










Serviços Personalizados
artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282
Rev. bras. crescimento desenvolv. hum. vol.22 no.1 São Paulo 2012
ORIGINAL RESEARCH
Transmission of anogenital warts in children and association with sexual abuse
Jefferson DrezettI; Raquel Molina de VasconcellosII; Daniela PedrosoIII; Marcia de Toledo BlakeII,IV; Adriana Gonçalves de OliveiraIV; Luiz Carlos de AbreuIV
ICoordenador do Núcleo de Violência Sexual e Abortamento Previsto em Lei do Centro de Referência da Saúde da Mulher - Hospital Pérola Byington
IINúcleo de Violência Sexual e Abortamento Previsto em Lei do Centro de Referência da Saúde da Mulher - Hospital Pérola Byington
IIIPsicóloga do Núcleo de Violência Sexual e Abortamento Previsto em Lei do Centro de Referência da Saúde da Mulher - Hospital Pérola Byington
IVLaboratório de Escrita Científica, Faculdade de Medicina do ABC
ABSTRACT
INTRODUCTION: the incidence of anogenital condyloma acuminata in children shows remarkable increase in the last two decades, as well as by its association with sexual abuse. However, this relationship presents controversies regarding the etiology of infection, which makes answering challenging, particularly in legal-ethical aspects.
OBJECTIVE: review of the literature about HPV transmission in children and relationship with sexual abuse.
METHODS: synthesis of data from the query to Journal Citation Reports (JCR-ISI), Medical Literature Analysis and Retrieval System Online (Medline), Scientific Electronic Library Online (Scielo) and the Latin American and Caribbean Health Sciences (Lilacs). MeSH descriptors were used Terms with syntax (HPV [All Fields]) AND ("Child Sexual Abuse," [MeSH Terms]). Relevant articles between 1989 and 2009 were selected. Legal-ethical aspects were consulted in the criminal law and Brazilian Child and Adolescent Statute.
RESULTS: different forms of non-sexual transmission of HPV in children are documented, including the vertical transmission, self and hetero inoculation of cutaneous warts, and acquisition by instruments. Studies are conflicting as to the applicability of HPV-DNA to differentiate the sexual transmission and not sexual anogenital warts.
CONCLUSION: evidence indicates that in children under two years non-sexual transmission of HPV should be strongly considered in the absence of genital lesions, another STD, or consistent history of abuse. The likelihood of association between HPV and sexual abuse increases directly with age, especially after five years.
Key words: papillomavirus infections; child sexual abuse; condylomata acuminata; infectious disease vertical transmission; domestic violence.
INTRODUCTION
Sexual abuse of children and adolescents is a worldwide phenomenon, both in developed and in developing countries1. Despite the high underreporting that this type of crime involves, 105 thousand cases of young women victims of sexual violence with non-fatal injury, with 27 000 cases between 10 and 14 years of age were conducted in the U.S. between 2004 and 20062.
It is estimated that 12% to 25% of girls and 8% to 10% of boys suffer some form of sexual abuse up to 18 years of age3. Girls are at greater risk of facing the problem, while boys are more likely to hide its occurrence4. The author of the sexual violence is generally known to the child and close family, sometimes responsible for its protection, often an expressive number of cases are performed by the biological father, grandfather or stepfather5. Less than 10% of children suffer sexual abuse by unknown6.
Children who are sexually abused often have different health problems or changes in behavior, without necessarily reporting the violence. Bleeding or genital pain, vaginal discharge, early pregnancy, recurrent urinary tract infection, abdominal pain without apparent cause, recurrent headache, enuresis, encopresis and chronic constipation are some conditions which, although not specific, are associated with sexual abuse3.However, in mostconfirmed cases of child sexual abuse, clinical examination findings are normal or nonspecific1,7,8.
The diagnosis of a sexually transmitted disease (STD) in a child agrees with the complaint of sexual abuse, and motivates a research when there is no such claim9.10. Some authors consider the diagnosis of a STD in childhood enough to requireevaluation to exclude sexual abuse11. Most studies agree, however, that the isolated presence of a STD is insufficient to ensure its occurrence9.
