










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores
Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282
Rev. bras. crescimento desenvolv. hum. vol.22 no.1 São Paulo 2012
ORIGINAL RESEARCH
Overweight in preschool children: analysis of a possible intervention
Viviane Gabriela NascimentoI; Emanuel Péricles SalvadorII; Janaína Paula Costa da SilvaIII; Ciro João BertoliIV; Marcia de Toledo BlakeV; Claudio LeoneVI
INutricionista, MSc, PhD, Pesquisadora de Pós-doutorado, Departamento de Saúde Materno-Infantil da Faculdade de Saúde Pública da Universidade de São Paulo
IIEducador Físico, MSc, Doutorando do Departamento de Nutrição da Faculdade de Saúde Pública da Universidade de São Paulo
IIINutricionista, MSc, Doutoranda do Departamento de Saúde Materno-Infantil da Faculdade de Saúde Pública da Universidade de São Paulo
IVMD, PhD, Professor Doutor do Departamento de Medicina da Universidade de Taubaté - cirojb@yahoo.com.br
VPsicóloga, Mestranda em Saúde Coletiva na Faculdade de Medicina do ABC, Professora da Universidade Federal do Pará - marciablake@ufpa.br
VIMD, PhD, Professor Titular do Departamento de Saúde Materno-Infantil da Faculdade de Saúde Pública da Universidade de São Paulo
ABSTRACT
INTRODUCTION: Obesity is increasing progressively in childhood. In response to this trend, several institutions have carried out programs to prevent childhood obesity.
OBJECTIVE: To develop an intervention project aimed at the overweight prevention in 2-3 year-old children at public daycare centers and analyze the feasibility of its implementation.
METHODS: nine daycare centers were randomly selected probabilistically: four composing the sample object of intervention and five in the group without intervention. There have been comments systematized for the recognition of the routine of feeding and physical activity of daycare centers, from which was outlined and implemented an intervention. It was predefined that the intervention should be simple, of low cost, hardly raising the burden of local labor and result in a participatory process.
RESULTS: Food was scheduled by the school lunch company outsourced by the city, which offered oversized portions. Physical activities were restricted and without regular schedule. The nutritional intervention adapted the quantity of food served at lunch, also avoiding the repetition of the meal. For physical activities, it was established that they would be daily, during 30 minutes and of high energy expenditure. All changes were designed and implemented with effective participation of staff in the daycare, in a maximum of 12 weeks.
CONCLUSION: it is possible to develop and deploy a simple intervention, tailored to local realities of daycare centers, aimed at improving the nutritional status of children.
Key words: preschool children; overweight; nutritional intervention; daycare; physical activity.
INTRODUCTION
Obesity is becoming increasingly common in children, which can result in health problems in both childhood and adulthood1. This has been motivating several studies to quantify the extent of the problem among children 2-4, demonstrating that weight excess is affecting ever-younger children, becoming an even more serious public health problem5.
As a consequence of this alarming trend, several institutions in the world have sought to carry out obesity prevention programs6. In this scenario it is essential to develop public policies for the overweight prevention in childhood, particularly in schools, because they are the ideal place, as currently children spend much of their day to day at preschool or school7.
The curricula of health education at the time have included strategies proposed as interventions to reduce chronic health problems related to sedentary lifestyle and eating habits8, within the public health. However, few studies of interventions to reduce overweight and obesity have been conducted specifically in children under 7 years of age9-11.
Early detection of changes in body composition during childhood is important because it contributes to the development of interventions that seek to prevent overweight and its possible consequences12. Currently, the preschool age has been identified as a critical period and favorable for targeted interventions for the obesity prevention13.
The objective of this study is to describe an intervention project aimed at 2-3 year-old children overweight prevention at public daycare centers, analyzing the feasibility of its implementation.
METHODS
This is the description and analysis of an intervention project that was conducted in a sample of daycare centers in the City of Taubaté, State of São Paulo, Brazil.
As a first step, meetings were held in the Department of Education and Culture of the city in 2009 to expose a synthesis of the project in order to submit it to the principals and obtain consent for its implementation. After that, based on the list of 59 public daycare centers existing, a sample was drawn up in order to obtain a number of children that corresponded to about 10% of all students under 4 years of age enrolled in daycare centers. This proportion was estimated as necessary for, after one year, be able to assess the impact of intervention on the nutritional status of the children.
