










Serviços Personalizados
artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282
Rev. bras. crescimento desenvolv. hum. vol.22 no.3 São Paulo 2012
ORIGINAL RESEARCH
A 10-month anthropometric and bioimpedance evaluation of a nutritional education program for 7 - to 14-year-old students
Rubens FeferbaumI; Claudio LeoneII; Rosemeire Casanova NogueiraIII; Patricia Neri CavalcantiIII; Eduardo Blanco CardosoIV; Monica Allende SerraV
IMD PhD - Children's Institute and Department of Pediatric Medicine. Faculty of Medicine of University of São Paulo
IIMD PhD - Department of Maternal and Infant Health, Faculty of Public Health, University of São Paulo
IIIDietitian - Industrial Social Service of São Paulo State - Quality of Life Department Solidarity and Cultural and Social Development Fund of the State of São Paulo
IVMD PhD - Continuing Education Program of the Oswaldo Cruz Alemão Hospital (Unit Mooca), São Paulo
VPsychologist MSc PhD - Educational Advising. United Metropolitan Colleges - FMU
ABSTRACT
Over the past several decades, an increasing prevalence of excessive weight has been observed among children. Considering the importance of schools in promoting health, the implementation of individualized educational interventions in a school setting is necessary. The present study aimed to determine the influence of a nutritional education program in promoting the healthy eating habits and nutritional status of school-aged students. A total of 416 children and adolescents between 7 and 14 years of age who were enrolled in 2 complementary public schools were evaluated. A 10-month intervention in one of the schools was based on a nutritional education program targeting the students, legal guardians and school staff and involved substantial changes in the school meal menu. Weight, height, BMI, lean mass and body fat mass were evaluated in both the intervention (school 1) and the control (school 2) groups. At the beginning of the study, both school 1 and 2 exhibited a prevalence of overweight (34.0% and 28%, respectively) and obese students (16.9% and 10.4%, respectively); obesity was significantly reduced by the end of the study (p = 0.001). The growth of the students was considered normal for the age range in both schools, although it was slightly larger in school 1 (p = 0.04). Measurements of body composition, which were collected using bioelectrical impedance, indicated an increase in lean mass in both schools (p < 0.01) with an increase in body fat mass being observed only in school 2 (p = 0.01). These results, which are related to a significant reduction of the BMI, a change in bodily proportions and an increase in height growth for the students of school 1, indicate the beneficial aspects of the adopted diet.
Key words: school meals; nutritional education; body composition in children and adolescents.
INTRODUCTION
Nutritional transition, observed in developed countries since the 1970's, has progressively and increasingly affected emerging countries1,2 and influenced the rapidly growing prevalence of childhood obesity. Childhood obesity has been associated with several complications not only in childhood and adolescence but also in adulthood and is becoming a true worldwide epidemic3,4.
Several studies have shown a direct correlation between the duration of obesity and cardiovascular disease morbidity and mortality3. Therefore, the increasing observation of obesity in younger populations, including lower-income populations5, indicates a serious problem.
Unfortunately, educational campaigns based on providing additional nutritional information have failed to improve eating habits. Food consumption habits reveal motivations other than eating to remain healthy, and the following can be observed among the influencing factors on diet: individual preferences, acquired habits, schedule conditioning, financial resources, the degree of importance granted to satisfying the appetites or requirements of the various members of a given household, etc6. Ignoring these factors will condemn any campaign on nutritional education to failure. Until now, the government-adopted measures aimed at changing the eating habits of a population have been inefficient. Therefore, before devising methods on how to change those habits, one must strive to understand the nutritional behavior of the studied population; only then should one plan the most efficient approach to influence the study subjects of a given cultural and historic moment.
For Brazilian children between the ages of 7 to 14 years who consume at least one meal each school day, the relevance of the schools' role in promoting health and good eating habits may be fundamental, necessitating individualized interventions that are oriented toward avoiding or correcting nutritional disorders. The goal would be to ensure the normal development and growth of the target population.
To evaluate a nutritional education program devised for public school students with the goal of promoting healthy eating habits and to analyze and compare the resulting changes in the nutritional states of the students by anthropometric and bioimpedance (BIA).
METHODS
The present paper describes a prospective and controlled intervention study. The participants consisted of 416 children and adolescents between 7 and 14 years old of both genders who were enrolled in 2 complementary public schools located in the São Paulo city center.