The risk of STD acquisition depends on the type of molestation and is unlikely to occur when there is no direct physical contact with the author 5.12. Its prevalence among children who suffer sexual violence has significant variability. Neisseria gonorrhoeae infection can range from 2.8% to 28%, the finding of Chlamydia trachomatis from 1.2% to 8%, Trichomonas vaginalis 1% to 6%, Treponema pallidum between 0.1% and 1.5 %, and herpesvirussimple 0.1% 0.5%13.14. About 60% of children with these STI have normal or nonspecific findings in anogenital examination15.
The incidence of anogenital condyloma acuminata in children has increased markedly over the past two decades as the interest in its association with sexual abuse14. Anogenital warts induced by HPV can be transmitted by different forms of sexual abuse, either by oral-genital contact, genital-genital, genital-anal or digital manipulation of the child´s vagina and/or anus16.
This relationship remains controversial and not always easily established, which makes the care of these cases challenging to the health professional, particularly with regard to ethical and legal consequences. Many health professionals do not feel safe to care for children with complaints of sexual abuse, or do not consider themselves capable of performing the clinical examination in these circumstances, particularly because of the limited knowledge about the dynamics of sexual abuse9.
However, most studies argues that HPV infection does not necessarily result from sexual contact and that other forms of contamination should be considered17. Knowledge about the natural history of HPV infection and its mechanisms of transmission, as well as factors related to sexual abuse of children, are necessary for the proper handling of these cases. Thus, the objective is the review of related literature on mechanisms of HPV transmission in children and relation of infection with sexual abuse.
METHODS
Review of literature in the form of articles and data synthesis. Databases were consulted in the Journal Citation Reports (JCR-ISI), Medical Literature Analysis and Retrieval System Online (Medline), Scientific Electronic Library Online (SciELO) andthe Latin American and Caribbean Health Sciences (LILACS). The search strategyused DeCS / MeSH with the syntax (HPV [All Fields]) AND ("Child Abuse, Sexual"[MeSH Terms]). The search result found clinical trials on the mechanisms of HPV transmission in children and association with sexual abuse.Additional ethical and legal aspects were consulted in the Brazilian Penal Code and Child and Adolescent/Statute.
RESULTS
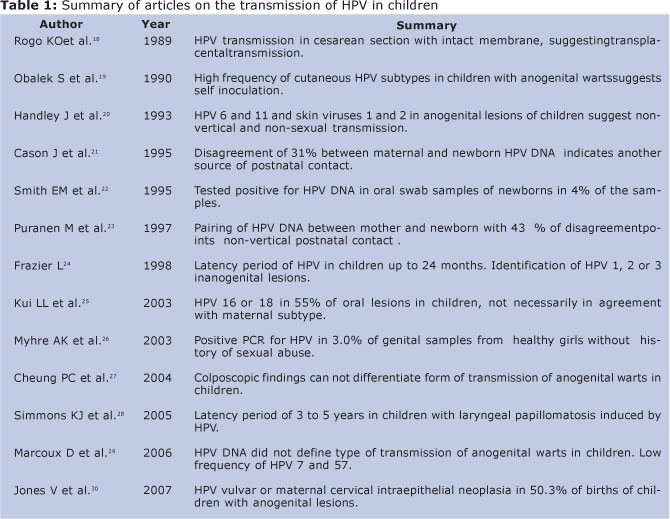
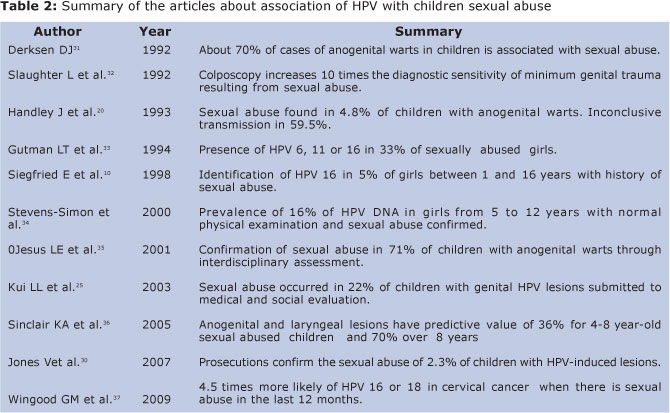
We identified and selected 21 articles indexed to the descriptors in the following databases from 1989 to 2009 that dealt with clinical trials of HPV transmission in children and association with sexual abuse. The summaries have been grouped into two tables, organized by the aspect of research: mechanisms of transmission of HPV (Table I) and the association between HPV and sexual abuse (Table II).
