










Serviços Personalizados
artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282
Rev. bras. crescimento desenvolv. hum. vol.20 no.2 São Paulo ago. 2010
PESQUISA ORIGINAL ORIGINAL RESEARCH
Motor learning in children with cerebral palsy
Carlos Bandeira de Mello MonteiroI; Cristiane Matsumoto JakabiII; Gisele Carla dos Santos PalmaII; Camila Torriani-PasinIII; Cassio de Miranda Meira JuniorI
IDoctorate
from the University of São Paulo and Professor of Science and Physical
Activity course at the University of São Paulo (EACH-USP)
IIGraduate in Physiotherapy at the University Center of United Metropolitan
Faculties (FMU)
IIIDoctorate from the University of São Paulo and Professor
in the School of Physical Education and Sport at the University of São
Paulo (EEFE-USP)
Author responsible for correspondence
ABSTRACT
INTRODUCTION:
cerebral palsy (CP) has the characteristic of causing changes in posture and
movement that hamper the achievement of functional activities. In the face of
motor disabilities, rehabilitation becomes essential and is an option based
on motor learning. However, it is important to research the motor learning process
in individuals with CP to make the organization of treatment programs more effective.
OBJECTIVE: Analyse the motor learning in children with CP.
METHOD: For the realization of this work, an experimental group (EG)
and a control group (CG) was used, comprised of four children matched in relation
to gender (one female and three masculine) and age (between seven and twelve
years). The task was to conduct a path into a maze in the shortest time possible.
The work consisted of two phases, being initially an acquisition phase (AQ)
and then transfers (immediate-IM; short-term-ST and long-term-LT).
RESULT: It was found that there was no statistical significance difference
between AQ and transfers evaluated with the following values: IM (z= -1.83,
p=0.07), ST (z= -1.83, p=0.07) and LT [EG (z= -1.83, p=0.07) and CG (z=
-1.46, p=0.14)].
CONCLUSION: In the process of maze task learning, when analyzing the
results between phases AQ and transfer, significant difference was not observed,
which means that individuals with CP showed learning capacity through task adaptation
equivalent to individuals without CP.
Keywords: cerebral palsy; maze learning; children.
INTRODUCTION
Cerebral palsy (CP) can be defined as a disorder of posture and movement capacity. This disorder is persistent, however, not unalterable, and is caused by lesion in the developing central nervous system (CNS), before, during birth or in the first months of infancy1,2. Stokes2 cites that disturbances of posture and movement can be defined as the inability of the body to confront effectively the effects of gravity as related to the Earth's surface through a support base. Thus, CP causes variable difficulties in the coordination of muscle action, with the resulting inability of the child to maintain posture and perform normal movements1,3-7. Accordingly, these individuals present complex motor alterations, being the primary deficits described by Papavasiliou8, such as abnormal muscle tone influencing posture and movement, change of balance and coordination, reduction in strength, loss of selective motor control with secondary contracture problems and bone deformities.
Considering the alterations presented and the difficulty in achieving alignment and adjustment of postures that permit the experience of daily activities, inclusion in programs of ongoing habilitation and rehabilitation is fundamental for an individual with CP, which may interfere significantly in the interaction of the child in relevant contexts. Thus, it is possible to influence the performance of not only basic motor markers (roll, sit, crawl and walk), but also the activities of the daily routine, such as bathing, feeding, dressing and moving around in varied environments, among others. Due to insufficient responses about the benefits of a rehabilitation program in the improvement of an individual with CP8 and the increase of interest in motor function9,10, the physiotherapist and other health professionals who work with CP can apply the knowledge derived from motor learning to organize a program of treatment based on scientific evidence from this basic area of knowledge8.
As phenomenon, motor learning can be defined as the capacity of the individual to perform a motor skill inducing a relatively permanent improvement in performance as a result of practice or experience11,12. In other words, it is the process along which skills become easily performed with the aid of practice and information13-15. During motor skill acquisition, the learner needs to perform trials to achieve a performance criteria or stabilize a behavior11,13.