The population of the study was divided into 2 groups: intervention (school 1: 213 students) and control (school 2: 203 students). No dietary or physical activity restrictions were imposed for inclusion in this study.
Over a period of 10 consecutive months, the nutritional intervention program in school 1 was structured by a permanent team of specialists in child nutritional education with effective participation by the educators of the school.
The program aimed to impart a greater awareness and consciousness to the students, school officials and educators by promoting healthy eating habits through meetings, lectures, culinary workshops, practical classes and recreational activities that were appropriate for the age group of the participants.
The intervention was modeled after Sesi-SP's Eat Well Program [Programa Alimente-se Bem do Sesi-SP]7. The menus followed the nutritional parameters of the aforementioned program.
Daily monitoring of the students was performed during mealtime by attempting new recipes and utilizing foods to their fullest extent (beyond what was normally consumed).
The Avanutri8 software was used to calculate the meal menus. The menus aimed to provide 40% to 50% of the uptake reference values of the following nutrients: the total energetic value (TEV), carbohydrates, proteins, fats, fiber9,10, calcium, iron and vitamins11.
Both of the schools provided a healthy meal on a daily basis; however, in the intervention school, the educational program aimed to offer a greater variety of vegetables and fruits, with the waste being calculated from the quantity of leftovers. The students were given more freedom to make choices regarding food quantity and variety because the meals were distributed in a "self-service" manner unlike in the control school, where meal distribution was performed using the portion system, and the students were unable to make a voluntary meal choice.
Weight and height measurements were performed on students from both schools at the beginning and end of the study using a standardized technique12,13.
The nutritional states of the students were evaluated using the Z-score for the weight/age, height/age, weight/height and BMI indices, according to the World Health Organization (WHO) reference values14 for each sex. The CDC 200015 referential was specifically chosen to calculate the weighted Z-scores. The students whose BMI was equal to or larger than 1 Z-score were considered to have excess weight (overweight and obese). Changes in the nutritional state were analyzed by calculating the changes in the Z-score values of the evaluated anthropometric parameters.
At previously designated times, the lean and body fat mass levels of the students were determined by BIA using the InBody 230 model by Biospace Co. Ltd., which is a Vector Impedance Apparatus, BIA System that uses 8 points of measurement; the lean and body fat mass values were compared sequentially.
The project was approved by the Ethics in Research Committee of Darcy Vargas Pediatric Hospital [Hospital Infantil Darcy Vargas]. The parents or legal guardians of the children completed and signed informed consent forms authorizing the children to participate in the study.
RESULTS
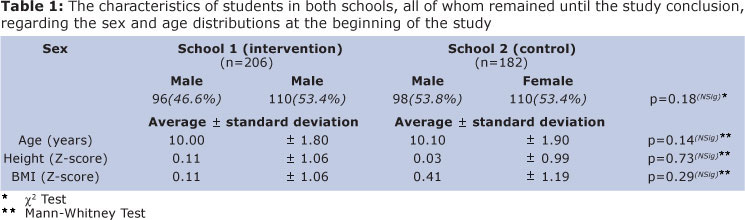
The data regarding the age, sex and initial conditions of the participants are summarized in Table 1; the sex and age distributions were similar in both schools. The average height and BMI values also failed to indicate any significant significant differences between the schools.
Table 1 indicates that the heights of the students were compatible with the WHO reference values14. The BMI values indicated that the students at both schools exhibited a tendency toward being overweight relative to the corresponding WHO reference.
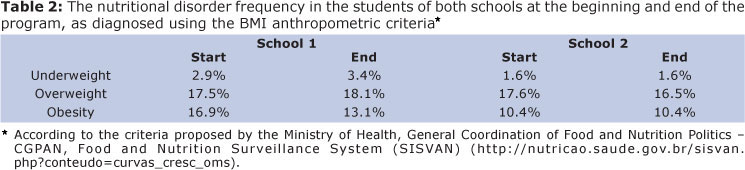
Overweight students were observed at both schools at the beginning of the study (Table 2).
