










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores
Compartilhar

 Permalink
PermalinkPsicologia: teoria e prática
versão impressa ISSN 1516-3687
Psicol. teor. prat. vol.20 no.2 São Paulo maio/ago. 2018
https://doi.org/10.5935/1980-6906/psicologia.v20n2p161-174
ARTICLES
HUMAN DEVELOPMENT
Social support and satisfaction of primary caregivers of children with cerebral palsy
El apoyo social y la satisfacción de los cuidadores primarios de los niños con parálisis cerebral
Tatiana AfonsoI; Fernando Augusto Ramos PontesII; Simone Souza da Costa SilvaIII
IFederal University of Pará, UFPA, PA, Brazil
IIFederal University of Pará, UFPA, PA, Brazil
IIIFederal University of Pará, UFPA, PA, Brazil
ABSTRACT
This study aimed to analyze the satisfaction with social support available to primary caregivers of children with CP. Participated 101 caregivers of children 0-12 years with cerebral palsy. Instruments: Social Support Scale, Scale of Satisfaction with Social Support, sociodemographic schedule and Gross Motor Function Classification System. Results: ANOVAs indicated that family satisfaction had the highest satisfaction followed by satisfaction with friends, intimate satisfaction and social activities. Pearson's test indicated that supports were positively related to the different types of satisfaction. The caregivers of older children reported less informational support and those who cared for more compromised children reported less satisfaction with intimacy. However, the level of general satisfaction was high due to the high satisfaction with the family, a relevant result within a positive perspective of the evaluation of families of children with CP.
Keywords: families of child with disabilities; health of the primary caregiver; support networks; special education; rehabilitation.
RESUMEN
Este estudio tuvo como objetivo analizar la satisfacción con el apoyo social disponible para los cuidadores primarios de niños con parálisis cerebral. Participado 101 cuidadores de niños de 0-12 años, con parálisis cerebral. Instrumentos: Escala de Apoyo Social, Escala de satisfacción con el apoyo social, el horario sociodemográfico y Sistema de clasificación de la Función Motora Grossa. Resultados: ANOVA indicó que la satisfacción familia tuvo la satisfacción más alta, seguido de la satisfacción con los amigos, intimidad y actividades sociales. La pueba de Pearson indicó que los apoyos estuvieron relacionados positivamente con los diferentes tipos de satisfacción. Los cuidadores de niños mayores relataron menor apoyo informacional y aquellos que cuidaban a niños más comprometidos relataron menor satisfacción con la intimidad. Por fin, el nivel de satisfacción general se mostró alto debido a la alta satisfacción con la familia, resultado positivo en la evaluación.
Palabras clave: las familias con hijos con discapacidad; la salud del cuidador principal; Las redes de apoyo; educación especial; rehabilitación.
Introduction
Social support networks are present in people's lives and, given their importance and multiple functions, comprise complex and multidimensional phenomena (Saranson, Saranson, & Pierce, 1990). They are constituted both by the objective aspects of coexistence, such as the number of friends, the frequency of contact, the existence of close friends and social contacts, and by subjective aspects, such as the perception of satisfaction with the support provided in the interactions (Ribeiro, 1999).
Social networks are defined as a set of significant systems and people that compose the relationship links perceived by an individual (Siqueira, Betts, & Dell'Aglio, 2006). Their complex nature involves interpersonal and intrapersonal characteristics. Thus, in interpersonal terms, they are constituted by groups of people with whom they are in contact and who may or may not offer help, covering support with different functions, while the intrapersonal perspective involves satisfaction with the support received (Griep et al., 2005).
Social support presents distinct functionalities, such as material support, affective support, emotional support, informational support and positive social interactions. It can make people believe that they are cared for, loved, esteemed and that they are members of a social network of meaningful relationships (Araújo et al., 2013).
Regarding the existing types of networks, those made up of relatives are shown to be the ones used most frequently (Silva Júnior, Brito, & Beltrão, 2010). These networks are more evident in situations where the need for help and protection is present, as in the case of the disability of a child (Gallagher & Whiteley, 2012; Thurston et al., 2011).
Among the impairments linked to disabilities, cerebral palsy (CBP) stands out as a condition that compromises different functions and structures of the body that can lead to limitations in relevant activities and restricted social participation. The presence of sensory deficits and convulsions are common, as is delayed cognitive development. Its evaluation should consider the needs of the child, the priorities of the family, the cultural context, and the support networks available (Cury & Brandão, 2011).