Throughout this process, a selection occurs between memory systems that enable the acquisition of some aspects most relevant to cognition, emotion and attention16, as well as the acquisition of cognitive structures, such as programs or plans of action11, schemes17, traits18, or the formation of complex neuromuscular synergies19.
Retention and transfer are two other crucial concepts in the motor learning process13,17,20. They are ways of testing learning in relation to the degree of permanence that was acquired after a period without practice (retention) and the capacity of acquiring a motor behavior practiced in a different context (transfer).
Thus, to verify that learning occurred with solidity, more than compare performance in the initial phase in relation to the final phase of acquisition, it is necessary to assess the performance in learning tests (i.e. retention and/or transfer)21-24. As explained above, it is crucial that the professional who works with individuals with CP can use instruments of easy application allowing the analysis of factors that interfere in acquisition, retention and transfer of motor skills25. A task that permits the evaluation of various neuropsychological aspects of planning, execution, spatial organization and implicit memory is the maze task. It also involves the operation of the intention to move towards reaching an objective and the planning of this action. The maze task consists of executing in the shortest possible time a path on a computer, the distance traversed in a single path, in a maze with one entrance and exit. Hence, it is believed that the stabilization of performance on this task may indicate the use of cognitive strategies and the formation of a program of action, which can be tested in transfer25.
Souza et al (2006)25 affirm that the maze task can be applied in the diagnostic evaluation of individuals with alterations in motor learning control and to identify what aspects are compromised during the execution of a motor task: information processing and strategic planning (number of errors), executive function (task runtime), learning (stabilization of performance) and spatial memory (maintenance of performance after distracter task and retention interval). Additionally, maze tasks have the advantage that they can be adapted to a diverse number of subjects, to the extent that they require basic motor skills, and can be applied to children, the elderly and people affected by neurological alterations25.
Thus, this work aims to investigate the process of motor learning in a maze task in children with CP in comparison to children without changes of posture and movement of the same age group. More in-depth knowledge surrounding the process of learning a motor skill in individuals with CP can contribute significantly to the adequate and effective organization of treatment programs for this population.
METHOD
This study was approved by the Ethics Committee of the University of São Paulo under protocol number 13364889. Informed consent was signed by legal guardian of the participants.
Groups
The experimental group (EG) was formed by four individuals with CP, residents in the metropolitan area of São Paulo and patients of the physiotherapy clinic of the University Center of United Metropolitan Faculties (FMU). The control group (CG) was formed by four children without changes of posture and movement. The groups were counterbalanced in relation to gender (one female and three males) and age (between seven and twelve years).
The inclusion criteria for participation in the study were: The consent to participate in the study of the patient's legally authorized representative, medical diagnosis of CP, and motor changes that characterize individuals with spastic diparesia (motor alterations more evident in lower limbs). Only participating in this study were individuals with level II CP, according to the Gross Motor Function Classification System (GMFCS), developed by Palisano et al. (1997)26. This system classifies children with CP into five levels according to motor function, which means that all the patients that were evaluated had conditions to walk without the aid of mobility devices.
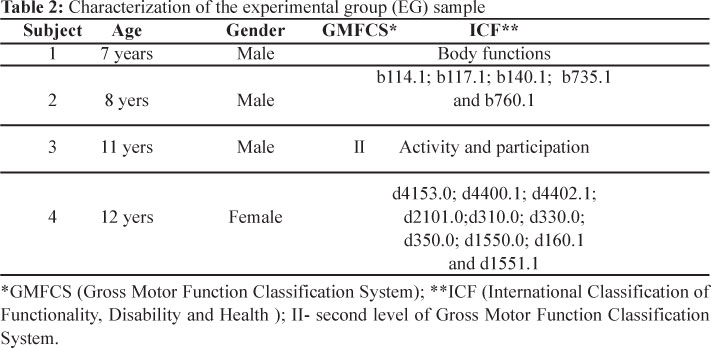
For the characterization of individuals and the composing of a homogeneous group, the International Classification of Functionality, Disability and Health (ICF)27 was also used. Gunnar and Stucki (2007)28 affirm that the ICF is an instrument that can be used for characterization of groups in scientific research. According to the World Health Organization (WHO), it is a useful classification system for the organization of homogeneous groups in scientific research, serving as a language for the classification of functionality and capacity. Therefore, the individuals selected for this study presented the same functional characteristic in the domain "body functions" (neuromusculoskeletal functions related to movement and mental functions) and the domain "activities and participation" (mobility, task performance, communication, basic skills, concentration and attention). Accordingly, considering the functions of the body, the evaluated individuals presented musculoskeletal functions related to muscle tone and the control of voluntary movements with mild impairment (b735.1 and b760.1, respectively ) and mental functions of orientation, intellectual and attention, also with mild impairment (b114.1, b117.1 and b140.1, respectively).
