










Serviços Personalizados
artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282
Rev. bras. crescimento desenvolv. hum. vol.21 no.3 São Paulo 2011
ORIGINAL RESEARCH
The SINASC descentralization and the completeness of variables on birth certificates, in municipalities of Minas Gerais from 1998 to 2005
Eliete Albano de Azevedo GuimarãesI; Antônio Ignácio de Loyola FilhoII; Zulmira Maria de Araújo HartzIII; Antônio José de MeiraIV; Zélia Maria Profeta LuzV
IDoutoranda
do Curso de Pós-Graduação em Ciências da Saúde
do Centro de Pesquisas René Rachou, FundaçãoOswaldo Cruz
- CPqRR/FIOCRUZ. Belo Horizonte, Minas Gerais. Professora do Curso de Enfermagem
do CampusCentro Oeste da Universidade Federal de São João Del
Rei, Minas Gerais
IIPesquisador do Centro de Pesquisas René Rachou, Fundação
Oswaldo Cruz -CPqRR/FIOCRUZ. Belo Horizonte, MinasGerais. Professor do Departamento
de Enfermagem Aplicada da Escola de Enfermagem da Universidade Federal deMinas
Gerais
IIIPesquisadora da Escola Nacional de Saúde Pública,
Fundação Oswaldo Cruz/ENSP/FIOCRUZ. Manguinhos, Rio deJaneiro
IVDiretor da Gerência de Inteligência Epidemiológica
da Secretaria de Estado de Saúde de Minas Gerais. CidadeAdministrativa,
Belo Horizonte, MG
VPesquisadora do Centro de Pesquisas René Rachou, Fundação
Oswaldo Cruz -CPqRR/FIOCRUZ. Belo Horizonte, Minas Gerais
ABSTRACT
Live Birth Information System (SINASC) was decentralized to improve information quality and its use. This study evaluated completeness of variables on mother and pregnancy, newborn, and childbirth, available on System database between 1998 and 2005. The study was carried out in 38 municipalities in the state of Minas Gerais. The assessment took into consideration population size and condition of municipalities management. Percentage of fields not filled out was defined as an indicator, and the standard of quality adopted was based on Mello Jorge et al. (1996). Values between 90% and 100% were considered adequate; 70% - 89.9% were not adequate, and critical when they were smaller than 70%. In general, in all municipalities evaluated there was improvement in Birth Certificates (DNV) filling throughout the period examined. It was observed important reduction of incompleteness in the variables race/color, education degree, marital status, children live births and dead birth. The decentralisation of the Information on the SINASC has enabled an improvement on information completeness in studied municipalities, regardless of the size and condition of municipalities management.
Key words: information systems; birth certificates; live births;
INTRODUCTION
The 1988 Brazilian constitution recognised health as a citizen's right and established the basis for the creation of the Unified Health System (SUS), which was based on the principles of universality, integrality, and social participation. The SUS aims to provide universal preventive and curative care through decentralised management1.
The decentralization of health services involves not only changes in health care model, but also enables creation of a network of relations that promotes community participation at all administrative levels, which contributes to democratization of public policies of management health1-2. It is a gradual and complex process which runs through a field with numerous obstacles and contradictions2.
The Laws of Health (8080/1990, 8142/1990, NOB-SUS 1991, 1993, 1996; NOAS-SUS 2001 and 2002) redefined institutional roles, co-responsibility between the government levels, system management, planning and control, and resources transfer to the collective and individual actions. In addition, these normative instruments have established rules and targets which are forcing brazilian municipalities front to need to organize information in health produced at the local level, enabling it to respond with greater agility and specificity of new logic managerial and redirection of sector. Health information systems have become instances of governability and negotiation between managers of three levels of government3-4.
SINASC - Live Births Information System, which was introduced in 1990 by Brazilian Health Ministry, was decentralized to all municipalities. SINASC data source is the Birth Certificates (DNV), an individualized document that must be completed for all live births occurred in the country on hospitals or at home3,5.
