the linear relationship between the variables using Spearman's ordinal coefficient. The results have been displayed in Table 3. As observed, overall, the correlations between substance use and QoL were very small, despite the trend towards a negative relationship pattern. The most expressive coefficients were found for the correlation between cocaine use and the environment dimension of the WHOQOL (rho = −0.31), and between the use of sedatives and all dimensions of the WHOQOL, physical (rho = −0.30), psychological (rho = −0.26), social (rho = −0.22), environment (rho = −0.23) and total (rho = −0.25). Even the correlation between the total scores of both instruments - variables with greater variance when compared to the others - was low (rho = −0.14).
Although the correlation coefficients inform about the relationship between the research variables, it is a type of bivariate analysis that does not control the effect sizes by the shared variance with other potentially related variables. Thus, multivariate linear regression analyses were conducted to estimate the unique partial relationship of each substance with the quality of life dimensions. There were five multivariate linear regression models: four predicting each WHOQOL-bref dimension (physical, psychological, social and environmental), and one predicting the total WHOQOL-bref score. In each model, the predictors were the ASSIST variables, that is, the total scores for the use of tobacco, alcohol, cannabis, cocaine, stimulants, inhalants, sedatives, hallucinogens and opioids. The inspection of the redundancy among the predictors based on the Tolerance coefficient revealed no value below 0.10. Therefore, no variables need to be excluded from the model.
The results of these analyses are displayed in Table 4. In general, substance use was able to explain a small portion of the QoL variance, between 3% (social and total) and 11% (environment). Only the model predicting the environmental dimension proved to be significant. The predictors with betas significantly different from 0 were the use of cocaine (-0.35) and sedatives (-0.27). It is also noteworthy that the use of sedatives presented a consistent pattern of negative (small to moderate) relationship with the dimensions of the WHOQOL-bref, even after controlling for the influence of the use of other substances.
Discussion
This study has two main sets of findings. The first one, central to the objective of the present study, concerns linear associations between substance use and QoL. The second, in turn, concerns the prevalence rates found for low-risk use/abstinence, moderate use and heavy use.
Both the correlational analyses and multivariate regressions presented mixed results regarding the possible effect of substance use on the QoL of individuals. More specifically, only the use of cocaine and sedatives was related to the WHOQOL dimensions. In the case of cocaine, a negative linear relation of small to moderate magnitude (β= -0.35) was found with the environment domain. This finding reveals that, in the present sample, cocaine use was associated with a greater negative perception of the quality of the individual's living environment was found, including his/her safety and resources in general (financial, health, transportation, residence). Accordingly, other studies have reported that cocaine use tends to influence mental health (Haasen, Prinzleve, Gossop, Fischer, & Casas, 2005), especially among individuals with a background history of depression (Helmus, Downey, Wang, Schuster), and during abstinence after intense use (Brown et al., 1998). Nevertheless, in this study, the impairment was found to be specific to the environmental domain, and not to physical health, to positive and negative affects or to relationships with significant others. One notable aspect, however, is the sample composition in this study, which included almost 90% of white individuals, one-third of whom gained an income superior to R$ 8,000.00. Thus, the losses these individuals experienced may be mitigated by the availability of some resources most of the population does not have. Therefore, this result should be viewed with reservations. Being a correlational design, one cannot deny a possible reverse effect either, responsible for the relationship between these variables. In other words, unstructured environments with few incentives towards personal and professional development can facilitate cocaine use.
A predictor that merits detailed analysis is the use of sedatives. This category of substances was negatively related to all domains of the WHOQOL-physical, psychological, social and environmental, and with the total score. One possibility is that, among the substances analyzed, this was the most detrimental to the quality of life of the people in the sample. Nevertheless, the modeling employed in this study does not reveal the nature of the true causal effect that links both variables. In this case, the impairment in the quality of life among users of anxiolytics and sedatives may exist prior to the contact with the substance. In fact, there is evidence that the main motives that lead people to use this type of medicine include a reduced quality of life, involving various physical, psychological, social and environmental aspects (Zagozdzon, Kolarzyk, & Marcinkowski, 2013). Therefore, the findings reported here indicate a consistent association, but do not permit establishing the causal orientation of the relationship, and the reduced quality of life may be exactly the reason why these users seek anxiolytic and sedative drugs. When without proper medical follow-up, of course, the use of these substances through self-medication may also be partially responsible for a decrease in quality of life, an effect that could be addressed in further research.