Considering activity and participation, as to mobility, the individuals are able to maintain seated without difficulties (d4153.0) and present mild difficulty to pick up and manipulate objects (d4400.1 and d4402.1, respectively). As to the demand task, there was no difficulty to undertake a complex task (d2101.0). In respect to communication, there were no difficulties presented in reception, production and conversation (d310.0, d330.0 and d350.0, respectively). As to learning and applying knowledge, no difficulties were presented in basic skills (d1550.0) and mild difficulty was presented in concentration/attention and complex skills (d160.1 and d1551.1, respectively).
Exclusion criteria were the presence of osteoarticular-structured deformities and surgery or chemical neuromuscular blocking within six months in the upper limbs, other associated diseases, and individuals with alterations in cognitive functions that impede collaboration and understanding of simple orders in the activities proposed.
Instrumentation and Design
Used as an instrument for evaluation, the paradigm of the maze task was used for its ease and adaptability to analyze the learning of a motor skill25. To accomplish the tasks, the author´s opted for the computer program developed by the Department of Mathematics of the Federal University of Rio Grande do Sul, presented by Souza et al. (2006), available at the site www.mat.ufrgs.br. Two drawings of mazes with only one correct path to be traversed were chosen; the first was used in the acquisition stage (AQ) and the following transfer phases (immediate transfer - IT, short-term transfer-ST and long-term transfer - LT). Figures 1 and 2 illustrate the variations of the task in each phase of the experiment.
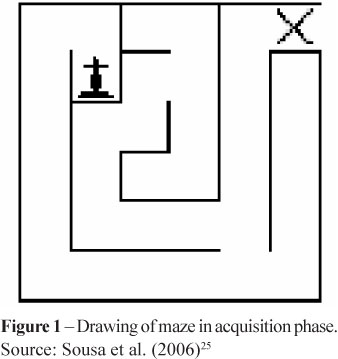
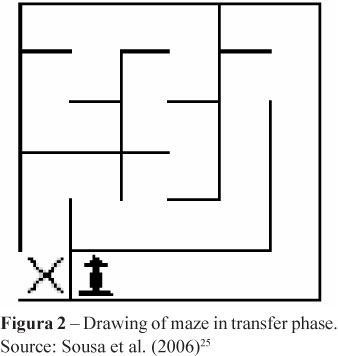
The experiment consisted of four phases (Table 1). First, the pretest was performed with three trials in order to enable the participant's knowledge of the task. In the second phase (acquisition-AQ), individuals practiced 30 trials along which the subject completed the path shown in Figure 1. The third phase, administered five minutes after the completion of AQ, was IT, which consisted of five trials using a different maze (Figure 2). In the fourth phase, ST, the subjects repeated the IT task after another five minutes of rest. The fifth and final phase was LT, executed seven days later, in which individuals performed the same task of IT and ST.
Procedures
The children were recruited individually in an appropriate room with a computer, desk and chair. One researcher was responsible for instruction and annotation of the time values on paper with the charting of the number of attempts. The values were registered by considering the total time for the completion of the task, which was provided by the program itself. The authors opted to use the maze task on the computer, on the grounds that it is a technological tool and a facilitator for individuals with CP29.
Each child was adequately positioned, sitting in front of the computer screen; the task was explained concurrently with the presentation of the maze, along which the child should traverse the path with the drawing (pointed to on the screen by the researcher) until the exit of the maze identified by an "x" (pointed to on the screen by the researcher). The child was instructed to perform the task as fast as possible using the buttons on the keyboard identified by the arrows of up, down, right side and left side.
