










Serviços Personalizados
artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282
Rev. bras. crescimento desenvolv. hum. vol.22 no.2 São Paulo 2012
ORIGINAL RESEARCH
Obtained and predicted values for maximal respiratory pressures of Brazilian children
Rafaela Andrade do Nascimento; Tania Fernandes Campos; Janiara Borges da Costa Melo; Raíssa de Oliveira Borja; Diana Amélia de Freitas; Karla Morganna Pereira Pinto de Mendonça*
Departamento de Fisioterapia, Campus Universitário. Avenida Senador Salgado Filho, 3000. Lagoa Nova, Natal, RN, Brasil
ABSTRACT
OBJECTIVE: to compare the values obtained from the evaluation of maximal inspiratory pressure and maximal expiratory pressure in a sample of Brazilian children with reference values for maximal respiratory pressures proposed by Szeinberg et al., Domènech-Clar et al., and with the predicted equations proposed by Wilson et al.
METHODS: observational, cross-sectional study. We assessed 40 female and male children from public schools, aged 7 to 10 years. Personal and anthropometric data were collected in addition to the measurement of maximal respiratory pressures by an MV150 analog manometer (Wika®).
RESULTS: mean maximal inspiratory pressure was -61,50 ± 18,14 cmH2O and -70,55 ± 17,94 cmH2O for girls and boys, respectively. Mean maximal expiratory pressure was 77,40 ± 19,00 cmH2O and 77,40 ± 19,04 cmH2O for girls and boys, respectively.
CONCLUSION: the values of maximal respiratory pressures obtained by this study in a sample of Brazilian children aged 7 to 10 years did not differ from those proposed by Domènech-Clar et al. However the reference values provided by Szeinberg et al. overestimated the values of maximal respiratory pressures of the children evaluated. The equations proposed by Wilson et al. were successful in predicting the values of maximal respiratory pressures in the population studied.
Key words: muscle strength; respiratory muscles; evaluation; reference values; child.
INTRODUCTION
Respiratory muscle strength is an important parameter in clinical practice since these muscles are primarily responsible for the work of breathing, that is, performance in ventilatory mechanics1. There are several methods of assessing respiratory muscle strength, among which pressure evaluation, the most widely cited in the literature.
Measuring maximal inspiratory and expiratory pressure (PImax and PEmax, respectively) is a relatively simple, quick and non-invasive test2,3. A number of authors have assessed respiratory muscle strength via maximal respiratory pressures in healthy individuals of different ages and ethnicities, in order to propose reference values or predictive equations4,7.
In pediatrics, neuromuscular disease and obstructive or restrictive respiratory disorders can compromise the strength of respiratory muscles as well as hampering quality of life among children8,9. Thus, measuring maximal respiratory pressures is important since, in association with possible respiratory muscle impairment, there is a continuous process of maturation and growth characteristic of the respiratory system in this phase of life10,11. In order to determine maximal inspiratory and expiratory pressure, values obtained must be compared with available reference values to establish the existence or not of respiratory muscle weakness.
Wilson et al.12 provided predictive equations for maximal respiratory pressure in children and adolescents from 7 to 17 years old. Szeinberg et al.13 proposed predictive equations and normal values for children, adolescents and young adults aged between 8 and 40 years. Domènech-Clar et al.14 established reference values for PImax and PEmax in the 8 to 17 year-old age range.
Nevertheless, there is insufficient supporting research concerning the assessment of respiratory muscle strength in Brazilian children, as well as a shortage of studies identifying predictive and normal values for this age group. As such, the present study aimed to compare normal maximal respiratory pressure values (PImax and PEmax) recorded in a sample of healthy children aged 7 to 10 years from the city of Natal, Brazil with those proposed by Szeinberg et al.13 and Domènech-Clar et al.14, in addition to determining whether the equations provided by Wilson et al.12 apply to this population.
METHODS
This is a descriptive, cross-sectional study, approved by the Research Ethics Committee of the Federal University of Rio Grande do Norte (UFRN) under protocol nº 317/2009, in accordance with resolution 196/96 of the National Health Council.
