










Serviços Personalizados
artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282
Rev. bras. crescimento desenvolv. hum. vol.21 no.3 São Paulo 2011
ORIGINAL RESEARCH
Emotional factors, life quality and adhesion of treatment in adult with type 2 diabetes
Luciane RamosI; Eleonora Arnaud Pereira FerreiraII
IDoutoranda
do Programa de Pós-graduação em Teoria e Pesquisa do Comportamento
do Núcleo de Teoria e Pesquisado Comportamento da Universidade Federal
do Pará (UFPA). Endereço: Rua Augusto Corrêa, 01, Campus
Universi-tário do Guamá, Belém, Pará. CEP 66.075-110,
fone: (91) 81694728, E-mail: lucianeramos@ufpa.br
IIProfessora Doutora do Programa de Pós-graduação
em Teoria e Pesquisa do Comportamento do Núcleo de Teoria ePesquisa do
Comportamento da Universidade Federal do Pará (UFPA)
ABSTRACT
This study has the objective to verify the relation among emotional factors (stress, anxiety and depression), quality of life and adherence to treatment in adults with type 2 diabetes. Thirty patients (18 women and 12 men) from ages 33 to 59, registered at the Hiperdia program of a Basic Health Care Unit, participated of this study.The instruments used were the Beck Anxiety Inventory, the Beck Depression Inventory, the Lipp Stress Symptoms Inventory (ISSL) and the general questionnaire of health and quality of life (SF-36).Treatment adherence was measured by the last test results of glycated hemoglobin.The results showed no correlation between emotional factors and adherence to treatment. However, there was a significant correlation between diabetes time of diagnosis and adherence, suggesting that the longer the participant had the disease, the greater the difficulty in maintaining stable blood glucose levels and adhering to the prescribed guidelines.Also, a positive correlation between low adherence and family structure was observed.These results suggest that other factors, besides the emotional ones, should be considered in the adherence to treatment analysis.
Key words: diabetes; stress; anxiety; depression; quality of life; adherence to treatment.
INTRODUCTION
Diabetes is a disease that affects 220 million people worldwide.According to the World Health Organization, diabetes is a public health problem, causing social and economic impact, both in terms of productivity (related to absenteeism), and high costs (related to leading causes of hospitalization).These consequences are important in a way that diabetes prevention and treatment may be taken care of more cautiously by public health services.
Epidemiological studies show that the prevalence and incidence of diabetes in Brazil have increased over the years.It's estimated there are 11 million people suffering from diabetes, mostly patients with type 2 diabetes.These have become concerning facts since there is no cure for this illness and for the complications that result from it1,2. If not treated properly, diabetes may lead the individual to have, in the long term, chronic and irreversible complications such as dysfunction and failure of organs, such as kidneys, eyes, nerves, heart and blood vessels, causing diseases such as neuropathy, nephropathy, retinopathy, myocardial infarction, strokes and infections.
Diabetes treatment is a very complex one as it involves changes in the patients' lifestyles.Caring for self-monitoring of blood glucose, regular physical activity, medication administration (oral hypoglycemic agents and/or insulin) and the maintenance of a healthy diet are important to keep blood glucose levels stable and, consequently, prevent chronic complications.
The American Diabetes Association3 recommends that social and psychological variables should be included as an ongoing part in the management of the disease.It also highlights the need for emotional factors like depression, anxiety and stress to be evaluated when there is a low glycemic control, suggesting that these factors are extremely important for following treatment recommendations since they're part of the standards for diabetes care.
Emotional factors in the management of diabetes
Studies show that patients with chronic disease diagnoses are more likely to develop pathological forms of stress, anxiety and depression4-7.These studies suggest that these individuals, when exposed to aversive situations, present difficulties in the management of the disease, thus affecting their adherence to treatment and consequently their quality of life.In the case of diabetes, specifically, studies suggest there is a positive correlation among these factors and the course of the disease8-11.