Nine daycare centers were randomly selected resulting in a sample of 845 children of two and three years of age, enrolled in classes of the first level, that is, the first year of stay in daycare. Of the nine centers sampled, the first four selected comprised the sample batch of intervention (intervention group) and the five remaining the group without intervention (comparison group), to obtain a similar number of children in both groups.
After obtaining the Board of Education authorization for the project, meetings were held with the coordinator responsible for the daycare centers and the nine principals of the selected centers aiming to present and provide explanations on the proposed intervention, its objectives, and the guidelines that would delimit its implementation.
At these meetings we tried to sensitize the principals showing the importance of contributing to the control of young children weight excess. At this stage the principals still did not know what would be the daycare centers where it would be performed the intervention.
Once this first stage has been overcome, it was initiated a period of systematic observation of the daycare centers routine in both groups, especially what was related to the preschoolers´ routine of feeding and physical activity.
The meetings and comments were made by the researcher (nutritionist) and by the physical educator, as was previously defined that the intervention would have to encompass changes in both diet and physical activity of children during the period that they remained in the daycare center.
After the prepared remarks, a report of what had occurred was written, following all the activities of preschoolers spent in whole or in part, until their leaving.
Who was responsible for dropping off and picking up the children at the daycare centers, how many teachers were there in each class, how many classes of the first level were there and who was responsible for the children's meals and the physical space of the centers were systematically checked.
In order to know the children eating patterns, the meals served in daycare centers were reported, followed by timetables, which was the daily menu and how the preparation and provision of meals to children was.
As for physical activity it was observed who was responsible for recreational activities, which activities were planned and how they were performed, their duration and how many times per week they were actually performed. It was also checked whether there was place and/or enough equipment for physical activity.
All observations were conducted in the nine daycare centers participating in the study, with unmarked provided visits on different days of the week by the researchers. The observation period was approximately fifteen days.
After concluding the remarks, a further meeting was held with the principals of the centers to communicate which had been selected to take part in the intervention group and what would be the comparison group. As scheduled, from then the principals of the group comparison not more participated in the meetings for the discussion and implementation of the project.
The detailing of the project was performed, hereinafter, aiming to combine the observed in day care centers with the parameters set to guide the intervention.
These parameters, previously defined by the researchers, established that the intervention should be as simple as possible, be low cost (no cost if possible), and that would interfere little with the preschools day to day, so that it would not add more work to the activities which were held by the employees. Drafted the proposal, further meetings were scheduled for presentation and discussion of it with the intervention group principals.
For implementation of the dietary intervention it was carried out a training of the school principals and the kitchen staff. Specific training for the intervention of physical activity was carried out with the professors responsible for recreation.
After starting the process of implantation, systematic visits were performed at least once a week, varying the day in each daycare center and without being previously scheduled. The purpose was to oversee, to give support and to check the progress of implementation of the proposed activities. After two months of weekly supervision, it became biweekly, but remained a weekly telephone contact with the daycare principals of the intervention group. In addition, monitoring and extraordinary meetings with principals of daycare centers were made when necessary.
At the beginning there was local supervision once a month in the centers of the comparison group to make sure that these preschools were not modifying the routines established by the Department of Education.
One year after the intervention starting, as a means of evaluating the implantation, individual interviews with the principals were also conducted. This activity, using a semi-structured script of questions, previously prepared, in order to avoid interferences or suggestions that could occur if performed on a group, aimed at knowing the opinion of each principal.
RESULTS AND DISCUSSION
From the list of students enrolled in daycare centers it was found that there were a total of approximately 4000 children aged 2 and 3 years old in the kindergarten class I and that their number was very variable in each daycare center.