Subject selection and inclusion criteria
Participants were children of both sexes between 7 and 10 years old, enrolled in public schools in the city of Natal. The maximum age limit was defined according to article 2 of the Children and Adolescents Act15, which considers an individual a child until the age of 12. The minimum age was established based on the ability to understand and correctly execute the maneuvers12.
Four schools from the city of Natal were randomly selected, in accordance with the age range studied, from a list of state schools provided by the State Health Secretariat - Rio Grande do Norte state. Following approval by the 1st Regional Board of Education - DIRED, the principals of the chosen schools were contacted to request consent. In each participating school, 40 children were selected (10 from each age group, 7-8-9-10) and given an informed consent form (in appropriate language, for their parents or guardians), containing explanations of the objectives, importance and procedures involved in the study, as well as some recommendations for the assessment day, such as not engaging in strenuous physical activity the previous day, wearing comfortable clothes and not consuming a substantial meal at least 3 hours prior to evaluation procedures. An additional questionnaire was also presented containing questions regarding the child's health status, to be completed by parents or guardians.
Once written informed consent was received and the completed questionnaires returned, the latter were analyzed and data collection procedures were conducted on those eligible to participate. It is important to note that even with parental consent, children who refused to participate were not obliged to do so.
Exclusion criteria
Children excluded from the sample were those diagnosed with chronic lung disease or neuromuscular disorders; evident chest deformity; submitted to prior chest surgery; recent trauma of the upper airways, chest or abdomen; history of smoking; acute middle ear problems; abdominal hernia; glaucoma or retinal detachment; neurological and/or cognitive impairment; using medication that might compromise muscle strength; underweight or overweight/obese2. The percentile was used to determine their relative position among children of the same age and sex in relation to body mass index. Thus, individuals with a BMI percentile lower than five and greater than 85 were excluded due to classification as underweight and overweight or obese, respectively16.
Study sample
Among the 160 randomly selected children, 46 were considered eligible for the study. Of these, 6 were excluded for inability to correctly perform the manometer procedures. The final sample of the present study consisted of 40 children; 20 boys and 20 girls.
Identifying and storing data
A previously standardized evaluation chart was used to collect personal and anthropometric data, as well as information obtained in the respiratory assessment of maximal inspiratory and expiratory pressures.
Body weight was established on a QIE - 2003B Personal Scale balance (Batiki®, Brazil), with a 150 kilogram limit. The subject was asked to remove their shoes and position themselves on the scale long enough to allow verification of the value provided by the instrument.
Height was determined using a 150 cm measuring tape fixed onto a wall 50 cm above the ground. Children remained erect, with their head in a neutral position and their back and heels pressed against the wall. The measurement was taken from the floor to the top of the head.
Maximal respiratory pressure
Maximal respiratory pressure was evaluated using an MV150 analogue manometer (Wika®, Brazil), calibrated from -150 to +150 cmH2O, with a 35 cm long and 0.5 cm wide tube attached to a rigid, flat plastic mouthpiece. This contained a 1mm wide hole on its upper surface to prevent glottal closure combined with the action of facial muscles from producing additional pressure that may interfere with measurement results2. In accordance with Black and Hyatt4, PEmax assessment required participants to breathe in until reaching total lung capacity and then perform a maximal respiratory effort until residual volume. For PImax evaluation, subjects breathed out until residual volume and then executed an inspiratory effort until total lung capacity. Children were instructed on how to correctly carry out the test.
PImax and PEmax values were obtained via pressure generated in the mouth when participants executed a maximal effort against an occluded airway. All pressures were measured with children sitting in a comfortable position and no restrictions as to lung expansion. In order to prevent air leakage, a nose clip was used with adequate adjustment of the lips around the mouthpiece, which was sterilized with a 1% sodium hypochlorite enzymatic detergent.
The maneuver was repeated at least three times to obtain two reproducible maneuvers (where values between the two differed by no more than 10% of the highest value)2 and pressures were sustained for at least one second4. During PEmax testing, the lips and cheeks of participants were compressed to prevent the generation of extra pressure by the buccinator muscle and prevent air leakage from the mouthpiece17. A time interval of approximately one minute was applied between efforts12. Since this was an effort-dependent test, verbal encouragement was given during the procedure. All resulting values were recorded, but only the highest was considered. Maneuvers were repeated a maximum of seven times14.
