










Serviços Personalizados
artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282
Rev. bras. crescimento desenvolv. hum. vol.22 no.1 São Paulo 2012
ORIGINAL RESEARCH
Profile of the free distribution of emergency contraception for adolescents in São Paulo's counties
Regina FigueiredoI; Silvia BastosII; Joyce Lenz TellesIII
IInstitute of Health of the Department of Health of São Paulo. Rua Santo Antonio, 590, CEP 01314-000, São Paulo, Brazil. Master's degree in Anthropology from the University of Sao Paulo. Researcher, Institute of Health. Project developed at the Center for Health Practice of the Health's Institute of Health Ministry of São Paulo from 2006 to 2008, self-financed
IIDoctor in Science and Master in Public Health. Researcher, Institute of Health Department of São Paulo
IIINurse Specialist in Family Health of State University of Londrina and Specialist in Public Health in Institute of Health Department of São Paulo
ABSTRACT
The position adopted by São Paulo's counties, which received amounts of emergency contraception from the Federal Health Department in 2005 and 2006, is described in relation to the distribution of these to adolescents. Using quantitative surveys carried out with semi-structured questionnaires sent by e-mail to the Municipal Health Offices: influxes, services and health care professionals and the criteria of dispensation were examined. Of the total, 91.0% answered to the research, demonstrating that 85.4% began to offer the method to adolescents less than 18 years old, especially at emergency rooms (69.1%). At public health care clinics traditional and public family health care clinics there was less integration, 65.3% and 37.6%, and in services specialized in adolescent care only 31.9% of the counties offer them (percentages not excludent). Usually, the distribution is carried out by doctors and/or nurses, but 30% of clinics sub-utilize the nursing potential. Cases of sexual violence are fundamentally attended to, but excluding these cases, there is a drop of 10 to 30 percentage points in the distribution of emergency contraceptive to adolescents in cases of the failure or non-use of the regular contraceptive. The conclusion is that there exists selectivity in the method's dispensation, very scarcely offered in Basic Adolescent Health Care Services, which makes it difficult for adolescents to have access to emergency birth control in situations where pregnancy is a risk. This selective behavior among health care professionals has become common practice and goes against the initial objectives of the Federal Health Department. This position is due in part to health care professionals not being up to date on the laws and federal norms concerning Sexual and Reproductive Health, and also to the lack of knowledge of the method's mechanism action (sometimes identified as dangerous or abortive), as well as the prejudice towards adolescent sexual practices-leading to the purchasing of emergency contraceptive in drugstores and its incorrect use.
Key words: health management; family planning; birth control; adolescent; contraceptives post-coital hormonal; emergency contraception.
INTRODUCTION
Starting with the mid-80s, the World Health Organization (WHO)1 emphasized the importance of the emergency contraception in the prevention of unplanned pregnancies and therefore abortions, as the only contraceptive method for post-coital use. This contraceptive, popularly known as "the morning-after pill," is effective in preventing pregnancy in 98% of the cases (if used within 24 hours after unprotected intercourse) to 75% (within 25 to72 hours)2.
For this reason, the method is presented as a contraceptive strategy aiming to promote sexual and reproductive health, that should be freely distributed inclusive among the adolescents3, once this public group shows maturity, evolution of psychological patterns, identity configuration and is in the stage of passing from the dependent child life to the adult independence4, factors that often lead to the practice of unprotected sex5. Coming from these risk factors, the adolescent pregnancy, because of its repercussions, is seen today as a social and health problem due to the potential risk and impact onto the teenagers and their babies6.
According to IBGE - Brasilian Institute Geography and Statistics, in the decade the number of mothers aged between 15 and 17 increased from 6.9% to 7.6%7. It is estimated that, in most of the cases, the pregnancy in adolescence is occurring, in average, between the first and fifth sexual intercourse5. The situations related to pregnancy/childbirth, that represent the third cause of hospitalization among girls aged under 19 in SUS - Unified Health System8, are also expressed in number of abortions among the under 19 years of age public, to which are attributed 1/4 of the maternal deaths in the nationwide9.
Thus, the access to Family Planning strategies proves to be crucial to adolescents in order for them to be able to exercise their right to sexual health at this stage of life. In Brazil, aiming to expand the supply variety of contraceptives and promote the risk reduction of these occurrences, the emergency contraception was included in the Family Planning guidelines starting with 199610; in the same decade was regulated its free distribution in the Victims of Sexual Violence Care Unites11. Both issues were recommending the administration of combined oral contraceptive pills (Yuzpe method), the only administration method available in that time. Both documents present the directions for using the method in pregnancy risk cases, inclusive by adolescentes10, 11.
Currently, emergency contraception is prescribed prioritizing its format as a single dose (1.5 mg tablet or two tablets of 0.75 mg levonorgestrel), introduced in Brazil with authorization from ANVISA - National Agency of Sanitary Surveillance in 199812. The Ministry of Health2 recommends the method for any case where there exists exposure to the risk of pregnancy: non-use, misuse, or failure of the regular contraceptive method as well as sexual violence/rape. This initiative is considered crucial in countries like Brazil, where abortion is permitted only in special situation, a fact that enhances the practice of illegal abortions and, consequently, high maternal mortality rates13,14.
