










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Curriculum ScienTI
Curriculum ScienTIIndicadores
Compartilhar

 Permalink
PermalinkSMAD. Revista eletrônica saúde mental álcool e drogas
versão On-line ISSN 1806-6976
SMAD, Rev. Eletrônica Saúde Mental Álcool Drog. (Ed. port.) vol.11 no.4 Ribeirão Preto dez. 2015
https://doi.org/10.11606/issn.1806-6976.v11i4p224-233
ARTIGO ORIGINAL
DOI: 10.11606/issn.1806-6976.v11i4p224-233
Adherence to drug treatment regarding the users of psychosocial attention centers with mood disorders and schizophrenia1
Adhesión al tratamiento medicamentoso de los usuarios de centros de atención psicosocial con trastornos de humor y esquizofrenia
Ana Carolina ZagoI; Elaine TomasiII; Carolina Carbonell DemoriIII
IMSc, Adjunct Professor, Universidade da Região da Campanha, Bagé, RS, Brazil
IIPhD, Adjunct Professor, Universidade Federal de Pelotas, Pelotas, RS, Brazil
IIIDoctoral student, Universidade Federal de Pelotas, Pelotas, RS, Brazil. Adjunct Professor, Universidade da Região da Campanha, Bagé, RS, Brazil
ABSTRACT
The objective was to identify the prevalence and factors associated with non-adherence to psychiatric medication among users of Psychosocial Attention Centers. Dealing with a cross-sectional study, sheltering a prospective cohort of 563 users of Psychosocial Attention Centers in Pelotas. Household interviews were conducted and two questionnaires were applied. The prevalence of lack of accession was 32%, without significant differences according to gender, income, time of illness, diagnosis and type of medicine. Young individuals with higher education, with a partner, less frequent at the Psychosocial Attention Centers and with adverse effects, were least adherent to treatment. The lack of adhesion of the participants is mainly related to the adverse effects. Health policies need to focus on addressing this issue, proposing new strategies of adherence to treatments.
Descriptors: Cumplimiento de la Medicación; Esquizofrenia; Trastornos del Humor.
RESUMEN
La finalidad fue identificar la prevalencia y factores asociados a la no adhesión a medicamentos psicofármacos entre usuarios de los Centros de Atención Psicosocial. Se trata de estudio trasversal, anidado a una cohorte prospectiva con 563 usuarios de los Centros de Atención Psicosocial de Pelotas. Fueron desarrolladas entrevistas domiciliares y aplicados dos cuestionarios. La prevalencia de la falta de adhesión fue del 32%, sin diferencia significativa según el género, renta, tiempo de enfermedad, diagnóstico y tipo de medicamento. Individuos jóvenes, con mayor escolaridad, con compañero, con menor frecuencia a los Centros de Atención Psicosocial y con efectos adversos fueron menos adherentes al tratamiento. La falta de adhesión de los participantes está principalmente relacionada a los efectos adversos. Las políticas de salud necesitan dedicarse al enfrentamiento de ese problema, proponiendo nuevas estrategias de adhesión a los tratamientos.
Descriptores: Medication Adherence; Schizophrenia; Mood Disorders.
Introduction
Psychiatric attention went through profound changes in many countries, including Brazil. These changes culminated in 2001 with the enactment of law No. 10.216, known as the law of the Psychiatric Reform and a ban on the construction of new psychiatric hospitals in the country. The law stipulates that people with mental disorders should be treated preferentially in community services(1), i.e. different substitute services to psychiatric hospitals united themselves, so as to constitute a set of references with ability to absorb and accommodate individuals in distress.