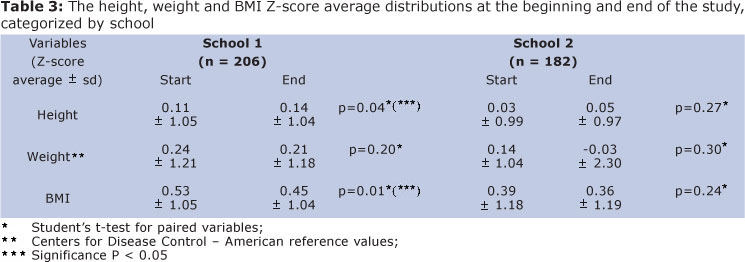
Table 3 summarizes the anthropometric results determined at the beginning and end of the study for both schools. An adequate growth relative to weight and height was observed, and the students of school 1 showed a statistically significant increase in height, which was not observed in school 2.
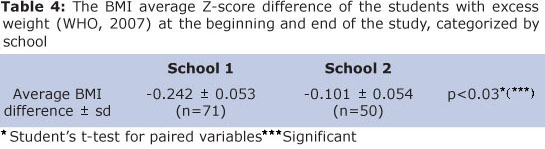
As outlined in Tables 3 and 4, a statistically significant reduction of the average BMI Z-score was observed in the students from school 1 relative to the initial BMI measurements.
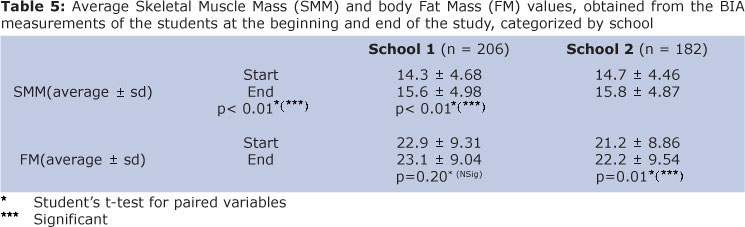
Table 5 indicated that the body compositions of the children, measured using BIA, showed a significant increase in muscle mass for both groups. The students from school 2 also showed an increase in body fat mass percentage; this increase was not observed among the students from school 1.
Concerning the eating habits of the students, a 30% increase in fruit and vegetable consumption was observed in school 1 with a 95% acceptance rate and a simultaneous 33% reduction in organic waste.
The families of the students were also observed to be involved in scheduled meetings, with the mobilization of all the legal guardians of the students.
DISCUSSION
The transition between childhood and adolescence is a crucial stage in human development, involving multiple physiological and psychological changes. Both of these types of change exert a direct influence on behavior, nutritional requirements and eating habits. Hormonal surges also play a role and result in important individual body composition changes. Consequently, the energy and nutrient requirements during this period are greater relative to other stages of life16,17.
The social and cultural factors that characterize the present time tend to affect dietary patterns and levels of physical activity. In addition, they are largely dependent upon the developing individual. Consequently, the individual may acquire maladaptive habits that typically persist throughout adulthood with a concomitant increase in health risks. It has been shown that the presence of nutritional disorders during childhood and adolescence can cause a remarkable increase in the probability of certain diseases, such as dyslipidemia/atherosclerosis18, eating disorders, obesity/diabetes19, osteoporosis20 and certain types of cancer21.
The current study arose from a set of problems associated with the Brazilian children population, stemming from inadequate eating habits in conjunction with changes in nutritional behavior and an absence of physical activity. The 2008/2009 Family Budget Survey22, undertaken by the Brazilian Institute of Geography and Statistics [Instituto Brasileiro de Geografia e Estatística], showed that 1 in 3 children between 5 and 9 years old was overweight according to the WHO guidelines23. The prevalence of overweight among young people between 10 and 19 years old increased from 3.7% in 1970 to 21.7% in 2009.
Although the problems associated with excess weight are not exclusive to Brazil, no comparable data on food and nutrient intake is available from the U.S.A. or from the countries of the European Union, despite the alarming data that have been observed. The absences of multicentric studies examining a large volume of individual cases and unified methodologies complicates the development of proposals centered on evidence-based health promotion. Moreover, quantitative evaluation of the nutritional state of children and adolescents is often difficult because no succinct definition of child obesity exists. However, in an attempt to contemplate and unify all of these aspects, the WHO14 advocates using the 85th and 95th percentiles (P85 and P95) of growth curves as threshold points for the diagnosis of obesity.