The beginning of free distribution of emergency contraception in the Brazilian public health system, under the one-pill dosing form was initiated by the Ministry of Health in 2002, first in the Victims of Sexual Violence Care Units; in 2003 began the free distribution through the Public Health Care System, aiming the supply to the UBSs (Primary Health Care Units), initially in few cities registered in the programme12. The distribution into the Primary Health Care Units became significant in 2005 due to the "2004-2007 Action Plan" developed by the Ministry of Health15, which included the growth of the contraceptives distribution area, proceeding to the first major quantity acquisition16, 65,370 contraceptives units were shipped to 153 Brazilian municipalities; in the same year, technical material was drafted and distributed to the health professionals and managers seeking guidance on this new issue2. In 2006, continuing the same policy, the Ministry of Health sent 49,952 other doses to 573 municipalities across the country17. Considering only the state of São Paulo, during 2005 and 2006, loads of emergency contraception were sent to 119 (18.5%) of its 645 municipalities, prioritizing those with 100,000 inhabitants or more.
The relevance of studying the implementation processes of this input in the Primary Health Care System, as well as the description of its flows, the involvement of the professionals and its supply to the public in the cities is crucial in order to assess whether the public health goals advocated nationally are efficiently implemented. At the same time, the adolescents' case deserves a detailed analysis for illustrating that the introduction of this method is also benefiting this very social category.
Thus, this research aims to describe the modus operandi adopted by the municipalities of the Sao Paulo state which received large amounts of emergency contraception from the Ministry of Health in 2005 and 2006, aiming its free distribution to adolescents.
METHODS
The research "Evaluation of the Emergency Contraception Free Distribution in the Municipalities of São Paulo State", developed by the Institute of Health of the Ministry of Health of São Paulo state between May of 2006 and December of 2007, aimed to identify: the responsible, the established flows, organizations and professionals involved in supplying the emergency contraception in the 119 counties benefited with loads of contraceptives freely supplied by the Ministry of Health between 2005 and 2006, as well as the public benefiting of this input and the criteria used into its free distribution, conveniences and barriers into the distribution effectiveness.
The data collection was conducted between September and November of 2006 through semi-structured questionnaires distributed to the local health departments named by the Ministry of Health as beneficiaries of the method. Data was quantitatively organized and analyzed using the SPSS 12.0 software, considering simple frequencies for the situational description, since the expansion of the results for the entire state was not intended, each city showing distinct and specific circumstances and having a differential input acquisition by the municipality of Sao Paulo. The research complied with the Resolution 196/96 of the National Committee of Health of the Ministry of Health, being approved by the Committee of Ethics in Human Research of the Institute of Health of the Department of Health of São Paulo state in 2006.
The article is prioritizing the analysis of the emergency contraception free distribution in the public health care units, the offer of easy access to the method for the adolescents at common risks of unplanned pregnancy (like non-contraceptive use or failures of the ones in use); in other words, being focused on the Primary Health Care Units (including the Family Health strategy), as well as Emergency Care Units and Specific Care Units for Adolescents.
RESULTS
Of the 119 municipalities in the state of São Paulo benefited by the distribution of emergency contraception by the Ministry of Health in 2005 and 2006, 101 (84.9%) confirmed receiving the input and responded the survey. The others reported not receiving the method, so they were excluded from the analysis. The city of Sao Paulo has not responded the survey, so the data presented reveals the situation of other big, medium and small cities.
Among the counties that confirmed receiving the method, 2 (2.0%) reported inability to freely distribute the loads to the population because of the expired validity. Another 16 (15.9%) responded that the free distribution to the public had not started yet "from other reasons." Thus, only 77 (76.2%) out of the total municipalities benefited from the Ministry of Health initiated the free distribution and, therefore, responded the questionnaire in its entirety, these being considered for the analysis of flows, professionals involved in the process and criteria procedure adopted in the free distribution of the input. Yet, the amount of services presented in item 1 of the results was estimated taking into account the 101 municipalities that have confirmed the reception of the input, while 23.8% of them are unable to present a detailed analysis of its distribution.
- Free Distribution of Emergency
Contraception in Differente Health Units:
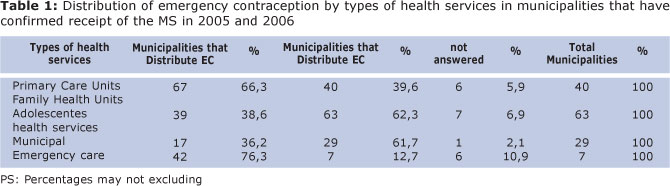
Of the 101 municipalities that have confirmed the delivery of the emergency contraception, 47 (46.5%) reported having special health care services for adolescents. Of these, only 17 (36.1%) reported the commencement of the emergency contraception free distribution. In all the surveyed municipalities exist UBSs - Primary Health Care Units (including USFs - units promoting strategies for Family Health), of these 67 (59.3%) included the free distribution of the method in the traditional UBSs and 39 (35.8%) in USFs.