Faced with the diagnosis of a child with CP, the direct or indirect activation of the social support network is expected, contributing to good parental and family functioning and favoring the reestablishment of the emotional well-being of the parents (Britner et al., 2003). Social support networks are able to help in the process of parental adaptation, allowing parents to exercise their role more adequately, taking into account the challenges in the various daily activities that are often of long duration, require attention and possibly even lead to an imbalance between the other activities of their routines (Cury & Brandão, 2011; Gallagher & Whiteley, 2012; Thurston et al., 2011). In this sense, receiving more social support results in less overload and higher levels of well-being, as well as fewer symptoms associated with psychological distress and a lower perception of the negative impact of the disability (Gallagher & Whiteley, 2012; Thurston et al., 2011). However, in spite of the evidence that indicates an association between the support network and the reduction of stress and distress, with an immediate beneficial effect on health, studies have highlighted that the presence of the support network does not always translate into intimate satisfaction, as a caregiver may have a negative perception of the support available (Al-Gamal & Longo, 2013).
The perception of the person regarding the social support received can modify it, with it being this perception, rather than the objective support, that will exert an emotional moderating effect faced with difficult situations. The interactions that make up the support network have more impact when evaluated as satisfactory by those who receive the support. In this sense, it is the perception, not the physical characteristics of the social networks that determine the quality of the support received (Santos, Pais-Ribeiro, & Lopes, 2003).
Taking into consideration the satisfaction, the most subjective aspect of the network, studies with families of children with disabilities in different cultural contexts present contrasting results in relation to the support network available (Alaee et al., 2014; Huang, Kellett, & St John, 2010; Huang, Kellett, & St John, 2012; Kurtuncu et al., 2013). Kurtuncu et al. (2014) investigated Muslim mothers of 15 children with CP living in Turkey and detected some difficulties related to low satisfaction with the support networks, such as problems in the personal and marital relationships, as well as difficulties in the process of social inclusion and in the access to the formal care networks.
In agreement with these findings, the work of Huang, Kellett, & St John (2012) and Huang, Kellett, & St John (2010) with Chinese mothers of children with CP (N = 15) indicated that they felt lonely in the role of principal caregivers, were hostile to their husbands' families and, therefore, had little or no social support. In addition to these studies, from the reports of the 20 participants of the study by Alaee et al. (2014) in Iran, it was identified that the parents perceived the services provided to be inadequate. From the interviews, the researchers highlighted that the perception of social support was unsatisfactory, which caused suffering for the parents as they felt helpless and without an adequate structure of acceptance and guidance.
Al-Gamal & Longo (2013), working with 204 parents of children with CP in Jordan, identified that family support correlated negatively with the emotional and marital problems of the caregivers. This study indicated that low social satisfaction was shown to be an important aspect related to health and well-being, rather than the severity of the disability itself.
Considering the importance of expanding the knowledge regarding satisfaction with the support received of caregivers of children with CP, an important aspect for the evaluation of the emotional health of the people that are considered essential for the health of these children, the present study aimed to describe the frequency of the main types of social support available to caregivers of children with CP and the level of social satisfaction of the participants with this support. This study is unique as it was carried out in a differentiated cultural context, the Amazon, Pará state, Brazil, making it original in terms of population and region, which have little representation in studies related to inclusion.
Method
Participants
The participants of this study were 101 parents and guardians of children between 0 and 12 years of age diagnosed with cerebral palsy and receiving care in a referral center specialized in the areas of childhood growth and development in the capital city of Belém, Pará state, Brazil. Children who, in addition to the diagnosis of cerebral palsy, had genetic syndromes and/or autism spectrum disorders were excluded from the sample.
Collection environment
The data collection was performed in the waiting rooms of a university referral hospital for the care of children with CP, with the caregivers being invited to participate in the study while waiting for the consultations of their children.
Data collection procedure
Ethical procedures
The project was submitted to the Ethics Committee of the Health Sciences Institute (Instituto de Ciências da Saúde - ICS) of the Federal University of Pará, receiving authorization (No. 473.140) and a consent form was signed.
Data collection
After the participant read the consent form and agreed to participate, the interviewer initiated the application of the instruments in the following order: SDI, GMFCS, MOS, and ESSS. The average time for the application of the four instruments was one hour.