Participants themselves randomly selected which pressure (PImax or PEmax) would be measured first and an interval of five minutes was adopted between Pimax and PEmax assessment2.
Statistical analysis
Data were analyzed using SPSS 15.0 software (Statistical Package for the Social Science), adopting a significance level of 5%. Descriptive statistics were performed to characterize the sample. The Shapiro-Wilk test identified normal data distribution, followed by the unpaired Student's t-test to establish the existence of differences between the mean Pimax and PEmax values obtained and those recorded by Szeinberg et al.13 and Domènech-Clar et al.14. The regression equation proposed by Wilson et al.12 was used to calculate the PImax and PEmax values of participants and the paired Student's t-test was applied to compare these values with those obtained in the present study.
RESULTS
The means recorded in the study sample for the variables age, weight, height and percentile were 8.40 ± 1.15 years; 32.18 ± 9.47 kg; 1.32 ± 0.08 m; percentile of 63.65 ± 21.03, respectively. For PImax, the mean observed was -63.97 ± -21.51 cmH2O and for PEmax, 69.45 ± 20.04 cmH2O. The mean values obtained for anthropometric data and maximal respiratory pressure distributed by sex, for all children assessed, are shown in table 1.

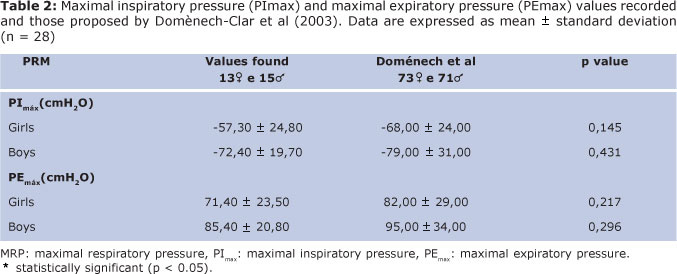
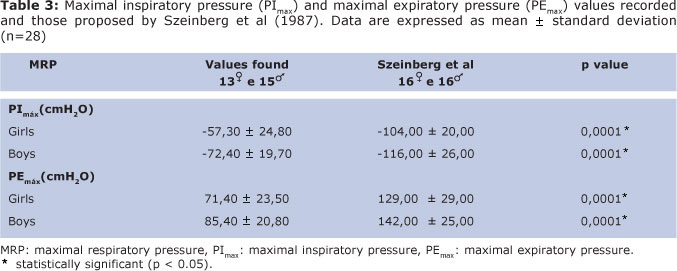
Tables 2 and 3 show the PImax and PEmax values recorded in this study for 8 to 10 year-olds and the normal values proposed by Doménech-Clar et al.14 and Szeinberg et al.13, respectively, for the same age range. The unpaired Student's t-test for independent samples found no significant difference between these data and those obtained by Doménech-Clar et al.14 for both sexes. However, when compared with the study by Szeinberg et al.13, a significant difference was observed for both boys and girls. Data were presented separately and expressed as centimeters of water (cmH2O).
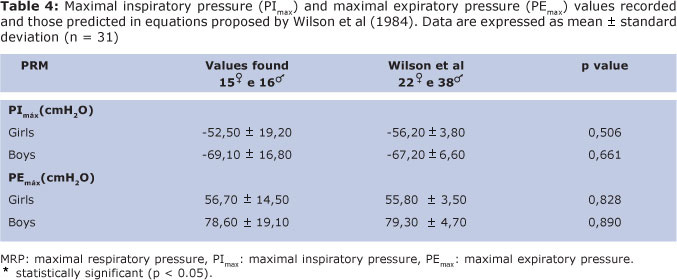
The predictive equations of normal values provided by Wilson et al.12, for boys and girls from 7-17 years-old, enabled the prediction of maximal respiratory pressures for the 7 to 9 year-old age group and their comparison with results obtained. Table 4 depicts the comparative analysis of the maximal inspiratory and expiratory pressures recorded and those predicted by Wilson et al.12
DISCUSSION
The normal values observed in this study when evaluating maximal respiratory pressure in 7 to 10 year-old Brazilian children were different when compared with reference values suggested by Szeinberg et al.13. However, measurements obtained here were similar when compared with those reported by Domènech-Clar et al.14. It is important to underscore that this comparative analysis was conducted between similar age groups.