The care at Psychosocial Attention Centers -CAPS include, in addition to individual and group care and therapeutic workshops, the dispensation of medicines free of charge to its users(2). Therefore, it is necessary that there is patient compliance to the prescribed drug regimen, in order to ensure greater effectiveness of the therapy. According to the World Health Organization (WHO, 2003), treatment adherence refers to the extent to which patients accept and follow the recommendations of doctors or other health professionals regarding the use of a particular therapy(3). On average, the non-adherence in psychiatric disorders is around 50%(4). Among psychiatric diseases seen in CAPS are mood disorders and schizophrenia. Mood disorders include manic episodes, depressive episodes, bipolar affective disorder, various types of depression and other affective disorders(5). These are highly prevalent diseases, preferably treated with antidepressants and mood stabilizers. Schizophrenia is a disorder of chronic evolution that requires prolonged treatment with the use of antipsychotics. Membership is critical to the success of the treatment, since there is an association between the failure and recurrences, rehospitalizations and persistence of psychotic symptoms(6).
In relation to the drugs used in the treatment of these diseases, these cause numerous side effects, ranging from autonomic symptoms - dry mouth, urinary retention and postural hypotension - until symptoms in the central nervous system - sedation or insomnia, increase or decrease of appetite, dizziness, agitation, irritability, decreased reasoning, reduction of reflexes, tremors, among others(2). Previous studies, conducted in several countries, as factors associated with the lack of membership in mood disorders and Schizophrenia: adverse effects of medicines(7-8), young age(4.7), low-income(9), oblivion(4.7), find that the medication is unnecessary(7) and were reluctant to take the prescribed medication(7).
Therefore, this study aimed to identify the prevalence and factors associated with medication non-adherence of psychiatric drugs among users of Psychosocial Attention Centers in Pelotas, RS, with mood disorders and schizophrenia.
Materials and methods
This study it outlined in a cross-sectional design with a prospective cohort. The individuals were identified and included in the cohort from the records of seven CAPS, where also the address of residence was obtained. The second follow-up, where the data of this article originated, occurred from May to August 2007. Household interviews were conducted by a team of scholars of Psychology and Social work (UCPEL) and Nursing (UFPEL), selected and trained, after the pilot study. All the users of the seven CAPS of Pelotas were included in this study found in the second monitoring with a diagnosis of schizophrenia (ICD-10 F 20.0 F 29.9) and mood disorders (ICD-10 F 30.0 to 39.9 F). In this study, all data were collected directly with the carriers of these diseases. After the signing of the informed consent, users answered two questionnaires. The first contained general information about users and their treatments and the second contained specific information on each psychotropic medicine used. For each of these instruments a manual has been prepared to standardize data collection.
The survey was conducted within the standards required by the Declaration of Helsinki and approved by the Research Ethics Committee of the Catholic University of Pelotas (Protocol 20.051, 14th of December 2005).
The test of Morisky(10) was used to measure the lack of membership, divided into intentional and unintentional. Regarding the first, the questions were: 1) When you feel well, do you sometimes not take your medicine? 2) When you feel bad with the medicine, do you sometimes stop taking it? Because of the lack of non-intentional adherence, the questions were: 1) Do you ever forget to take your medication? 2) Are you sometimes careless regarding the time of taking your medicine? The dependent variable was "lack of adherence", disregarding the intention. The independent variables studied were gender, age, education, income per capita, living with a partner, time of diagnosis, type of disorder, time of CAPS, type of used medicine, access to medicines, reporting of adverse effects and the number of adverse effects. In addition, information was obtained about the need to use daily medication, and if the patient didn’t use in the 15 days prior to the interview and the reasons for it.
The diagnosis (ICD-10), the time of CAPS and service-intensive, semi-intensive and not-intensive were obtained from medical records and information on hospitalizations were collected with the relatives. Other information used in these analyses was provided directly by users of the CAPS. After coding, tabulation and reviewing, two entries independent of the instruments were held in Epi Info 6.04 program, whose structure was prepared for the verification of size and consistency. After the final edition of the database, this was converted to the statistical package Statistical Package for the Social Science (SPSS), 13.0, in which analyses were made. The Chi-square test was used for the verification of differences between proportions, considering the statistical significance level of 5%, Also calculated were the prevalence and confidence intervals of 95%.
Results
In the follow-up visit, 563 users of CAPS were included, of which 201 had a diagnosis of schizophrenia (36%) and 362 had mood disorder (64%). That sample matched the 74% of users with schizophrenia and 80% of users with mood disorders, identified in the baseline study.