The data were organized in blocks (BL) of six trials and analyzed through descriptive and inferential analysis.
Data analysis
In virtue of the reduced amount of observations and by the violation of the assumptions of normality and equality of variances, the data were analyzed using non-parametric techniques. Three analyses were developed:
(1) Intragroup acquisition: in order to detect the performance trends from the beginning to the end of acquisition, comparing the acquisition blocks in each of the groups separately, through the Friedman two-way analysis of variance.
(2) Intragroup transfer: comparison in each group separately between the last block of acquisition and each of the phases of transfer (Wilcoxon test).
(3) Intergroup transfer: comparison of each of the three phases separately of CG with EG performance (Mann-Whitney U test).
For all tests, the level of statistical significance adopted was 5%. The statistical program used was SPSS (Statistical Package for Social Sciences), version 13.0.
RESULTS
Following are the results that will be presented in two parts; characterization of the sample and statistical data.
a) Characterization of the sample
Below are the characteristics of the individuals of EG with age, gender, GMFCS and ICF values (Table 2).
a) Data analysis
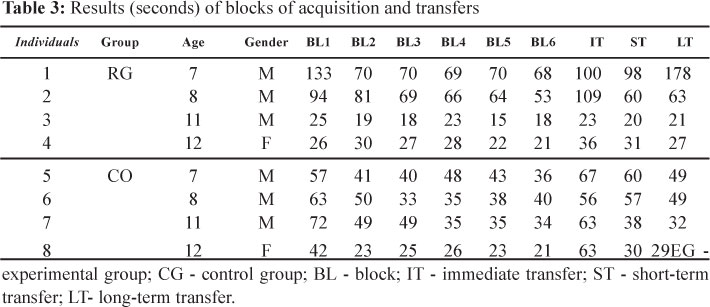
Table 3 shows the results, in seconds, of the maze task of EG and CG with the values of the six blocks of the acquisition phase, followed by the values of transfers.
(b.1) Intragroup acquisition analysis
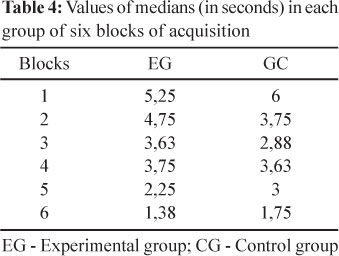
The objective of this analysis was to identify, in each of the groups, the improvement of performance throughout the six blocks of acquisition. Friedman two-way analysis of variance demonstrated significant statistical difference with both EG (X2 = 12.78, p = 0.026) and CG (X2 = 11.72, p = 0.039). The direction of differences can be identified with the inspection of medians (Table 4), which indicates, in both groups, the decrease in task runtime. Therefore, it can be inferred that there was a significantly improvement of performance for the final phase of acquisition, including the group with cerebral palsy.
b.2) Intragroup transfer analysis
Comparisons between the last block of acquisition with each block of transfer (IT, ST and LT) were performed through three paired analyses (BL6 x IT, BL6 x ST and BL6 x LT) of Wilcoxon. It was verified that there was no significant difference between BL6 and IT for both groups (z =-1.83, p = 0.07), between BL6 and ST for both groups (z= -1.83, p=0.07), and between BL6 and LT [EG (z= -1.83, p=0.07) and CG (z=-1.46, p=0.14)]. Thus, since no significant difference occurred, it can be inferred that there was adaptation to the modification of the task. This can be interpreted as reflecting that the subjects acquired the capacity to transfer what was practiced in acquisition to a new situation imposed by modification of the maze task.
(b.3) Intergroup transfer analysis
The Mann-Whitney U test, which compares the EG and CG in each of the transfers, did not indicate significant differences between groups in IT (z = 0, p = 1), ST (z =-0.15, p = 0.88) and LT (z = 0, p = 1).
DISCUSSION
The research question posed in this study was: are individuals with PC, those that have alterations in posture and the capacity of movement, able to learn a motor task and carry it out functionally, with the ability to adjust to new environmental demands? The task chosen was the maze, which employs fine motor movement for the use of the computer keyboard by upper-extremity segments; therefore, it can be considered a day-to-day motor action of great current importance29. In the maze task, children without motor changes have as the primary challenge to choose the correct path; individuals with PC have, in addition to the choice of the correct path, difficulty in performing the movement.
