










Services on Demand
article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Share

 Permalink
PermalinkInteramerican Journal of Psychology
Print version ISSN 0034-9690
Interam. j. psychol. vol.41 no.1 Porto Alegre Apr. 2007
ENFRENTANDO A LOS OTROS: ESTIGMA EN EL SECTOR SALUD
AIDS-related stigma and health professionals in Puerto Rico
El estigma relacionado al SIDA y los profesionales de la salud en Puerto Rico
Yamilette Ruiz-Torres1,2; Francheska N. Cintrón-Bou; Nelson Varas-Díaz
University of Puerto Rico, San Juan, Puerto Rico
ABSTRACT
This study addresses an important issue in the AIDS epidemic in Puerto Rico: AIDS stigma among health professionals and health profession students. AIDS stigma has been documented among health services providers such as doctors, nurses, psychologists, and social workers. It has detrimental effects of the services provided and the lives of people living with HIV/AIDS (PLWHA). The main objective of this study was to explore AIDS stigma manifestations among a sample composed of eighty health professionals and health profession students who participated in in-depth qualitative interviews. Four thematic categories stemmed from the data analysis process. These addressed the following subjects: social manifestations of stigma, stigma manifestations in the workplace, use of sensitive information to control PLWHA, and surveillance of PLWHA. Participants manifested instances of stigmatization they had witnessed in their work and training scenarios. Furthermore, they elaborated on the need to place effective surveillance mechanism on PLWHA in order to control the epidemic.
Keywords: Acquired Immune Deficiency Syndrome, Stigma, Health professionals, Puerto Rico.
RESUMEN
Este estudio aborda un tema de importancia en la epidemia del VIH/SIDA en Puerto Rico: el estigma que emana de profesionales de la salud y estudiantes de dichas profesiones. El estigma relacionado al VIH/SIDA se ha documentado entre profesionales de la salud de la medicina, enfermería, psicología y trabajo social. El mismo tiene efectos detrimentales en los servicios provistos y las vidas de las personas que viven con VIH/SIDA (PVVS). El objetivo principal de este estudio fue explorar las manifestaciones del estigma relacionado al VIH/SIDA en una muestra de ochenta profesionales de la salud y estudiantes de profesiones de la salud que participaron en entrevistas cualitativas a profundidad. Cuatro ejes temáticos emanaron del análisis de las entrevistas. Estos abordaron los siguientes temas: manifestaciones sociales de estigma, manifestaciones de estigma en sus escenarios de trabajo, uso de información sensitiva para controlar a las PVVS, y la vigilancia de las PVVS. Las personas participantes describieron manifestaciones de estigma que habían presenciado en sus escenarios de trabajo y adiestramiento. Además, proveyeron descripciones elaboradas sobre la necesidad de implantar sistemas efectivos de vigilancia sobre las PVVS para controlar la epidemia.
Palabras clave: Síndrome de Inmunodeficiencia Adquirida, Estigma, Profesionales de la salud, Puerto Rico.
The Island of Puerto Rico is located in the Caribbean, between the Caribbean Sea and the North Atlantic Ocean, and to the east of the Dominican Republic. For centuries it was inhabited by aboriginal people and in 1493 it was claimed by the Spanish Crown following Christopher Columbus' second trip to the Americas. In 1898, after 400 years of colonial rule that saw the indigenous population nearly exterminated and the inclusion of African slave labor introduced, Puerto Rico was conceded to the United States as a result of the Spanish-American War. Puerto Ricans were granted American citizenship in 1917, and popularly elected governors have served since 1948. In 1952, a constitution was enacted providing for internal self-government while the Island remains a commonwealth associated with the United States of America and subject to federal law (Central Intelligence Agency, 2004). Puerto Rico's population is 3,808,610 as of the US Census carried out in 2000 (US Census Bureau, 2000). It is in this context that the HIV/AIDS epidemic plays out. A country with strong Latin American roots, enmeshed in the social and cultural context of the United States of America.
Puerto Rico and the HIV/AIDS Epidemic
Although Hispanics comprised just 13.7% of the US population in 2003, they accounted for 20.3% of new AIDS cases reported that year, a proportion that has remained steady over the past five years. Hispanics represented 19.9% of people living with AIDS at the end of 2003 (Health Resources and Services Administration [HRSA], 2005). These numbers evidence how hard the epidemic has hit the Hispanic population, Puerto Ricans included.