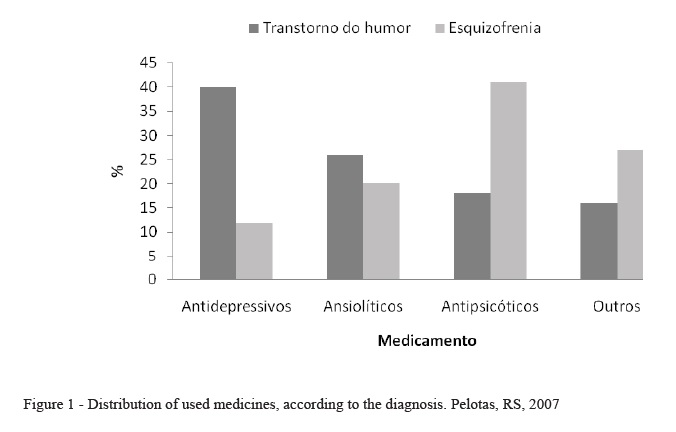
The average age of respondents was 47 years, ± 12 years of standard deviation (SD). Regarding the sex, 66% were female and approximately 73% of the people were white. As for the marital status, 47% of respondents reported to having a partner. The average education was 5.1 years (SD = 3.4). The average per capita income in minimum wages (SM) was 1.2 (SD = 1.2). The disease was, on average, 15.8 years (SD = 14.8). The average time of treatment in CAPS, according to the chart of the respondents, was 3.6 years (SD = 1.9). Almost all users (95%) used some type of medicine. In total, the use of medicines mentioned is 1418 for the 15 days preceding the interview, averaging 2.7 drugs per user (SD = 1.5). About 20% of individuals reported not having free access to all the drugs and the main reasons were the non-availability of the drug CAPS and financial difficulties to acquire them. Of the total medicines used, 30% were antidepressants, 26% antipsychotics, 24% anti-anxiety drugs and 20% other medicines. The medicines used by users with mood disorder, 40% were antidepressants, 26% anti-anxiety drugs, 18% antipsychotics and 16% other drugs. Already in relation to users with schizophrenia, 41% were antipsychotics, 20% anxiolytics, 12% antidepressants and 27% other drugs (Figure 1).
About one third (33%) of the medicines examined showed some adverse effects: 22% of medicines presented only one, 9% presented two and 2% presented three or more adverse effects. The anti-anxiety drugs were responsible for 38% of such effects and the most often reported were: very sleepy (19%), hungry (9%), insomnia (6%) and decreased appetite (5%). In addition to these, also were reported dry mouth, stomach problems, digestive problems, apathy, agitation and tremors.
Considering all the drugs studied, the lack of total membership was 32%, respectively 9% intentionally and 28% unintentionally (Figure 2). It was observed that, regarding medicines, 71 users have reported both types of non-adherence, which explains the 5% more lack of membership in the sample (Figure 2).