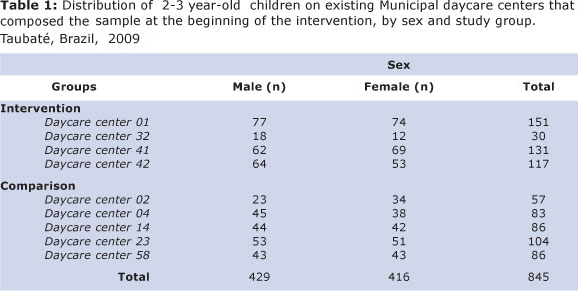
Therefore, it was decided to draw sequen-tially the daycare centers to form two groups, the first for action and then the comparison one, until achieving a total of around 400 preschool children in each group, about 10% of the total (Table 1). This number was estimated as necessary (including possible losses) to perform a comparison of the nutritional status of children at the beginning and at the end of the intervention. To complete the sample batch of each group it was necessary to randomly select four daycare centers for intervention and 5 for comparison.
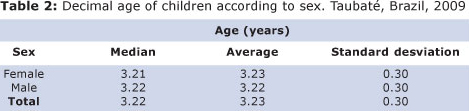
In the final sample, the average age of children was 3.23 years, almost identical for both sexes (Table 2).
The initial stage of systematic observation of the selected daycare centers showed that:
1. The food was maintained in accordance with the schedule of the menu prepared by the school lunch outsourced company, contracted by the City.
2. The standard menu of daycare centers included breakfast, lunch, afternoon snack and for the full time children, a soup for dinner.
3. It was not allowed that the child would take them to the daycare food from home, with the exception of children with allergy or any food intolerance.
4. The daycare workers, who did not belong to the outsourced company staff, could not enter the kitchen area. Only the principals were authorized to do so.
5. With outsourcing conducted by the City, alleging food safety reasons, the contractual terms limited a lot the possibilities for intervention by the study team.
6. The contacts with the company responsible for the childcare feeding supply, in attempting to contribute to any eventual change in the diet, were unsuccessful, so that the intervention had to be shaped so as to be adapted to the already existing food standards in the centers.
7. The portions offered to children at lunchtime, the main meal, were oversized, well above the appropriate amount of food for a 2 or 3 year-old child. There were no previous criteria that defined the quantity to be offered, leaving it to the sole discretion of the kitchen staff.
8. There were also no rules about what to do when a child wanted to repeat the meal, which facilitated the access to an even greater amount of food.
As a result of outsourcing, the intervention was based on existing food in daycare centers, making it impossible to have modifications for breakfast, the afternoon snack and dinner.
Changing these meals would change the amount and type of used foods, which would cause a loss of food purchased by the company, and an increase in the cost of meals, as a consequence of the inclusion of new foods not originally foreseen in the contract.
Based on the observed and the premises of the project, it was chosen to perform the intervention only at lunch, resizing the portions so as to adapt them to the real needs of children as well as introducing minor possible modifications on the menu, using available food.
According to Wabitsch14, portion size is one of the factors determining the amount of calories in a meal, which may contribute to progressively install the overweight. The author recommends that for the prevention of its development, to pay close attention to the size of the portions served, which should be appropriate for the age and size of children.
From this statement, to standardize the quantity supplied has become a way to get a simple nutritional intervention and that of course would not change the routine of the kitchen or even the daycare center as a whole.
The calculation of the daily nutritional needs of the children enrolled in daycare centers was based on the Resolution / CD / FNDE Nr. 38, July 16, 200915. For the calculations of the adequacy of the food amounts were used the Recommended Dietary Allowances16 for 1 to 3 year-old children. Resizing the portions and the type of food offered (if possible), and calculating the distribution of meals during their stay in the daycare, was based on that proposed by Philippi et al17.
To calculate the composition of the preparations were used the Tabela para Avaliação de Consumo Alimentar em Medidas Caseiras18 and the Tabela Brasileira de Composição de Alimentos19, allowing to estimate the approximate number of calories and nutrients distribution.
A very precise way of calculating a menu from the preparations available in the daycare was unworkable in practice. Therefore, the quantities were standardized in order to be nearly adequate. The dish offered to children, in the centers of the intervention group, came to be composed of: 3 tablespoons of rice, one scoop of beans and 2 tablespoons of meat (usually prepared soaked, chopped or ground) and 1 spoon (soup) of side dish.
All the guidelines on the standardization of portion size to be offered to children have been passed to principals through training conducted in their own centers and this information was also passed to the kitchen staff.
Regarding physical activity, observation showed that there was nothing specifically programmed for the periods provided for recreation. The activities were restricted and left to the discretion of the daycare staff and to the children´s wishes, all suggesting that physical activity, in practice, was not seen as a priority in childcare.