System comes in, mostly, to improve information relating to newborn, mother and conditions of birth6 and enable also monitoring quality of produced data in terms of coverage7, reliability8-9 and completeness of information10-12. Variables, such as birth weight, length of gestation, type of birth, age maternal education degree and parity are used in the construction of health and demographic indicators of a population, and evaluated in agreements of primary care and in planning of surveillance actions in health13. Although it is a specific system, information of SINASC, when accessible to managers and the community, can contribute to the planning of health actions focused on this populacional segment13.
In spite of normative and institutional advances and on health information policy, the decentralization of SINASC has presented barriers in its operationalization, mainly in relation to effectiveness of its informations13.
For some municipalities in the state of Minas Gerais (MG), the implantation of SINASC began in 1994, but for the majority of them, decentralization has started in 199814. In spite of improvement information quality in the State, there are still gaps in informational process, in particular in collection, processing and use of data14-16. Variations in coverage and quality of data are still verified, what can be related to the differentiated form with which decentralization of system in municipalities occurred.
In this context, evaluative studies are essential, allowing determine the value or meaning of an activity, program or policy, as well as to correct or improve actions to increase relevance, effectiveness and efficiency of health activities17. In this study the objective was to evaluate completeness of Birth Certificates in municipalities of MG from 1998 to 2005.
MethodS
This work is a normative assessment of completeness of Birth Certificate in the municipalities of MG from 1998 to 2005. The assessment is considered normative when it is done according to the defini-tions of standards and criteria17-18. The criteria used to evaluate the DNV completeness, in this study, followed the parameters proposed by Melo Jorge et al6.
According to the Master Plan for Regionalization of Minas Gerais (PDR), the state is divided into 13 Health Macroregions, considered the territorial basis of health care planning, on the basis of demographic and socioeconomic characteristics, geographical, sanitary and epidemiological, provision of services and relations between municipalities. These macro-regions are divided into 75 micro-regions that cover the universe of 853 municipalities in 28 Regional Health Managers, which differ in socio-sanitary, size and form of management19.
In this study were selected from the National Register of Health Establishment (CNES), 394 municipalities from Minas Gerais with health establishments where occur births. These were classified according to the following parameters: regional location in PDR19 and population size.
On the basis of inhabitant number, three categories of population size were considered by the authors: municipalities with less than 10.000 inhabitants considered small; municipalities with 10.000 to 49.999 inhabitants, medium-sized and municipalities with over than 50.000 inhabitants, considered large.
Evaluated municipalities
For the evaluation 38 municipalities were randomly selected, among the 394, three municipalities in each macro-region of health, with a municipality for each size in each of the macro-regional; except Jequitinhonha Macro-region, which were selected two municipalities (medium and small size), since in this region there is no large. These were classified according to the condition of municipalities management in Unified Health System (SUS), being 24 municipalities authorized in Full Primary Care Management (GPAB) and 14 qualified to Full Municipal System Management (GPSM).
Data Collection
The data were obtained by means of a CD-Rom with the consolidated information on live births for the period 1998 to 2005, available by Health Surveillance Secretariat of Health Ministry20-21.
The population studied was composed by the total number of live births of resident mothers in the municipalities studied, between 1998 and 2005. The beginning of the SINASC decentralization for the municipalities of Minas Gerais was in 1998 and 1999. For this reason, in this study, we consider that the years 2000 and 2005 correspond to the period post-descentralization14.
Analysis of the data
The information of live birth were analyzed based on variables related to the child (gender, birth weight, race/color, Apgar 1º minute and Apgar 5º minute), to motherly attributes (age, level of instruction, marital status, number of children born alive and number of children born dead) and to pregnancy and childbirth (duration of pregnancy, number of prenatal visits, type of pregnancy and type of parturition). Used concepts and definitions in each variable were those recommended by Health Ministry, according to the Manual of Instructions for DNV completing5.
To analyze incompleteness of variables, percentage of fields not filled were defined as indicator , these being blank fields and fields with the code 9 (ignored) 5. Despite the lack of methodological clear in SINASC's manual filling, that was the option for analysis of completeness of variables in face of operational difficulties, since data tabulation provided by the Ministry of Health does not allow to differentiate the variables that do not were filled (blank) of those who were actually ignored by the informant11.