Of these 101 municipalities, 55 (54.4%) reported to have PAs - Emergency Care Units. In 76.3% of these municipalities was reported the commencement of emergency contraception free distribution in their units (Table 1):
- Free Distribution of Emergency
Contraception in Adolescent's Care Units:
Of the 17 (36.2%) municipalities that have initiated the free distribution of emergency contraception in Specific Adolescent Care Units, 2 (11.8%) responded to be offering the method "only for adult women", in other words, aged above 18, reducing to at least 15 (31.9%) the free distribution among the legal under-aged adolescents (Figure 1).
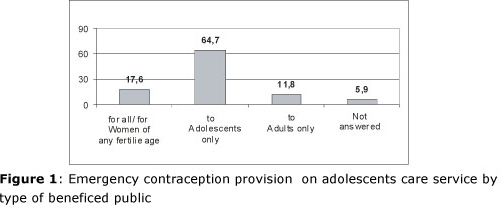
Regarding the attendance situation, in 13 of the units, (76.5% of them) the emergency contraceptive was freely offered in any situation of pregnancy risk, in 1 of them (5.9%) only in regular contraceptive failure cases of and in 2 of these (11.8 %) only in sexual violence cases.
The prescription of the input in 8 (47.1%) of these municipalities was issued only by physicians, in other 8 (47.1%) by physicians and/or nurses and in 1 (5.9%), exclusively by nurses. In 5 of the (30.3%) municipalities the free distribution of the method was carried on only after a scheduled appointment and in the other 12 (70.0%) there was no such requirement. Specific guidance on the dosage was given to the public in 4 of the municipalities (25.0%); in the other 12 (75.0%) was also provided guidance on the importance of a carefully choice of a regular contraceptive method and the regular use of condom to prevent sexually transmitted diseases (STDs), including AIDS.
- Free Distribution of Emergency
Contraception in the Emergency Units:
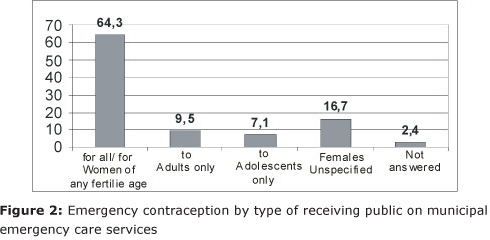
Of the 101 municipalities that have confirmed receiving emergency contraception from the Ministry of Health, 55 (54.5%) had municipal Emergency Care Units (PAs), 12 (21.8%) of them being municipalities that do not have Specific Adolescents Care Units. Of the municipalities with PAs, 42 (76.3%) introduced the free distribution of emergency contraception in their units. Of these, 4 (9.5%) provided the method "for adult women only" (aged 18 or more); 3 (16.7%) "for adolescents only", considering the range between puberty and adulthood; 27 (64.3%) for "women of any childbearing age"; in 7 (16.7%) there was no specification on the public's age (Figure 2).
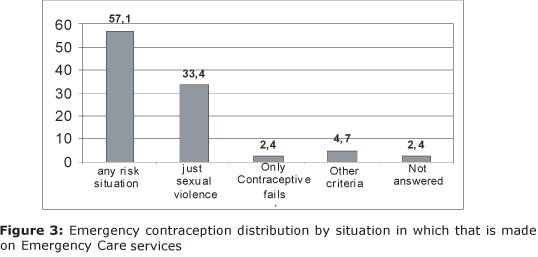
In 14 (33.4%) of the municipalities where the PAs units freely offer the method, the prescription is made only in sexual violence cases. In 1 (2.4%) only in regular contraceptive failure cases, in 2 (4.7%) there is another criteria for the prescription, and in 24 (47.1%) in any situation of pregnancy risk (Figuere 3).
The prescription in the PAs was carry on in 6 (35.3%) of the counties only by physicians, in other 6 (35%) by doctors or nurses, in 1 (5.9%) exclusively by nurses and in 4 (23, 5%) by other professionals; in 6 of the municipalities (35.3%) was not required scheduled appointment in order to obtain the emergency contraceptive, the attendance being immediate, other 3 (17.6%) required scheduling an appointment and 8 (47.1%) did not provide information.
- Free Distribution of Emergency
Contraception in Primary Health Care Units:
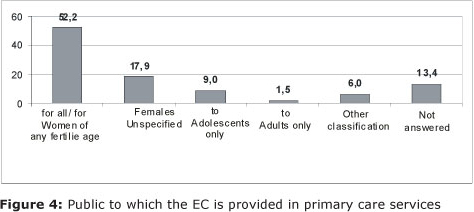
All counties that confirmed receiving loads of emergency contraception from the Ministry of Health have primary health care units (UBSs). Of these, 67 (59.3%) had implemented the free distribution in their units. The prescription is made in 1of them (1.5%) just to "adult women" (age 18 or more) and 41 (61.2%) responded they also benefit the adolescents aged under 18 (Figure 4).
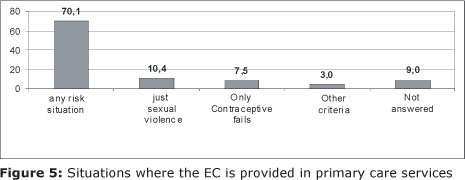
The free provision of the method in UBSs was being attended in 7 (10.4%) counties only for sexual violence cases, in 5 (7.5%) only for regular contraceptive failure cases, in 47 (70.1%) for any risk of pregnancy cases and in 2 (3.0%) was confirmed the free distribution for other situations (Figure 5).