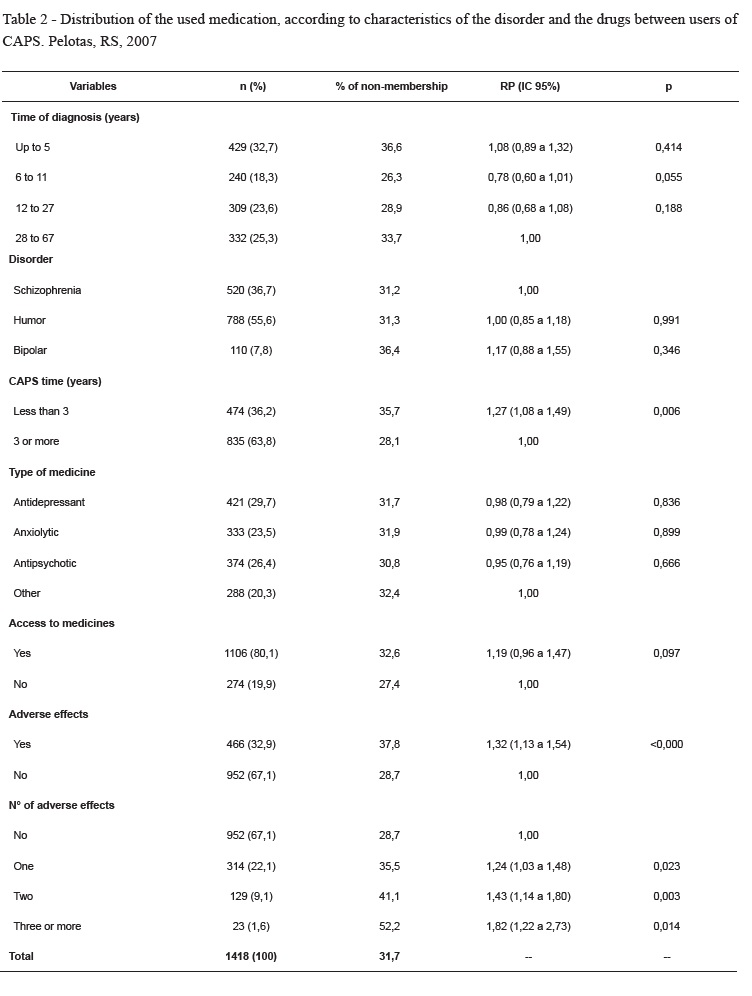
There was no significant difference in the prevalence of lack of total membership according to the genre, per capita income, the disease, the diagnosis and the type of medicine. Highlights include a tendency to greater lack of adherence among patients with bipolar disorder. Individuals between 17 and 29 years showed 71% higher prevalence of lack of adherence to treatment, when compared with those of 60 years or more. The highest educational level was also significantly associated with, because individuals with complete elementary school presented a higher lack of membership 28% than those with less study time (Table1). Users with less than three years frequenting CAPS had 27% more lack of adhesion than with increased frequency. The medicines for which there were reports of adverse effects had less support. Observed was the greater the number of adverse effects, the lower the membership was, reaching 82% with a greater lack of adhesion between who mentioned three or more effects (Table 1).
With these results, it was necessary to investigate the association between these variables with the objective of finding potential confounding factors. Schooling and frequency to the CAPS have not been associated with the occurrence of adverse effects, however, the age is associated with the largest account among the youngsters. Stratified for age analysis revealed that the occurrence of adverse effects can only be associated with the lack of adherence to the age groups intermediates, i.e. between 30 and 59 years. For the young and old, adverse effects aren’t associated with the lack of membership.
Discussion
In Brazil, only few studies have been realized on treatment adherence, conducted with users of the CAPS. Some of the findings refer mainly to the abandonment of treatment and fouls the appointments in primary and secondary services from public, in certain regions of the country(11-12). There are researches which evaluated treatment adherence in specific psychiatric disorders such as depression, bipolar disorder and schizophrenia(4, -16 7.13). The prevalence of lack of membership was of 32% for users of CAPS of Pelotas with schizophrenia and mood disorders, similar to that found in a study by the United Kingdom with 634 patients with psychiatric diseases was 34.2%(17). A sample of 223 patients with bipolar disorder showed 30% of low treatment adherence(18). Another study, conducted with patients with bipolar disorder, found 46% of non-adherence to treatment(19). Sajatovic et al.(20) researched lack of membership in 323 patients with bipolar disorder, and found that among the 22% of non-members are those who stopped taking or have taken less than 50% of the prescribed medication. Lanouete et al.(9) researched 17studies not-adherence with psychotropic drugs, and realized that 41% of Latin-Americans, 31% of Euro-Americans and 43 percent of African Americans do not adhere to treatment.
In a study with 6201 psychotropic users in Canada, the prevalence of lack of membership of individuals who used antipsychotics, sedatives, anxiolytics, antidepressants and mood stabilizers ranged from 34.6 to 45.9%(4).
Although the test of Morisky was already available for over two decades, he has been widely used to research membership in other pathologies and the only study found was that of Copeland and associates(19) who have studied patients with bipolar disorder.