Aiming to identify the interference of emotional factors on self-care in patients with type 1 and type 2 diabetes, Santos-Filhoet al.9 conducted three studies.Study 1, with eight type 1 diabetes school-age children; Study 2, with eleven type 2 diabetes patients, aged 50 to 76 years; and Study 3, with seven participants from 44 to 66 years old.In the three studies, a semi-structured interview guide about the emotional reactions of participants was used.The emotional reactions identified were: fear, sadness, depression, rage/anger and anxiety/stress.Such reactions, according to the authors, are present both at the moment of diagnosis and in the manner that patients cope with the illness during treatment. According to the authors, diabetes turned out to be a disease that, regardless of age and etiology, causes a negative impact on the individual's life.From this point of view, they suggest that health professionals ought to be sensitive to these aspects of the patient's life, since the emotional manifestations may be related to an appropriate glycemic control and the patients' quality of life.
The study performed by Maia and Araújo8 suggests that the psychological profile and the type 1 diabetes degree of acceptance by the patient can directly influence the glycemic control.In this study, the influence of the patients' psychological profiles was verified, through a questionnaire that assessed the patients' feelings regarding the disease, compared with their blood glucose levels.The results showed that 60.4% of patients were coping well or very well with the disease and 13.90% reported they were ashamed of saying publicly they had been diagnosed with diabetes, while 60.4% confirmed they were afraid of having a hypo or hyperglycemic crisis in a public place.These are prominent findings because they point towards a broader understanding of this sickness, suggesting that psychological aspects are important in the search for strategies to cope with the disease, preventing complications caused by diabetes.
A study conducted by Silva, Pais-Ribeiro and Cardoso7 compared levels of anxiety, depression and stress among diabetic patients with and without chronic complications. The participants in this study were 316 patients aged 16 to 84 years; 55.4% were female and 59.8% had complications caused by the disease.The participants answered a life events scale, adapted into Portuguese by Silva, Pais-Ribeiro, Cardoso and Ramos12 and an anxiety and depression inventory (Hospital Anxiety and Depression Scale [HADS]).Data were statistically analyzed and they suggest that patients with chronic complications presented higher depression levels compared to others, but did not differ in relation to anxiety levels. There was no difference in the negative stress (distress) among participants, but participants with chronic complications showed less positive stress (eustress).There was no difference regarding negative stress (distress) among participants. However, participants with chronic complications showed less positive stress (eustress).
Riveros, Cortazar-Palapa, Alcazar and Sánchez-Sosa13 performed a study whose objective was to evaluate the effects of a cognitive-behavioral intervention on patients with diabetes and/or hypertension. 51 patients from a family medicine unit in Mexico City participated of the study, with a mean age of 54.27 years, 17 with hypertension, 27 with diabetes and 7 with diabetes and hypertension.The Quality of Life and Health Inventory proposed by Riveros, Sánchez-Sosa and Groves14, the Beck Anxiety Inventory and the Beck Depression Inventory (adapted) and the Health and Daily Living Form Manual developed by Moos, Cronkite, Billings and Finney15 were used, in addition to the adherence and wellbeing daily self-monitoring system, produced by Cortazar-Palapa, Riveros and Sánchez-Sosa16, which assesses the patients' adherence to medication, diet, physical activity and health-risk behaviors.The aim was to investigate quality of life, anxiety, depression, coping styles, adherence and wellbeing in this group of patients. The results suggest that the performed interventions provided a significant improvement of the investigated variables, as well as a decrease in glucose levels and blood pressure of participants.Based on these results, the authors concluded that in the health system context, it's not enough that the patient receives only instructions and information about the disease and treatment, without being provided with careful attention and monitoring by health professionals.
Proposing to examine the effectiveness of a stress management training in 26 patients with type 2 diabetes, Surwitet al.10 used the STAI*, the Perceived Stress Scale and the General Health Questionnaire SF-36.Concomitant with the application of these instruments, a diabetes education program and a stress management program were implemented. The results showed that the stress management training was associated to a small but significant reduction in glycated hemoglobin (A1C) when compared with the group submitted only to the diabetes education program.These findings suggest the effectiveness of stress management training on glycemic control in patients with type 2 diabetes.
Due to the complexity involved in diabetes, the literature indicates that aspects related to the patient, such as emotional factors and life history, are relevant in serving this population, since these are important factors for the treatment and prevention of chronic complications brought about by the disease when the patient does not engage in the guidelines provided by health professionals.The objective of this study was to investigate the relationship of emotional factors with quality of life and adherence to treatment in adults with type 2 diabetes.