Among the 67 municipalities that offer the method in UBSs, 14 (20.9%) have stated the need for scheduled appointments for delivering the method. In 25 of the units (37.3%) the free distribution was being performed only by physicians, in 23 (34.3%) by physicians or nurses and in 7 (10.4%) only by nurses. In 7 (10.4%) of the municipalities, were indicated other professionals involved in the free distribution of the emergency contraception and 5 (7.5%) did not answer the question.
- Free Distribution of Emergency
Contraception in Family Health Units:
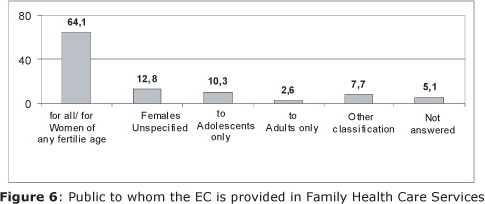
Of the 101 municipalities that received loads of emergency contraception from the Ministry of Health all have USFs, and, of these, 39 municipalities (38.6%) have implemented the free distribution of the method in their units, given that in 1 (2.6%) municipality the service is offered only "for adult women" and in 29 (74.4%) counties is supplied also to adolescents of any child-bearing age (Figure 6) and in 38 (97.4%) could perform the service but gave vague answers or did not answer.
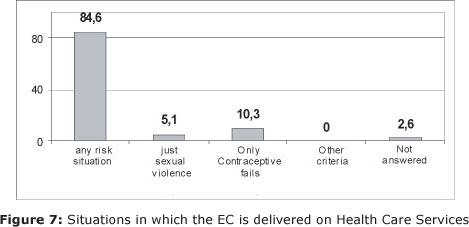
Of USFs that were freely providing the method, 2 (5.1%) were offering it only in sexual violence cases; 33 (84.6%) in any risk of pregnancy case; 5 (7.5%) only in regular contraceptive fail cases and 4 (10.3%) also in other situations (Figure 7).
If required, 20.5% of the municipalities demanded an appointment in order to provide the method in their units. In 14 (38.9%) of them the free distribution was performed only by physicians; in 2 (5.6%) counties by doctors or nurses; in 15 (41.7%) exclusively by nurses; in 3 (8.3%) were identified other professionals involved in the free distribution of the contraception, and 5 (13.9%) did not answer the question.
- Free Distribution of Emergency
Contraception for Adolescents Considering and Excluding Sexual Violence Cases
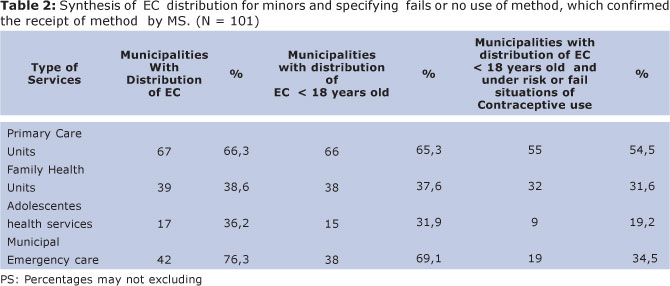
From the 85.4% of the 101 counties that received and the claimed the free distribution of the method to adolescents, 69.1% of the cases occur in cities that have PAs. Excluding the cases of rape, only 34.5% of the municipalities with PAs attend adolescents in any other common risk of pregnancy situation.
Similarly, the supply of the method to this very public in the traditional UBSs and USFs that occurs in respectively in 65.3% and 37.6% of the counties, is reduced to 54.5% and 31.6% when excluded the cases of sexual assault/rape (Table 2).
- Impediments in The Implementation of
Emergency Contraception
Among the 101 counties that have confirmed receiving emergency contraception from the Ministry of Health, 18 (17.8%) reported obstacles in its implementation. Regarding the cause of these difficulties, 12 (66.7% of those citing problems, 11.9% of total) reported as coming from UBSs, 8 (44.4% of those citing, 7.9% of total) as coming from USFs; 8 (44.4% of those citing, 7.9% of total) as impediments coming from the Health Department and its managers; in 5 (16.7%, 10.6% of the municipalities that have these units) originating from the Adolescent Care Services.
The types of problems identified were: 5 of them (27.8%) cited the resistance of the Departments' of Health sectors to implement the free distribution of the method, in 4 (22.2%) the deficiency to authorize the release of the input by the nursing staff and in 9 (50%) other obstacles as: the request of signed consent forms for users in order to obtain the method; (being required the signature or physical presence of the legal guardian for adolescents under 18 and cases where it was attempted or actually refused the delivery for adolescents' use. Besides, was noted in the data collected, the clear refusal to provide the method to adolescents younger than 18 years in 14.6% of these municipalities. Was also cited a case of refusal to supply patients with HIV/AIDS.