About the instruments
Sociodemographic Inventory (SDI): investigates issues related to the sociodemographic data; characterization of the family system and data related to the child with cerebral palsy.
GMFCS - Gross Motor Function Classification System (Palisano et al., 1997): comprises part of the GMFM (Russell et al., 2011), which is a scale of measurement of the gross motor function of children with CP. It evaluates the child in five levels (I, II, III, IV, and V) according to the age considering what the child can accomplish in terms of gross motor function. Level I - walks without limitations, Level II - walks with limitations, Level III - can walk with the help of walking frame or crutches, has difficulty walking outside the home and in the community, Level IV - limited mobility, requires a wheelchair to move outside the home and in the community and Level V: severely limited mobility, transported in a manual wheelchair.
Social Support Scale - Medical Outcomes Study Social Support Survey (MOS): adapted for the Brazilian population by Griep et al. (2005), the Brazilian validation studies found good internal consistency of the items with Cronbach's alphas from 0.76 (Griep et al., 2005; Zanini et al., 2009). In a pilot study performed by the authors, Cronbach's alpha values ranged from 0.75 to 0.86, results considered favorable. In the present work, the Zanini et al. (2009) version was used, composed of 19 questions that begin with the sentence: If you need it, how often can you count on someone...?". The participants respond on a scale ranging from "Never" to "Always." It consists of five dimensions: material support; affective support; positive social interaction; emotional support and informational support.
Social Support Satisfaction Scale (Escala de Satisfação com o Suporte Social - ESSS): Developed and validated by Ribeiro (1999), it aims to evaluate social satisfaction. It presents good internal consistency (Cronbach's alpha) of 0.85 and consists of 15 phrases that allow the subjects to indicate their degree of agreement with each statement (whether or not the phrase applies to their individual situation). It is structured on a Likert type scale with five response positions, "completely agree," "mostly agree," "do not agree or disagree," "mostly disagree," and "completely disagree." The ESSS allows four dimensions or factors to be extracted: Satisfaction with friends/friendships that measures satisfaction with friendships and includes five items (3, 12, 13, 14 and 15); Intimacy that measures the perception of the existence of intimate social support and includes four items (1, 4, 5 and 6); Satisfaction with the family that measures satisfaction with existing family support and includes three items (9, 10 and 11); and Social activities that measures satisfaction with social activities performed and includes three items (2, 7 and 8).
Data analysis procedure
Social Support Scale - Medical Outcomes Study Social Support Survey (MOS)
This scale was scored as follows: 1 for the answer never, 2 for rarely, 3 for sometimes, 4 for almost always and 5 for always. In order to facilitate the analyses of the dimensions, the scores were transformed into percentages in which the sum of the points obtained by the questions of each dimension was divided by the maximum possible score in the same dimension (which varied according to the number of questions). The result of the ratio (total score obtained/maximum score of the dimension) was multiplied by 100. The caregivers who failed to answer any question in a certain dimension were excluded from the calculation of that score (Griep et al., 2005).
ESSS (Social Support Satisfaction Scale)
This was scored as follows: 1 for the answer totally agree, 2 for mostly agree, 3 for do not agree or disagree, 4 for mostly disagree and 5 for totally disagree. Exceptions were the inverted items: 4, 5, 9, 10, 11, 12, 13, 14 and 15. In addition to the scores by dimensions, the ESSS generates a total score, with higher scores corresponding to higher satisfaction and lower scores indicating lowest levels of satisfaction with the social support. In the present study low satisfaction corresponded to values between 0 and 25, medium satisfaction between 25 and 50 and high satisfaction between 50 and 75.
In addition to the descriptive statistics, the ANOVA (comparing the sum of the responses obtained in each domain of the MOS and ESSS with the demographic data) and Chi-square, Equality of Two Proportions (characterizing the distribution of the relative frequency of the results of the MOS and ESSS scales) parametric tests were used. Furthermore, Pearson's correlation, the Correlation Test and the P-value (significant, positive/proportional, negative/inversely proportional) were used. A significance level of 0.05 (5%) was defined for this study, in which all confidence intervals were established with 95% statistical confidence. When determining the quality of a correlation, the following classification was used: 1-20% very poor; 20%-40% poor; 40%-60% regular; 60%-80% good and 80%-100% very good.