METHODS
Participants
30 patients attended at the HiperDia program of a Basic Health Care Unit in Belém (PA/Brazil) participated of this study, in which 18 were female and 12 male, diagnosed with type 2 diabetes.The inclusion of participants obeyed the following criteria: aging from 25 to 59 years; being registered at the HiperDia program for at least six months; and having agreed to sign the Informed Consent Form [ICF] (project approved by the Research Ethics Committee - CEP/NMT, Protocol n.047/2009).The patients excluded from the study were the ones that hadn't been registered in the Program; those that had recently enrolled; patients who had neurological sequelae (such as retinopathy, neuropathy, or amputation), the ones who were in use of prescribed medication for the control of psychiatric disorders, and those that did not agree to sign the ICF.
Instruments
The participants responded to the following instruments:
a) Interview Guide: a script developed for this study, containing open and closed questions in order to collect detailed information about the sociodemographic and clinical characteristics of participants such as age, sex, education level, profession/occupation, the patient's medical history concerning the disease, as well as the history of adherence to diabetes treatment.
b) Brazilian Criterion of Economic Classification (CCEB) [Brazilian Association of Research Companies - AssociaçãoBrasileira de Empresas de Pesquisa - ABEP]18: an interview guide that defines the economic status of the brazilian population by estimating the purchasing power of the informants.In this study, it aimed to determine the socioeconomic status of participants.
c) Stress Symptoms Inventory for Adults (ISSL)19: a validated inventory, approved by the Federal Council of Psychology, used in researches and clinical activities for the diagnosis of stress in adults.It consists of three tables which refer to the symptoms (physical and psychological) and to the four phases of stress (alarm, resistance, near-exhaustion and exhaustion), subdivided temporally in symptoms experienced by the individual in the last 24 hours, in the last week and in the last month.
d) Beck scales:a set of four inventories used as a self-assessment measure of depression, anxiety, hopelessness and suicide attempt, validated for the Brazilian population by Cunha.20 In this study, the Anxiety Inventory (BAI) and the Depression Inventory (BDI) were used.The Beck Anxiety Inventory (BAI) was proposed to measure the common symptoms of anxiety. It consists of 21 listed symptoms, each one containing four alternatives, in ascending order of anxiety level.The scale classifies anxiety as: minimal (0-9 points); mild (10-16 points); moderate (17-29 points); and severe (30-63 points).The Beck Depression Inventory (BDI) consists of 21 categories of symptoms and activities, each one containing four alternatives, in ascending order of depression level.The patient should choose the answer that best fits his/her last week. The sum of scores identifies the level of depression.The following result is proposed for the degree of depression: minimal (0-11 points); mild (12-19 points); moderate (20-35 points); and severe (36-63 points).
e) SF-36 Health Survey:Instrument translated and validated into Portuguese in accordance with the International Quality of Life Assessment Project (IQOLA).It is a questionnaire with 36 items that covers eight aspects (functional capacity, physical aspects, pain, general health, vitality, social and emotional aspects as well as mental health).It provides a final score, from 0 to 100, where 0 corresponds to the worst overall health status and 100 to the best one.
f) Patient's multidisciplinary medical record: a document on which all kinds of treatment provided in the outpatient visits are recorded. It may also contain prescriptions for treatment and laboratory test results such as glycated hemoglobin.
Setting
Data were collected in a Basic Health Care Unit in the city of Belém/Pará/Brazil. The unit works as a clinic for patient care in primary health care programs, including the HiperDia, for patients with hypertension and diabetes mellitus.In this unit, the HiperDia program is developed by a team of professionals consisting of doctors, nutritionists, nurses and nursing technicians. Data collection was performed in an outpatient room, offered as courtesy for interviewing the participants.
Procedure
The patients in the waiting room at the Health Care Unit, who were waiting for medical attention, were invited to participate in the study.Those who fit the inclusion criteria and agreed to sign the Informed Consent Form were asked to respond, individually, to the Interview Guide, the Brazilian Criterion of Economic Classification and the instruments: Lipp Stress Symptoms Inventory (ISSL), Beck Anxiety Inventory (BAI), Beck Depression Inventory (BDI) and SF-36 Health Survey, in that order. Then the researcher analyzed each patient's medical records, collecting data regarding glycated hemoglobin levels.