DISCUSSION
Knowing the insufficient amount of Specific Adolescents Care Units in the Sao Paulo's counties (only 46.5% of the municipalities in the research, usually 1in each city), the possibility that adolescents could access the emergency contraception for the most common pregnancy risks such as failure or non-use of regular contraception18 can only be accomplished by freely distributing it through UBSs, including USFs, and PAs. Thus, we can note that, even if 85.4% of the 101 municipalities that received the method generally stated to freely distribute it to adolescents, it appears that much less than half was benefiting teenagers aged under 18 in the primary health units, mainly in the PAs (in 69.1% of the cities that have PAs), this rate being almost halved (34.5%) for situations other then rape, which are much more often faced by adolescents.
The same sharp drop in the rate of municipalities that freely provide emergency contraception to under 18s in other pregnancy risk situations (other than the sexual violence) is observed in traditional UBSs and USFs (from 65.3% and 37.6% of municipalities , respectively, to 54.5% and 31.6%) showing restrictions in distributing the method for common risk situations faced by adolescents. Nevertheless, the most traditional UBSs were the units that offered easier access to the method for adolescents aged under 18, at any risk situation.
Ironically, the Specific Adolescent Care Units, which should be more responsive to this policy, showed more restrictions in provide it to minors under 18 years (only 31.9% did so). In 12.7% the free distribution is only in rape cases, which adds another drop in the results (to 19.2%) for other pregnancy risk situations.
This undersized free distribution (only 54.5% of the municipalities surveyed) for any common pregnancy risk, faced in the daily adolescent life, provide evidence to managers and public health professionals about the need to update the approach and the legislation on Sexual and Reproductive Health for adolescents, especially in the 14.6% of the municipalities who effectively refused to carry out the free distribution for this audience at any risk situation. Denying emergency contraception, or offering it in a limited way (only for sexual violence cases) restricts the principles advocated by ECA - Statute of Children and Adolescent19, that turn adolescents into citizens with equal rights, being able to change their social status with respect to the old legislation.
The ECA states that it should be granted for this social category the "equal access to actions and services for the promotion, protection and restoration of health"19. Such promotion includes, of course, preventive measures in the field of Sexual and Reproductive Health, an area that is focused on the main causes of morbidity and mortality in adolescents, so it automatically integrates the guidance and access to contraception for STD/AIDS - as provided to the sexually active adult audience. In this sense, adolescents have the same right to the Family Planning practice guaranteed by the Constitution20, which should be generally applied by SUS throughout the free distribution of pregnancy prevention methods, as well as access to condoms for protection against STDs, as the National Program on STD/AIDS states.
The beginning of sexual life in Brazil and thus the risk for unplanned pregnancy begins, on average, at 15-16 years, depending on the region, as shown in the PNDS - 2006 National Demographic Health Survey21, pointing out the importance of information provision, but mainly, the access to contraception, including emergency contraception for adolescents.
This awareness must be carry out independently of the presence of parents or legal guardians, as cited in the "Theoretical Framework and Reference on Sexual and Reproductive Health of Adolescents and Youth"22. This regulation aims to ensure the well-being and health of adolescents and professional ethics, respecting the individual right to privacy and confidentiality, and corroborate the Federal Medicina23, the Board of Medical Ethics24 and the Brazilian Pediatrics Association25.
For this reason should be mandatory the informed consent of the adolescent in order to establish contact with his family and/or legal tutors22, a policy that would endorse the confidence and presence of adolescents in the public health care units. In more complex situations is recommended that the health professionals should encourage and suggest teenagers a closer relation with theirs' families/legal tutors, and exclusively in the cases of adolescents' life-threatening situations, as the Ministry clearly stipulates, the break of the confidentiality clause by professionals and the immediate notification of the legal tutor22.
All these principles of extensive care in Sexual and Reproductive Health, especially when it comes to adolescents, are internationally recommended through the UN Conferences in Cairo and Beijing, of which Brazil is a signatory, thus leading to a federal level of application in the health care practices.
Another restricting factor into the access to the emergency contraception for adolescents is the requirement of medical exams, reducing the potential of UBSs' nursing staff in more than 30% of the surveyed municipalities, as well as the requirement of scheduled appointments in order to obtain the contraceptive, observed in 20% of the units. The Family Planning Law No. 9.263/9620, guarantees the competence of health professionals, regulating the attendance, information and contraceptive actions, using the methods available for these purposes, which include oral-hormonal contraceptives, and therefore emergency contraception.
With respect to the nursing staff, what currently exists at federal level is: the Law of Professional Exercise No.7.498/8626 and The Resolution No. 271/0227. This legislation defines that the free distribution of contraceptives to teenagers and women can also be performed in nursery appointments or at the units' admission desk, including the prescription and administration of these drugs available in the public health units' pharmacies24. In this sense, the involvement of nurses in providing emergency contraception helps into avoiding the "queue jump" cases, doctors' extra-burden or waiting time factors that threaten its higher effectiveness in the first 24 hours2.
The nursing staff plays a key role and has legal authority to operate in the Health Promotion procedures of nursing appointments, front-desk attendance and home appointments, together with its important part in Health Education.