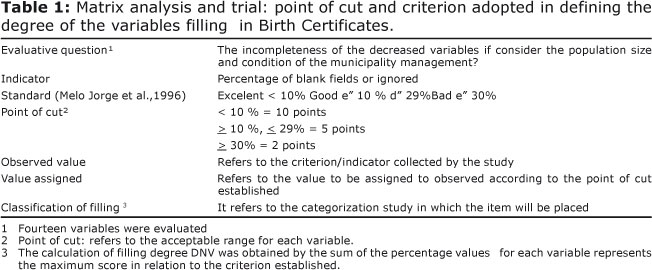
The quality criterion adopted was defined by Mello Jorge et al.6, which is based on percentage of incompleteness of filling in fields of DNV (filling as ignored/blank). The filling is considered excellent when these percentages do not exceed 10.0%, is considered good when the percentage range between 10.0% to 29.9 % and is considered bad when this percentage is higher than 30.0%.
It was calculated the average of percentage of incompleteness of each variable to the set of municipalities, according to population size and condition of municipalities management at SUS.
On the basis of observed percentage of completeness , scores were attributed for each variable. Thus, the variables with excellent quality of filling received 10 points, the good quality received five points, and the poor quality received two points. Calculation of DNV filling degree was obtained by percentage represented by sum of values found for each variable, in relation to maximum score achievable in the variable. Values between 90% and 100% were considered adequate; 70% - 89.9% were not adequate, and critical when they were smaller than 70% (Table 1).
For the analysis of the data was used the Microsoft Office Excel 2007.
This study was approved by Ethics Committee of René Rachou Research Center /FIOCRUZ (0001.0245.000-09).
RESULTS
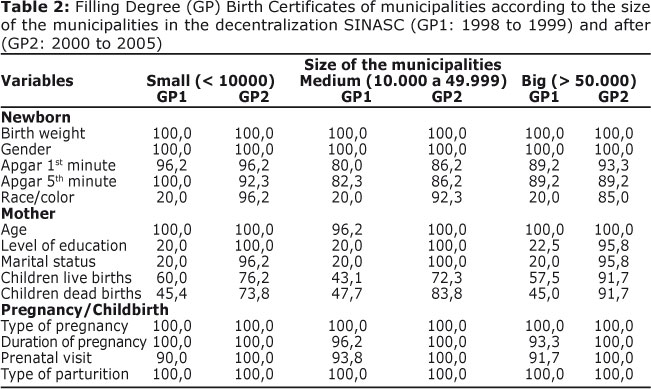
With SINASC decentralization, it has been found, for studied municipalities, regardless of size and condition of municipalities management, adequate filling (90% - 100%) for most of the variables present in DNV (Tables 2, 3).
In assessing the size of the municipalities, all variables related to child showed an increase in the degree of filling DNV. The completeness of birth weight and gender was considered adequate before and after the decentralization of SINASC. In the variables, Apgar index in the first minute, and Apgar index in the fifth minute, the filling ranged from not adequate (70% to < 89.9 %) till appropriate (90 % -100 %). The biggest increase in the filling degree of DNV among the variables related to the child was found in the variable race/color, considering that this field presented critical filling in the first two years of implementation of SINASC (Table 2).
In relation to the filling of maternal characteristics, except for maternal age, which was appropriate for all sizes from its implementation, all the other variables showed improvement for completeness after the year 2000. The education level, marital status, children live births and dead births were the worst filling - for the first two years, from critical (< 70 %) till not appropriate (70% to < 89.9% ). However, it was noted that an important increase in the filling degree of these variables, especially to large size municipalities, that had adequate filling to all of them. In small and medium-sized municipalities were observed inadequate filling on the variables children live births and dead births.
All of the variables related to pregnancy and parturition had adequate filling for all the municipalities, in both evaluated periods.
