










Serviços Personalizados
artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282
Rev. bras. crescimento desenvolv. hum. vol.22 no.3 São Paulo 2012
ORIGINAL RESEARCH
Autonomic modulation and functional capacity in diabetes mellitus type 1 and 2 subjects
Rafael Leite AlvesI; Flávio Mariz FreitasII; Alline Sancha Nascimento FernandesII; Sabrina Campos FerrazII; Edson da SilvaIII; Clynton Lourenço CorrêaIV; Luciana Duarte Novais SilvaV
IProfessor Substituto do Departamento de Ciências Básicas da Saúde da Universidade Federal dos Vales do Jequitinhonha e Mucuri (UFVJM), Rua da Glória, 187, Centro - CEP: 39100-000 - Diamantina (MG), Brasil
IIFisioterapeutas graduados pela Universidade Federal dos Vales do Jequitinhonha e Mucuri (UFVJM) , Rua da Glória, 187, Centro - CEP: 39100-000 - Diamantina (MG), Brasil
IIIProfessor Assistente do Departamento de Ciências Básicas da Saúde da Universidade Federal dos Vales do Jequitinhonha e Mucuri (UFVJM), Rua da Glória, 187, Centro - CEP: 39100-000 - Diamantina (MG), Brasil
IVProfessor Adjunto do Curso de Fisioterapia da Universidade Federal do Rio de Janeiro (UFRJ), Rua Prof Rodolpho Paulo Rocco, s/n, Ilha do Fundão - CEP: 21941-913 - Rio de Janeiro (RJ), Brasil
VProfessora Adjunta do Departamento de Fisioterapia Aplicada da Universidade Federal do Triângulo Mineiro, Avenida Getúlio Guaritá, 159, Bairro Abadia - CEP: 38025-440 - Uberaba (MG), Brasil
ABSTRACT
OBJECTIVES: Evaluation of heart rate variability (HRV) during cardiovascular autonomic tests and functional capacity of patients with type 1 and type 2 DM.
METHODS: Fifteen individuals with DM and twelve healthy ones were evaluated during cardiovascular autonomic tests of maneuver enhancement of respiratory sinus arrhythmia (RSA), handgrip and Valsalva. In addition, the Paschoal test was applied to evaluate submaximal functional capacity. During the tests, autonomic heart rate variability (HRV) was collected by recording the RR intervals, considering the rates in the time domain (RMSSD and pNN50) and frequency domain, as low and high frequency (LF and HF) and the relationship between them (LF / HF). Besides the analysis of HRV and capillary glucose, the distance traveled during Paschoal test was also recorded.
RESULTS: The values related to blood glucose levels were significantly higher (p <0.05) in DM1 and DM2 groups compared to controls. PNN50 values for DM1 in all tests were lower compared to CDM1. No statistical difference was found when compared DM2 with CDM2. The distance of Paschoal test was similar between groups of individuals with diabetes and their respective controls.
CONCLUSION: The variable pNN50 was lower in individuals with DM1, suggesting reduced of the parasympathetic activity in these individuals, but no change in functional capacity, as measured by Paschoal test when compared to the control group.
Key words: diabetes mellitus; autonomic nervous system; heart rate; functional capacity.
INTRODUCTION
Diabetes Mellitus (DM) is a group of metabolic disease characterized by hyperglycemia resulting from defects secretion or insulin action, or both. The disease is associated to increased mortality and high risk development of complications micro-and macrovascular complications, as well as neuropathies, blindness, kidney failure and limb amputations1,3. It is responsible by expenditures in health and substantial reduction in the ability to work and the expectation of life1,2,3.
Cardiovascular autonomic neuropathy is a common dysfunction autonomic found in DM patients DM, causing abnormalities in heart rate control, and dynamic vascular4.
Autonomic dysfunction may be evaluated by the heart rate variability (HRV), which reflects the periodic fluctuations in heart rate instantaneous and the duration of intervals between R waves (R-Ri) consecutive electrocardiogram, and is therefore depending on the activity of sympathetic and parasympathetic nervous system5,6.