Using the BMI in statistically homogeneous populations (Table 1) as a quantitative indicator of the nutritional state, the average BMI value measured in both schools tended toward overweight students and was approximately 0.5 standard deviation (sd) above the WHO-advocated median14. This finding was consistent with observations of school-aged children in Brazil and is likely a result of the ongoing nutritional transition and a reflection of the worldwide ongoing trend that was first observed in industrialized countries in the early 1980s1,24.
At the beginning of the study, overweight frequencies of 34.4% and 28.0% and obesity frequencies of 16.9% and 10.4% were observed for schools 1 and 2, respectively (Table 2). Although the measurements collected at the end of the study indicated a trend toward reduction, a statistically significant reduction of these proportions was not observed. However, when considering the obese children from school 1, the degree of obesity was reduced at the end of the intervention period. The fact that this result did not extend to the proportion of overweight children may theoretically be attributed to the short duration of the intervention. One should also emphasize that the intervention did produce changes in the anthropometric parameters; in particular, there was a significant reduction in the BMI average Z-scores of the obese children (Tables 3 and 4), who presumably had more room to improve their nutritional habits.
There are several published random clinical studies on children and adolescent obesity prevention in school environments (each with important methodology limitations), several reviews25-30 and a small number of clinical practice guides31-33. Moreover, these studies display an important level of heterogeneity concerning the strategies employed (diet and physical activity), place of intervention (school, work and home) and the recruitment of families during the process. Because of this heterogeneity, it is ultimately difficult to establish an obvious cause-and-effect association from the findings of these studies, even when the duration of the intervention is not considered.
Satisfactory results can be observed among the dietary interventions for obesity prevention that focused particularly on children and adolescents and lasted for 1 year or more, such as Planet Health34, which included 1,295 students from 11 to 12 years old in 10 schools in the United States. The intervention focused on dietary changes and a reduction of sedentary behaviors and produced a significant decrease in obesity in the intervention group, whereas the obesity levels remained stable in the control group. However, the APPLES (Active Programme Promoting Lifestyle in Schools) study, which was developed in England and involved 634 students from 7 to 11 years old for approximately 1 year, revealed no statistically significant changes in the BMI values35. Longer nutritional interventions, up to 2 years, were also revealed to be ineffective36.
Of the few existing studies performed on children and adolescents that lasted less than 1 year, a study conducted in Chile that was carried out over a 6-month period must be discussed. This study aimed to improve nutritional education and promote physical activity among 2,375 children enrolled in primary schools37. The final evaluation of the intervention revealed no significant differences in the BMI between the intervention and control groups.
These results showed that the success of an intervention did not depend on the duration of the intervention "per se," in spite of standardized diets and regular physical activity. The results depended on the facilitating factors rather than on the individuals themselves.
A likely facilitating factor to reduce BMI in overweight children over a relatively short 10-month period, as in the present study, lies in the awareness process, which involves the students, their parents and educators. Various interventions may have a positive (albeit small) effect on fruit and vegetable consumption when applied equally to both genders. The biggest effects were observed on interventions that involved the parents of the children and the professors who directly addressed them38.
Regarding physical activity, not all of the programs developed to treat overweight and obese children and adolescents have been effective in reducing BMI39. However, it is well known that physical activity may temporarily reduce the body fat mass percentage40,41 and consequently, the presence of cardiovascular disease risk factors42,43.
In the present study, children with previous organic diseases or special dietary requirements were not included in the study. All of the participants showed good physical performance and overall conditioning. Therefore, neither complementary physical activity nor specific dietary restrictions were applied.
One of the differentiating factors of the present study when compared to previous studies was the fact that the students were allowed to choose their meals according to their individual preferences and their reported experience of good "taste." As a result, their meals were more appealing, and they were allowed to practice the pleasure of meal autonomy. The increase in variety, the diversity of appetites contemplated and the variety of healthy and affordable food made available to both the school and family environments enabled the students enrolled in school 1 to choose from various appetizing options, which were then partially replicated in their households by involved parents. Therefore, it appears that for an intervention to become effective, one should not focus solely on the nutrients necessary for a health/disease balance but rather focus on the pleasure derived from food. This approach enables a larger preference for the consumption of in-season fruits, greens and vegetables, leading to an integral uptake of all of their components, and creates a situation in which the primary consumers, the students, are more involved along with their families.
Student growth was considered normal for the age range; however, growth was significantly greater in the intervention school (school 1; Table 3). The meals offered to the school 1 students were almost certainly a positive influencing factor toward achievement of the height standard. In this regard, correcting the nutritional habits of children through their adoption of a well-balanced diet will ensure their normal development in the majority of cases.