The research shows that 17.8% of municipalities reported problems in the implementation of emergency contraception, obstacles that included in 7.9% of cases the managers themselves. The lack of information and update on the methods' mechanism of action, regarding its' technical and scientific aspects, shows that many still believe to be risky or abortive. At the same time, it turns out to be very present, in the professional and managerial practice, the personal ethic factors with respect to guidance and free distribution of contraceptives to adolescents, indicating the resistance to recognize them, especially girls, as self-ruling individuals in their sexuality and sexual practices.
This transposition of day to day culture into the public health is also depicted: in the restriction of the free distribution of emergency contraception to this audience, where the prescription is made only in cases of sexual violence and in situation when authorization from the legal tutors is required. This transposition was also reported by Lefevre et al28, in the research on South Area of São Paulo UBSs, where about 15.0% of professionals interviewed stated that they would not recommend emergency contraception to adolescents in any case and 23, 3% responded they consider the religion of the user when prescribing it, reinforcing the erroneous idea of the method as an abortive.
It has to be pointed out that the decentralization and municipalization of health care services have hampered the follow-up and monitoring of policies implementation at national level, making it easier for managers and local health workers to build resistance into its execution29. This was demonstrated by legal lawsuits in Sao Jose dos Campos, Jundiai and Vargem (municipalities of São Paulo), which attempted to create their own laws aiming to prohibit the sale and free distribution of the method - actions barred by the Public Prosecutor as being unconstitutional30.
All these obstacles perpetuate the neglect of adolescents, leaving them in constant vulnerability state in relation to Sexual and Reproductive Health, mainly towards unplanned pregnancies and infections with STD/AIDS31, showed by the high pregnancy rates below 19 years of age (about 21% of the country), apart of the abortion cases, which overwhelm the SUS hospitals8. Such occurrences are often the result of situations experienced by girls and boys who are beginning their sexual life and, therefore, have unprotected sex because they are starting to accept themselves as sexually active and still have no perception of the clear risks of these practices5,32.
The completion of the emergency contraception free distribution among teenage audiences is therefore crucial at this moment when there already exists an ample acknowledgement about the method (96%) between jovens33 and its use has been made without the guidance of health care professionals, behavior observed in more than 20% of the sexually active high school students of the state of São Paulo18, data reported nationally in the 2006 PNDS21. In some groups of university students from various regions of the country, Silva33 found a use of 41.8%.
The fact that the method turned widely known and is being used by young people, leads to alarm about its' potential abusive use6. Meanwhile, national and international studies show that the use of emergency contraception to a decrease in the use of other regular contraception methods, nor condoms.18, 34, 5, 35 This figures can be considered as "luck", while the public health services omitted this issue. By not freely providing emergency contraception to adolescents, not giving a speech on its correct use, taking advantage of the demand in its units and provide accurate information and advice on the choice of a regular contraceptive method, this public is sent to acquire it directly in private pharmacies and drugstores, like the majority of adolescents (74% in São Paulo), as observed by Figueiredo and cols18.
This happens because, although in our country the method requires prescription (unlikely other countries), this condition is not usually complied36. The direct sale of the medicine into pharmacies already exceeded 5 million annual doses in Brasil37, largely acquired by adolescents, as also Castro and Rodrigues Portugal38 mention, existing a large approval in the usage of the method in case of emergency.
Is this non-oriented purchase that gives space to cases when adolescents are adopting the misuse of the emergency contraception method as a regular one, like Araujo and Costa39 noted in the Pernambuco public health system; even if the regular monthly usage does not still reach a high rate, less than 15% of this public is using it continuously as noted by Figueiredo et al18, this percentage will tend to grow if there will be no change in the attendance of adolescents in the public health units.
Thus, even though exists an initial attempt to freely distribute the emergency contraception to the population, only about half of the studied São Paulo municipalities, which confirmed receiving the loads sent by the Ministry of Health, offered the method to adolescents aged under 18. The highest distribution rate to this audience occurred in the counties that benefit of PA units, in 2/3 of the surveyed municipalities in the UBSs and in only 1/3 in the USF units. The free distribution of the contraceptive in all these health units is restricted and more focused on the sexual violence cases so its implementation rate drops from 10 to 30 percentage points (except for the USFs where decreased 5 points) for prescribing it in other risky conditions recommended by the Ministry of Health such as failure or non-use of regular contraception method by adolescents.
It was also noted that there still exists misinformation about the action mechanism of the method among professionals who fear that it is too strong, dangerous or abortive, which indicates the need of technical update on the information about this contraceptive. Likewise, there seems to be a concern for many managers and health professionals in the attendance of adolescents aged under 18 who solicit regular or emergency contraception, proving their need to update on Sexual and Reproductive Rights of adolescents. These concerns create access restrictions that are present in both USFs and UBSs, as well as in PAs. There were also observed municipalities that created "additional" obstacles into the free access of this public to the emergency method by clearly restricting its free distribution, or conditioning it by setting random age ranges (from 13, 15 of age, etc.., depending on the health care unit), or by requiring authorization or physical presence of the legal tutors in order to prescribe it.
The Adolescent Care Units, contrarily to theirs' mission of health promotion for this very population, also showed resistance in providing access to the emergency contraception. This clearly shows as not seeing the method as an important medicinal alternative to promote health, to be used for reducing pregnancies and abortions or as a way of attracting the adolescents to these units.