Domènech-Clar et al.14 proposed reference values when assessing maximal respiratory pressure in 392 children and adolescents aged between 8 and 17 years. The sample was subdivided into the following age groups: 8-10; 11-14; 15-17 years.
Comparative analysis of maximal respiratory pressures in the 8 to 10 year-olds comprising the study sample with reference values provided by Domènech-Clar et al.14 for the subgroup in the same age range showed no statistical difference. Moreover, these normal values may be appropriate for the population of Brazilian children studied. Several methodological aspects of these two studies were similar (maneuvers were carried out in the same position, using a noise clip and the same lung volume and time periods for sustaining maximal pressures). Comparative analysis of the values recorded in both investigations also identified similarity with research by Domènech-Clar et al.14, in that maximal respiratory pressures increased with age and are greater in boys than girls. Previous studies corroborate these findings6,18,19. Zapletal et al.20 reported that lung elasticity is not constant between the ages of 6 and 17 years and increases with rising weight, age and body surface area. Loosli and Potter21 also noted that the increase in lung elastic fibers, which occurs from the post-natal to adult phases, may explain the evidence of higher maximal respiratory pressures with increased age.
Szeinberg et al.13 investigated respiratory muscle strength in 270 children, also subdivided into different age groups. The reference values proposed by these authors and comparatively analyzed against findings from the present study were those obtained for 8 to 10 year-olds. In contrast with the applicability of values proposed by Domènech-Clar et al14 for the population represented in this study, the normal values suggested by Szeinberg et al.13 overestimated respiratory muscle strength and therefore do not seem appropriate for Brazilian children of both sexes in the same age range.
One-third of the present study sample of children aged between 8 and 10 years were 10 year-olds. This information is not provided in the investigation conducted by Szeinberg et al.13 and as such, the presumption that values proposed by these authors are inadequate may be because the mean age recorded was higher that that of children assessed in this study. This hypothesis is supported by several authors who associate increased age with greater respiratory muscle strength14,18,19.
Szeinberg et al.13 reported that a portion of some of the 10 year-olds studied engaged in physical activity, but provide no details as to the extent of this activity or whether children in other age groups were also physically active. In a longitudinal study of 44 boys aged from 11 to 17 years, Matecki et al.19 found that physical activity may have a positive effect on maximal respiratory pressures (all subjects in this investigation participated in physical activity). Given that the amount of physical activity was not taken into account in the present study, this may explain the difference observed when comparing the two studies.
Recent research observed that maximal respiratory pressure can vary according to the ethnicity of the population studied. Moreover, normal values and predictive equations proposed for individuals from one country may differ from those suggested for populations from other countries22,23. Parreira et al.24 also noted that normal and predictive values for PImax and PEmax can differ between individuals of the same country.
Normal values and those predicted using equations proposed by Wilson et al.12 have been widely cited by a number of researchers since their publication. The authors subdivided a sample of 235 children and adolescents into three age groups, the first of which comprised 60 children aged from 7 to 9 years. In order to compare the findings of Wilson et al12 with measurements recorded in the present study, normal PImax and PEmax values were predicted for 7 to 9 year-old children using the equations provided by these authors. Results show that although the authors suggested the same equations for predicting maximal respiratory pressure in children between the ages of 7 and 17 years, these equations appear to be suitable for the population represented in this study. Conclusions drawn from the findings of both studies involving large samples may provide an explanation for the lack of significant differences between values predicted by Wilson et al.12 and those found in this investigation25,26.
Carpenter et al.25 analyzed respiratory muscle strength using PImax and reported that although their large sample exhibited sufficient power to identify associations with sex, age, education, race, health status and other factors, these correlations were not necessarily clinically significant. Furthermore, due to the study design, the authors were unable to predict whether race is a clear factor. Windisch et al.26 evaluated 533 healthy subjects between 10 and 90 years old from different regions and concluded that demographic and anthropometric factors showed little significance, despite the unexplained variability between subjects.