Although weight is not regarded as an important parameter to assess the nutritional state of children in this age range (it is not typically considered for children over the age of 5),44 the obtained data showed no statistically significant variations in the weight averages recorded for either school (Table 3). However, the BMI values calculated from the BIA showed an increase in lean mass among both groups of students, but the body fat mass values only showed an increase in the control school (Table 5). The absence of a body fat mass increase in the children enrolled in the intervention school reinforced the positive effect of the intervention. These results, in conjunction with the significant decrease in the BMI, changes in body proportion and height increase, validate the benefits of the new dietary habits.
Considering the relatively short duration and reduced number of schools (2) of the experiment, these results indicate that new clinical trials should be continuously developed. These studies will enable researchers to develop and perfect a more effective intervention method to prevent childhood excess weight gain and obesity. Such studies will also enable researchers to test the efficiency of brief interventions in primary care and school meal preparation with the goal of establishing healthy meal habits. It is important to emphasize that for children and adolescents to change their lifestyles through nutritional education in conjunction with physical education, one must intervene at an early age and in a continuous manner. Without adopting new dietary measures and lifestyle changes in both children and their families, the chances of successfully decreasing the morbidity from excess weight gain and obesity at the beginning of adulthood will certainly be compromised.
The results obtained in the present work initiated the Food Consciousness Program [Programa Consciência Alimentar], which was applied to the Municipal School Network of the State of São Paulo [Rede Municipal Escolar do Estado de São Paulo]45,46.
ACKNOWLEDGMENTS
Tereza Toshiko Watanabe (in memoriam): Nutritional and Social Responsibility Division of Industrial Social Service - São Paulo Regional Department [Divisão de Nutrição e Responsabilidade Social do Serviço Social da Indústria (SESI) - Departamento Regional de São Paulo]; Luiz Roberto Barradas Barata (in memoriam): São Paulo State Secretary of Health [Secretaria da Saúde do Estado de São Paulo-SP]; and Sergio Antonio Bastos Sarrubbo: Darcy Vargas Pediatric Hospital [Hospital Infantil Darcy Vargas], São Paulo-SP.
REFERENCES
1. Popkin BM. The obesity epidemic is a worldwide phenomenon. Nutr Rev. 1998;56(4):106-14. [ Links ]
2. Popkin BM. The nutrition transition and its health implications in lower income countries. Public Health Nutr. 1998;1(1):5-21. [ Links ]
3. Oliveira CL, Fisberg M. Obesidade na infância e adolescência - Uma verdadeira epidemia [Childhood and adolescence obesity - a real epidemic]. Arq Bras Endocrinol Metab. 2003;47(2):107-8. [ Links ]
4. Mello ED, Luft VC, Meyer F. Obesidade infantil: como poderemos ser eficazes? [Childhood obesity: toward effectiveness?] J Pediatr (Rio J). 2004;80(3):173-82. [ Links ]
5. Nascimento VG, Schoeps DO, Souza SB, Souza JMP, Leone C. Risk of overweight and obesity in preschoolers attending private and philanthropic schools. Rev Assoc Med Bras. 2011;57(6):643-7. [ Links ]
6. McDougall, P. Teenagers and nutrition: assessing the levels of knowledge. Health Visit. 2004;71(2):62-4. [ Links ]
7. Serviço Social da Indústria (SESI), Departamento Regional de São Paulo. Alimente-se bem: 200 receitas econômicas e nutritivas. 12ª ed. [Industrial Social Service (SESI), São Paulo Regional Department. Eat well: 200 inexpensive and nourishing recipes. 12th ed]. São Paulo: SESI-SP; 2008. [ Links ]
8. Santana RI. Avanutri sostware de avaliação e prescrição nutricional [Avanutri nutritional evaluation and prescription software]. Rio de Janeiro version 4.0; 2009. [ Links ]