PAs are crucial into accessing the method in the weekends, however, considering the burden of these units, it is obvious the need of the decentralization of this process and its inclusion into the Family Planning strategy of the UBSs and USFs.
The distribution of the emergency contraception should exclude any form of short or medium term scheduled appointment requirement, since its effectiveness totally depends on its emergency use. It is therefore necessary to develop fast access mechanisms that guarantee its effectiveness and, at the same time, attend the adolescents' demand with the minimum possible exposure in order to avoid their embarrassment.
Health care services should maximize the use of its human resources including in the nursing staff routines the free distribution of the emergency contraception. It was noted the waste of this resource in more than 1/3 of the surveyed units which are not adopting the COFEN requirements. Nurses and other common health workers, after trained, could disseminate information about the emergency contraception in their communities; this way they would achieve greater performance and would bond with teenagers through "out-doors" actions and would have the opportunity to guide and inform outside the schedule hours of the UBSs and USFs. It is also recommended the insertion of the emergency contraception strategies not only in theirs' oral advices, but also in the educational materials.
Although the research found that there exist guidelines on contraceptive methods and STD/AIDS prevention in most of the municipalities that are freely distributing it to adolescents, continue to exist ¼ who do not complete it. Therefore, it is essential that all the professionals and referral units attend the demand of emergency contraception in the UBSs and USFs for all the family planning participants, in gynecological exams and during the prescription of regular use contraceptives, which are safer, in order to provide a full care service on STDs/AIDS as well as HPV prevention among this audience.
In order to expand and facilitate the purpose of these actions, the trained nurses and communities' health workers, supervised by their staff, can also play an important role in disseminating and establishing links with other sectors and services that work with the population, such as: drug addicts centers who treat adolescents, centers that work with teenagers at social risk or with mental disorders or deficits, or STD/AIDS prevention centers that work with teenagers, as well as pharmacies, non-governmental organizations that are also related to the teenage audience. Thus, the chance of free distribution and access to the method will be extended, reducing the large spectrum of adolescents' vulnerabilities through proactive guidelines against risky sexual relations.
It should be highlighted that the slight mention and low distribution of emergency contraception to adolescents in the public health units recorded during this study, leads to the self-medication with the method by uncontrolled purchase in pharmacies and increases the risk of its misuse, as improperly, repetitive and without accurate directions. At the same time, is keeping away the adolescents from useful additional information on sexual and reproductive health, which ultimately forfeits theirs' rights granted by policies and regulations.
REFERENCES
1. World Health Organization Emergency Contraception: A guide to the provision of services [online]. [Accessed 12/11/2007]. Available at http://www.who.int [ Links ]
2. Ministry of Health Emergency contraception: Questions and answers for health professionals, Brasilia, 2005. 20p. [ Links ]
3. Legal framework of the Ministry of Health: Health, a right of adolescents. Brasilia, 2005. 58p. Series A. Technical Standards and Manuals. [ Links ]
4. World Health Organization El embarazo y el en la abortion adolescence: report of la Reunion de la OMS. Geneva, 1975. p. 10. Technical Reports Series. [ Links ]
5. Figueiredo R, Neto J. Andalaft Use of Emergency Contraception and Condoms among Teens and Young. New York: Journal of SOGIA-BR. 2005, 2 (2): 4-6. [ Links ]
6. Monteleoni ML, Takiuti AD, Conception I, J. Kerr Emergency Contraception and Adolescents [abstract]. Latin American Congress of Gynecology and Obstetrics, 2006, Rio de Janeiro, Brazil. [Text on the Internet]. New York: REDECE, 2005. [Accessed November 2010]. Available at: http://www.redece.org/resumo%20albertina. [ Links ]pdf
7. IBGE. Young Mothers. Brasilia, 2008 [accessed November 2010]. Available at: http://www.ibge.gov.br/ibgeteen/datas/saude/jovensmaes.html [ Links ]
8. DATASUS. Hospitalization data [accessed 2010]. Available in http:www.datasus.gov.br [ Links ]
9. IPAS. Rio de Janeiro: Youth Network, 2005 [accessed November 2010].Available at: http://www.ipas.org.br [ Links ]
10. Ministry of Health Emergency contraception. Support Planned Parenthood. Support service to Women's Health, Brasília, 1996. p.121-125. [ Links ]
11. Ministry of Health Prevention and Treatment of Diseases Resulting from Sexual Violence Against Women and Teens - Technical Standard. Brasilia, 1999. 40 p. [ Links ]