As of today, there are an estimated 2.1 million PLWHA in Latin America and the Caribbean. Around 300,000 people contracted HIV in 2004, and at least 130,000 died of AIDS in the same year. The Caribbean has the second highest rate of HIV infection in the world after sub-Saharan Africa, with 440,000 PLWHA (International HIV/AIDS Alliance, n.d.). In Puerto Rico itself, the numbers are alarming. Almost 30,000 cases of AIDS were confirmed as of March, 2004 (PASET, 2004). Of those cases, 18,370 have died. The most common means of transmission among male adults are needle sharing for drug use (54%), unprotected homosexual activity (21%), and unprotected heterosexual activity (14%). Among females the main means of transmission are unprotected heterosexual activity (60%) and needle sharing for drug use (37%). In total, the most common adult/adolescent means of transmission were needles sharing (50%), unprotected heterosexual activity (24%), and unprotected homosexual activity (17%).
These numbers are important because they show the epidemiological face of the disease. Puerto Rico lives on the boundaries on Latin America and the United States. On the one hand it lies in the second most affected geographical region of the world (the Caribbean), and on the other it is home to many of the most disproportionately affected minority groups of the United States (Hispanics). Still, the social implications of living with the disease reveal a more human side of the epidemic that surpasses numbers. HIV/AIDS continues to negatively impact the lives of those who live with the disease and makes daily life even harder. One of the main obstacles that PLWHA face is the existing manifestations of AIDS-related stigma which is very present in Puerto Rican society (Varas-Díaz, Serrano-García, & Toro-Alfonso, 2004).
What is Stigma?
The concept of stigma appears in Ancient Greece, where it was used to describe a mark in the body or a tattoo on the skin of a person. This was evidence of the person's participation in a negative action and the identification of a person that needed to be avoided (Crawford, 1996). It has also been defined as a mark printed in a supernatural way on the bodies of saints, an imposed mark with incandescent iron as a symbol of a penalty or slavery, and as evidence of a bad reputation (Real Academia Española, 1992). Stigma is also defined as a social construction associated to the recognition of a difference that is based on a characteristic or a mark and the subsequent unworthiness of the person that has it (Dovido, Major, & Crocker, 2000). These definitions reflect the basic concepts of the notion of stigma. These are: 1) stigma implies a mark or body delimitation with a negative meaning; 2) these marks reflect a non desirable aspect of the person that have them; and 3) stigma has negative implications for the person that has it (Varas-Díaz et al., 2004).
It is also vital to address Erving Goffman's (1963) ideas about stigma, since his work is widely credited with providing the theoretical underpinnings that frame most stigma research (HRSA, 2003). For Goffman, stigma is an attribute that is deeply discrediting within particular social interactions. Due to this negative mark that fosters stigma, the stigmatized is considered almost inhuman. Goffman identified three types of stigma: 1) body abominations; 2) individual blemishes of character; and 3) the tribal stigmas. Body abominations are based on physical deformation of a particular person. For example, people that lack any part of their body can suffer this type of stigma. Individual blemishes of character are related to the way a person is or how he/she behaves. For example, people that have mental disorders, are imprisoned, or have drug and/or alcohol addictions can suffer from this type of stigma. Finally, tribal stigmas are transmitted through lineage by being part of a racial, ethnic, national, religious, or other groups.
In their work, Varas-Díaz et al. (2004) summarize some of the most important characteristics of the concept of stigma. These are: 1) the stigma is a negative mark with an important bodily component; 2) stigma is related to the interpretation of both the stigmatized and the stigmatizer; 3) when stigmas are developed, ideas regarding the devalued nature of that person are fostered; 4) the stigmatizing process has primarily negative consequences; and 5) there are generalized ideas about stigmatized people in our society. These definitions have served to develop a better understanding of the stigma surrounding HIV/AIDS.
AIDS-Related Stigma
The HIV/AIDS epidemic has fostered several responses in society which include prejudice, fear, and even in some occasions, hysteria (Kelly, St. Lawrence, Smith, Hood, & Cook 1987). The negative interpretations of HIV/AIDS and PLWHA have been coined as AIDS-Related Stigma. This term reflects the magnitude of the stigma associated to HIV/AIDS (Herek & Glunt, 1988). This type of stigma is directed towards people that are perceived to be infected with HIV, without taking into consideration if they really are infected or if they manifest AIDS symptoms (Herek & Glunt, 1988). Therefore, people associated to HIV/AIDS by work or family relations can be stigmatized, even when they are not PLWHA (Snyder, Omoto, & Crain, 1999). Herek and Glunt (1988) discuss two major sources of this stigma: the identification of AIDS as a deadly disease and the association of AIDS with already stigmatized groups, especially gay men.
Diseases associated with the highest degrees of stigma share common attributes: 1) the person with the disease is seen as responsible for having it; 2) the disease is both progressive and incurable; 3) the disease is not well understood among the public; and 4) the symptoms cannot be concealed. HIV infection fits this profile (HRSA, 2003). People infected with HIV are often blamed for their condition. Second, although HIV is treatable, it is nevertheless an incurable and progressive disease. Third, HIV transmission is not well understood by many in the general population. Finally, although asymptomatic HIV infection can often be concealed, the symptoms of HIV-related may not be. HIV-related symptoms may be considered repulsive, ugly, and disruptive to social interaction (HRSA, 2003).