The associative pattern of stimulant use also deserves a separate analysis. All the standardized regression coefficients were positive, but of low magnitude (0.13-0.30), and did not reach statistical significance. The lack of significance indicates that the confidence interval for the effect sizes included zero and that, therefore, associations may be due to chance. It may also be the case that these positive relations of low magnitude do exist and were not detected only because of the reduced statistical power and sample size. In this case, although unexpected, the positive associations may be due to the idiosyncratic composition of the sample, composed of young, mostly white individuals with favorable economic conditions. Thus, the economic situation may be the exogenous variable responsible for both phenomena, that is, having the money to buy stimulants and having favorable living conditions. This confounding variable would need appropriate controls in studies with expanded samples, with greater socioeconomic diversity. It should be emphasized that, in case of an endogenous relation (i.e. use of stimulants and QoL being associated because they are both influenced by the socioeconomic level), the relationship between the variables may be null or even inverse (Antonakis, Bendahan, Jacquart, & Lalive, 2010). This aspect should be better investigated.
The second result refers to the usage prevalence estimates found for each substance in the ASSIST questionnaire. Although most prevalence estimates are consistent with the results reported in earlier studies (Medeiros, Rediess, Hauck Filho, Martins, & Mazoni, 2012; Peuker, Fogaça, & Bizarro, 2006; Wagner & Andrade, 2008), the exceptions draw attention. A rather high percentage - superior to 50% - was classified in the category of moderate-use on the ASSIST for tobacco, alcohol and cannabis. Although alcohol abuse among young people is relatively more common when compared to other individuals (Peuker et al., 2006), the moderate use of these three substances was much higher than reported in other studies (Medeiros et al., 2012; Wagner & Andrade, 2008). For the mere sake of illustration, in the study by Medeiros et al. (2012), using a university sample from Rio Grande do Sul, the proportion of students included in this same ASSIST category was 19.2% for tobacco, 12.9% for alcohol and 7.4% for cannabis. The indices found here are, therefore, noteworthy because they are not typical of the pattern of substance use among young Brazilians. Further studies with larger and more representative samples are required to ascertain whether this is a trend for certain population groups or an idiosyncrasy of this sample.
An important limitation of this study is the sample composition, as already mentioned. There is evidence that socioeconomic status acts as a moderator in the relationship between personality traits and substance use (Sutin, Evans, & Zonderman, 2013). That is, characteristics that are risk factors in some portions of the population may not be in others, because resources are available that mitigate their negative influence. As a research agenda, it would therefore be important to try and replicate this study with economically more diversified samples, in order to verify if the effects and prevalence rates found here are based on other contexts. In addition, it would be desirable to investigate whether the effects reported here continue when investigating the phenomenon in samples from other regions of Brazil. Overall, extended samples in future studies will be central to judge the consistency of the parametric estimates reported here.
Another noteworthy limitation is the lack of control over other variables that may play a role, interfering with the relationship between substance use and quality of life. Specifically, the presence of mental disorders may impact this relationship, which is why this aspect should be addressed in future research. For example, in controlling for the presence of mental disorders, some regression coefficients may be greater than those reported here if there are suppressive effects (Maasen & Bakker, 2001). A suppression effect occurs when the relationship between the variables X and Y is smoothened as a function of the omission of the variable Z from the model. If the presence of some mental disorder acts as a suppressive variable, then the results may be slightly different when testing the same model in a mixed community and psychiatric-patient sample. In this study, there was no control in the sense of differentiating individuals with or without a history of mental disorders or other medical conditions. Therefore, investigating the stability of the model parameters reported herein in other types of samples is still necessary.
Yet another point deserves a comment. Caution is due to the interpretation of these findings as if they were causal evidence of a relationship between the variables. The coefficients reported here characterize the partial relationship between the predictors and the dependent variables in the context of the model, but do not necessarily reflect the true nature and causal flow acting on these variables. A two-way, mutually influential relationship between substance use and quality of life is perfectly possible. Attempts to generalize the results described herein should be made in view of this important limitation.
The study represents a contribution to the Brazilian literature on substance use and QoL, identifying specific associations between the use of certain drugs and impairments in QoL dimensions. Even under the possibility of an idiosyncratic sample, the findings reported here illustrate the importance of further investigating associations between the variables across diverse population groups without incurring invalid generalizations.
