










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores
Compartilhar

 Permalink
PermalinkSMAD. Revista eletrônica saúde mental álcool e drogas
versão On-line ISSN 1806-6976
SMAD, Rev. Eletrônica Saúde Mental Álcool Drog. (Ed. port.) vol.11 no.4 Ribeirão Preto dez. 2015
https://doi.org/10.11606/issn.1806-6976.v11i4p234-42
ARTIGO ORIGINAL
DOI: 10.11606/issn.1806-6976.v11i4p234-42
Depression among pregnant women at the end of pregnancy
La depresión en gestantes al final del embarazo
Valéria Feitosa de Sousa MouraI; Luiz Jorge PedrãoII; Adrielle Cristina Silva SouzaIII; Rafaela Peres BoaventuraIII
IMSc, RN, Hospital e Maternidade Dona Regina, Palmas, TO, Brazil
IIProfessor, Escola de Enfermagem de Ribeirão Preto, Universidade de São Paulo, PAHO/WHO Colaborating Centre for Nursing Research Development, Ribeirão Preto, SP, Brazil
IIIDoctoral Students, Faculdade de Enfermagem, Universidade Federal de Goiás, Goiânia, GO, Brazil
ABSTRACT
The research can be described as a quantitative study which aimed to examine depressive patterns among pregnant women. Interviews were conducted as well as a Beck Depression Inventory, applied to 42 pregnant women with gestational age under 36 weeks. Obtained results: 17% of pregnant women had indicative signs of depression and 7% had dysphoria. During the research it was perceived that being 35 years or more, not having a partner, having a low family income, being black and having a job were risk factors and determinants for depression. None of the pregnant women who practiced recreational activities presented signs of depression, while 20.6% not enjoyed these activities showed depression. It is concluded that depression is a reality in the lives of pregnant women and prenatal care is important for the detection of these patterns.
Descriptors: Depression; Pregnant Women; Psychiatric Nursing.
RESUMEN
Se trata de un estudio cuantitativo con objeto de verificar la existencia de cuadros depresivos en embarazadas. Fueron llevadas a cabo entrevistas y aplicado el Inventario de Depresión de Beck a 42 embarazadas con edad gestacional igual o superior a 36 semanas. Fueron encontrados: el 17% de las embarazadas tenía señales indicativos de depresión y 7% disforia. Se percibió que edad de 35 años o más, no tener pareja, renta familiar baja, ser negra y poseer empleo fueron factores de riesgo determinantes para la depresión. Ninguna de las embarazadas que practicaba actividades de ocio presentó indicativos de depresión, mientras el 20,6% que no disfrutaba de estas actividades presentaba depresión. Se concluye que la depresión es una realidad en la vida de las embarazadas y el prenatal es importante para detectar estos cuadros.
Descriptores: Depresión; Mujeres Embarazadas; Enfermería Psiaquiatrica.
Introduction
Throughout history, the attendance of pregnant women was focused on the creation of the healthy newborn (NB), dealing with the physical and psychological needs of the mother(1) wasn’t part of the attendance. However, in recent times, the factors responsible for maternal mortality, such as the multiple births, low schooling, previous state of women’s health (especially malnutrition and anemia), pregnancy in adolescence and lack of family planning (orientation, in the case of pregnancy)(2).
Currently, a concern has risen regarding researching topics related to women’s health, paying attention to these issues, which are considered a priority by health teams, through the pursuit of strategies to provide better assistance to pregnant women. However, in Brazilian literature, few studies were found on the occurrence of mental disorders during pregnancy and puerperal period such as a depression(2).
Since ancient times there are records about depression, like the old testament’s account of the story of King Saul, one of the oldest, which describes the depressive syndrome, as well as the story of the suicide of Ajax in Homer’s Iliad. Approximately 400 BC, Hippocrates made the first reports of melancholy. In the late 19th and early 20th century, the studies developed by Kraepelin who contributed fundamentally to the characterization of moods as Nosological entities(3).
Pregnancy is a period of transition, part of the natural process of human development, which causes various transformations to the well-being of women, changing their psyche and their socio-family role(4).
As for the emergence of depression among women, the gravid-puerperal period has great incidence of mental disorders, therefore requiring special attention to maintain or recover the well-being of both the woman and the child, and to prevent future difficulties(4-5).