The Consequences of AIDS-related Stigma
AIDS-related stigma poses threats to the physical and psychological well-being of PLWHA. AIDS-related stigma has multiple consequences (HRSA, 2003). These are: 1) the deterioration of interpersonal relationships; 2) the manifestation of negative emotions; 3) adverse effects to health as a consequence of the rejection of the HIV antibody test; 4) anxiety; 5) depression; 6) guilt; 7) loss of support; 8) isolation; 9) difficulties with family dynamics; 10) emotional or physical violence, and (11) the deterioration of relations with health care providers. Other negative consequences of AIDS stigma include: 1) the development of new infections as a consequence of people deciding not inform others of their condition; 2) loss of health insurances; 3) social discrimination; 4) loss of employment; 5) problems accessing health services; 6) stress related to hiding the condition; and 7) the development of discriminatory policies by governments (Herek, 1999; Leary & Schreindorfer, 1998; Varas-Díaz et al., 2004).
The consequences of AIDS stigma are worsened when it emanates from sectors of the population that are of vital importance to PLWHA. One such case is AIDS-related stigma manifested by health professionals which can limit access to services that are essential for the quality of life of PLWHA.
AIDS-related Stigma and Health Professionals
Having access to health care services can be a problem for PLWHA because health scenarios themselves can be a source of stigma. Research from early on in the epidemic evidenced that health care providers' fear of contagion and death had negative effects on their attitudes toward and treatment of PLWHA (HRSA, 2003). These attitudes were largely based on worries related to their vulnerability to the infection (All & Sullivan, 1997). Researchers have attributed stigmatizing attitudes among health professionals to lack of contact with PLWHA, fear of infection, and anxiety related to death (Weinberger, Conover, Samsa, & Greenberg, 1992). Fear of infection has been documented even among providers that are aware of universal precautions to avoid infection in the workplace (Wallack, 1989). These attitudes can lead to denial of services and condemnation of sexual activity and drug use (McCann, 1999).
Still today, some health professionals avoid treating PLWHA and evidence of stigma continues to emerge from survey research and anecdotal reports. As part of the community in general, these professionals are susceptible to a lot of the stereotypes and biases that characterize the rest of the society (All & Sullivan, 1997; Kelly et al., 1987). The stigmatizing attitudes towards PLWHA among health professionals are unfortunate because it is to these professionals that they frequently reveal their positive status (Sowell, Lowenstein, Moneyham, Demi, Mizuno, & Seals, 1997). AIDS stigma affects the well-being of PLWHA and influences their personal choices about disclosing their serostatus to others (Herek, 1999). These attitudes and stigmatizing situations are also problematic and have negative consequences in the services that PLWHA receive. For example, some studies have documented the unavailability of health services providers to treat PLWHA (Varas-Díaz et al., 2004). In light of these potentially negative consequences the main objective of this study was to explore AIDS stigma manifestations among a sample composed of health professionals and health profession students in Puerto Rico.
Method
In order to achieve the proposed objective of the study we developed and implemented an exploratory design using a qualitative technique. This was done through the implementation qualitative in-depth interviews with health professionals and health profession students.
Participants
The total sample of the study was composed of 80 participants. We interviewed 80 participants (40 health professionals and 40 health profession students) equally divided among the following disciplines: medicine (n=20), nursing (n=20), psychology (n=20), and social work (n=20). The inclusion criteria for the health professionals were: 1) that they were older than 21 years of age; 2) that they voluntarily participated in the study; and 3) being active practitioners of their profession at the moment of the interview; and 4) that they worked in health institutions in which PLWHA could receive services (e.g. public hospitals, community based organizations, etc). We developed these inclusion criteria in order to ensure that the professionals could legally consent to participate, that they did so without being coerced, that they could talk about their past and recent work experiences, and that these experiences were in scenarios in which PLWHA receive or could receive health services.
The inclusion criteria for the health profession students were: 1) that they were older than 21 years of age; 2) that they voluntarily participated in the study; 3) that they were health profession students at the moment of the interview; and 4) they had completed at least one practice in a health care institution at the moment of the interview as part of their training. These inclusion criteria ensured that students could legally consent to participate, that they did so without being coerced, and that they could talk about their past and recent training experiences. Students from the fields of medicine and psychology were recruited at a graduate level (MA, PhD or PsyD) since these degrees are required in Puerto Rico to practice each profession. Students from social work and nursing were recruited from both graduate and undergraduate levels since both professions can practice with such degrees.