Results
Characteristics of the caregivers and scores of the MOS and ESSS
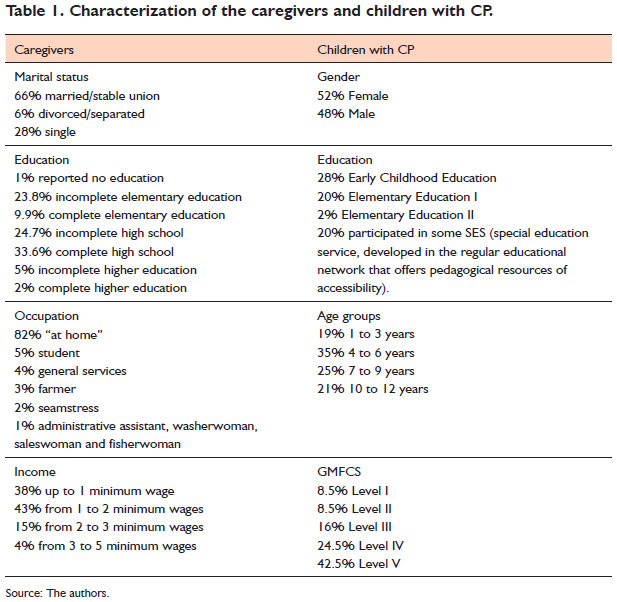
The sample consisted of 101 caregivers, most of whom were women and mothers (87% mothers, 6% grandmothers, 4% foster mothers, 1% fathers and 1% stepmothers), with a mean age of 33.2 years (SD=8.3 years). Regarding the marital status, 66% were married or in stable unions, 6% were legally separated or divorced and 28% were single. The father was cited by 30% of the participants as the secondary caregiver, the grandmother was mentioned by 17% and 20% of the participants reported having no secondary support at all.
Economic impoverishment was present among the majority of the caregivers. In this sense, the results showed that in 85% of the cases, the families received some kind of government financial support such as the Benefício de Prestação Continuada or the Programa Bolsa Família. The main demographic characteristics of the caregivers and of the children are described in Table 1.
The total score obtained with the ESSS indicated that only 1% of the caregivers reported low social satisfaction, while 37.6% were evaluated with medium satisfaction and 61.4% with high social satisfaction. In general, the caregivers were satisfied with the support received.
Regarding the means of the percentages presented in each dimension of the ESSS, it was observed that the lowest score (56%) was in the social activities dimension, followed by intimate satisfaction (65%), satisfaction with friends (74%) and satisfaction with family (87%), which presented the highest level of satisfaction.
The dimensions investigated by the ESSS were correlated with the sociodemographic characteristics of the participants. A significant correlation was found between the results in the social activities dimension and the answers given in the marital status item, showing that the married/stable union caregivers were more satisfied with their social activities than the unmarried ones (p=0.001). The results in the intimacy dimension also correlated with the answers given regarding the marital status, however, the level of significance was close to the level of acceptance (p=0.077). These data indicate that married caregivers present greater satisfaction regarding intimacy when compared to separated and single caregivers.
In addition to marital status, there was a significant correlation between declared incomes and results in the intimacy dimension (p=0.092, a value close to the acceptance limit), showing that higher incomes were associated with higher satisfaction in the intimacy dimension.
Characteristics of children with CP and the scores of MOS and ESSS
Pearson's correlation was used to measure the relationship between the ages of the children and the five degrees of the GMFCS with the scores of the protocols. The Correlation Test was used to validate the correlations. The highest correlation occurred between the ages of the children and the responses given in the Information dimension (MOS-SSS) with a value of -33.4%. This value, because it is negative, indicates that the higher the age, the lower the Information score.
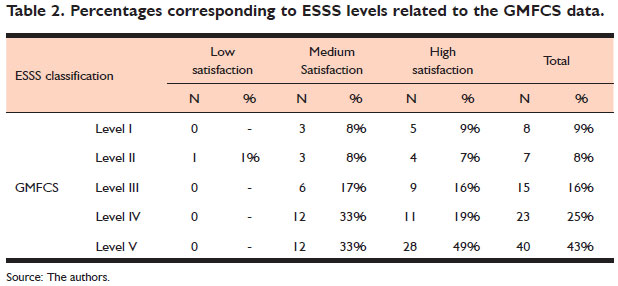
The general social satisfaction scores were correlated with the GMFCS levels. Table 2 presents the percentages found.