12. R. Figueiredo Emergency Contraception in Brazil: the need, access and national politics. Rev. of Sexual and Reproductive Health. IPAS, September, 2004. 18p. [Accessed 13/11/2010]. Available at: http://www.ipas.org. [ Links ]br
13. Hardy E, Duarte GA. & Et al. Emergency contraception in Brazil: facilitators and barriers. Rio de Janeiro: Book of Public Health, 2001, 17 (4): 1031-1035. [ Links ]
14. Wannmacher L. Emergency contraception: evidence versus prejudice. Rational drug use: selected topics. Brasilia, 2005, 2(6): 1-6. [ Links ]
15. Ministry of Health Women's Health Coordination. Plan of Action 2004-2007. Brasília, 2004. 48p. [ Links ]
16. Ministry of Health Policy Report. Department of Health Care Department and Strategic Action Program. Annual Report 2003 to 2006 - National Policy for Integral Attention to Women's Health. Brasilia, 2007. 128p. Series C - Projects, Programs and Reports. [ Links ]
17. Figueiredo R, Bastos S. Final Report of the Survey Assessment of Distribution Emergency Contraception in the municipalities of São Paulo. London: Institute of Health, 2008. 52p. [ Links ]
18. Figueiredo R, Escuder MM, LR Puppo, Puerto Alvez MCG. Knowledge and Use of Emergency Contraception for adolescents: a study with high school students of São Paulo. London: Institute of Health, 2008. 36p. [ Links ]
19. Brazil. Statute of the Child and Adolescent (ECA): Law No. 8069, July 13, 1990. [ Links ]
20. Brazil. Federal Law No. 9263, January 12, 1996. http://www.jusbrasil.com.br/legislacao/anotada/2899797/art-10-da-lei-9263-96 [ Links ]
21. Ministry of Health Center for Analysis and Planning. DHS - National Demographic and Health of Children and Women in 2006. Brasilia, 2009. 302p. [ Links ]
22. Mystery of Health and Theoretical Framework Reference: Sexual and Reproductive Health of Adolescents and Youth. Brasilia: MS, 2006. 56p. Series B - basic texts of health. [ Links ]
23. CFM - Federal Council of Medicine. Code of Medical Ethics. Brasilia, 1988. [ Links ]
24. COFEN - Federal Council of Nursing. Resolution 271/2002. Brasilia, 2002. [ Links ]
25. Saito MI, MM Leal. The exercise of sexuality in adolescence: the contraception issue. New York: Journal of Pediatrics, 2003; 25 (1): 36-42. [ Links ]
26. Brazil. Act 7498/86. Regulation of Professional Practice Nurses. Official Gazette: Brasilia, June 26. 1986, Section 1, p.9273-5. [ Links ]
27. Brazil. Resolution 271/02. COFEN, 2002. Disponible In: http://site.portalcofen.gov.br/node/4308 [ Links ]
28. Lefebre F (ed). Health professionals, teenagers and emergency contraception: helping to decide. New York: IPDSC, 2010. 32p. [ Links ]
29. ECOS - Communication on Sexuality. Reference Framework for the Promotion and Defense of the Rights of Juveniles to Emergency Contraception. New York: Echoes, 2006. 25p. [ Links ]
30. Figueiredo R, Bastos S. Health and sexual and reproductive rights: the Judiciary must guarantee access to emergency contraception. TMM Keinert, Bastos de Paula SH, JRA Bonfim. London: Institute of Health, 2009. p.119-26. [ Links ]
31. Aine Schutt-J, M. Maddaleno Salud Sexual y adolescent reproductive jóvenes y en las Américas: implicaciones en y political programs. PAHO, 2003. 38p. [ Links ]
32. Vieira LM, Saes SO, Doria AAB, Goldberg, TBL. Reflections on contraception in adolescence in Brazil. Recife: Journal of Maternal and Child Health. 2006, 6 (1): 135-40. [ Links ]
33. FC Silva. Emergency contraception: knowledge, experience and opinion of health care students from four universities. Federal Brazil. São Paulo, 2009.Thesis (MA) - University of Sao Paulo.109 p. [ Links ]
34. Raine & T et al., Direct Access to Emergency Contraception Through Pharmacies and Effect on Unintended Pregnancy and STIs - a randomized controlled trial. Journal of the American Medical Association. 2005, 293 (1): 54-62. [ Links ]
35. Belzer, M & col. Advanced Supply of Emergency Contraception for Adolescent Mothers Increased Utilization or without Reducing Condom Contraception Primary Use. Journal of Adolescent Health. 2003, 32 (2): 122-3. [ Links ]
36. Bastos S, Bonfim JRA, Kalckmann S, Figueiredo R. Fernandes MEL. Prevention of sexually transmitted diseases and seeking emergency contraception in pharmacies and drugstores of São Paulo. London: Health and Society Magazine. 2009, 18 (4): 787-99. [ Links ]
37. IMS Health. Data from national survey of pharmaceutical sales, 2009 [accessed October 2011]. Available in http://www.redece.org [ Links ]
38. Castro JF, Rodrigues VMCP. Knowledge and attitudes of young people in the face of emergency contraception. New York: Journal of the School of Nursing [online]. 2009, 43 (4): 889-94. [ Links ]
39. MSP Araújo, Costa LOBF. Sexual behavior and emergency contraception among teenagers in public schools in Pernambuco, Brazil. Rio de Janeiro: Journal of Public Health (online). 2009, 25 (3): 551-562. [ Links ]
 Corresponding author:
Corresponding author:
reginafigueiredo@isaude.sp.gov.br
Manuscript submitted Feb 15 2011
Accepted for publication Dec 29 2011.

{kind=link}
{kind=link}