Pregnancy is a critical period in the life cycle of the woman, being a situation that involves profound transformations, characterized by physical, psychological and social changes. The postpartum is considered to be the period in which the distress can lead to depression, developing into a postpartum depression, manifested with varying intensity, becoming a factor that hinders the establishment of a secure bond between mother and child, interfering in future interpersonal relations(4).
Mental disorders in pregnancy, childbirth and the puerperium are not a homogeneous entity. These include disorders from transient patterns up to serious situations, that can lead to irreparable damage to the expectant mother, fetus and even to the partner(5).
In this way, it’s clear that the care provided by nursing team professionals is fundamental to the prevention or recovery from depression during pregnancy and period of great importance in the life of the woman. The nurse should advance guidance, continuously assess the mental health of the pregnant women and new mothers, offering therapeutic interventions of nursing. In addition referrals have to be made when the resolution is not within the reach of their professional competence, as a failure, even though small, can result in consequences whose gravity is hard to assume(5).
Therefore, this study shows importance from identifying the occurrence, the institutions and health professionals in order for them to develop strategies for the prevention and control of gestational depression, resulting in benefits to the quality of the service provided, avoiding costly expenses for the re-establishment of health and improving the service offered to the woman and family.
Thus, this study aimed to examine depressive patterns among pregnant women at the end of pregnancy, comparing pregnant women with and without signs of depression, with respect to the variables age, marital status, skin color, income, employment relationship, associated diseases, planned pregnancy and leisure activities.
Method
Quantitative study, descriptive and transversal type, based on primary data in order to evaluate the appearance of depressive symptoms among pregnant women. The present study was conducted in a low-risk maternity ward in the city of Ribeirão Preto, in the year 2008. The research consists of 42 pregnant women with gestational age equal or above 36 weeks, met in the prenatal consultation referred to motherhood, in a period of 15 days, established for the conduct of research. The delimitation of this period was due to the return to a weekly prenatal consultation, most were with the same patients, saturating the sample. Pregnant women were included who have agreed to participate in research, signing the free informed consent and, with gestational age equal or greater than 36 weeks, literate and completely filled two proposed data collection instruments: a questionnaire, built specifically for the purposes of this research, containing general information about the expectant mother and the Beck Depression Inventory(6-7) being one of the most accepted instruments, on hand for the assessment of the intensity of the depression in psychiatric patients, but aw well for detecting the possibility of depressive patterns in population considered normal(8).
There are different proposals for the cut-off points to distinguish the level of depression by using the Beck Depression Inventory(6). The guidelines are different for undiagnosed samples, scores above 15 to detect gender dysphoria and scores above 20 for depression. The data were processed manually, arranged in tables and analyzed by means of descriptive statistics, using a database of Microsoft Office Access 2003.
The project was assessed and approved by the Research Ethics Committee on Human beings of the nursing school in Ribeirão Preto, University of São Paulo and the pregnant women participants signed an informed consent (protocol number 0472/2006).
Results and discussion
When comparing pregnant women with and without signs of depression, it was found that 7% (3) of the pregnant women had gender dysphoria, understood as excessive pain, anguish, agony, agitation and restlessness and 17% (7) showed depression, defined as a demotion of mood, energy reduction and decreased activity(9).
In general, depression is a very common disease, affecting 10% to 20% of the population, and studies show that its incidence is increasing(10). An association has been pointed out between social support, depression and anxiety among pregnant women, applying the scale of depression of Edinburgh, 29.5% of women showed depressive symptomatology(11), concluding a larger number than the one found in the present study.
Pregnant women in the age between 16 and 39 years, pregnant teenagers between 16 and 19 years, 21% of the sample; young people, those between 20 and 34 years, 74% of the sample; and older, those with a gestational age of 35 years or more, 5% of the sample. Teenage pregnancy is associated with an increased risk of suicide, both during pregnancy and the postpartum period and at the same time, a higher incidence of depression(12).
In adolescence, all the women present accelerated growth of sexual characteristics and also face the steps of development, such as the establishment of the identity, development of sexual orientation, emancipation of the family and determining the professional goal. At this stage some of these situations can cause great stress and gestation is considered as an additional stress(13).
Crossing the age of pregnant women with depression, only 11.1% of teenagers had these signs. A higher risk of depression, according to the present research, is concluded for pregnant women above 35 years old, 50% of the sample. Similar data were found in a study, showing that depression was more common among pregnant women, adults with 46.5%, compared to adolescents, with 37.5%(4).