It can be observed in Table 2 that the majority of the caregivers of children evaluated in Level V demonstrated high satisfaction with the social support (49%), indicating that the parents of children with greater compromise were more satisfied. This was followed by medium satisfaction among the caregivers of children evaluated at level IV and V (33% each).
The analysis of the frequency of responses obtained in the ESSS dimensions revealed that the caregivers of very compromised children (IV and V) had lower levels of satisfaction in the intimacy dimension. On the other hand, the caregivers of children assessed at levels I and III exhibited higher levels of satisfaction in the social activities dimension, and the former also revealed high levels of satisfaction with friends and family.
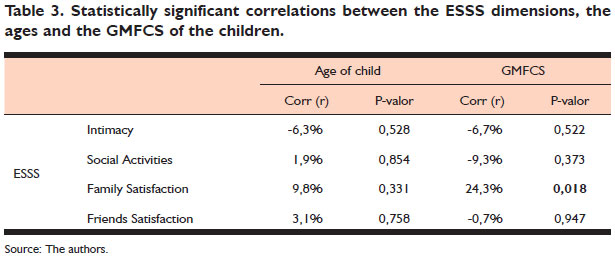
Table 3 presents the correlations between the characteristics of the children and the perception of social satisfaction of the caregivers. The dimensions of the ESSS were correlated with the characteristics of age and GMFCS levels.
The only significant correlation occurred between the responses obtained in the satisfaction with the family dimension and the GMFCS levels, being positive, indicating, therefore, that the caregivers of more compromised children reported greater satisfaction with the social activities performed in the family.
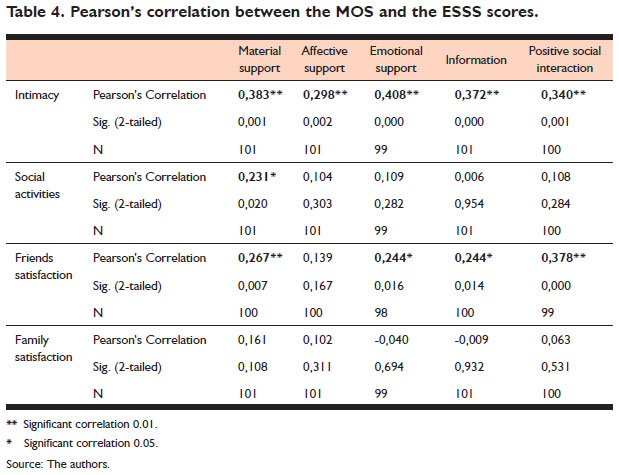
In order to explore possible relationships between the dimensions of social satisfaction and the dimensions of the support received by the caregivers, Pearson's correlation was used. Table 4 shows the crossing of social support and social satisfaction.
There were correlations between the responses to the Intimacy dimension and all the results of the MOS dimensions (material support, affective support, emotional support, informational support and positive social interactions). The responses pertaining to the social activities dimension were correlated with those found in material support, while the results involving satisfaction with friends were related to greater material support, emotional support, informational support and positive social interaction.
Discussion
The sample consisted of caregivers, mostly mothers, who reported their occupation as being "at home", a condition that requires the presence of social support, considering that mothers taking the role of primary caregivers end up giving up their careers, exclusively occupying themselves with care for the child with CP (Gallagher & Whiteley, 2012; Thurston et al., 2011). In addition, the social data showed that the mothers lived in contexts of economic impoverishment, emphasizing the need for different types of support in order to guarantee the maintenance of their well-being in the difficult routine of caring for their children (Araújo et al., 2013; Siqueira, Betts, & DellÁglio, 2006). Faced with the scenario of impoverishment associated with intensive care, the importance of the measures related to health and well-being, such as social satisfaction, was discussed, relating it to the characteristics of the caregivers. In this sense, it was observed that the married/stable union caregivers presented higher rates of social satisfaction. These results indicate the importance of the companion's presence, considering the sharing in different levels of support, as well as the benefit generated by the activities and affective exchanges (Araújo et al. 2013; Britner et al., 2003).
These findings reinforce the results of other studies regarding the analysis of families of children with CP: that marital satisfaction and social support have been shown to be strong indicators of good family functioning (Britner et al., 2013). Thus, caregivers that are more satisfied with their partners tend to feel more supported and effective in their care tasks (Araújo et al., 2013; Thurston et al., 2011).