According to the results obtained, it was verified that the entire sample (EG and CG) presented a significant decline of task runtime between the first and last BL of acquisition. This means improvement of performance occurred with practice, which permits the analysis of transfer tests and, from them, infer the occurrence of learning. During the process, the learner passes from an initial phase, characterized by a high number of errors, inconsistency and a high demand of attention, to a later stage that is characterized by consistency, few errors and a reduced demand of attention. With practice, less unnecessary movements occur and the consequent optimization of energy and decrease in task runtime causes the sequence of movements to progressively gain more fluency and harmony. According to classic motor skill definitions, the practice with complex and intentional information involves mechanisms (perception, decision and effector) that through the learning process becomes organized and coordinated in such a way as to achieve predetermined objectives with maximum certainty and minimum expenditure of energy30,31.
Thus, practice provides functional stabilization in the task, allowing the achievement of an optimal control in execution, theoretically leading to functional standard, when the system is able to adapt to new conditions11,32. A standard of function is achieved through practice and negative feedback. Therefore, the learner goes through a process of differentiation, in which an unstable general and homogeneous state gives rise to a stable specific and heterogenic state33. In initial trials, the magnitude and variability of errors are large, characterizing the movements as inconsistent and disordered. With repetitions, the end relation to achieve the goal of the task is strengthened towards stable states. In other words, the execution of movement becomes orderly and consistent, characterized by a reduction of the magnitude and variability of errors.
It is worth emphasizing that, by comparing described values of medians in acquisition, the performance of individuals with CP was better than the individuals without CP, in the majority of blocks. This result in the acquisition can be discussed, probably, by motivation during task execution; individuals with CP proved to be more motivated, while individuals without CP appeared to have considered the task easy and unmotivating. Motivation is one of the factors that affect the motor learning process, especially in the acquisition phase, because it enables better information processing, favoring the retention and transfer that was acquired through the process of practice11,13,32. Also in this context, motivation also seems to affect the performance of motor skills, since the learner has to pay more attention in the execution of the task, increasing involvement and participation34-36.
The most important results of this study concern the comparisons within and between groups in transfer, since the modification of the task requires the capacity of adaption from the learners. The main goal of practice is not to facilitate the performance of temporary effects during acquisition but provide better lasting performance (attributed to learning) in tests of retention and transfer11,13,37,38. Thus, a fundamental aspect of motor learning is that skills are performed in environments that demand constant capacity of adapttion11,13. This adaptation, however, only occurs where situations challenging the capacity of movement have already been acquired, so that new structures of action have to be formed to meet the requirements imposed by the environment. Hence, initially the individual needs to identify the motor problem that, as an example, can be placed in a maze task.
Maze tests allow the possibility to evaluate various neuropsychological aspects, such as executive function, spatial learning and implicit memory25. After identifying the problem, the subject needs to formulate a plan of action, which should generate a hypothesis as to how it would be possible to achieve this goal, predicting and anticipating the implementation of the action. The next step is to put into practice the established plan of action, transforming a mental image into effective movements. In this phase, a complex muscular system must be coordinated so that various muscles are activated in an organized way. Because transforming plans of action into movement are rarely perfect in initial trials, individuals need to analyze the errors and try to correct them in following trials. When the cycle described above is repeated enough, the transition occurs from uncoordinated actions of great cognitive demand to highly accurate movements, where complex neuromuscular synergies are activated with minimal involvement of attention. This process is called learning19.
The intragroup analysis of the last block of acquisition for each of the transfers indicated absence of differences in both groups. Therefore, a more complex situation, task alteration, did not elicit a significant drop in performance. Accordingly, the subjects with CP and the subjects of CG presented good adaptability to a different version of the maze task. The analysis between the groups in transfer confirm the good capacity of adaption of both groups without differences between them, given the absence of significant performance difference (task runtime) between EG and CG, in all tests of transfer.