The results were analyzed using descriptive statistics and correlation tests (Chi-Square, Pearson Correlation, ANOVA) using SPSS version 15.0, considering the socio-demographic variables, emotional state indicators obtained through standardized instruments, and adherence to treatment obtained from the last test results of glycated hemoglobin.In this case, the parameters adopted by the Brazilian Diabetes Society (SociedadeBrasileira de Diabetes - SBD) and the American Diabetes Association (ADA) were used. The values they suggest as indicative of diabetes control are equal to or less than 6.5%.
RESULTS
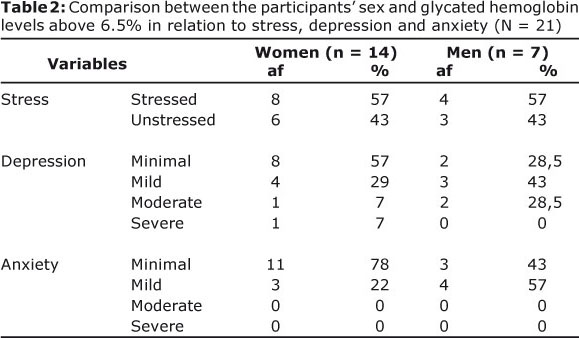
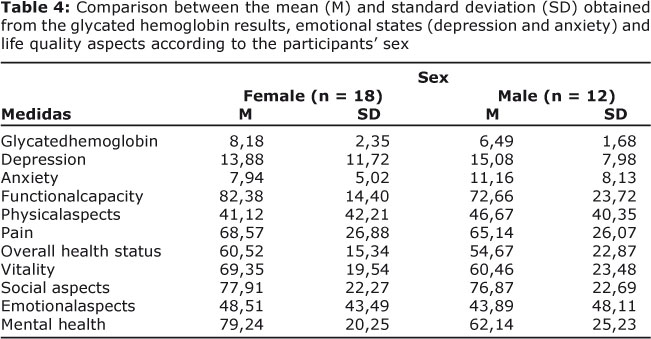
Initially, there were descriptive analyses of the instrument results and the participants' sociodemographic characteristics.Table 2 describes the comparison between the participants' sex and glycated hemoglobin levels above 6.5% in relation to stress, depression and anxiety. Table 3 describes the frequency and percentage of participants with glycated hemoglobin levels above 6.5% who had impaired quality of life according to the SF-36 and comparison between sexes, ending with Table 4, which compares the mean (M) and standard deviation (SD) obtained from the glycated hemoglobin results, emotional states (depression and anxiety) and life quality aspects according to the participants' gender.
DISCUSSION
In the health care field, some studies have been making important progress in identifying needs associated with chronic diseases such as psychophysiological problems, persistent medical symptoms, with valid assessments being developed to measure clinical outcomes in many different cultures, emphasizing the importance of sex, age, racial and ethnic diversity, from the most distinct interventions.
Chronic diseases are incurable as well as of a non-contagious nature. It's characterized by a long latency period, a prolonged course, the existence of some well-known risk factors which may cause disability. Similarly, all of those features might also characterize type 2 diabetes.As most chronic diseases it is associated with or caused by a combination of social, cultural, environmental and behavioral factors.Thus, the objective was to evaluate if emotional factors like stress, anxiety and depression are related to quality of life and adherence to treatment in adults with type 2 diabetes.