The recreational activities were limited to twice a week and held to activities characterized as stimulating the fine motor coordination, such as: jigsaw puzzles, storytelling, listening to music, painting, whose realization, though useful for children fine motor development, did not result in a significant expenditure of energy.
Aiming to encourage more intense physical activity, the intervention was based on the existing equipment in the daycare centers and children's play behavior. These activities were planned as periods of exercise, to be performed daily, lasting thirty minutes. Their achievement was defined as being the responsibility of teachers of kindergartens in the intervention group. The physical activity intervention had as reference the study by Alhassan et al20 for 3 to 5 year-old children.
The teachers were trained by a physical education teacher, to constantly stimulate the children to participate in activities, making them to participate throughout the period in recreation activities that promote higher energy expenditure. At the same time, the proposed activities aimed at stimulating the overall coordination and development of capabilities such as speed, endurance and strength. Thus, there were no added burden to the centers and there was no need for new spaces and/ or equipment.
The weekly on-site supervision, to evaluate the implementation showed that the standardized food prepared was easily incorporated into the routine of the daycare. Both principals and kitchen staff demonstrated to understand the importance of standardization, putting it into practice and, when necessary, appealed to supervisors to clarify any doubts and to make suggestions. The changes planned for the physical activities were also readily accepted and utilized by staff and children.
The largest centers, due to the large number of children who attended them were those that had more difficulties in the implementation of standardized food and physical activity, demanding a closer and more frequent supervision.
After about two months of supervision, in order that the guidelines had already took part of the routine activities of daycare centers, the direct supervision became fortnightly. At the same time were maintained weekly telephone contacts, as the supervisory visits were intended to monitor the progress of the intervention and provide support against any problems that might arise.
In scheduled follow-up meetings were discussed issues related to healthy eating. At these meetings the principals brought their questions which were discussed in group seeking to clarify them. In addition, they discussed a variety of topics, dealing mainly on breastfeeding, infant feeding and obesity.
At these meetings, questions brought by principals were common such as the possibility of passing this information along to parents and /or guardians. As a consequence an educational material focused on healthy eating was prepared, with the contribution of principals who could participate in the process of preparing it, so that the same could be adapted to the reality of childcare. Throughout this development process, the principals showed much interest and were very participative.
According to the research team, the principals' participation was critical for the deployment and implementation of both interventions (food and physical activity) to fruition. Without the support received from the principals, who throughout the years of intervention, motivated employees in order to make everyone feel involved in the project; implementation certainly would not have been successful.
In the principals´ interviews, recorded at the end of the year of intervention, their speeches allowed to see that the intervention food/nutrition and physical activity were carried out very close to what had been planned, subject to the peculiarities of each daycare center.
In the principals´ opinion the greatest difficulty was the proposal of feeding, since they also needed to obtain the support of the kitchen staff, which was from the company hired by the city to provide meals.
Another difficulty reported was related to the interaction with teachers. All cited principals have had some difficulty to explain the action and motivate the teachers, which, however, once achieved, made the intervention to be carried out smoothly and cooperatively.
During the intervention year, it was undoubtedly very clear the change on the principals´ behavior in relation to nutrition and physical activity.
The recognition of its importance was such that in the four intervention centers, the change of the portions, did not repeat the meal and physical activity has become a routine as part of daily life including 4 year-old children who regularly attended at these same daycare centers.
Despite the limitations imposed by conditions of the centers for the development of this project, it could be seen, by the description of the process and its evolution, there is the possibility of to reach a intervention locally appropriate, what is an essential characteristic for it being actually deployed.
This, compared to the characteristics of the existing school feeding program in our country, stresses the importance of these interventions must be simplified as much as possible, taking into account the peculiarities of each place, including the daycare centers. It also shows that it is essential that they provide a truly participatory process, open to the entire community during the planning and deployment, to actually have a chance to be realized.