9. FAO/WHO/UNU. Human energy requirements. Report of a joint FAO/WHO/UNU expert consultation. Rome: Food and Agriculture Organization; 2001. [ Links ]
10. World Health Organization/Food and Agriculture Organization. Joint report of expert consultation. Diet, nutrition and the prevention of chronic diseases. Geneva: World Health Organization; 2003. (WHO Technical Report Series; 916). [ Links ]
11. Institute of Medicine. Dietary reference intake for energy, carbohydrate, fiber, fat, body fat acids, cholesterol, protein, and amino acids. Washington, DC: National Academy Press; 2005. [ Links ]
12. Frisancho R. Anthropometric standards for the assessment of growth and nutritional status. Ann Arbor: The University of Michigan Press; 1999. [ Links ]
13. Organización Panamericana de la Salud. Conjunto de acciones para la reducción multifactorial de enfermedades no transmisibles [Actions for multifactorial non-transmissible disease reduction], Washington, DC: OPS; 1997. [ Links ]
14. WHO. Growth reference data for 5-19 years, 2007. Available from: http://www.who.int/growthref/en/. [ Links ]
15. National Center for Health Statistics, Centers for Disease Control and Prevention [homepage on the Internet]. Atlanta, GA: Department of Health and Human Services; [updated May 20, 2004; cited 2004 November 4]. 2000 CDC Growth Charts: United States; [about 3 screens]. Available from: http://www.cdc.gov/growthcharts. [ Links ]
16. FAO/WHO/ONU. Expert consultation report. Energy and protein requirements. Geneva: WHO; 1985. (Technical Report Series; 724). [ Links ]
17. Southon S, Wright AJA, Finglas PM, Bailey AH, Loughridge JM, Walker AD. Dietary intake and micronutrient status of adolescents: effect of vitamin and trace element supplementation on indices of status and performance of verbal and nonverbal intelligence. Br J Nutr. 1994;71(6):897-987. [ Links ]
18. Csábi G, Török K, Jeges S, Molnár D. Presence of metabolic cardiovascular syndrome in obese children. Eur J Pediatr. 2000;159(1-2):91-4. [ Links ]
19. Marcos A, Montero A, López-Varela S, Morandé G. Eating disorders (obesity, anorexia and bulimia), immunity and infection. In: Tontisirin K, Susking R, editors. Nutrition, immunity and infection disease in infants and children. 45th Nestle Nutrition Workshop. Bangkok, Thailand. Vevey. Nestle Nutrition Services. 2001;45:243-79. [ Links ]
20. Molgaard C, Thomsen BL, Michaelsen KF. Influence of weight, age and puberty on bone mineral content in healthy children and adolescents. Acta Paediatr. 1998;87(5):494-9. [ Links ]
21. Frankel S, Gunnell DJ, Peters TJ, Maynard M, Davey Smith G. Childhood energy intake and adult mortality from cancer: the Boyd Orr Cohort Study. BMJ. 1998;316(7130):499-504. [ Links ]
22. Pesquisa de orçamentos familiares 2008-2009. Informe. Quarto Fórum SIPD [2008-2009 family budget survey]. Report. Fourth SIPD Forum. Rio de Janeiro, 2008. p.24. [ Links ]
23. WHO Multicentre Growth Reference Study Group. Breastfeeding in the WHO Multicentre Reference Study. Acta Paediatr. 2006;(Suppl 450):16-26. [ Links ]
24. Flegal KM, Carroll MD, Ogden CL, Johnson CL. Prevalence and trends in obesity among US adults, 1999-2000. JAMA. 2002;288(14):1723-7. [ Links ]
25. Flynn MA, McNeil DA, Maloff B, Mutasingwa D, Wu M, Ford C, et al. Reducing obesity and related chronic disease risk in children and youth: a synthesis of evidence with 'best practice' recommendations. Obes Rev. 2006;7(Suppl 1):7-66. [ Links ]
26. Connelly JB, Duaso MJ, Butler G. A systematic review of controlled trials of interventions to prevent childhood obesity and overweight: a realistic synthesis of the evidence. Public Health. 2007;121(7):510-7. [ Links ]
27. Brown T, Summerbell C. Systematic review of school-based interventions that focus on changing dietary intake and physical activity levels to prevent childhood obesity: an update to the obesity guidance produced by the National Institute of Health and Clinical Excellence. Obes Rev. 2009;10(1):110-41. [ Links ]