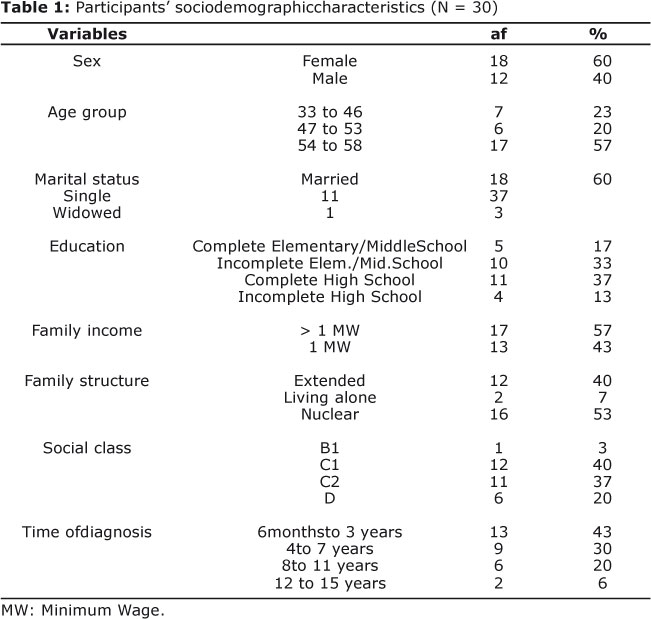
Table 1 presents the participants' sociodemographic characteristics.It is observed that 60% of the sample were female and 40% male.Most of them were aged 54 to 58 years (57%), were married (60%), had an education level corresponding to complete High School (37%), belonged to C1 social class (40%), and lived with more than a minimum wage (57%) in a predominantly nuclear family (53%).
The analysis of glycated hemoglobin levels collected in the medical records indicated that 70% of the participants presented values above 6.5%, pointing out a difficulty in controlling diabetes.Of those, 67% were female (n = 14) and 33% male (n = 7). These participants' glycated hemoglobin levels ranged from 6.8 to 14% and the time of diabetes diagnosis varied from 6 months to 15 years.
After, through Chi-Square(c2) statistical test, a correlation analysis was made between adherence to treatment and the sociodemographic variables sex, age group, marital status, education and family income.In this analysis, only the 21 participants (14 women and 7 men) who had glycated hemoglobin results suggesting difficulty in controlling diabetes were considered.The results indicated that there wasn't a statistically significant relationship between these variables.
The relationship between adherence to treatment and the participants' family structure was analyzed as well. The results demonstrated a significant association between these variables, that is, those participants who had low adherence to treatment were those who had a predominantly nuclear family structure (r = 0.047).
The results obtained using the instruments that assessed emotional factors were first analyzed according to the sex of the participants with difficulties of adherence. As for stress, it was observed that there was no significant difference between the sexes, for 57% of women and 57% of men obtained results in the ISSL suggesting the existence of stress, as shown in Table 2.
As for the depression inventory, the female participants showed, predominantly, percentages suggestive of minimal (57%) and mild depression (29%). The male participants had higher scores, with results indicating mild (43%) or moderate depression (43%).
In the anxiety inventory, most women obtained results indicating the existence of minimal anxiety (78%), whereas most men (57%) had mild anxiety.
Based on these data, it's possible to infer that this population presented no significant difference between the sexes regarding stress, anxiety and depression levels.Although the results display different percentages, these data reveal that there was no statistically significant difference between the sexes. In other words, the emotional factors in this population did not differ in relation to gender.
For the correlation analyses between quality of life, assessed by the SF-36 (including functional capacity, physical aspects, pain, overall health status, vitality, social aspects, emotional aspects and mental health), and treatment adherence difficulty (n = 21), Pearson's correlation was used with a significance level of p > 0.05.Table 3 shows the results from this analysis.
From the obtained results, there were some differences between the sexes.The male participants had low scores in functional capacity (48.5%), vitality (47%) and social aspects (36.25%), compared to the scores of female participants. Regarding the emotional aspects, the female participants had very low scores for emotional aspects (5%).It is possible to observe that these data, in general, indicate a level of impairment in these life quality aspects of participants. However, statistical correlation tests pointed out that poor adherence was not significant for the participants' quality of life.
The analysis of the relationship between the time of the participants' diabetes diagnosis and the adherence to treatment was made through Pearson's correlation test with a significance level of p=0.01.A result equal to r = 0,591 was obtained.Based on this result, it's feasible to assume that there is a moderate positive correlation between the time of diagnosis and adherence, i.e., the longer the time of the participant's diabetes diagnosis, the higher the glycated hemoglobin level, indicating a low rate of adherence to treatment.
ANOVA was used in order to compare the participants' means and standard deviations with respect to quality of life, emotional factors and treatment adherence.Table 4 presents these results.
Concerning the participants' quality of life aspects, there was a significant difference with regard to functional capacity, overall health status and mental health, for the male participants proved to be more engaged in these quality of life aspects than the female participants.
In relation to the emotional factors (depression and anxiety), there was no significant difference in the means found among men and women.