References
Antonakis, J., Bendahan, S., Jacquart, P., & Lalive, R. (2010). On making causal claims: a review and recommendations. The Leadership Quarterly, 21(6),1086-1120. doi:10.1016/j.leaqua.2010.10.010 [ Links ]
Baylen, C. A., & Rosenberg, H. (2006). A review of the acute subjective effects of MDMA/ecstasy. Addiction, 101(7),933-947. doi:10.1111/j.1360-0443.2006.01423.x [ Links ]
Brown, R. A., Monti, P. M., Myers, M. G., Martin, R. A., Rivinus, T., Dubreuil, M. E., & Rohsenow, D. J. (1998). Depression among cocaine abusers in treatment: relation to cocaine and alcohol use and treatment outcome. The American Journal of Psychiatry, 155(2),220-225. doi:10.1176/ajp.155.2.220 [ Links ]
Choenni, V., Hammink, A., & van de Mheen, D. (2015). Association between substance use and the perpetration of family violence in industrialized countries: a systematic review. Trauma, Violence & Abuse, 18(1),37-50. doi:10.1177/1524838 015589253 [ Links ]
Conway, K. P., Vullo, G. C., Nichter, B., Wang, J., Compton, W. M., Iannotti, R. J., & Simons-Morton, B. (2013). Prevalence and patterns of polysubstance use in a nationally representative sample of 10th graders in the United States. The Journal of Adolescent Health: Official Publication of the Society for Adolescent Medicine, 52(6),716-723. doi:10.1016/j.jadohealth.2012.12.006 [ Links ]
Davis, L., Uezato, A., Newell, J. M., & Frazier, E. (2008). Major depression and comorbid substance use disorders. Current Opinion in Psychiatry, 21(1),14-18. doi:10.1097/YCO.0b013e3282f32408 [ Links ]
Erceg-Hurn, D. M., & Mirosevich, V. M. (2008). Modern robust statistical methods: an easy way to maximize the accuracy and power of your research. American Psychologist, 63(7),591-601. doi:10.1037/0003-066X.63.7.591 [ Links ]
Galea, S., Nandi, A., & Vlahov, D. (2004). The social epidemiology of substance use. Epidemiologic Reviews, 26(1),36-52. doi:10.1093/epirev/mxh007 [ Links ]
Gramenzi, A., Caputo, F., Biselli, M., Kuria, F., Loggi, E., Andreone, P., & Bernardi, M. (2006). Review article: alcoholic liver disease ? Pathophysiological aspects and risk factors. Alimentary Pharmacology and Therapeutics, 24(8),1151-1161. doi:10.1111/j.1365-2036.2006.03110.x [ Links ]
Haasen, C., Prinzleve, M., Gossop, M., Fischer, G., & Casas, M. (2005). Relationship between cocaine use and mental health problems in a sample of European cocaine powder or crack users. World Psychiatry: Official Journal of the World Psychiatric Association (WPA), 4(3),173-176. [ Links ]
Havassy, B. E., & Arns, P. G. (1998). Relationship of cocaine and other substance dependence to well-being of high-risk psychiatric patients. Psychiatric Services, 49(7),935-940. doi:10.1176/ps.49.7.935 [ Links ]
Helmus, T. C., Downey, K. K., Wang, L. M., Rhodes, G. L., & Schuster, C. R. (2001). The relationship between self-reported cocaine withdrawal symptoms and history of depression. Addictive Behaviors, 26(3),461-467. Retrieved May 18, 2018, from http://www.ncbi.nlm.nih.gov/pubmed/11436938 [ Links ]
Henrique, I. F. S., De Micheli, D., Lacerda, R. B. de, Lacerda, L. A. de, & Formigoni, M. L. O. de S. (2004). Validação da versão brasileira do teste de triagem do envolvimento com álcool, cigarro e outras substâncias (ASSIST). Revista da Associação Médica Brasileira, 50(2),199-206. doi:10.1590/S0104-42302004000200039 [ Links ]
Klimas, J., Neary, A., McNicholas, C., Meagher, D., & Cullen, W. (2014). The prevalence of common mental and substance use disorders in general practice: a literature review and discussion paper. Mental Health and Substance Use, 7(4),497-508. doi:10.1080/17523281.2014.939221 [ Links ]
Laudet, A. B. (2011). The case for considering quality of life in addiction research and clinical practice. Addiction Science & Clinical Practice, 6(1),44-55. [ Links ]
Maasen, G. H., & Bakker, A. B. (2001). Suppressor variables in path models: definitions and interpretations. Sociological Methods & Research, 30(2),241-270. doi:10.1177/0049124101030002004 [ Links ]
Machado, W. de L., & Bandeira, D. R. (2012). Bem-estar psicológico: definição, avaliação e principais correlatos. Estudos de Psicologia, 29(4),587-595. doi:10.1590/ S0103-166X2012000400013 [ Links ]
Martins, M. E., Ribeiro, L. C., Baracho, R. A., Feital, T. J., & Ribeiro, M. S. (2012). Qualidade de vida e consumo de alcoólicos em hepatopatas do sexo masculino. Revista de Psiquiatria Clínica, 39(1),5-11. doi:10.1590/S0101-60832012000100002 [ Links ]