DISCUSSION
HPV can infect both skin and mucous membranes. Most infections regress spontaneously within two years in people with preserved immunity. More than 130 subtypes of HPV are identified so far, although only about a third of them can infect the anogenital mucosa, oral or laryngeal, prevailing subtypes 6, 11 and 1638. HPV infection is one of the most common STD in sexually active adults39. Approximately10% of the adult population has clinic genital lesions induced by the virus10.
There is consistent evidence in literature associating HPV infection in cases involving sex crimes. In adult women who suffer sexual violence, its incidence ranges between 2% and 40%40-42. A longitudinal study, controlled and randomized, with 665 American young women found that those with a history of sexual abuse in the past 12 months were 4.5 times more likely to test positive for HPV 16 or 18 in the cervix, suggesting sexual abuse as a risk factor for infection by HPV37.
Study with 42 prepuberal children with anogenital warts found that 28.6% acquired HPV by vertical transmission, 7.1% resulted from self inoculation of warts located on the hands, and only 4.8% were associated with sexual abuse. The mode of transmission of HPV was considered inconclusive in 59.5% of the studied children, being not possible to relate the infection to sexual abuse20.
The maternal history of vulvar condyloma or cervical squamous intraepithelial lesion at time of delivery was observed in 50.3% of children under nine years who presented different clinical forms of the disease30. A similar finding was for HPV-induced lesions located in the oral cavity of children with frequent maternal history of vulva condyloma during pregnancy25.
Vertical transmission commonly occurs during vaginal delivery in women with HPV, even if there are no clinical signs of the disease. Less commonly, the contamination of the newborn in women undergoing cesarean section, seems independent of the membrane integrity, possibly via ascending transplacental18. The possibility of HPV transmission to the fetus remains poorly understood, although there are inferences that it can occur via hematogenous, via the semen during fertilization, or maternal ascending, as it occurs in other infections during pregnancy16.
The investigation of the presence of HPV DNA in oral swab samples of newborns has shown conflicting results, ranging from 4% to 87%16,22. In addition, the HPV detected in the newborn may be different from that identified in the mother between 31% and 43% of the cases22, 23. This pairing divergence allows us to assign to the postnatal infection other source not associated with sexual abuse16.
The appearance of anogenital warts in the first years after birth can be justified by the long latency period of HPV in cases of vertical transmission. Similar condition can be observed for perinatal infection by Chlamydia trachomatis, which may last two to three years after birth43 . Most of the studies limits the period within 24 months ofbirth, although fewer investigations suggest longer periods of three to five years,based on incubation of laryngeal papillomatosis 24.28. This hypothesis, however, conflicts with the results that the average age in laryngeal HPV infections were lower than that found in anogenital lesions36.
In addition to the incubation period, the child's age at the time of appearance of lesions has important relationship with a diagnosis of sexual abuse. Study of 124 children with anogenital warts, oral or laryngeal, found an average age of 6.5 ± 3.8 years for children victims of sexual abuse, compared with 3.6 ± 2.3 years in cases where the abuse was dismissed36.
The predictive value of HPV-induced lesions in cases of sexual abuse was 36% for children between four and eight years old, and 70% in over eight years. The results suggest that the probability of HPV infection may be due to the sexual abuse increases significantly with the child´s age. At the same time, anogenital warts in the first two years of life are associated with other methods of transmission, other than sexual contact 36.
The relationship between tests to identify the subtype of HPV DNA and sexual abuse of children shows mixed results. Among 40 young women raped with age between one and 16 years, was found 5% of positive PCR tests for HPV 1610. In another study, HPV DNA was detected in the genital tract of 16% of abused girls aged between five and 12 years, with normal physical examination, while no cases were observed in those in which sexual violence was not proved34. In another group of confirmed sexual abused girls, HPV subtypes 6, 11 or 16 were observed in 33% of the cases33. On the other hand, HPV DNA was detected in genital swabs for 3.0% of healthy girls and no history of sexual abuse26.