Therefore, CP does not appear to have had an influence on the performance of the modified maze task, a fact that is interesting, both in the point of view of the characterization of the subjects with CP and intervention with this population. The initial hypothesis of task difficulty for learners with CP was not corroborated, perhaps because in the acquisition phase, motivation and perseverance of the CP learners were greater when compared to learners without CP. This could have offset possible differences in the comparison between groups in the transfer phase. One of the characteristics of motor skill acquisition is the execution of motor tasks with reduced time. Similar times between the groups in the modified maze task (transfer) probably reflected similar capabilities in information processing speed. Many motor tasks require quick responses to environmental stimuli, as well as quick adjustments or corrections based on the results of previous performances. A significant factor in the speed of central processing is the amount of information elicited from the complexity of information, the time required to process the information and the individual's capacity to process the information39,40. It seems that all participants of the present study were able to deal satisfactorily with these three variables. This finding could have important insights for intervention with people with CP, not only in rehabilitation but also in practice of physical activity.
The findings of this present study could be contrasted with a small number of studies that were conducted with individuals with CP within the scope of motor learning. The fact that individuals with CP have learned a task supports the findings of Hemayattalab and Rostami (2010)41, Reid (2002)42 and Chen et al. (2007)43 with tasks of dart throwing and virtual reality, in which individuals with CP have improved the quality of movement. Some authors44,45 have chosen to investigate the learning of individuals with CP through changes in neural structures (via neuroimaging examinations) and have verified the occurrence of learning in regards to neural, detecting activation in cortical areas and correlations between performance in executing motor tasks and brain activity in different encephalitic areas.
Because there are few studies using knowledge derived from motor learning in individuals with CP, it is important to emphasize the need for further studies to better understand the factors that affect the acquisition of motor skills in this particular population. It has been suggested that future investigations into motor learning can manipulate different forms of practice (variability, distribution, and fractionation) and information (extrinsic feedback, demonstration/instruction, establishment of goals and internal/external focus) to the learner with CP. The variability of practice, which consists of variations in characteristics of context or variations of motor task being practiced, seems to be a priority, given its direct involvement in the interventions proposed for these subjects. In individuals with mental impairment, varied practice proved to be successful to provide the learner the capacity to adapt to new situations (transfer test)46; in individuals with CP, the role of variation has been identified as fundamental in generating elaborated motor strategies47.
CONCLUSION
In the process of learning a maze task, both individuals with CP and individuals without CP presented improved performance, observed through the decrease of runtime throughout acquisition. Regarding learning, measured through transfer tests, individuals with CP showed capacity of adaptation equivalent to individuals without CP.
REFERENCES
1. Aicardi J, Bax M. Cerebral palsy. In: Aicardi J. Diseases of the nervous system in childhood. Clinics in developmental medicine. London: Mac Keith Press; 1992. p. 334-932. [ Links ]
2. Stokes M. Neurologia para Fisioterapeutas. São Paulo: Premier; 2000. [ Links ]