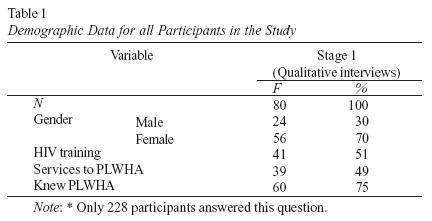
The demographic data from participants can be seen in Table 1. Most of the sample was composed of females as in most of these health professions (psychology, nursing and social work) they outnumber men. Half had received some kind of HIV related training and had provided services to PLWHA at some time. Seventy five percent of participants knew someone living with HIV/AIDS. The mean age for the sample was 32. The most common range for income was between $20,000 and $30,000 n=47 (59%).
Selection and Screening
The research team recruited participants in several scenarios which included the following: government agencies, public housing projects, public hospitals, public schools, and public and private universities. The initial steps for the recruitment were telephone calls to the directors of these institutions to explain the purpose of the study and to request permission to invite employees and students to participate in the study. After we obtained permission, the research team personally identified potential participants in order to ensure that they did not feel obliged by supervisors or teachers to participate in the study.
We explained to each potential participant the purpose of the study and we invited them to participate. Those that wanted to take part completed a consent form explaining the nature of the study, their participation, and the measures in place to ensure their confidentiality. The consent form also mentioned the following issues: 1) the benefits and risks of their participation, 2) the time that their participation required, 3) the possibility of ending their participation at any time, 4) the possibility of requesting psychological services if they needed them due to their involvement in the study, and 5) the right to receive the results of the study.
Instruments
We developed several instruments as part of the study which are described here. These were the following: screening form, socio demographic data questionnaire and the qualitative in-depth interview guide.
Screening form - This screening form served as a guide for recruiters to ensure that all participants met the inclusion criteria previously described. Each form included a question for each of the criteria and contact information (in the case of the qualitative interviews). This form was completed with participants for both the qualitative and quantitative stages.
Socio demographic data questionnaire - This self-administered questionnaire included 30 questions addressing variables such as gender, age, sexual orientation, marital status, area of residence, employment status, professional training, and income. The questionnaire version completed by health profession students also included questions related to their current training scenario.
In-depth interview guide (Varas Díaz, 2005) - This interview guide served to maintain a minimum level of uniformity in the subjects that were explored during the interviews. This guide was composed of questions addressing seven subject areas: 1) training and work experiences related to HIV/AIDS; 2) definitions of illness; 3) personal perception of the HIV/AIDS epidemic in Puerto Rico; 4) potential contributions of health professionals and students in issues related to the lives of PLWHA; 5) perception on society's opinions regarding PLWHA; 6) health professionals' opinions regarding PLWHA; and 7) the bodily dimensions of the HIV/AIDS epidemic. The guide included specific instructions for the person interviewing to follow.
The guide of the interview was evaluated by a panel of six judges that included researchers in the area of HIV/AIDS and a PLWHA in order to establish ensure the appropriateness of its content. After incorporating their feed back we carried out a pilot study with eight people (four professionals and four students). The results of the pilot study evidenced that the participants understood the questions and they were able to answer them without difficulties.
Procedures
As an initial step for the implementation of the interviews, interviewers participated in formal training sessions on the following subjects: 1) AIDS stigma definitions; 2) the role of stigma in the HIV/AIDS epidemic; 3) ways in which stigma is manifested among health professionals; 4) ethical dimensions of the study; 4) adequate forms of recruitment; and 5) implementation of the interview, specifically the phrasing of the questions and the use of follow up questions when needed.
When the participants were recruited, a date for the interview was scheduled in a place of the participant's choosing. That place needed to meet the following requirements: 1) be a private place; 2) without interruptions; and 3) in which the person that was interviewed felt comfortable. At the moment of the interview the interviewer explained once again the purpose of the study and the nature of their participation. After the person agreed to participate, they signed the consent form, completed the socio demographic data questionnaire, and proceeded to participate in the interview. The interviews lasted on average an hour and a half. When the interviews were completed, they were transcribed by people already trained and submitted to a qualitative analysis.
Analysis
The information gathered through the in-depth interviews was subjected to a qualitative analysis. It was our interest to understand how the participating health professionals and students perceived PLWHA. In order to achieve this goal the interviews were transcribed through a supervised process to ensure fidelity (Poland, 2002). The research team met on a weekly basis to identify themes or patters in the data related to our objectives. Once those themes were identified the research team searched for texts that evidenced them. All selected texts were discussed to ensure that they were in accordance with the themes they were associated to (Phillips & Ardí, 2002). Once these texts were selected they were coded with the use of qualitative analysis computer software (Nudist Nvivo V.1.). All themes were finally discussed by the research team and descriptions of each were generated.