Some authors argue that the identification of HPV viral subtype can add information about the transmission of anogenital warts in children17. However, the diagnosis of HPV DNA are insufficient to differentiate safely vertically transmitted injuries of those resulting from sexual exposure24. Although DNA- HPV 16 or 18 was found in 55% of warts located in the oral cavity of children, pairing between mother and son do not necessarily show consistent, avoiding to associate these cases with the vertical transmission25. Study with 42 children detecting HPV DNA was associated both with the possibility of vertical transmission, such as through sexual contact20. In another study of 72 children under 12, patients with anogenital warts, was not possible to establish the mode of warts transmission based only on the identified HPV subtype29.
Anogenital warts in children can also be caused by HPV 1, 2 or 3, usually found in skin warts, indicating the possibility of self inoculation or hetero inoculation practiced without intent for parents and/or other caretakers19, 20.24. In addition, anogenital warts in children may be associated with both HPV 6 and 11 as the cutaneous HPV 1 and 2, indicating the likelihood of transmition different from vertical and sexual44. HPV7 or 57 infections in chidren show similar difficulty of interpretation, although affect significantly fewer cases29.
Evaluation of colposcopic anogenital warts does not allow to differentiate those arising from sexual abuse from the ones transmitted by other mechanisms. However, the test proves effective for diagnosing and documenting minor injuries to the anogenitalmucosa resulting from sexual abuse, difficult to identify during the clinical examination27.45. In such cases, the use of colposcopy increases by almost ten times the minimum identification of traumatic injuries, assisting in documentation and in the process of evidence of sexual abuse32.
The relationship between sexual abuse and HPV infection has variable outcome in literature, concluding with an occurrence between 0.1% and 70% of children with genital warts30,31,46. Different methods of investigation of the circumstances of sexual abuse and child assessment influence the results. A retrospective study of children between six months and nine years of age found 2.3% of sexual abuse when subjected to evaluation by the judicial system30. In other experiments, confirmation of sexual abuse has reached 22% when associated medical and social assessment, and 71% when applied interdisciplinary research25.35.
Most authors consider that the diagnosis of sexual abuse depends crucially on the quality of history, the experience of professionals involved in assessment and examination of the child47. However, there are reports that another etiology of genital warts can be confused with those caused by HPV. Considering the possible legal ramifications, it is appropriate to confirm infection with biopsy of typical or suspicious lesions, or to use another diagnosis method valid for HPV36.48.
The American Academy of Pediatrics considers sexual abuse as physical genital contact, oral or anal sex with the child, including actions that do not involve direct relationship with the abuser, such as exhibitionism, voyeurism and pornography12.Most sex crimes against children, however, does not involve acts of vaginal or anal penetration, which makes the probative material evidences uncommon7.
In Brazil, criminal law typifies the crimes of rape and rape of vulnerable in Articles 213 and 217-A, respectively. The law criminalizes any sexual act done without the victim's consent with the use of force or psychological intimidation, or sexual acts committed against children under 14 years old, sick people, mentally ill or any condition that prevents valid consent or offering resistance49.
Articles 13 and 245 of the Estatuto da Criança e do Adolescente(ECA), Law nº 8069, 1990, establish a legal duty of health professionals to communicate the Council of Guardianship suspected or confirmed cases of abuse against children and adolescents under 18 years, including sexual abuse50. This action is fundamental to the protection of children and adolescents in a vulnerable position, interrupting the cycle of sexual violence, often within the family5.
However, the Law does not establish which situations are considered suspected or confirmed of sexual abuse, no criteria or procedures that must be adopted by health professionals for this diagnosis50. Thus, it is for health professionals carefully evaluate whether there are consistent grounds to proceed with the communication to the protection agency.
This evaluation should not be precipitated by external factors and, where possible, should incorporate interdisciplinary actions involving physicians, psychologists and social assistants5. Health professionals should know the possible ways of transmission and incubation periods of HPV-induced anogenital and oral warts, to ensure adequate assistance to the child and consider the need to guide and enlighten the parents or legal guardians47.