REFERENCES
1. Meyer F, Mello ED, Luft VC. Obesidade infantil: como podemos ser eficazes? J Pediatr. 2004; 80(3): 173-82. [ Links ]
2. Shoeps DO, de Abreu LC, Valenti VE, Nascimento VG, de Oliveira AG, Gallo PR, Wajnsztejn R, Leone C. Nutritional status of pre-school children from low income families. Nutr J. 2011; 10: 43. [ Links ]
3. Monteiro CA, Conde WL. Tendência secular da desnutrição e da obesidade na infância na cidade de São Paulo (1974-1996). Rev. Saúde Pública. 2000; 34(6 Supl):52-61. [ Links ]
4. Medeiros CCM, Cardoso MAA, Pereira RAR, Alves GTA, França ISX, Coura AS, Carvalho DF. Nutritional status and habits of life in school children. J Hum Growth Dev. 2011; 21(3):789-797. [ Links ]
5. Chinn S, Rona RJ. Prevalence and trends in overweight and obesity in three cross-sectional studies of British children. BMJ. 2001; 322(7277): 24-6. [ Links ]
6. Journet B, Ahluwalia N, Dupuy M, Cristini C, Négre-Pages L, Grandjean H et al. Prevention of overweight in preschool children: results of kindergarten-based interventions. Int J Obes. 2009; 33: 1075-83. [ Links ]
7. Silveira JA, Taddei JA, Guerra PH, Nobre MR. Effectiveness of school-based nutrition education interventions to prevent and reduce excessive weight gain in children and adolescents: a systematic review. J Pediatr. 2011; 87(5): 382-92. [ Links ]
8. Jacob A. School programs. In: Chen C, Dietz WH, editors. Obesity in childhood and adolescence. Philadelphia: Lippincott Williams & Wilkins. 2002; 257-72. [ Links ]
9. Summerbell CD, Waters E, Edmunds LD, Kelly S, Brown T, Campbell KJ. Interventions for preventing obesity in children. Cochrane Database of Syst Rev. 2005. Issue 3 Article n. CD001871. [ Links ]
10. Bluford DA, Sherry B, Scanlon KS. Interventions to prevent or treat obesity in preschool children: a review of evaluated programs. Obesity. 2007;15:1356-72. [ Links ]
11. Reilly JJ, Kelly L, Montgomery C, Williamson A, Fisher A, McColl JH et al. Physical activity to prevent obesity in young children: cluster randomized controlled trial. BMJ. 2006; 68:1006-11. [ Links ]
12. Dietz WH. Childhood weight affects adult morbidity and mortality. J Nutr.1998; 128 (2Suppl): S411-14. [ Links ]
13. Wofford LG. Systematic review of childhood obesity prevention. J Pediatr Nurs. 2008;23: 5-19. [ Links ]
14. Wabitsch M. Overweight and obesity. In: Koletzko B, editor. Pediatric Nutrition in Practice. Basel: Karger; 2008. p. 151-154. [ Links ]
15. Ministério da Educação. Resolução/CD/FNDE nÚ 38 de 16 de julho de 2009. Dispõe sobre o atendimento da alimentação escolar aos alunos da educação básica no Programa Nacional de alimentação Escolar-PNAE. Diário Oficial União. 17 jul 2009; Seção 1:10. [ Links ]
16. National Research Council (US), Subcommittee on the tenth edition of the RDAs. RDA - Recommended dietary allowances. Washington (DC): National Academy Press; 1989.p. 24-38. [ Links ]
17. Phillippi ST, Cruz ATR, Colucci ACA. Pirâmide alimentar para crianças de 2 a 3 anos. Rev. Nutr. 2003; 16(1): 5-19. [ Links ]
18. Pinheiro ABV, Lacerda EMA, Benzecry EH, Gomes MCS, Costa VM. Tabela para Avaliação de Consumo Alimentar em Medidas Caseiras. 5. ed. São Paulo: Atheneu. 2005. 131 p. [ Links ]
19. Universidade Estadual de Campinas, Núcleo de Estudos e Pesquisas em Alimentação. Tabela Brasileira de Composição de Alimentos. 4. ed. Campinas, SP; 2011.161 p. [ Links ]
20. Alhssan S, Sirard JR, Robinson TN. The effects of increasing outdoor play time on physical activity. Int J Pediatr Obes. 2007; 2: 153-158. [ Links ]
 Corresponding author:
Corresponding author:
Claudio Leone.
E-mail: leone.claudio@gmail.com
Manuscript submitted Oct 20 2011
Accepted for publication Feb 08 2012.