Clatworthy et al.(18) found that the relationship between gender and lack of adhesion and between age and lack of accession were not significant. Bulloch and Patten(4) also did not observe an association between lack of accession and gender for any of the classes of drugs studied. Sawada et al.(17) reported better performance of antidepressant therapy for men. Users of the CAPS with higher education (eight years or more) joined 28% less compared to those of lower educational level. Cooper et al.(7) reported that the socio-demographic variables were not significantly associated with lack of adherence to treatment. In a study with Latino’s living in the United States, low socioeconomic status was related to lack of adherence to treatment(9).
The example of Bulloch and Patten(4) and Cooper and colleagues(7), in Pelotas also lack of adherence was highest among younger people. A possible explanation is that more young people could be more involved in productive activities and have a sex life more active than the older ones, which, in both cases, the adverse effects of the drugs would be most undesirable.
Users with partner joined 27% less in relation to the treatment which had no partner. A case scenario would be that these individuals had a greater emotional support and, therefore, do not feel the need to take the prescribed medication, and another possible explanation would be that some psychotropic drugs can cause sexual dysfunction, negatively affecting the marital relationship(21).
About one third (33%) of the medicines examined showed some adverse effects. Studies with schizophrenic patients showed adverse effects as the reason not to adhere to treatment(14). Kikert et al.(8) conducted a study in four countries in Europe with schizophrenic patients and reported that 21% of them justified its lack of membership as a result of the adverse effects. Cooper et al.(7) showed adverse effects as one of the reasons that patients who use psychotropic drugs stop taking them, while 14.2% reported such reason.
Final Considerations
In addition, recall bias limitation that can be present in any cross-sectional study, the prevalence of lack of membership herein may have been affected by a deficit of additional memory due to the characteristics of the sample and information directly referred to by the user. Particularly for those with schizophrenia, there may have been sub-related of non-membership, since one of the features of the disease is the distortion of reality.
Another limitation of the study is related to the fact that if you restrict to a particular group of subjects surveyed, both in geographical terms and include only individuals found on the second visit. Subsequent studies can shed light on the treatment adherence of Psychosocial Attention Centers users of other cities, as well as of individuals not linked to CAPS.
Once the drug therapy is an integral part of the attention to the bearer of distress within the SUS, it is important to assess whether users of the CAPS are really fulfilling the medical recommendations and using prescription medicine, since this is a way to optimize costs, avoid relapses and decrease the number of hospitalizations, all of them paid with public funds.
Some ways to improve adherence to treatment are linked to a healthy professional relationship with the patient, as in the case of information on the medications used, their benefits and side effects, as well as the possible replacement in case of non-acceptance by the patient.
References
1. Antunes SM, Queiroz MS. A configuração da reforma psiquiátrica em contexto local no Brasil: uma análise qualitativa. Cad Saude Publica 2007; 23(1):207-15. [ Links ]
2. Brasil. Saúde Mental no SUS: acesso ao tratamento e mudança do modelo de atenção. Relatório de Gestão 2003-2006. Brasília: Ministério da Saúde, Secretaria de Atenção à Saúde/DAPE; 2007. [ Links ]
3. World Health Organization. Adherence to long term therapies: evidence for action. Geneva: WHO Library Cataloguing-in-Publication Data; 2003. [ Links ]
4. Bulloch AG, Patten SB. Non-adherence with psychotropic medications in the general population. Soc Psychiatry Psychiatr Epidemiol 2009;45(1):47-56. [ Links ]
5. Amaral RA, Malbergier A, Andrade AG. Manejo do paciente com transtornos relacionados ao uso de substância psicoativa na emergência psiquiátrica. Rev Bras Psiquiatr. out 2010; 32(supl.2):104-11. [ Links ]
6. Vedana KGG, Miasso AI. A interação entre pessoas com esquizofrenia e familiares interfere na adesão medicamentosa? Acta paul. enferm. 2012; 25(6):830-6. [ Links ]
7. Cooper C, Bebbington P, King M, Brugha T, Meltzer H, Bhugra D, et al. Why people do not take their psychotropic drugs as prescribed: results of the 2000 National Psychiatric Morbidity Survey. Acta Psychiatr Scand 2007; 116(1):47-53. [ Links ]
8. Kikkert MJ, Schene AH, Koeter MW, Robson D, Born A, Helm H, et al. Medication adherence in schizophrenia: exploring patients’, carers’ and professionals’ views. Schizophr Bull 2006; 32(4):786-94.