Although there is no consensus on how to proceed in those cases, the high prevalence of non-sexual transmission of HPV in children under two years old makes sexual abuse unlikely, though can not be decisively away. It is debatable whether the isolated presence of oral oranogenital warts in children under two years should necessarily be communicated to the government services ofchildren protection with suspicion of sexual abuse. It is exceptwhen associated with abnormalities on physical examination, presence of other STD,change in the child´s behavior, or if sexual abuse is suspected or confirmedby parents or other caretaker or guardian51.
After the child is two or three years old, the communication to the competent authority and the sexual abuse investigation areconsidered necessary measures against anogenital and oral lesions induced by HPV. The conduct is based on the greater likelihood of association with sexual abuse found in different studies, even when there is no complaint by the parents or in the child's narrative51.
The association between oral and anogenital warts induced by HPV and sexual abuse of children reserve contradictory aspects. Different forms of non-sexual transmission of HPV in children are documented. Evidence suggests that in children under two or three years, non-sexual transmission of HPV should be strongly considered, since there is no other concomitant STD, history of sexual abuse, evidence of genital trauma or ruptured hymen.
In children above that age the likelihood of sexual abuse becomes greater. However, in any age of child sexual abuse can be definitely ruled out. Studies are conflicting regarding the applicability of methods for identification of HPV subtype to differentiate sexual and nonsexual transmission forms of anogenital and oral warts in children. The genitoscopia and anoscopy also do not differentiate the type of transmission by theappearance of the lesions. However, these methods have shown better sensitivityand higher specificity for identifying genital and perianal minor injuries resulting from sexual abuse.
REFERENCES
1. Gilbert R, Widom CS, Brown K, Fergusson D, Webb E, Janson S. Burden and consequences of child maltreatment in high-income countries. Lancet, 2009;373(9657):68-81. [ Links ]
2. Gavin L, MacKay AP, Brown K, Har-rier S, Ventura SJ, Kann L, et al. Sexual and reproductive health of persons aged 10-24 years - United States, 2002-2007. MMWR SurveillSumm, 2009;58(6):1-58. [ Links ]
3. Sapp MV, VandevenAM. Update on childhood sexual abuse. Curr. Opin Pediatr, 2005; 17(2): 258-264. [ Links ]
4. Berkoff MC, Zolotor AJ, Makoroff KL, Thackeray JD, Shapiro RA, Runyan DK.Has this prepubertal girl been sexually abused? JAMA, 2008; 300 (23): 2779-2792. [ Links ]
5. Drezett J, Caballero M, Juliano I, Prieto ET, Marques JA, Fernandes CE. Study of mechanisms and factors related to sexual abuse in female children and adolescents. J Pediatr, 2001;77(5):431-9. [ Links ]
6. Finkelhor D,Hotaling G, Lewis IA, Smith C. Sexual abuse in a national survey of adult men and women: prevalence characteristics and risk factors. Child Abuse Negl, 1990; 14(1): 19-28. [ Links ]
7. Drezett J, Junqueira L, Tardelli R, Antonio IP, Macedo Jr H, Vertamatti MAF, Pimentel RM, Abreu LC. Influence of forensic examination on the accountability of sexual violence authors in teenagers. Rev Bras Cresc e Desenv Hum. 2011;21(2)189-97. [ Links ]
8. Hornor G. Ano-genital warts in children: sexual abuse or not? J Pediatr Health Care, 2004;18(4):165-70. [ Links ]
9. Hammerschlag MR, Guillén CD. Medical and legal implications of testing for sexually transmitted infections in children. Clin Microbiol Rev, 2010; 23(3): 493-506. [ Links ]