As for marital status, 46% of pregnant women had a common-law marriage, 31% was single, 21% was married and 2% was separated. Although 31% (13) being single, three (23.0%) of them had some partner, even living together, the other 10 (77%), didn’t have any type of partner offering support during this period.
In relation to pregnant women with indicative signs of depression and the presence of a partner, it was observed that 30% had no partner who showed depression, against 12.5% of those with a partner, that exhibited this disorder, as shown in Table 1. One of the risk factors most often associated with depression in pregnancy is the lack of partner or family and social support(14).
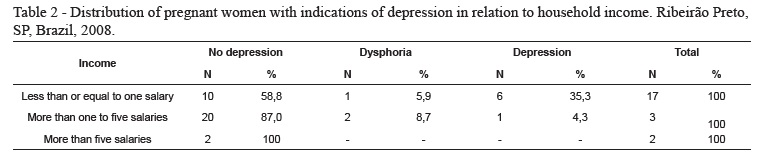
The maternity ward where the research was conducted is located in the outskirts and aimed to meet a population with low income, confirmed in this study. The majority of pregnant women surveyed, 54.7% (23), reported receiving between a minimum wage and five minimum wages, 40.5% (17) had a household income less than or equal to the minimum wage and only 4.7% (2) of pregnant women received more than five minimum wages.
As shown in Table 2, pregnant women with lower income, 35.3%, showed the risk of depression, while those with family income above five minimum wages did not have indications of depression. This result does not indicate that pregnant women with greater financial stability do not have depression. This fact could be due to sampling reduction in pay grade above five minimum wages, but in a way, to meet the results of another study, which showed that the risk factors most often be associated with depression among pregnant women with economic difficulties(14).
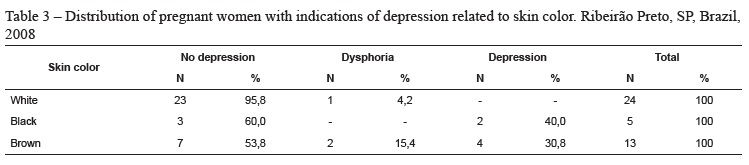
According to the skin color of pregnant women participating in the survey, the majority declared themselves as white, 57.1% (24), followed by brown, 31% (13), and black skin, 11.9%(4).
The prevalence of depression in pregnancy is greater among a group of low-income women, black and with low level of education(14), because the black women’s mental health is affected by its double condition; being black and woman(15). However, the exact incidence of depression among black women is not clear.
Regarding the relationship between the presence of indications of depression and skin color, 40% of pregnant black women showed depression, while no white nationals presented indications of depression, as shown in Table 3.
In the present study, 33.3% (14) of pregnant women worked outside the home, as shown in Table 4, and the other, 66.7% (28), were housewives. A variety of jobs was mentioned by pregnant women, such as: Maid; Cleaner of hotel rooms; Cashier; Nursing Assistant and Promoter.
In the comparison between depression and work, it was found that 21.4% of pregnant women who had a job had indications of depression, while the percentage of pregnant women who weren’t employed showed indications of depression was 14.3%.
Until the mid-twentieth century the values for women were getting married, have children, care for them and the husband and taking care of the household. Through a series of circumstances, among them events and situations caused by wars, women began to realize the capability of performing other tasks, and this changed other necessities, which resulted in other values(16).
Thus, the woman has regained its place in society and in the professional field, next to the man. However, many women were unable to "compromise" in its actions imposed by the development of the current context. Aware of their difficulties they suffer the impossibility to reconcile its traditional and professional functions entirely, feeling guilty in front of the husband, children and professional environment, reprimanding by their inability to harmonize all aspects involved in this situation. Before the accumulation of tasks it’s then susceptible to a series of internal crises and may develop into depression(16).
Table 4 shows that the accumulation of responsibilities can be a predisposing factor to the onset of a depression.
Important to note that this survey was conducted in a low-risk maternity, meaning that the majority of pregnant women did not present co-morbidities that exacerbate with pregnancy or would be triggered in this period, which could put both the life of the pregnant woman and the fetus at risk. Only two (5%) of the 42 pregnant women had some sort of disease, one said to have asthma and the other woman had hypertension and diabetes.