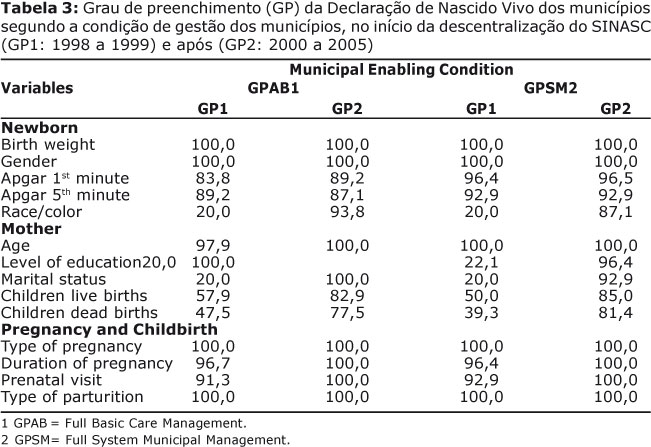
The analysis results of the variables according to the condition for the management of the municipalities listed in Table 3, showed that the fields relating to birth weight, newborn gender, mother's age, duration of pregnancy, type of pregnancy, type of parturition and prenatal consultation showed adequate completeness and little changed during the periods. It was found important increase in the degree of filling in the variables race/color, degree of education, marital status, children born dead and live births (Table 2). Considering the variables live births and children born dead, the filling is still not adequate among the municipalities evaluated, regardless of the condition for the management of the municipalities in SUS. And the completeness of the variable race/color is still inadequate among the municipalities in GPSM. The variables, Apgar Index in first minute and Apgar Index in fifth minute were stable in both periods, with better fill in all the municipalities qualified as GPSM.
DISCUSSION
Although the study do not portray the information quality of SINASC from the perspective of its process, it was observed that the decentralization of the Information System, in all of the municipalities evaluated, regardless of population size and the condition for the management favored the improvement of the filling of the information in the DNV, corroborating other studies in different places of the country10-12,22-24.
It is understood that the municipal management imbued with the power to assess, plan, and decide actions aimed to monitor the information about live births depending on the context and interests, valuing the use of health information. The process of decentralization of government policies for health has produced advances with the permanent constitution of negotiations, pacts and legal framework. Whereas the indicators pacts maternal-infant and of coverage in primary health care and health surveillance, it requires of the managers greater proximity to the SINASC and with the source of capitation events, involving the monitoring of the data13 collection. In addition, a possible explanation is that in the process, there was a breakthrough in information policy and technology in health systems3.
Among the variables assessed, highlight the relating to birth weight, newborn gender, ,age of the mother and all the fields relating to pregnancy and childbirth (duration of pregnancy, the number of prenatal visits, type of pregnancy and type of parturition) that presented the best completeness, maintaining adequate during the periods. This information is available in the medical records of newborn and the puerperal or the pregnancy card, which facilitates recording of data9.
In relation to variables Apgar 1st. minute and Apgar 5th minute, it was observed that the degree of filling ranged from not adequate till adequate over the years. The best results were observed in all the municipalities authorized in GPSM. Costa and Frias12 have questioned the reliability of the information, since that the data filled by non-qualified professionals - those who do not have technical knowledge to assign the value on the conditions of the child vitality in 1st and 5th minute - tend do not be filled in, or can be filled with addiction, repeating the same value.
The fields of DNV related to race/color of the child, the degree of maternal education, marital status, children live births and dead births presented the greatest variation of completeness. Even in the municipalities evaluated for small and medium-size are still the filling not adequate for the variables children live births and dead births. Mello Jorge et al.6 already demonstrated the same in the first studies to evaluate the SINASC, and problems with these variables are still observed in more recent studies10-12,24. It is possible that the incompleteness records of these variables be done in some questions such as: deficiencies related to the lack of qualified human resources; lack of constant involvement of the different professionals who deal with health information, including managers; lack of knowledge of responsible professional for filling in DNV; lack of information in the medical records of puerperal and newborn, up to the ignorance of certain information by accompanying and subjectivity involved in the definition of the variables categories, especially of race/color of the newborn12,24-25.