10. Siegfried E, Rasnick-Conley J, Cook S, Leonardi C, Monteleone J. Human papillomavirus screening in pediatric victims of sexual abuse. Pediatrics, 1998;101(1Pt1):43-7. [ Links ]
11. Bechtel K.Sexual abuse and sexually transmitted infections in children and adolescents. Curr Opin Pediatr, 2010; 22(1): 94-9. [ Links ]
12. Kellogg N. The evaluation of sexual abuse in children. Pediatrics, 2005;116(2):506-12. [ Links ]
13. Glaser JB, Hammerschlag MR, Mccormack WM. Epidemiology of sexually transmitted diseases in rape victims. J Infect Dis, 1989; 11(2): 246-54. [ Links ]
14. Ingram DL, Everett VD, Lyna PR, White ST, Rockwell LA. Epidemiology of adult sexually transmitted disease agents in children being evaluated for sexual abuse.Pediatr Infect Dis J, 1992;11(11):945-50. [ Links ]
15. Girardet RG, Lahoti S, Howard LA, Fajman NN, Sawyer MK, Driebe EMet al. The epidemiology of sexually transmitted infections in suspected child victims of sexual assault. Pediatrics, 2009;124(1):79-86. [ Links ]
16. Syrjanen S, Puranen M. Human papillomavirus infections in children; the potential role of maternal transmission. Critical Review of Oral Biological Medicine, 2000;11(2):259-274. [ Links ]
17. Vanhooteghem O, Müller G, de la Brassinne M. Anogenital condylomata in the children. Practice guidelines for a medical expertise. Rev Med Liege, 2007;62(3):151-4. [ Links ]
18. Rogo KO, Nyansera PN. Congenital condylomataacuminata with meconium staining of amniotic fluidand fetal hydrocephalus: case report. East Afr Med J, 1989;66(6):411-413. [ Links ]
19. Obalek S, Jablonska S, Favre M, Walczak L, Orth G. Condylomata acuminata in children: frequent associa-tion with human papillomaviruses responsible for cutaneous warts. J Am Acad Dermatol, 1990; 23(2Pt1): 205-13. [ Links ]
20. Handley J, Dinsmore W, Maw R, Corbett R, Burrows D, Bharucha H, Swann A, Bingham A. Anogenital warts in prepubertal children: sexual abuse or not? Int J STD AIDS, 1993;4(5):271-9. [ Links ]
21. Cason J, Kaye JN, Jewers RJ, Kambo PK, Bible JM, Kell B, et al.Perinatal infection and persistence of human papillomavirus types 16 and 18 in infants. I Med Virol, 1995;47(3):209-218. [ Links ]
22. Smith EM, Johnson SR, Cripe T, Perlman S, McGuinnessG, Jiang D, et al. Perinatal transmission andmaternal risks of human papillomavirus infection.Cancer Detect Prevent, 1995; 19(2):196-205. [ Links ]
23. Puranen M, Yliskoski M, Saarikoski S, Syrjanen K,Syrjanen S. Exposure of an infant to cervicalhuman papillomavirus infection of the mother iscommon. Am I ObstetGynecol, 1997; 176(5):1039-1045. [ Links ]
24. Frazier L. Genital warts in children. The American Professional Society of the Abuse of Children Advisor, 1998; 11:9-12. [ Links ]
25. Kui LL, Xiu HZ, Ning LY. Condyloma acuminatum and human papilloma virus infection in the oral mucosa of children.Pediatr Dent, 2003;25(2):149-53. [ Links ]
26. Myhre AK, Dalen A,Berntzen K,Bratlid D.Anogenital human papillomavirus in non-abused preschool children. Acta Pediatr, 2003;92(12):1445-52. [ Links ]
27. Cheung PC, Ko CH, Lee HY, Ho LM, To WW.Correlation of colposcopic anogenital findings and overall assessment of child sexual abuse: prospective study. Hong Kong Med J, 2004; 10(6):378-83. [ Links ]
28. Simmons KJ, Hicks DJ. Child sexual abuse examination: is there a need for routine screening for N. gonorrhoeae and C. trachomatis. J. Pediatr Adolesc Gynecol, 2005;18(5):343-345. [ Links ]
29. Marcoux D, Nadeau K, McCuaig C, Powell J, Oligny LL. Pediatric anogenital warts: a 7-year review of children referred to a tertiary-care hospital in Montreal, Canada. Pediatr Dermatol, 2006;23(3):199-207. [ Links ]
30. Jones V, Smith SJ, Omar HA. Nonsexual transmission of anogenital warts in children: a retrospective analysis. ScientificWorldJournal, 2007; 7: 1896-9. [ Links ]