There is a high incidence of depression in patients admitted for non-psychiatric diseases. This type of depression goes unrecognized in many cases and is not being treated properly. Depression is found in all levels of severity of non-psychiatric diseases, although its intensity and frequency are larger among patients with a disease that is more severe. Studies suggest that about one third of patients hospitalized for psychiatric problems don’t report symptoms of mild to moderate depression and even one fourth can have a depressive illness. Thus, it’s common that a depression is accompanied by many other diseases(13).
In the present study, linking disease with indications of depression, it was observed that 50% of pregnant women who reported having some type of indications this psychopathology, as shown in Table 5, however, the sample of patients who reported having any disease was small, the fact that the motherhood of the study was low risk, further studies are needed with pregnant women at high risk for such confirmation.
To relate the occurrence of mental disorders with family history, four (9.52%) pregnant women claimed to have a family history of mental disorders, two reported that such disorders were depression and the other two didn’t know what the kinds of disorders were. However, relating family history of mental disorder with indications of depression, no association was observed, since the pregnant women who were in the family with these disorders showed no indications of depression.
The pattern of genetic inheritance occurs through complex mechanisms, being impossible to delete the psychosocial effects on the development of mental disorders, causative roles in the onset of mood disorders among some people(3,15).
The likelihood of having a mood disorder decreases according to the degree of relatedness(3). This fact may have occurred in the present study, since pregnant women have not beenquestioned about the relationship related to relatives who had any history of mental disorder. Other hypotheses may relate to family and social support of these pregnant women, which in addition to genetic factors, there are also the psychosocial factors influencing the development of depressive patterns, or, even, by the small number of pregnant women who have a family history of mental disorders.
Another topic studied in this research was the planning of pregnancy. In this respect, the results showed that 18 (42.86%) of pregnant women planned pregnancy and 24 (57.14%) didn’t plan, pointing out that most pregnant women didn’t plan their pregnancies. This fact does not favor the depression during pregnancy, in the present study, where pregnant women who didn’t plan the pregnancy showed no indications of depression, and only two that didn’t plan, showed gender dysphoria.
Many times the unplanned pregnancy is well accepted by the woman, preventing the development of depressive patterns. In addition, it should be noted, that the non-acceptance of pregnancy should not be equated to rejection of the child. The woman may not accept the pregnancy, but can feel love for the child who will be born(17) is not reported in this study because pregnant women were not questioned in relation to the acceptance of the child.
To relate the development of leisure practices disorder, only eight (19.5%) of pregnant women had some leisure activity, and were mentioned as leisure activities: reading, hiking, going to the movies and spending time with family. Leisure is a social necessity, whose purpose is to promote a relaxation stress compensator of society and the physical and mental wear and tear, also understood as occupation, in which the individual can surrender to their own free will, which is to relax, to enjoy themselves, to recreate and entertain themselves, or to cultivate the social conviviality with friends and, especially, family, getting rid of professional obligations, family and/or social(18).
The findings of this study showed that none of the pregnant women who spend time on leisure activities showed indications of depression, while 20.6% of pregnant women who didn’t spend time on leisure activity had indications of depression. A previous study(19) showed that women who did not participate in regular leisure activities showed a higher prevalence of mental disorders (40.9%) than those who participated regularly in any leisure activity (31.6%), pointing out that the impossibility or the restriction of free time can affect mental health.
The front significant data reported here suggests carrying out further research, including the importance of investigating the frequency of occurrence of depression among pregnant women, gleaming improvements in assistance to pregnant women and recent mothers, increased the quality of life of these women.
The study presented limitations as to the population and sample. The population set for this study was limited to pregnant women at low risk, not including women more susceptible to the development of mental disorders. Another important limitation refers to the size of the sample, due to the small number, the results are only considered for the population in question.
Conclusion
The results of this study conclude that depression is a reality among pregnant women, whereas 17% of them showed indications of depression and 7% showed dysphoria. Depression occurs more often among pregnant women older than 35 years, black, who worked with a lower family income, with no partner and leisure activities. It is necessary to emphasize the importance of involving elements regarding family assistance and nursing health teams with the capability of verbalization and facilitating to their concerns and feelings.
References
1. Ministério da Saúde (BR). Parto, aborto e puerpério: assistência humanizada à saúde. Brasília (DF): Ministério da Saúde (FEBRASGO); 2003. [ Links ]
2. Luis MAV, Oliveira ER. Transtornos mentais na gravidez, parto e puerpério, na região de Ribeirão Preto – SP – Brasil. Rev Esc de Enferm USP. 1998;32(4):314-24.