Regarding the different types of satisfaction, it was observed that in the intimacy dimension the responses found were positively related to all the types of support of the MOS scale. The low values indicated that although the answers pertaining to the intimate satisfaction dimension were related to the types of support investigated, they did not occur exclusively, being explained by other factors considering that it is a perceptual phenomenon (Santos, Pais-Ribeiro & Lopes, 2003). However, it can be affirmed that the presence of these types of support positively favored the perception of greater social satisfaction mainly in the intimacy aspect.
The data showed that feeling more satisfied, especially regarding intimacy, was related to more types of support. This finding shows that despite the lack of support and material aid, the caregivers reported that they were satisfied with friends and family, showing high scores for total social satisfaction.
Good general social satisfaction was evident in the results, mainly among the caregivers of children evaluated as being more compromised (level V of the GMFCS), which contradicts the data found by Kurtuncu et al. (2014) and Alaee et al. (2014), who found that caregivers of more compromised children with CP felt less satisfied with the support. In addition, among the dimensions analyzed, satisfaction with the family was significantly more present, suggesting that positive characteristics mark the families of children with CP, empowering them and making them more competent in the exercise of their functions in the context of the disability (Gallagher & Whiteley, 2012; Thurston et al., 2011).
The caregivers of children with more severe levels of compromise that were more satisfied could rely on a supportive network of family and friends able to support them in their various needs. The levels of impairment of the disability indicated, therefore, a greater need for social support, failing to present themselves as merely dysfunctional aspects (Araújo et al., 2013, Britner et al., 2013). From this perspective, the increased compromises of the children demanded greater social support, made available to caregivers in order to meet their real needs.
Social satisfaction is an important regulator of emotional balance, which is capable of alleviating the perception of economic and social difficulties experienced by caregivers and is therefore associated with higher levels of well-being (Gallagher & Whiteley, 2012; Thurston et al., 2011). It presents itself as an important resource in the analyses regarding the social support networks and has its main source in the family.
Final considerations
It is hoped that this work will contribute to the studies about the caregivers of children with CP, highlighting their needs and helping in the comprehension of the psychological mechanisms that are involved in the care for children with these specificities. One limitation of the study is the fact that it was carried out only with parents of children with CP. In the future this could be extended to parents of children with typical development, deepening the comparative analysis. Furthermore, it was carried out in a single state, with the recommendation that it should be replicated in other regions.
It is considered that not all the objectives were achieved, as the use of perceptive scales was found to be limited for the access of perceptual phenomena such as satisfaction. However, it is hoped that this will encourage perspectives that take into consideration studies based on family resources, favoring the generation of resources such as counseling or support groups for parents. This would deepen the analyses regarding the benefits provided by the various emotional support networks.
References
Alaee, N., Shahboulaghi, F. M., Khankeh, H., & Kermanshahi, S. M. K. (2014). Psychosocial challenges for parents of children with cerebral palsy: a qualitative study. Journal of Child and Family Studies, 24,2147-2154. doi:10.1007/s10826014-0016-3 [ Links ]
Al-Gamal, E., & Longo, T. (2013). Psychological distress and perceived support among Jordanian parents living with a child with cerebral palsy: a cross-sectional study. Scandinavian Journal of Caring Sciences, 27,624-631. doi:10.1111/j.1471-6712.2012.01071.x [ Links ]