At last, when analyzing the presence of emotional factors related to quality of life and glycated hemoglobin levels, the results revealed that, although no statistically significant differences were found in relation to adherence, they are present.
By and large, the results demonstrated that in this population there wasn't a statistically significant association between emotional factors and treatment adherence (evaluated through glycated hemoglobin levels), which indicates that emotional factors were not determining variables for the lack of adherence.Yet, data illustrate that, even if there is no causal relationship between these variables, there are changes concerning emotional factors in individuals living with diabetes4-7.
Other correlated variables, such as the longest time of diagnosis and the highest glycated hemoglobin levels, were significant for the indication of the participants' poor adherence.Nevertheless, poor adherence was not statistically significant for the participants' quality of life.
In general, this study showed no statistically significant differences among participants in relation to sociodemographic characteristics such as gender, marital status, with regard to adherence to treatment, nor a statistically significant correlation between the later and age or education of the participants.Despite such findings, it's not recommendable to discard the existence of association between these variables, since the literature corroborates these are paramount for developing appropriate lifestyles so that the patient can live with the disease in a healthier way.21
Another very relevant finding in this study was the level of adherence correlated with the participants' nuclear family structure. These data indicate that participants with higher glycated hemoglobin levels had a predominantly nuclear structure, which corroborates some studies in which the lack of family support is identified as a hampering factor for adherence to the treatment of a chronic disease, diabetes in this context.22
These data suggest that other variables may be interfering in these participants' adherence.However, in this study, it was not possible to identify which factors contributed to poor adherence, suggesting the need for longitudinal studies accompanying the individual in the process of adherence to treatment.
It is necessary to consider the importance of emotional factors in individuals living with chronic diseases like diabetes, offering emotional support and training in strategies for coping with the disease.
REFERENCES
1. World Health Organization. Diabetes, Fact sheet, [periódico online]. 2011 Jan [acesso em 3 mar 2011]. Disponível em http://www.who.int/mediacentre/factsheets/fs312/en/. [ Links ]
2. Sociedade Brasileira de Diabetes - SBD. Cuidados de Enfermagem em diabetes mellitus. Em Manual de Enfermagem da Sociedade Brasileira de Diabetes. Citado em 25/03/2011, Disponível em: http://www.diabetes.org.br/attachments/1118_1324_manual_enfermagem.pdf. [ Links ]
3. American Diabetes Association. Standards of medical care in diabetes. Diabetes Care, 34 (1, Supplement). 2011 [acesso em 25 mar 2011 Disponível em: http://care.diabetesjournals.org/content/34/Supplement_1 /S11.extract. [ Links ]
4. Ataíde M.B. C., & Damasceno M. M. C. Fatores que interferem na adesão ao autocuidado em diabetes. 2006Revista de Enfermagem UERJ, RJ, 14 (4): 518-23. Retirado em 09/07/2008, de Disponível em: http://www.portalbvsenf.eerp.usp.br/scielo.php?script=sci_pdf&pid=S0104-35522006000400005&lng=pt&nrm=iso&tlng=. [ Links ]
5. Carvalho, N. S., Ribeiro, P. R. Ribeiro, M. Nunes, M. P. T. Cukier, A. & Stelmach R. Asma e doença pulmonar obstrutiva crônica: Uma comparação entre variáveis de ansiedade e depressão, Jornal Brasileiro de Pneumologia, 2007; 33(1), 1-6. [ Links ]
6. Chaves, E. C. & Cade, N. V. Efeitos da ansiedade sobre a pressão arterial em mulheres com hipertensão Revista Latino-americana de Enfermagem março-abril; 2004; 12(2), 162-167. [ Links ]