3. Kaplan HI, Sadock BJ, Grebb JA. Compêndio de psiquiatria: ciência do comportamento e psiquiatria clínica. 9ª ed. Porto Alegre: Artmed; 2007. [ Links ]
4. Falcone VM. et al. Atuação multiprofissional e a saúde mental de gestantes. Rev Saúde Pública. 2005;39(4):612-8. [ Links ]
5. Lowdermilk DL, Fishel AH. Complicações pós-parto. In: Lowdermilk DL, Perry SE, Bobak IM. O cuidado em enfermagem materna. Porto Alegre: Artmed; 2002. p. 746-74. [ Links ]
6. Gorenstei NC, Andrade L. Inventário de depressão de Beck: propriedade psicométricas da versão em português. Rev Psiquiatr Clín. 1998;25(5 ed esp):245-50. [ Links ]
7. Beck AT, Steer RA, Garbin MG. Psychometric properties of the Beck depression inventory: twenty-five years of evolution. Clin Psychol Rev. 1988;(8):77-100. [ Links ]
8. Marcolan JF. Análise comparativa das escalas psicométricas de depressão:um subsídio para a avaliação clínica do enfermeiro psiquiátrico. [Tese de Doutorado em Enfermagem]. São Paulo: Escola de Enfermagem da Universidade de São Paulo; 2002. 163 p. [ Links ]
9. Organização Mundial de Saúde. Classificação Estatística Internacional das Doenças e Problemas Relacionados à Saúde (CID – 10). São Paulo: EDUSP; 1997.
10. Espinose AF. Guia Prático de Enfermagem: Psiquiatria. In: Espinose AF. Psicopatologia Geral. Rio de Janeiro: Mac Graw-Hill; 2002. p. 41-98. [ Links ]
11.Baptista MN, Baptista ASD, Torres ECR. Associação entre suporte social, depressão e ansiedade em gestantes. Rev Psicol. 2006 jan/jun;7(1):39-48. [ Links ]
12. Vasques R, Piñeros S. Sicopatología en madres adolescentes. Pediatría. 1997;32(4):229-38. [ Links ]
13. Sinclair BP. Promoção e prevenção de saúde. In: Lowdermilk DL, Perry SE, Bobak IM. O cuidado em enfermagem materna. Porto Alegre: Artmed; 2002. p. 57-77. [ Links ]
14.Lovise GM, López JRRA, Coutinho ESF, Patel V. Poverty, violence and depression during pregnancy: a survey of mothers attending a public hospital in Brazil. Psychol Med. 2005;35(10):1485-92. [ Links ]
15. Stuart GV, Laraia MT. Enfermagem psiquiátrica: princípios e prática. 6ªed. Porto Alegre: Artmed; 2001. [ Links ]
16. Luís MAV. Contribuição da assistência de enfermagem de saúde mental dirigida à população de gestantes em nível de prevenção primária. [Dissertação de Mestrado em Enfermagem Psiquiátrica]. Ribeirão Preto: Escola de Enfermagem de Ribeirão Preto da Universidade de São Paulo; 1983. 120 p. [ Links ]
17. Saunders RB. Cuidado de Enfermagem durante a Gestação. In: Lowdermilk DL, Perry SE, Bobak IM. O cuidado em enfermagem materna. Porto Alegre: Artmed; 2002. p. 219-63. [ Links ]
18. Camargo RAA, Bueno SMV. Leisure, life besides work for a soccer team of hospital workers. Rev. Latino-Am. Enfermagem. 2003;11(4):490-8. [ Links ]
19. Araújo TM, Pinho OS, Almeida MMG. Prevalência de transtornos mentais comuns em mulheres e sua relação com as características sócio-demográficas e o trabalho doméstico. Rev Bras Saúde Mater Infant. 2005;5(3):337-48. [ Links ]
Received: Jul. 11th 2014
Accepted: Oct. 20th 2015
Correspondência
Luiz Jorge Pedrão
Universidade de São Paulo. Escola de Enfermagem de Ribeirão Preto
Departamento de Enfermagem Psiquiátrica e Ciências Humanas
Av. Bandeirantes, 3900 Bairro: Monte Alegre
CEP: 14040-902, Ribeirão Preto, SP, Brazil
E-mail: lujope@eerp.usp.br


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}