Results
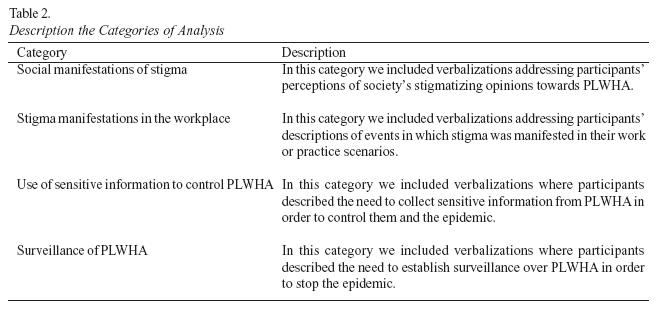
We organized the participants' verbalizations into four categories that evidenced several forms of stigmatization of PLWHA. In Table 2 we describe each of these categories. In this section, we present verbalizations from the interviews that encompass each of the categories. In order to identify the presented texts we use the following codes: PM (Professional Medicine); PP (Professional Psychology); PSW (Professional Social Work); PN (Professional Nursing); SM (Student Medicine); SP (Student Psychology); SSW (Student Social Work); and SN (Student Nursing). We also used M to represent males and F to represent females, I for interviewers and P for participants.
Social Manifestations of Stigma
In this category we included verbalizations addressing participants' perceptions of society's stigmatizing opinions towards PLWHA. Participants understood that Puerto Rican society has overall negative opinions towards PLWHA. They indicated that society's stigma manifestations occurred as a consequence of lack of education and information. They also mentioned that stigma manifestations are related to the association of HIV to homosexuality, drug use, promiscuity, divine punishment, fear of contagion, and the influence of the media. These were answers to the question: What do you think is society's general opinion about PLWHA?
P: "…that they are people that are ill. People that have the potential to keep infecting others. People that got infected because they were doing things that they shouldn't be doing... and that they are going to die". (PSW/F)
P: "This woman lived with her son. Her son was an HIV patient. When she discovered it, she put plastics on all the furniture. She gave him plastic dishes to eat out of, with plastic utensils, and plastic cups. When her grandchildren came to visit her he couldn't be in the house or had to stay in his bedroom. I understand this is total ignorance to what HIV is. In the public housing project where I work I saw one of the clients have a fight with another girl. The other girl yelled "Go away. You are putrid". Those are comments that you see and there is still a lot of discrimination, a lot of rejection from the community and family". (PSW/F)
P: "...A lot of them think that they have that illness because they were asking for it, because they did not protect themselves. That they wanted to do whatever they wanted without being careful. A person that is ill cannot be touched… it is like having them isolated. That is what most people think". (SN/F)
P: "...that they are depraved, that they are promiscuous, that they are people that haven't done good in their life. That they are drug users or that they are gay.
I: And why do you think opinions are like this? Why do people think this way?
P: I think that the press and the media, maybe due to sensationalism, they focus on characteristics associated to the patients that are not necessarily the ones that respond to a reality". (PP/F)
I: "Have you witnessed first hand an event that you understand was prejudiced for a PLWHA?"
P: "Yes, a person that worked at Burger King that had HIV and worked making hamburgers. Someone from the hospital went and saw him. The person told the manager, or something like that, and the manager put him to work cleaning. The wages were the same, everything was the same, but he did not want to... This is a true story, something that someone told me last week. The person felt so bad that he took the first weeks mopping the floor and the next week he resigned from his position". (SP/F)
Stigma manifestations in the workplace
In this category we included verbalizations addressing participants' descriptions of events in which stigma was manifested in their work or practice scenarios. Participants made reference to examples to evidence the stigma manifestations that can be seen in health scenarios such as hospitals and clinics. During the interview they mentioned feeling resistant to mention these examples since they were compromising the professional ethics of their workplaces, as well as their colleagues conduct. Even while facing this difficulty during the interview, the majority of the participants agreed that discrimination exists in health scenarios. The examples provided by participants were related to discriminatory acts and opinions of other health professionals, and not themselves. They made reference to how stigma is manifested by lack of training and by isolating patients.
I: "How do you think these attitudes manifest themselves in the work scenarios?"
P: "They feel fear. If they get pricked (with a needle). I had a case like that happen to me personally. I needed some blood tests and the lady got pricked with the needle she used to take my blood. She pricked herself and she said to me: ´You don't have HIV/AIDS right?" And I said to her: "Well… there are my blood tests if you want to analyze them". I mean, there are professionals like that`". (PSW/F)
I: "Do you think that health profession students should receive specialized training in HIV?"
P: "Yes. Because sometimes when you say "I have an HIV patient in the floor" then they all get crazy. It is the same when you have a tuberculosis patient. Everyone gets crazy with the tuberculosis patients". (SM/M)
I: "Do you think that discrimination does not exist in the health scenarios or is it just hard to spot?"