The results of this study were similar to the research performed in a state of northeast12, even using different methodologies, express evidence in relation to the quality of information from SINASC. Costa & Frias12 to evaluate historical evolution of completeness in DNV in Pernambuco, between 1996 and 2005, saw important increase in the percentage of municipalities with excellent completeness, highlighting the variable race/color, maternal schooling, maternal marital status and number of prenatal visits. They reported that unfortunately, in some localities, incompleteness are still checked in variable number of live births, the number of children born dead, Apgar 1st minute and Apgar 5th minute.
In another study, Mello Jorge et al.10 to analyze the quality of brazilian vital statistics from design and deployment of SINASC verified that the information of the DNV is improving dramatically, both coverage and completeness of their data. They reported that the biggest incompleteness fields are due to the variables color/race of the child, Apgar 1st minute and Apgar 5th minute, maternal education, children live births and dead births.
Romero Anol Cunha11 recognized in federal units in 2002, differences in the percentage of incompleteness of DNV. By using the variables in white along with the ignored variables as the unit of analysis, the authors observed that the variables of maternal age, gender of the newborn, marital status, level of education and birth weight had good to excellent completeness, while the fields relating to reproductive history mother, children live births and dead births were filling of bad to regulate.
In Minas Gerais, in the year 2000, Souza16 showed larger incompleteness 10% in the variables, number of living children, number of dead children, race/color, Apgar 1st minute and Apgar 5th minute.
Recent study conducted in Teresina24 pointed trend of quality improvement of filling in the DNV, with good filling the form, except for the variable number of dead children that presented incompleteness between 10% and 29.9%.
This study showed improvement in the information quality of SINASC after its decentralization; however, further studies are required for the evaluation related to the structure, process and the impact of the information generated by the System. Only in this way it will be possible to check if this information of quality is used in the monitoring process, evaluation and decision of health care to the child and the woman.
Acknowledgments: The authors thank the Health Secretariat of Minas Gerais for helpful comments.
Funding: Foundation for Research of the Minas Gerais - FAPEMIG; Oswaldo Cruz - Fiocruz Foundation - FIOCRUZ.
REFERENCES
1. Vieira da Silva LM. Avaliação do processo de descentralização das ações de saúde. Ciênc Saúde Coletiva. 1999; 4(2):331-339. [ Links ]
2. Ferla AA, Leal MB, Pinheiro, R. Um olhar sobre práticas avaliativas em descentralização do sistema de saúde: construindo uma abordagem analítica para atuação em rede. In: Pinheiro R, Mattos RA. Gestão em Redes. Práticas de Avaliação, formação e participação na Saúde. Rio de Janeiro: CEPESC; 2006. [ Links ]
3. Brasil. Ministério da Saúde. Portaria Nº 116, de 11 de fevereiro de 2009. Regulamenta a coleta de dados, fluxo e periodicidade de envio das informações sobre óbitos e nascidos vivos para os Sistemas de Informação em Saúde sob a gestão da Secretaria de Vigilância em Saúde. Ministério da Saúde, Secretaria de vigilância em Saúde; 2009. [ Links ]
4. Branco MA. Informação e Saúde: uma ciência e suas políticas em uma nova era. Rio de Janeiro: Fiocruz; 2006. [ Links ]