Maximal respiratory pressure observed in this study identified greater respiratory muscle strength in boys, corroborated by previous research reporting similar results12,14,27,28. This same behavior has been recorded in investigations assessing respiratory muscle strength among adolescents and adults1,4,14,18,29,30. Schrader et al.18 reported that this increase in strength occurs as the child grows, although it is seen to a lesser extent in girls, where values tend to stabilize after the age of 16 years. The authors also observed that boys display greater respiratory muscle strength and are therefore capable of generating higher pressures for all lung volumes when compared to girls. These same authors found that the difference between the sexes is basically related to the passage of air/lung dimensions ratio, with boys achieving better elastic recoil and greater pressure in upper airway distension, thereby generating greater expiratory flow; whereas girls display lower residual volumes and total lung capacity, producing lower pressures.
The lack of available studies to support findings for children at the younger end of the age range assessed may be considered a limitation of this study. Results of a multicentric study might also enable a more detailed analysis of the influence of sociodemographic factors on respiratory muscle strength in different populations.
CONCLUSION
The maximal respiratory pressures obtained in the present study for a sample of 7 to 10 year-old Brazilian children did not differ from those proposed by Domènech-Clar et al.14. However, reference values provided by Szeinberg et al13 overestimated maximal respiratory pressure measurements recorded for the children evaluated. In addition, the equations proposed by Wilson et al.12 were capable of predicting values for maximal respiratory pressure in the population studied. Given the lack of available reference values for maximal respiratory pressures in Brazilian children, this study may be considered an important tool to guide practitioners and/or researchers as to suitable parameters for assessing respiratory muscle strength in this population.
REFERENCES
1. Neder JA, Andreoni S, Lerario MC, Nery LE. Reference values for lung function tests. II. Maximal respiratory pressures and voluntary ventilation. Braz J Med Biol Res. 1999;32(6):719-27. [ Links ]
2. Souza RB. Pressões respiratórias estáticas máximas. J Pneumol. 2002;28 Suppl 3: S155-65. [ Links ]
3. Vasconcellos JA, Britto RR, Lopes RB. Avaliação da musculatura respiratória. In: Brittom AR, Brant TC, Parreira VF. Recursos manuais e instrumentais em fisioterapia respiratória. Barueri: Manole; 2009. p. 11-22. [ Links ]
4. Black LF, Hyatt RE. Maximal respiratory pressures: normal values and relationship to age and sex. Am Rev Respir Dis. 1969;99: 696-702. [ Links ]
5. Costa D, Gonçalves HA, Lima LP, Ike D, Cancelliero KM, Montebelo MIL. Novos valores de referência para pressões respiratórias máximas na população brasileira. J Bras Pneumol. 2010;36(3):306-12. [ Links ]
6. Tomalak W, Pogorzelski A, Prusak J. Normal values for maximal static inspiratory and expiratory pressures in healthy children. Pediatr Pulmonol. 2002;34(1):42-6. [ Links ]
7. Simões RP, Deus AP, Auad MA, Dionísio J, Mazzonetto M, Borghi-Silva A. Pressões respiratórias máximas em indivíduos saudáveis sedentários de 20 a 89 anos da região central do Estado de São Paulo. Rev Bras Fisioter. 2010;14(1):60-7. [ Links ]
8. Trinca MA, Bicudo IMP, Pelicione MCF. A interferência da asma no cotidiano das crianças. Rev Bras Crescimento Desenvolv Hum. 2011;21(1):70-84. [ Links ]
9. Costa ASM, Britto MCA, Nóbrega SM, Vasconcelos MGL, Lima LS. Vivências de familiares de crianças e adolescentes com fibrose cística. Rev Bras Crescimento Desenvolv Hum. 2010; 20(2):217-27. [ Links ]
10. Prasad SA, Main E, Dodd ME. Finding consensus on the physiotherapy management of asymptomatic infants with cystic fibrosis. Pediatr Pulmonol. 2008; 43(3): 236-44. [ Links ]