Medeiros, S. B. de, Rediess, S. V., Hauck Filho, N., Martins, M. I. M., & Mazoni, C. G. (2012). Prevalência do uso de drogas entre acadêmicos de uma universidade particular do sul do Brasil. Aletheia, (38-39),81-93. Recuperado em 5 maio, 2018, de http://pepsic.bvsalud.org/scielo.php?script=sci_arttext&pid=S1413-03942012000 200007&lng=pt&nrm=iso&tlng=pt [ Links ]
Narvaez, J. C. M., Pechansky, F., Jansen, K., Pinheiro, R. T., Silva, R. A., Kapczinski, F., & Magalhães, P. V. (2015). Quality of life, social functioning, family structure, and treatment history associated with crack cocaine use in youth from the general population. Revista Brasileira de Psiquiatria, 37(3),211-218. doi:10.1590/15164446-2014-1494 [ Links ]
Orley, J., & Kuyken, W. (1993). Quality of life assessment: international perspectives. Paris: Springer. [ Links ]
Pasareanu, A. R., Opsal, A., Vederhus, J.-K., Kristensen, Ø., & Clausen, T. (2015). Quality of life improved following in-patient substance use disorder treatment. Health and Quality of Life Outcomes, 13,35-38. doi:10.1186/s12955-015-0231-7 [ Links ]
Peuker, A. C., Fogaça, J., & Bizarro, L. (2006). Expectativas e beber problemático entre universitários. Psicologia: Teoria E Pesquisa, 22(2),193-200. doi:10.1590/S0 102-37722006000200009 [ Links ]
Rudolf, H., & Watts, J. (2009). Quality of life in substance abuse and dependency. International Review of Psychiatry, 14(3),190-197. doi:10.1080/09540260220144975 [ Links ]
Seibel, S. D. (2010). Dependência de drogas (Vol. 2). São Paulo: Atheneu. [ Links ]
Sher, K. J., & Trull, T. J. (2002). Substance use disorder and personality disorder. Current Psychiatry Reports, 4(1),25-29. doi:10.1007/s11920-002-0008-7 [ Links ]
Shorey, R. C., Stuart, G. L., & Cornelius, T. L. (2011). Dating Violence and substance use in college students: a review of the literature. Aggression and Violent Behavior, 16(6),541-550. doi: https://doi.org/10.1016/j.avb.2011.08.003 [ Links ]
Sutin, A. R., Evans, M. K., & Zonderman, A. B. (2013). Personality traits and illicit substances: the moderating role of poverty. Drug and Alcohol Dependence, 131(3),247-251. doi:10.1016/j.drugalcdep.2012.10.020 [ Links ]
The WHOQOL Group (1998). Development of the World Health Organization WHOQOL-bref quality of life assessment. Psychological Medicine, 28(3),551-558. [ Links ]
Van Dyke, N. A., & Fillmore, M. T. (2015). Distraction produces over-additive increases in the degree to which alcohol impairs driving performance. Psychopharmacology, 232(23),4277-4284. doi:10.1007/s00213-015-4055-2 [ Links ]
Wagner, G. A., & Andrade, A. G. de. (2008). Uso de álcool, tabaco e outras drogas entre estudantes universitários brasileiros. Revista de Psiquiatria Clínica, 35,48-54. doi:10.1590/S0101-60832008000700011 [ Links ]
Waziry, R., Jawad, M., Ballout, R. A., Al Akel, M., & Akl, E. A. (2016). The effects of waterpipe tobacco smoking on health outcomes: an updated systematic review and meta-analysis. International Journal of Epidemiology, 46(1),32-43. doi:10.10 93/ije/dyw021 [ Links ]
World Health Organization (2002). The Alcohol, Smoking and Substance Involvement Screening Test (ASSIST): development, reliability and feasibility. Addiction, 97(9),1183-1194. doi:10.1046/j.1360-0443.2002.00185.x [ Links ]
Zador, P. L., Krawchuk, S. A., & Voas, R. B. (2000). Alcohol-related relative risk of driver fatalities and driver involvement in fatal crashes in relation to driver age and gender: an update using 1996 data. Journal of Studies on Alcohol, 61(3),387-395. doi:10.15288/jsa.2000.61.387 [ Links ]
Zagozdzon, P., Kolarzyk, E., & Marcinkowski, J. T. (2013). Quality of life and social determinants of anxiolytics and hypnotics use in women in Poland: a population-based study. The International Journal of Social Psychiatry, 59(3),296-300. doi:10.1177/0020764012440676 [ Links ]
Zubaran, C., & Foresti, K. (2009). Quality of life and substance use: concepts and recent tendencies. Current Opinion in Psychiatry, 22(3),281-286. [ Links ]
 Mailling address:
Mailling address:
Luiz Felipe Ayres Bernardes
Rua Major Querino Pereira de Morais, 124, Centro
Itapetininga - SP. CEP: 18200-060
E-mail: luizbernardes.psi@gmail.com
Submission: 7.19.2016
Acceptance: 5.2.2018

{kind=link}
{kind=link}
{kind=link}
{kind=link}