P: "I know that there are people that have said… they go to a public hospital or to an office and since they know that the person is HIV positive, a drug user, or lives in public housing, they make the person wait until the end of the day. When people arrive they get served at the end of the day, to see if the person gets tired and leaves. This can be a form of discrimination".(PM/M)
I: "Have you been in situations where discrimination is evident in health scenarios?"
P: "Yes. People that are drug addicts or drug users sometimes arrive and they are left to the side. I have seen doctors that do not provide services for them. They say "I am not going to serve them" and do not do it". (SP/F)
P: "...we also have two isolation rooms that are used when there are no beds in medicine.… For me it is a condition that it is seen as very threatening. Even though we have the preparation and know how to protect ourselves of the illness, there is a lot of fear. It is something, I would, say emotional. For example, in the morning I come and they tell me that I have been assigned from rooms 25 to something. Well… in that bedroom is isolation and there is an AIDS patient. Well… it is like, I preferred not to have it. It is not that I am rejecting the person, but I would prefer not to have to intervene". (PN/F)
Use of sensitive information to control PLWHA
In this category we included verbalizations where participants described the need to collect sensitive information from PLWHA in order to control them and the epidemic. Unlike both categories previously described in which stigma emanating from others was mentioned, in this category instances of personal stigmatizing perspectives are evidenced.
The participants suggested the need to collect information regarding: age, sex, mean of infection, time that the person has lived with the illness, full name, address, social security number, medical regime, work scenarios and level of education. Participants mentioned that information could be used for prevention efforts, to provide medicines and measure their effectiveness, and to keep updated for statistics regarding the epidemic. They also mentioned the need to use this information as part of a census mechanism to understand if the epidemic has improved or worsened. Although described as information that would be used for benefitial purposes, participants recognized that it would entail in some cases interfering with the right to privacy of PLWHA. What was most evident in all the verbalizations was the perceived need to create a detailed data bank with the profiles of PLWHA as a way to control the epidemic.
I: "Do you think that the Health Department should create a register of the new cases and of the cases that already exist in the country?"
P: "I think so, yes. I also think that the basic information of the person should be collected: name, address, social security, and etcetera. I would say it is important to know how that person got the virus because that will give us information that we need to try to prevent it in the future". (PSW/F)
I: "Do you think it is important to ask that person their name and the address?"
P:"Yes. Because that way if by coincidence it is necessary to go to their houses you have the address to go to. Because you are not going to a municipality (town) to say "X person" is like this: "this hair color, this skin color…"(PN/F)
I: "If a man goes to have the test, what information do you think is important to gather from his history?"
P: "...if he is married, what is his sexual preference, if he has a partner, if he has tattoos, with how many partners he has been with in the last years, if he knows who he has been with. The most information possible".
I: "Why do you think it is important to know his sexual preference?"
P: "…Because that way, I mean, if this is for a prevention plan, to be able to control. One will be able to guide people that are involved with that human being". (PP/F)
Surveillance of PLWHA
In this category we included verbalizations where participants described the need to establish surveillance over PLWHA in order to stop the epidemic. Participants indicated different ways of supervising PLWHA in order to control their behaviors so they do not infect other people. For example, this surveillance would be useful to determine if PLWHA could adopt a child, regulate the sexuality of PLWHA, address the issue of children with HIV in schools, and to determine types of work that they could engage in. One participant went as far as to recommend mandatory HIV testing for all people who are going to get married.
I: "In some cases PLWHA want to adopt children and raise them. What do you think the Family Department should do with these cases of adoption?"
P: "To investigate both parts, the place where they live, how they live, what they do, their occupation, all of that because if they are going to give a child to this family, it has to be a responsible family, that are oriented about their illness. So they do not… a baby that is not guilty of anything… that he gets infected. But mostly to investigate the place, how they live". (SN/F)
I: "Even though there are fewer cases of children that live with HIV/AIDS, let's imagine that you have a son or a daughter and that you know that in the same school there is another boy that has HIV. Would you be worried about the security of your son?"
P: "…I don't think he will be infected with AIDS only for sharing with another boy."
I: "Would you say something to him to protect himself?"
P: "Let us suppose beforehand that I know that the kid has AIDS and my son doesn't know it. I would not tell him because then my son, for example, would fear the kid. But I would explain about the illness and about the precautions, etc. But I do not think it would create a danger to share with him because he is a school peer".
I: "Would you recommend something to the school? Would you recommend something to the teacher?"
P: "Yes, because I would be very attentive because… suppose they fight or there is physical contact that involves cuts and wounds. In that sense, they should have supervision". (SP/F)
I: "Do you think a person that is HIV+ should avoid having sex?"