11. Stick S. The contribution of airway development to paediatric and adult lung disease. Thorax. 2000;55(7):587 - 94. [ Links ]
12. Wilson SH, Cooke NT, Edwards RTH, Spiro SG. Predicted normal values for maximal respiratory pressures in caucasian adults and children. Thorax. 1984;39(7): 535 - 8. [ Links ]
13. Szeinberg A, Marcotte JE, Roizin H, Mindorff C, England S, Tabachnik E et al. Normal values of maximal inspiratory and expiratory pressures with a portable apparatus in children, adolescents and young adults. Pediatr Pulmonol. 1987;3(4):255-8. [ Links ]
14. Domènech-Clar R, López-Andreu JA, Compte-Torrero L, De Diego-Damiá A, Macián-Gisbert V, Perpiñá-Tordera M et al. Maximal static respiratory pressures in children and adolescents. Pediatr Pulmonol. 2003; 35(2): 126-32. [ Links ]
15. Estatuto da criança e do adolescente. Disponível em: http://www.planalto.gov.br/ccivil/LEIS/L8069.htm. Acessado em: 22 jul. 2009. [ Links ]
16. World Health Organ. Physical status: the use and interpretation of anthropometry. Report of a World Health Organ Expert Committee. World Health Organ Tech Rep Ser. 1995; 854: 1-452. [ Links ]
17. Oliveira KMC, Macêdo TMF, Borja RO, Nascimento RA, Medeiros Filho WC, Campos TF et al. Força muscular respiratória e mobilidade torácica em crianças e adolescentes com leucemia aguda e escolares saudáveis. Rev Bras Cancerol. 2011; 57(4):511-7. [ Links ]
18. Schrader PC, Quanjer PH, Olievier IC. Respiratory muscle force and ventilatory function in adolescents. Eur Respir J. 1988;1(4):368 - 75. [ Links ]
19. Matecki S, Prioux J, Jaber S, Hayot M, Prefaut C, Ramonatxo M. Respiratory pressures in boys from 11-17 years old: a semilongitudinal study. Pediatr Pulmonol. 2003;35(5):368-74. [ Links ]
20. Zapletal A, Paul T, Samanek M. Pulmonary elasticity in children and adolescents. J Appl Physiol. 1976;40(6):953-61. [ Links ]
21. Loosli CG, Potter E I. Pre- and post-natal development of the respiratory portion of the human lung with special reference to the elastic fibers. Am Rev Respir Dis. 1959; 80 Suppl 1: S5-23. [ Links ]
22. Evans JA, Whitelaw WA. The assessment of maximal respiratory mouth pressures in adults. Respir Care. 2009;54(10):1348 - 59. [ Links ]
23. Leal AH, Hamasaki TA, Jamami M, Di Lorenzo VAP, Pessoa BV. Comparação entre valores de força muscular respiratória medidos e previstos por diferentes equações. Fisioter Pesqui. 2007;14(3):25-30. [ Links ]
24. Parreira VF, França DC, Zampa CC, Fonseca MM, Tomich GM, Britto RR. Pressões respiratórias máximas: valores encontrados e preditos em indivíduos saudáveis. Rev Bras Fisioter. 2007;11(5):361-8. [ Links ]
25. Carpenter MA, Tockman MS, Hutchinson RG, Davis CE, Heiss G. Demographic and anthropometric correlates of maximum inspiratory pressure: the atherosclerosis risk in communities study. Am J Respir Crit Care Med. 1999; 159(2): 415-22. [ Links ]
26. Windisch W, Hennings E, Sorichter S, Hamm H, Criée C.P. Peak or plateau maximal inspiratory mouth pressure: which is the best? Eur Respir J. 2004:23(5):708-13. [ Links ]
27. Gaultier C, Zinman R. Maximal static pressures in healthy children. Respir Physiol. 1983;51(1):45 - 61. [ Links ]
28. Wagener JS, Hibbert ME, Landau LI. Maximal respiratory pressures in children. Am Rev Respir Dis. 1984;129(5):873-5. [ Links ]
29. Smyth RJ, Chapman KR, Rebuck AS. Maximal inspiratory and expiratory pressures in adolescents: normal values. Chest. 1984;86(4):568 - 72. [ Links ]
30. Leech JA, Ghezzo H, Stevens D, Becklake MR. Respiratory pressures and function in young adults. Am Rev Respir Dis. 1983; 128(1):17-23. [ Links ]
 Corresponding author:
Corresponding author:
kmorganna@ufrnet.br
Manuscript submitted Jan 08 2011
Accepted for publication Aug 19 2011
This study is part of a dissertation entitled "Predictive equations for maximal respiratory pressures of Brazilian children", held in Natal at the Federal University of Rio Grande do Norte (UFRN) - Graduate Program in Physical Therapy in 2011.

{kind=link}
{kind=link}
{kind=link}