Araújo, Y. B., Reichert, A. P. da S., Vasconcelos, M. G. L., & Collet, N. (2013). Fragilidade da rede social de famílias de crianças com doença crônica. Revista Brasileira de Enfermagem, 66(5),675-681. Recuperado em 19 maio, 2018, de http://www.redalyc.org/articulo.oa?id=267028883006 [ Links ]
Britner, P., Morog, M., Pianta, R., & Marvin, R. (2003). Stress and coping: a comparison of self-report measures of functioning in families of young children with cerebral palsy or no medical diagnosis. Journal of Child and Family Studies, 12(3),335-348. doi:10.1023/A:1023943928358 [ Links ]
Cury, V. C. R., & Brandão, M. de B. (2011). Reabilitação em paralisia cerebral. Rio de Janeiro: MedBook. [ Links ]
Gallagher, S., & Whiteley, J. (2012). Social support is associated with blood pressure responses in parents caring for children with development disabilities. Research in Developmental Disabilities, 33,2099-2105. doi:10.1016/j.ridd.2012.06.007 [ Links ]
Griep, R. H., Chor, D., Faerstein, E., Werneck, G. L., & Lopes, C. S. (2005). Validade de constructo de escala de apoio social do Medical Outcomes Study adaptada para o português no Estudo Pró-Saúde. Cadernos de Saúde Pública, 21(3),703-714. doi:10.1590/S0102-311X2005000300004 [ Links ]
Huang, Y.-P., Kellett, U. M., & St John, W. (2010). Cerebral palsy: experiences of mothers after learning their child's diagnosis. Journal of Advanced Nursing, 66(6),1213-1221. doi:10.1111/j.1365-2648.2010.05270.x [ Links ]
Huang, Y.-P., Kellett, U. M., & St John, W. (2012). Being concerned: caregiving for Taiwanese mothers of a child with cerebral palsy. Journal of Clinical Nursing, 21,189-197. doi:10.1111/j.1365-2702.2011.03741.x [ Links ]
Kurtuncu, M., Akhan, L. U., Yildiz, H., & Demirbag, B. C. (2014). Experiences shared through the interviews from fifteen mothers of children with cerebral palsy. Journal Sexuality and Disability, 33(3)349-363. doi:10.1007/s11195-014-9373-5 [ Links ]
Palisano, R., Rosenbaum, P., Walter, S., Russell, D., Wood, E., & Galuppi, B. (1997). Development and validation of a gross motor function classification system for children with cerebral palsy. Developmental Medicine and Child Neurology, 39,214-223. doi:10.1111/j.1469-8749.1997.tb07414.x [ Links ]
Ribeiro, J. L. P. (1999). Escala de Satisfação com o Suporte Social (ESSS). Análise Psicológica, 3,547-558. [ Links ]
Russell, D., Rosenbaum, P. L., Avery, L. M., & Lane, M. (2011). Medida da função motora grossa GMFM-66 & GMFM-88: manual do usuário. São Paulo: Memnon. [ Links ]
Santos, C., Pais-Ribeiro, J., & Lopes, C. (2003). Estudo de adaptação da Escala de Qualidade de Vida do Familiar/Cuidador do Doente Oncológico (CQOLC). Revista Portuguesa de Psicossomática, 5(1),105-118. Recuperado em 24 maio, 2018, de http://www.redalyc.org/articulo.oa?id=28750112 [ Links ]
Saranson, B. R., Saranson, I. G., & Pierce, G. R. (1990). Social support: an international view. New York: John Wiley & Sons. [ Links ]
Silva Júnior, M. D., Brito, R. C. S., & Beltrão, M. C. de M. (2010). Fatores interpessoais das redes sociais de parentesco. Ciências & Cognição, 15(3) 100-110. Recuperado em 24 maio, 2018, de http://pepsic.bvsalud.org/scielo.php?script=sci_arttext &pid=S1806-58212010000300010 [ Links ]
Siqueira, A. C., Betts, M. K., & Dell'Aglio, D. D. (2006). A rede de apoio social e afetivo de adolescentes institucionalizados no Sul do Brasil. Revista Interamericana de Psicología/Interamerican Journal of Psychology, 40(2),149-158. Recuperado em 19 maio, 2018, de http://www.redalyc.org/articulo.oa?id=28440202 [ Links ]
Thurston, S., Paul, L., Loney, P., Ye, C., Wong, M., & Browne, G. (2011). Associations and costs of parental symptoms of psychiatric distress in a multi-diagnosis group of children with special needs. Journal of Intellectual Disability Research, 55(3),263-280. doi:10.1111/j.1365-2788.2010.01356.x [ Links ]
Zanini, D. S., Verolla-Moura, A., & Queiroz, I. P. de A. R. (2009). Apoio social: aspectos da validade de constructo em estudantes universitários. Psicologia em Estudo, 14(1),195-202. doi:10.15448/1980-8623.2016.3.23098 [ Links ]
 Mailling address:
Mailling address:
Tatiana Afonso
Rua Alegre 156, apto. 143 bl. 01, bairro Santa Paula
São Caetano do Sul, SP, Brazil
E-mail: afonso_tatiana@hotmail.com
Submission: 11.7.16
Acceptance: 2.19.18

{kind=link}
{kind=link}
{kind=link}
{kind=link}