P: "…doesn't have to avoid them, because the right that they have as human beings cannot be avoided. But, having the precautions… First they have to reveal it to the person that has the sexual relationship and use protection, and take precautions. The maximum of protection they can have… try to have the same partner". (SM/F)
I: "Do you have any another comments before we finish the interview?"
P: "Yes. I think that the Health Department should work with making the HIV tests compulsory for people that are going to get married". (PM/F)
Discussion
We would like to begin our discussion of the findings by addressing one methodological issue of importance. These interviews were hard to carry out. Social desirability was evident during the process as participants did not want to be identified as stigmatizers of PLWHA. Still, we feel that we were able to assess manifestations of stigma by implementing detailed and in-depth interviews. Taking this fact into consideration it is understandable that the first two categories of the analysis were related to opinions and actions that "other people" manifest. For example, in the first category we can see how participants were mostly concerned and fluently described how they perceive "society" stigmatizes PLWHA. In the second category, they were able to be more detailed and express instances of AIDS stigma they had witnessed in their work scenarios. Still, this transition from society to health professionals was difficult for participants and interviewers, as the first expressed feeling that they were reporting inappropriate information about colleagues of their work or training scenarios.
As we dwelled deeper into personal opinions regarding PLWHA we were able to examine two specific instances related to AIDS stigma. These were related to the supervision and surveillance of PLWHA. Information seems to be a major concern for the interviewed sample. Specifically, gathering personal information from PLWHA. Although some of this information is currently gathered in Puerto Rico as part of the Health Department's surveillance system (mean of infection, age, gender), other information suggested went far beyond what is collected today, and would potentially infringe on the privacy of PLWHA. This included names, addresses, social security numbers and even levels of education. Although participants described that the information would be used for prevention efforts, the potential use of such data is worrisome.
This worry regarding the use of sensitive data from PLWHA was corroborated when participants manifested the need to supervise and regulate those living with the virus. Instances from work scenarios to sexual activity were described as areas that needed to be regulated with the use of the gathered information in order to stop PLWHA from infecting others. The use of sensitive information, in light of these attitudes towards surveillance of the sick, poses a major challenge for PLWHA and a fertile ground for AIDS stigma. Participants seemed to agree that PLWHA were responsible for the spread of the epidemic and that proper surveillance of their activities would be an essential prevention effort. These views on prevention regularly violate the rights of PLWHA and foster stigma.
These findings must be understood in light of the ongoing discussions, or lack thereof, regarding the HIV/AIDS epidemic in Puerto Rico. Two main issues stand out: 1) government officials have publicly stated that the epidemic is currently under control, and 2) funding for HIV medication is provided by the United States under the Ryan White Care act. These two facts have fostered little public discussion regarding the ever-growing nature of the epidemic in the Island. Furthermore, the availability of medicine with relative ease (in comparison to other Latin American countries) has promoted complacency among many that seem to think that the worst part of the epidemic is far behind us. Within an epidemic hat is perceived as being under control and with the alleged "main necessity" of PLWHA financed by the United States, it seems evident to participants that the only real need left would be to control those that already have HIV in order to completely stop the epidemic. It is in this rationale that surveillance efforts are a manifestation of stigma in the Puerto Rican context.
As health care service providers and as future professionals it is important to reflect upon issues like the ones presented in this study. As professionals, we have a responsibility towards those that need our services. Due to the growing number of HIV/AIDS cases in Puerto Rico and the world it is imperative to develop strategies to eradicate AIDS stigma. This is particularly important among health professionals and students, since they interact on a daily basis with PLWHA and are expected to provide quality health services. These manifestations of stigma represent an obstacle to the services that they offer. We must continue exploring the different manifestations of AIDS stigma among health professionals to develop culturally embedded interventions that are relevant to their concerns, fears, and stigmatizing attitudes.