9. Lanouette NM, Folsom DP, Sciolla A, Jeste DV. Psychotropic medication nonadherence among United States Latinos: a comprehensive literature review. Psychiatr Serv 2009; 60(2):157-74. [ Links ]
10. Morisky DE, Green LW, Levine DM. Concurrent and predictive validity of a self-reported measure of medication adherence. Med Care 1986; 24(1):67-74. [ Links ]
11. Melo AP, Guimaraes MD. Factors associated with psychiatric treatment dropout in a mental health reference center, Belo Horizonte. Rev Bras Psiquiatr 2005; 27(2):113-8. [ Links ]
12. Ribeiro MS, Poço JLC. Motivos referidos para abandono de tratamento em um sistema público de atenção à saúde mental. Rev APS 2006; 9(2):136-45. [ Links ]
13. Miasso AI, Monteschi M, Giacchero KG. Bipolar affective disorder: medication adherence and satisfaction with treatment and guidance by the health team in a mental health service. Rev. Latino-Am. Enfermagem 2009;17(4):548-56. [ Links ]
14. Nicolino Paula Silva, Vedana Kelly Graziani Giacchero, Miasso Adriana Inocenti, Cardoso Lucilene, Galera Sueli Aparecida Frari. Esquizofrenia: adesão ao tratamento e crenças sobre o transtorno e terapêutica medicamentosa. Rev. esc. enferm. USP 2011; 45(3):708-15. [ Links ]
15. Ribeiro MS, Alves MJM, Vieira EMM, Silva PM, Lamas CVD. Fatores associados ao abandono de tratamento em saúde mental em uma unidade de nível secundário do Sistema Municipal de Saúde. J Bras Psiquiatr 2008; 57(1):16-22. [ Links ]
16. Santin A, Cereser K, Rosa A. Adesão ao tratamento no transtorno bipolar. Rev Psiquiatr Clin 2005; 32(Suppl. 1):105-9. [ Links ]
17. Sawada N, Uchida H, Suzuki T, Watanabe K, Kikuchi T, Handa T, et al. Persistence and compliance to antidepressant treatment in patients with depression: a chart review. BMC Psychiatry 2009; 16:9-38. [ Links ]
18. Clatworthy J, Bowskill R, Parham R, Rank T, Scott J, Horne R. Understanding medication non-adherence in bipolar disorders using a Necessity-Concerns Framework. J Affect Disord 2009; 116(1-2):51-5. [ Links ]
19. Copeland LA, Zeber JE, Salloum IM, Pincus HA, Fine MJ, Kilbourne AM. Treatment adherence and illness insight in veterans with bipolar disorder. J Nerv Ment Dis 2008; 196(1):16-21. [ Links ]
20. Sajatovic M, Bauer MS, Kilbourne AM, Vertrees JE, Williford W. Self-reported medication treatment adherence among veterans with bipolar disorder. Psychiatr Serv 2006; 57(1):56-62. [ Links ]
21. Costa AM, Lima MS, Mari Jde J. A systematic review on clinical management of antipsychotic-induced sexual dysfunction in schizophrenia. Sao Paulo Med J 2006; 124(5):291-7. [ Links ]
Received: Sep. 15th 2014
Accepted: Aug. 21st 2015
Corresponding Author:
Carolina Carbonell Demori
Universidade da Região da Campanha
Av. Tupy Silveira, 2099 Centro
CEP: 96400-110, Bagé, RS, Brasil
E-mail: carolinaufsm@hotmail.com
1 Paper extracted from master’s thesis "Adesão ao tratamento medicamentoso dos usuários dos CAPS em Pelotas, RS, com transtornos de humor e esquizofrenia", presented to Universidade Católica de Pelotas, Pelotas, RS, Brazil.


{kind=link}
{kind=link}
{kind=link}
{kind=link}