28. Kamath CC, Vickers KS, Ehrlich A, McGovern L, Johnson J, Singhal V et al. Behavioral interventions to prevent childhood obesity. A systematic review and meta-analyses of randomized trials. J Clin Endocrinol Metab. 2008;93 (12):4606-15. [ Links ]
29. Shaya FT, Flores D, Gbarayor CM, Wang J. School-based obesity interventions: a literature review. J Sch Health. 2008;78(4):189-96. [ Links ]
30. Wofford LG. Systematic review of childhood obesity prevention. J Pediatr Nurs. 2008;23(1):5-19. [ Links ]
31. National Institute for Health and Clinical Excellence. Obesity. Guidance on the prevention, identification, assessment and management of overweight and obesity in adults and children. NICE Clinical Guideline 43. December 2006. [ Links ]
32. Lau DC, Douketis JD, Morrison KM, Hramiak IM, Sharma AM, Ur E. 2006 Canadian clinical practice guidelines on the management and prevention of obesity in adults and children. CMAJ. 2007;176(8 Suppl):1-13. [ Links ]
33. Han JC, Lawlor DA, Kimm SYS. Childhood obesity. Progress and challenges. Lancet. 2010;375(9727):1737-48. [ Links ]
34. Gortmaker SL, Peterson K, Wiecha J, Sobal AM, Dixit S, Fox MK et al. Reducing obesity via a school-based interdisciplinary intervention among youth. Arch Pediatr Adolesc Med. 1999;153(4):409-18. [ Links ]
35. Sahota P, Rudolf MCJ, Dixey R, Hill AJ, Barth JH, Cade J. Randomized controlled trial of primary school based intervention to reduce risk factors for obesity. BMJ. 2001; 323(7320): 1029-32. [ Links ]
36. Donnelly JE, Jacobsen DJ, Whatley JE, Hill JO, Swift LL, Cherrington A et al. Nutrition and physical activity program to attenuate obesity and promote physical and metabolic fitness in elementary school children. Obes Res. 1996;4(3):229-43. [ Links ]
37. Kain J, Uauy R, Albala, Vio F, Cerda R, Leyton B. School-based obesity prevention in Chilean primary school children: methodology and evaluation of a controlled study. Int J Obes. 2004;28(4):483-93. [ Links ]
38. Thomas J, Sutcliffe K, Harden A, Oakley A, Oliver S, Rees R, et al. Children and healthy eating: a systematic review of barriers and facilitators. London: EPPI Centre, Social Science Research Unit, Institute of Education, University of London; 2003. [ Links ]
39. Daley AJ, Copeland RJ, Wright NP, Roalfe A, Wales JKH. Exercise therapy as a treatment for psychopathologic conditions in obese and morbidly obese adolescents: a randomized, controlled trial. Pediatrics. 2006;118(5):2126-34. [ Links ]
40. Atlantis E, Barnes EH, Fiatarone Singh MA. Efficacy of exercise for treating overweight in children and adolescents: a systematic review. Int J Obes (Lond). 2006;30(7):1027-40. [ Links ]
41. Carrel AL, Clark RR, Peterson S, Nemet BA, Sullivan J, Allen DB. Improvement of fitness, body composition, and insulin sensitivity in overweight children in a school-based exercise program: a randomized, controlled study. Arch Pediatr Adolesc Med. 2005;159(10):963-8. [ Links ]
42. Allen DB, Nemeth BA, Clark RR, Peterson SE, Eickhoff J, Carrel AL. Fitness is a stronger predictor of fasting insulin levels than fatness in overweight male middle-school children. J Pediatr. 2007;150(4):383-7. [ Links ]
43. Eisenmann JC, Welk GJ, Wickel EE, Blair SN. Combined influence of cardiorespiratory fitness and body mass index on cardiovascular risk factors among 8-18 year old youth: The Aerobics Center Longitudinal Study. Int J Pediatr Obes. 2007;2(2):66-72. [ Links ]
44. WHO Multicentre Growth Reference Study Group. WHO Child Growth Standards based on length/height, weight and age. Acta Paediatr. 2006;(Suppl 450):76-85. [ Links ]
45. Fundo Social de Solidariedade do Estado de São Paulo. Available from: http://www.fundosocial.sp.gov.br/portal.php/sobre-galerias [ Links ]
46. Decreto Nº 55.620, de 24 de Março de 2010. Available from: http://www.al.sp.gov.br/repositorio/legislacao/decreto/2010/decreto%20n.55.620,%20 de%2024.03.2010.htm [ Links ]
 Corresponding author:
Corresponding author:
rfeferbaum@uol.com.br
Manuscript submitted Aug 08 2011
Accepted for publication Jul 10 2012

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}