5. Brasil. Fundação Nacional de Saúde. Manual de instruções para o preenchimento da declaração de nascido vivo. Brasília: Centro de Documentação do Ministério da Saúde; 2001. [ Links ]
6. Mello-Jorge MHP, Gotlieb SL, Sabolli ML, Almeida MF, Latorre MR. O Sistema de Informação sobre Nascidos Vivos: primeira avaliação dos dados brasileiros. Inf Epidemiol SUS. 1996; 2:15-48. [ Links ]
7. Frias PG, Pereira DMH, Vidal AS, Lira PIC. Avaliação da cobertura do Sistema de Informações sobre Nascidos Vivos e a contribuição das fontes potenciais de notificação do nascimento em dois municípios de Pernambuco, Brasil. Epidemiol e Serviços de Saúde. 2007; 16(2): 93-101. [ Links ]
8. Silva AAM, Ribeiro VS, Borba Júnior AF, Coimbra LC, Silva RA. Avaliação da qualidade dos dados do sistema de informações sobre nascidos vivos em 1997 - 1998. Rev Saúde Pública. 2001; 35(6): 508-514. [ Links ]
9. Theme Filha MM, Gama SGN, Cunha CB, Leal MC. Confiabilidade do Sistema de Informações sobre Nascidos Vivos Hospitalares no Município do Rio de Janeiro, 1999-2001. Cad Saúde Pública. 2004; 20 Suppl 1:83-91. [ Links ]
10. Mello-Jorge MHP, Laurenti R, Gottlieb SLD. Análise da qualidade das estatísticas vitais brasileiras: a experiência de implantação do SIM e do SINASC. Cienc Saúde Coletiva. 2007; 12(3):643-54. [ Links ]
11. Romero ED, Cunha CB. Avaliação da qualidade das variáveis epidemiológicas e demográficas do Sistema de Informações sobre Nascidos Vivos, 2002. Cad Saúde Pública. 2007; 23(3):701-714. [ Links ]
12. Costa JMBS, Frias PG. Avaliação da completitude das variáveis da Declaração de Nascido Vivo de residentes em Pernambuco, Brasil, 1996 a 2005. Cad Saúde Pública. 2009; 25(3): 613-624. [ Links ]
13. Almeida MF, Alencar GP. Informações em Saúde: necessidade de introdução de mecanismos de gerenciamento dos sistemas. Inf Epidemiol SUS. 2000; 4:241-249. [ Links ]
14. Minas Gerais. Superintendência de Epidemiologia. Análise de situação de saúde de Minas Gerais. SES/MG; 2007. [ Links ]
15. Drumond EF, Machado CJ, França E. Subnotificação de nascidos vivos: procedimentos de mensuração a partir do Sistema de Informação Hospitalar. Rev Saúde Pública. 2008; 42(1): 55-63. [ Links ]
16. Souza LM. Avaliação do Sistema de Informação sobre Nascidos Vivos - SINASC, Minas Gerais e Mesoregiões, 2000 (Dissertação de mestrado). Belo Horizonte (MG): CEDEPLAR/FACE/UFMG; 2004. 112 p. [ Links ]
17. Hartz ZM, Vieira da Silva LM (Orgs.). Avaliação em Saúde: dos modelos teóricos à prática na avaliação de programas e sistemas de saúde. Rio de Janeiro: Fiocruz; 2005. [ Links ]
18. Contandriopoulos AP, Champagne F, Denis JL, Pineaut RA. Avaliação na área da saúde: conceitos e métodos. In: Hartz ZMA (Org.). Avaliação em saúde: dos modelos conceituais à prática na implantação de programas. Rio de Janeiro: Fiocruz; 1997. [ Links ]
19. Minas Gerais. Plano Diretor de Regionalização de Minas Gerais. Secretaria de Estado de Saúde de Minas Gerais, 2010. [Acesso em: 29 dez 2010]. Disponível em: http://www.saude.mg.gov.br/politicas_de_saude/plano-diretor-de-regionalizacao-pdr [ Links ]
20. Brasil. Ministério da Saúde. Banco de dados dos sistemas de informação sobre mortalidade (SIM) e nascidos vivos (SINASC) 1998 a 2004 (CD-ROM). Brasília: MS/SVS; 2006. [ Links ]
21. Brasil. Ministério da Saúde. Banco de dados dos sistemas de informação sobre mortalidade (SIM) e nascidos vivos (SINASC), 1999 a 2005 (CD-ROM). Brasília: MS/SVS; 2007. [ Links ]