3. Parker DF, Carriere L, Hebestreit H, Salsberg A, Bar OR. Muscle Performance and Gross Motor Function of Children With Spastic Cerebral Palsy. Develop-mental medicine and child neurology. 1993;35(1):17-23. [ Links ]
4. Boyce WF, Gowland C, Rosenbaum PL, Lane M, Plews N, Goldsmith CH, et al. The Gross Motor Performance Measure: Validity and Responsiveness of a Measure of Quality of Movement. Physical therapy. 1995;75(7):603-613. [ Links ]
5. Edwards S. Neurological physiotherapy. New York: Churchill Livingstone; 1996. [ Links ]
6. Bax M. Medical aspects of cerebral palsy. In: Finnie NR. Handling the young child with cerebral palsy at home. 3rd ed. London: Butterworth-Heinemann; 1997. [ Links ]
7. Diament A, Cypel S. Neurologia infantil. 4th ed. São Paulo: Atheneu; 2005. [ Links ]
8. Papavasiliou AS. Management of motor problems in cerebral palsy: A critical update for the clinician. Eur J Paediatr Neurol. 2009; 13(5): 387-396. [ Links ]
9. Bax M. Diagnostic assessment of children with cerebral palsy. Lancet Neurol. 2004;3:395. [ Links ]
10. Cans C. Surveillance of cerebral palsy in Europe: a collaboration of cerebral palsy surveys and registers. Dev Med Child Neurol. 2007;42(12):816-824. [ Links ]
11. Tani G. Aprendizagem motora: tendências, perspectivas e problemas de investigação. In: Tani G. Comportamento motor: aprendizagem e desenvolvimento. Rio de Janeiro: Guanabara Koogan; 2005. [ Links ]
12. Holmefur M, Krumlinde-Sundholm L, Bergstrom J, Eliasson A. Longitudinal development of hand function in children with unilateral cerebral palsy. Develop-mental Medicine & Child Neurology. 2009; 52(4): 352-357. [ Links ]
13. Magill R. A. Aprendizagem motora: conceitos e aplicações. 5th ed. São Paulo: Edgard Blücher; 2000. [ Links ]
14. Manoel EJ. A dinâmica do estudo do comportamento motor. Revista Paulista de Educação Física. 1999;13:52-61. [ Links ]
15. Lemieux TS, Penhune VB. The effects of practice and delay on motor skill learning and retention. Experimental Brain Research. 2005;161:423-431. [ Links ]
16. Lent R. Cem bilhões de neurônios: conceitos fundamentais de neurociência. São Paulo:Atheneu; 2001. p. 587-617. [ Links ]
17. Schmidt R, Wrisberg C. Aprendizagem e performance motora: uma abordagem da aprendizagem baseada no problema. 3rd ed. Porto Alegre: Artmed; 2001. [ Links ]
18. Adams JA. A closed-loop theory of motor learning. Journal of Motor Behavior. 1971; 3:111-50. [ Links ]
19. Teixeira LA. Aprendizagem de habilidades motoras na ginástica artística. In: Nunomura M, Nista-Piccolo VL. Compreendendo a ginástica artística. São Paulo: Phorte; 2004. [ Links ]
20. Kleim JA, Jones TA. Principles of experience-dependent neural plasticity: implications for rehabilitation after brain damage. Journal of Speech, Language, and Hearing Research. 2008; 51: 225-239. [ Links ]
21. Mulder TA. A process-oriented model of human motor behavior: toward a theory-based rehabilitation approach. Physical Therapy. 1991; 71: 157-64. [ Links ]
22.7 Carr JH, Shepherd RB. The changing face of neurological rehabilitation. Revista Brasileira de Fisioterapia. 2006; 10(2):147-56. [ Links ]
23. Salmoni A, Schmidt RA, Walter CB. Knowledge of results and motor learning: A review and critical reappraisal. Psychological Bulletin. 1984; 95: 355-386. [ Links ]
24. Emanuel M, Jarus T, Bart, O. Effects of focus of attention and age on motor acquisition, retention, and transfer: a randomized trial. Physical Therapy. 2008; 88(2): 251-60. [ Links ]
25. Souza DE, França FR, Campos TF. Teste de Labirinto: Instrumento de Análise na Aquisição de uma Habilidade Motora. Revista Brasileira de Fisioterapia. 2006; 10(3): 355-60. [ Links ]
26. Palisano R, Rosenbaum P, Walters S, Russel DJ, Wood EP, Galuppi P. Development and reliability of a system to classify gross motor function in children with cerebral palsy. Dev Med Child Neurol. 1997; 39: 214-23. [ Links ]
27. CIF - Classificação Internacional de funcionalidade, Incapacidade e Saúde/ [Centro Colaborador da Organização Mundial da Saúde para Família de Classificações Internacionais, organização e coordenação da tradução Cássia Maria Buchalla]. São Paulo: Editora da Universidade; 2003. [ Links ]