7. Silva, I., Pais-Ribeiro J., & Cardoso H.. Dificuldades em perceber o lado positivo da vida? Stress em doentes diabéticos com e sem complicações crónicas da doença. Avaliação Psicológica, 3(22), 597-605. 2004.Retirado em 27/11/2007, de Disponível em: www.scielo.oces.mctes.pt/pdf/aps/v22n3/v22n3a14.pdf. [ Links ]
8. Maia, F. F. R. & Araújo L. R.. Aspectos psicológicos e controle glicêmico de um grupo de pacientes com diabetes mellitus tipo 1 em Minas Gerais. Arquivos Brasileiros Endocrinologia e Metabologia, 2004; Vol. 48, n 2, p 261-266. [ Links ]
9. Santos-Filho, C. V., Rodrigues, W. H. C. & Santos R. B. Papéis de auto-cuidado - Subsídios para enfermagem diante das reações emocionais dos portadores de diabetes mellitus. Escola Anna Nery - Revista de Enfermagem, 2008, 12(1), 125-129. [ Links ]
10. Surwit RS, van Tilburg MA, Zucker N, McCaskill CC, Parekh P, Feinglos MN, Edwards CL, Williams P, Lane JD. Stress management improves long-term glycemic control in type 2 diabetes. Diabetes Care, 2002, 25(1):30-4. [ Links ]
11. Thomas, J., Jones, G., Scarinci, I. & Brantley, P.. A descriptive and comparative study of the prevalence of depressive and anxiety disorders in low-income adults with type 2 diabetes and other chronic illnesses. Diabetes Care, 2003, 26, Number 8. [ Links ]
12. Silva, I., Pais-Ribeiro, J., Cardoso, H., & Ramos, H. Contributo para a adaptação da Life Events Survey (LES) à população diabética portuguesa. Revista Portuguesa de Saúde Pública, 2003, 2, 49-60. [ Links ]
13. Riveros, A., Cortazar-Palapa, J., Alcazar, F. L. & Sánchez-Sosa, J. J. Efectos de una intervención cognitivo-conductual en la calidad de vida, ansiedad, depression y condición médica de pacientes diabeticos e hipertensos esenciales. International journal of clinical and health psychology, septiembre, año/vol. 5 numero 003, Asociación Española de Psicología Conductual (AEPC), granada, Espanha, 2004, p, 445 - 462. [ Links ]
14. Riveros, A., Sánchez-Sosa, J. J. e Groves, M. Inventario de calidad de vida y salud, InCaVisa: México Universidad Nacional Autonóma de México; 2004. [ Links ]
15. Moos, R., Cronkite, R., Billings, A. e Finney, J. Health and daily living form manual. Social Ecologic Laboratory, Department of Psychiatry and Behavioral Science. Palo Alto, CA: Veterans Administration and Standford University medical Center; 1986. [ Links ]
16. Cortazar-Palapa, J., Riveros, A., Sánchez-Sosa, J. J. Herramientas para la toma de decisiones en terapia cognitivo-conductual en escenarios médicos: el uso del sistema de autorresgistro. Ponencia presentada en el XII Congreso Mexicano de Psicología, Guanajuato, México; 2004. [ Links ]
17. Spielberger, C.D.; Biaggio, A.; Natalicio, L.F. - Manual do Idate- Rio de Janeiro, R.J., CEPA, 1979 [ Links ]
18. Associação Brasileira de Empresas de Pesquisa Critério de Classificação Econômica Brasil. Retirado em: 03/01/2010. Disponível em http://www.abep.org/novo/Content.aspx?ContentID=302. [ Links ]
19. Lipp, M. E. N. Inventário de sintomas de stress para adultos de Lipp. São Paulo: Casa do Psicólogo; 2000. [ Links ]
20. Cunha, J. A.. Escalas Beck. São Paulo: Casa do Psicólogo; 2001. [ Links ]
21. Silva, I. Pais-Ribeiro, J. Cardoso, H. Adesão ao tratamento da diabetes Mellitus: A importância das características demográficas e clínicas. Revista Referência IIª Série, 2006; nº 2. [ Links ]
22. Lopes, M. C. L., Marcon, S. S. A hipertensão arterial e a família: a necessidade do cuidado familiar Revista Esc de Enfermagem USP, 2009; 43(2): 343-50. [ Links ]
Manuscript submitted
mar 16 2011, accepted for publication Aug 20 2011. *
STAI: The State-Trait Anxiety Inventory was adapted into Portuguese by Spielberger,
Biaggio and Natalício (1979) from the original 1970 version developed
by Spielberger.It has a self-report scale that evaluates the individual's state
of anxiety as well as his/her personality traits. In Brazil, the Federal Council
of Psychology does not authorize the use of this instrument.


{kind=link}
{kind=link}
{kind=link}