References
All, C., & Sullivan, L. (1997). The effects of an HIV/AIDS educational programme on the anxiety level of nursing students. Journal of Advanced Nursing, 26, 798-803. [ Links ]
Central Intelligence Agency. (2004). The World Fact book 2004. Retrieved April 1, 2005, from http://www.cia.gov/cia/publications/factbook/geos/rq.html [ Links ]
Crawford, A. M. (1996). Stigma associated with AIDS: A meta-analysis. Journal of Applied Social Psychology, 26, 398-416. [ Links ]
Dovido, J. F., Major, B., & Crocker, J. (2000). Stigma: Introduction and overview. In T. F. Heatherton, R. E. Kleck, M. R. Hebl, & J. G. Hull (Eds.), The social psychology of stigma (pp. 1-28). New York, USA: The Guilford Press. [ Links ]
Goffman, E. (1963). Stigma: Notes on the management of spoiled identity. New York, USA: Simon & Schuster. [ Links ]
Health Resources and Services Administration. (2003, August). HIV/AIDS stigma. Retrieved April 13, 2005, from http://www.thebodypro.com/hrsa/stigma.html#4 [ Links ]
Health Resources and Services Administration. (2005). Hispanics and HIV/AIDS. Retrieved April 13, 2005, from http://hab.hrsa.gov/history/fact2005/hispanics_and_hivaids.htm [ Links ]
Herek, G. M. (1999). AIDS and stigma. American Behavioral Scientists, 42, 1106-1116. [ Links ]
Herek, G. M., & Capitanio, J. P. (1993). Public reactions to AIDS in the United States: A second decade of stigma. American Journal of Public Health, 83(4), 574-577. [ Links ]
Herek, G .M., & Glunt, E. K. (1988). An epidemic of stigma: Public reactions to AIDS. American Psychologist, 43(11), 886-891. [ Links ]
International HIV/AIDS Alliance. (n.d.). Latin America and Caribbean _ Overview. Retrieved April 13, 2005, from http://www.aidsalliance.org/sw7236.asp [ Links ]
Kelly, J. A., St. Lawrence, J. S., Smith, S., Hood, H. V., & Cook, D. J. (1987). Stigmatization of AIDS patients by physicians. American Journal of Public Health, 77(7), 789-791. [ Links ]
Leary, M. R., & Schreindorfer, L. S. (1998). The stigmatization of HIV and AIDS: Rubbing salt in the wound. In V. J. Derlega & A. P. Barbee (Eds.), HIV & social interaction (pp. 12-29). Thousand Oaks, USA: Sage. [ Links ]
McCann, T. V. (1999). Reluctance amongst nurses and doctors to care for and treat patients with HIV/AIDS. AIDS Care, 11(3), 355-359. [ Links ]
PASET. (2004, March). AIDS surveillance report. Department of Health, Commonwealth of Puerto Rico. [ Links ]
Phillips, N. & Ardí, C. (2002). Discourse analysis: Investigating processes of social construction. Thousand Oaks, California: Sage. [ Links ]
Poland, B.D. (2002). Transcription quality. En J.F. Gubrium & J.A Holstein (Eds.) Handbook of interview research: Context and method (págs. 629-649). Thousand Oaks, California: Sage. [ Links ]
Real Academia Española. (1992). Diccionario de la Real Academia Española (21a ed., Vol. 1). Madrid, Spain: Author. [ Links ]
Snyder, M., Omoto, A. M., & Crain, A. L. (1999). Punished for their own good deeds. American Behavioral Scientists, 42, 1175-1192. [ Links ]
Sowell, R. L., Lowenstein, A., Moneyham, L., Demi, A., Mizuno, Y., & Seals, B. (1997). Resources, stigma, and patterns of disclosure in rural women with HIV infection. Public Health Nursing, 14, 302-312. [ Links ]
US Census Bureau. (2000). Census 2000 demographic profile highlights. Retrieved April 1, 2005, from http://factfinder.census.gov/servlet/ [ Links ]
Varas Díaz,N. (2005. Qualitative AIDS stigma interview guide. Unpublished document. University of Puerto Rico: Graduate School of Social Work. [ Links ]
Varas-Díaz, N., Serrano-García, I., & Toro-Alfonso, J. (2004). Estigma y diferencia social: VIH/SIDA en Puerto Rico. San Juan, Puerto Rico: Huracán. [ Links ]
Wallack, J. J. (1989). AIDS anxiety among health care professionals. Hospital and Community Psychiatry, 40, 507-510. [ Links ]
Weinberger, M., Conover, C. J., Samsa, G. P., & Greenberg, S. M. (1992). Physicians' attitudes and practices regarding treatment of HIV-infected patients. Southern Medical Journal, 85, 683-686. [ Links ]
Yamilette Ruiz Torres. Doctoral candidate in clinical psychology at the University of Puerto Rico. Her research interest include stigma, HIV/AIDS, and training of health professionals. E-mail: yamilette_ruiz@yahoo.com
Francheska Cintrón Bou. Ph.D in social-community psychology and is an Assistant Researcher at the University of Puerto Rico's Beatriz Lassalle Graduate School of Social Work. Her research interests include stigma, HIV/AIDS, sexuality and the elderly.
Nelson Varas Díaz. PhD in social-community psychology and is an Assistant Professor at the University of Puerto Rico's Beatriz Lassalle Graduate School of Social Work. He is the first author of the book entitled "Estigma y diferencia social: VIH/SIDA en Puerto Rico". His research interests include social stigma, HIV/AIDS, social policy, research methodology, and the development of identity discourses related to health and illness.
1 Address: University of Puerto Rico, Beatriz Lassalle Graduate School of Social Work, PO Box 23345, San Juan, PR 00931-3345. . E-mail: nvaras@rrpac.upr.clu.edu
2 This study was funded by the United State's National Institute of Drug Abuse (1R21DA017643-01).