28. Gunnar G, Stucki G. Organizing human functioning and rehabilitation research into distinct scientific fields. Part II: Conceptual descriptions and domains for research. Journal of rehabilitation medicine. 2007;39(4): 293-8. [ Links ]
29. Sullivan KJ, Kantak SS, Burtner PA. Motor Learning in Children: Feedback Effects on Skill Acquisition. Physical Therapy. 2008; 88(6):720-32. [ Links ]
30. Benda RN. Sobre a natureza da aprendizagem motora: mudança e estabilidade... e mudança. Revista Brasileira de Educação Física. 2006; 20(5): 43-45. [ Links ]
31. Pellegrini AM. A aprendizagem de habilidade motoras I: o que muda com a prática? Revista Paulista de Educação Física. 2000; 3: 29-34. [ Links ]
32. Choshi K. Aprendizagem motora como um problema mal-definido. Rev. paul. Educ. Fís. 2000; 3: 16-23. [ Links ]
33. Bertalanffy LV. Teoria geral dos sistemas: aplicação à psicologia. In: Anohin PK, Bertalanffy LV, Rapoport A, Mackenzie WJM, Thompson JD. Teoria dos sistemas. Rio de Janeiro: Fundação Getúlio Vargas; 1976. [ Links ]
34. Paim MCC. Fatores motivacionais e desempenho no futebol. Revista da Educação Física/UEM. 2001; 12(2): 73-79. [ Links ]
35. Valenteini NC. A influência de uma intervenção motora no desempenho motor e na percepção de competência de crianças com atrasos motores. Rev. paul. Educ. Fís. 2002; 16(1); 61-75. [ Links ]
36. Shumway-Cook A, Woollacott MH. Controle motor. Teoria e aplicações práticas. 2nd ed. São Paulo: Manole; 2003. [ Links ]
37. Karni A, Meyer G, Rey-Hipolito C, Jezzard P, Adams MM, Turner R, et al. The acquisition of skilled motor performance: fast and slow experience-driven changes in primary motor cortex. Proceedings of the National Academy of Sciences. 1998; 95: 861-68. [ Links ]
38. Wulf G, Shea G, Lewthwaite R. Motor skill learning and performance: a review of influential factors. Med Educ. 2010; 44: 75-84. [ Links ]
39. Chiviacowsky S, Neves C, Locatelli L, Oliveira C. Aprendizagem motora em crianças: efeitos da freqüência autocontrolada de conhecimento de resultados. Rev. Bras. Cienc. Esporte. 2005; 26(3): 177-190. [ Links ]
40. Chiviacowsky S, Kaefer A, Medeiros FL, Pereira FM. Aprendizagem motora em crianças:"feedback" após boas tentativas melhora a aprendizagem?. Rev. bras. Educ. Fís. Esp. 2007; 21(2): 57-65. [ Links ]
41. Hemayattalab R; Rostami LR. Effects of frequency of feedback on the learning of motor skill in individuals with cerebral palsy. Research in Developmental Disabilities. 2010; 31: 212-217. [ Links ]
42. Reid D. The use of virtual reality to improve upper-extremity efficiency skills in children with cerebral palsy: a pilot study. Tech Disabil. 2002;14:53-61. [ Links ]
43. Chen YP, Kang LJ, Chuang TY, Doong JL, Lee SJ, Tsai MW, et al. Use of Virtual Reality to Improve Upper-Extremity Control in Children With Cerebral Palsy: A Single-Subject Design. Physical Therapy. 2007;87(11): 1441-57. [ Links ]
44. Rieckmann A; Bäckman L. Implicit Learning in Aging: Extant Patterns and New Directions. Neuropsychol Rev. 2009;19:490-503. [ Links ]
45. Orban P, Peigneux P, Lungu O, Albouy G, Breton E, Laberenne F, et al. The multifaceted nature of the relationship between performance and brain activity in motor sequence learning. NeuroImage. 2010; 49: 694-702. [ Links ]
46. Hemayattalab R, Movahedi A. Effects of different variations of mental and physical practice on sport skill learning in adolescents with mental retardation. Research in Developmental Disabilities. 2010; 31: 81-86. [ Links ]
47. Straub K, Obrzut JE. Effects of Cerebral Palsy on Neuropsychological Function. J Dev Phys Disabil. 2009; 21:153-167. [ Links ]
 Author responsible for correspondence:
Author responsible for correspondence:
Prof. Dr. Carlos Bandeira de Mello Monteiro
Work carried out in Physiotherapy Department
University Center of United Metropolitan Faculties
Rua Fidêncio
Ramos, 128 Apt 22
CEP 04551-010
Tele: +55 11 9953 0716
Email: carlosfisi@uol.com.br


{kind=link}
{kind=link}
{kind=link}