22. Barbuscia DM, Rodrigues-Júnior AL. Completude da informação nas Declarações de Nascido Vivo e nas Declarações de Óbito, neonatal precoce e fetal, da região de Ribeirão Preto, São Paulo, Brasil, 2000-2007. Cad. Saúde Pública. 2011; 27(6):1192-1200. [ Links ]
23. Silva GFS, Aidar T, Mathias TAF. Qualidade do Sistema de Informações de Nascidos Vivos no Estado do Paraná, 2000 a 2005. Rev Esc Enferm USP. 2011; 45(1):79-86. [ Links ]
24. Mascarenhas MDM, Gomes KRO. Confiabilidade dos dados do Sistema de Informações sobre Nascidos Vivos em Teresina, Estado do Piauí, Brasil - 2002. Cienc Saúde Coletiva. 2011; 16(1):1233-1239. [ Links ]
25. Almeida MF, Alencar GP, França Junior I, Novaes HMD, Siqueira AAF, Scchoeps D, et al. Validade das informações das declarações de nascidos vivos com base em estudo de caso-controle. Cad Saúde Pública. 2006; 22(3):1-9. [ Links ]
13. Almeida MF, Alencar GP. Informações em Saúde: necessidade de introdução de mecanismos de gerenciamento dos sistemas. Inf Epidemiol SUS. 2000; 4:241-249. [ Links ]
14. Minas Gerais. Superintendência de Epidemiologia. Análise de situação de saúde de Minas Gerais. SES/MG; 2007. [ Links ]
15. Drumond EF, Machado CJ, França E. Subnotificação de nascidos vivos: procedimentos de mensuração a partir do Sistema de Informação Hospitalar. Rev Saúde Pública. 2008; 42(1): 55-63. [ Links ]
16. Souza LM. Avaliação do Sistema de Informação sobre Nascidos Vivos - SINASC, Minas Gerais e Mesoregiões, 2000 (Dissertação de mestrado). Belo Horizonte (MG): CEDEPLAR/FACE/UFMG; 2004. 112 p. [ Links ]
17. Hartz ZM, Vieira da Silva LM (Orgs.). Avaliação em Saúde: dos modelos teóricos à prática na avaliação de programas e sistemas de saúde. Rio de Janeiro: Fiocruz; 2005. [ Links ]
18. Contandriopoulos AP, Champagne F, Denis JL, Pineaut RA. Avaliação na área da saúde: conceitos e métodos. In: Hartz ZMA (Org.). Avaliação em saúde: dos modelos conceituais à prática na implantação de programas. Rio de Janeiro: Fiocruz; 1997. [ Links ]
19. Minas Gerais. Plano Diretor de Regionalização de Minas Gerais. Secretaria de Estado de Saúde de Minas Gerais, 2010. [Acesso em: 29 dez 2010]. Disponível em: http://www.saude.mg.gov.br/politicas_de_saude/plano-diretor-de-regionalizacao-pdr [ Links ]
20. Brasil. Ministério da Saúde. Banco de dados dos sistemas de informação sobre mortalidade (SIM) e nascidos vivos (SINASC) 1998 a 2004 (CD-ROM). Brasília: MS/SVS; 2006. [ Links ]
21. Brasil. Ministério da Saúde. Banco de dados dos sistemas de informação sobre mortalidade (SIM) e nascidos vivos (SINASC), 1999 a 2005 (CD-ROM). Brasília: MS/SVS; 2007. [ Links ]
22. Barbuscia DM, Rodrigues-Júnior AL. Completude da informação nas Declarações de Nascido Vivo e nas Declarações de Óbito, neonatal precoce e fetal, da região de Ribeirão Preto, São Paulo, Brasil, 2000-2007. Cad. Saúde Pública. 2011; 27(6):1192-1200. [ Links ]
23. Silva GFS, Aidar T, Mathias TAF. Qualidade do Sistema de Informações de Nascidos Vivos no Estado do Paraná, 2000 a 2005. Rev Esc Enferm USP. 2011; 45(1):79-86. [ Links ]
24. Mascarenhas MDM, Gomes KRO. Confiabilidade dos dados do Sistema de Informações sobre Nascidos Vivos em Teresina, Estado do Piauí, Brasil - 2002. Cienc Saúde Coletiva. 2011; 16(1):1233-1239. [ Links ]
25. Almeida MF, Alencar GP, França Junior I, Novaes HMD, Siqueira AAF, Scchoeps D, et al. Validade das informações das declarações de nascidos vivos com base em estudo de caso-controle. Cad Saúde Pública. 2006; 22(3):1-9. [ Links ]
Manuscript submitted
mar 06 2011, accepted for publication Aug 30 2011. Correspondência para:
Correspondência para:
eguimaraes@cpqrr.fiocruz.br


{kind=link}
{kind=link}
{kind=link}