31. Derksen DJ. Children with condylomata acuminata. J FamPract, 1992; 34(4): 419-23. [ Links ]
32. Slaughter L, Brown CR. Colposcopy to establish physical findings in rape victims. Am J Obstet Gynecol, 1992; 166(1Pt1):83-6. [ Links ]
33. Gutman LT, St Claire KK, Everett VD, Ingram DL, Soper J, Johnston WW, Mulvaney GG, Phelps WC.Cervical-vaginal and intraanal human papillomavirus infection of young girls with external genital warts. J Infect Dis, 1994;170(2):339-44. [ Links ]
34. Stevens-Simon C, Nelligan D, Breese P, Jenny C, Douglas JM Jr. The prevalence of genital human papillomavirus infections in abused and nonabused preadolescent girls. Pediatrics, 2000;106(4):645-9. [ Links ]
35. Jesus LE, Cirne Neto OL, Monteiro do Nascimento LM, Costa Araújo R, Agostinho Baptista A. Anogenital warts in children: sexual abuse or unintentional contamination? Cad Saude Publica, 2001;17(6):1383-91. [ Links ]
36. Sinclair KA; Woods CR; Kirse DJ; Sinal SH. Anogenital and respiratory tract human papillomavirus infections among children: age, gender, and potential transmission through sexual abuse. Pediatrics, 2005; 116(4): 815-25. [ Links ]
37. Wingood GM, Seth P, DiClemente RJ, Robinson LS. Association of sexual abuse with incident high-risk human papillomavirus infection among young African-American women.Sex Transm Dis, 2009;36(12):784-6. [ Links ]
38. Vanchiere J, Demmer G. Human polyomaviruses and papillomaviruses. In: Feigin R, Cherry J, Demmler G, Kaplan S, eds. Textbook of Pediatric Infectious Diseases. 5th ed. Philadelphia, PA: Saunders; 2004: 1809-1831 [ Links ]
39. Carr J, Gyorfi T. Human papillomavirus: epidemiology, transmission, and pathogenesis. Clinics in Laboratory Medicine, 2000;20(2):235-254 [ Links ]
40. Estreich S, Forster GE, Robinson A. Sexually transmitted diseases in rape victims. Genitourin Med, 1990; 66(6):433-8. [ Links ]
41. Jenny C, Hooton TM, Bowers A, Copass MK, Krieger JN, Hillier SL, et al. Sexually transmitted diseases in victims of rape. N Engl J Med, 1990; 322(11): 713-6. [ Links ]
42. Lacey HB. Sexually transmitted diseases and rape: the experience of a sexual assault centre. Int J STD AIDS, 1990;1(6):405-9. [ Links ]
43. Bell TA, Stamm WE, Wang SP, Holmes KK, Grayston JT. ChronicChlamydia trachomatis infections in infants. JAMA, 1992;267(3):400-402. [ Links ]
44. Handley J, Hanks E, Armstrong K, Bingham A, Dinsmore W, Swann A, Evans MF, McGee JO, O'Leary J. Common association of HPV 2 with anogenital warts in prepubertal children. Pediatr Dermatol, 1997; 14(5): 339-43. [ Links ]
45. Hymel KP, Jenny C. Child sexual abuse. Del Med J, 1997;69(8):415-29. [ Links ]
46. Rehme MFB, Carvalho NS, Ihlenfeld MFK, Chuery ACS. Condiloma acuminado em crianças e adolescentes. Rev bras ginecolobstet, 1998; 20(7): 377-80. [ Links ]
47. American Professional Society on the Abuse of Children. Sexual abuse of children. In: Myers J, Berliner L, Briere J, Hendrix C, Jenny C, Reid T, editors. The APSAC handbook on child maltreatment. 2nd ed. Thousand Oaks Sage; 2001.p55-78. [ Links ]
48. Goldenring JM. Secondary syphilis in a prepubertal child.Differentiating condyloma lata from condyloma acuminata. N Y State J Med, 1989; 89(3): 180-1. [ Links ]
49. Delmanto C, Delmanto R, Delmanto-Jr R, Delmanto FMA, editores. Código penal comentado. São Paulo: Saraiva; 2010. [ Links ]
50. Estatuto da Criança e do Adolescente. São Paulo: Imprensa Oficial do Estado de São Paulo; 2008. [ Links ]
51. Atabaki S, Paradise JE. The medical evaluation of the sexually abused child: Lessons from a decade of research. Pediatrics, 1999; 104:178-86 [ Links ]
 Corresponding author:
Corresponding author:
jefferson@drezett.com.br
Manuscript submitted Apr 08 2011
Accepted for publication Sep 10 2011.

{kind=link}
{kind=link}