For this evaluation, some tests have been used since the invasive through block pharmacological (single or double lock of the cardiac sympathetic and parasympathetic)7,8, even by physiological maneuvers not invasive as Valsalva9 maneuver, active10,11 or passive12 postural maneuver, realization of respiratory sinus arrhythmia13, immersion of the face or hand in cold water test14 or change in altitude15. However, it is noteworthy that they are few studies have analyzed HRV during not invasive autonomic maneuvers in individuals with DM.
Through of the evaluation for HRV autonomic maneuvers can identify objectively cardiovascular autonomic neuropathy early stages and provide treatment options that based on control of symptoms and prevention of disease progression. Thus, it is possible to prevent cardiac events arising from complications of autonomic neuropathy, such as resting tachycardia and silent myocardial infarction, among others16.
Another important aspect for understanding of clinical diabetes Mellitus the functional capacity of affected individuals is research. Was published in Brazil, the Paschoal Test suggests that the prediction of physical capacity from an effort protocol performed on a cycle ergometer, similar Six-Minute Walk Test (6MWT)17. This test differs from the 6MWT for proposing a graduate of the physical capacity from the distance reached by the person while performing the same. Furthermore, connotes biomechanics differently due to the fact that person doing it in a sitting position which may reveal functional capacity different aspects and heart and breathing response.
Thus, the objective is to evaluate the heart rate variability (HRV) during cardiovascular autonomic tests and functional capacity in DM types 1 and 2 subjects.
METHODS
Casuistry
In the period between September 2008 and March 2009, 145 DM patients registered in Strategies Family Health (SFH) of Diamantina - MG were tried based on their records and notes of the register in the basic unit of health, 37 were pre-selected to participate in this study because at this point satisfies the inclusion criteria.
Pre-selected individuals were submitted to initial assessment, which consisted of anamnesis and verification of the medication at the time. Of these 37 subjects, 15 accepted or met the inclusion criteria, and others being excluded they were using beta-blocker or channel blocker calcium medication (16), presenting difficulties to perform the tests as osteoarthritis affecting the gait or other orthopedic conditions (1), physiological and/or neurological conditions as stroke (2), or by incompatibility between days and times assessments of the availability of volunteers (3).
Inclusion Criteria
Inclusion criteria consisted in: to be eighteen years or when smaller, have the consent free and informed consent signed by parents or responsible, have a diagnosis of DM type 1 and 2, with blood glucose levels greater than the 126mg/dL18.
Exclusion criteria
The exclusion criteria adopted in this study were normal values of glucose, arterial hypertension in stage 2 and 319, cardiopathies or pneumopathies confirmed or instability clinical, neuropathy unrelated the DM, regular physical activity more than one month, drugs beta-blockers, calcium channel blockers and beta-adrenergic agonists or the inability to understand and perform the tests.
Ethical aspects of research
The 27 individuals who agreed participate in the study were explained about the procedures which would be submitted and signed an informed consent, approved by the Ethics Committee of Federal University of the Vales do Jequitinhonha and Mucuri under resolution number 008/09.
Experimental protocol
The volunteers were divided into two groups which are: individuals with diagnosis of DM type 2 (DM 2, n = 10) and individuals diagnosed with DM type 1 (DM1, n = 5). The control groups consisted of individuals registered in the SFH or members of the University invited by the researchers, they should also meet the same inclusion criteria, except for the diagnosis of DM 1 or 2. The sample selected for the control totalized 12 individuals, distributed in two groups according to age should be similar to the experimental group: the control group for diabetes mellitus 1 (CDM1, n = 6) and the control group for diabetes mellitus 2 (CDM2, n = 6).
Autonomic tests and Paschoal Test
Autonomic cardiovascular tests adopted were Valsalva maneuver, maneuver enhancement of Respiratory Sinus Arrhythmia and Handgrip addition of a submaximal Paschoal test. They were held in sequence presented with a range rest for the variables cardiovascular return to values baseline.
The protocols were performed with the individual in the sitting position, always controlling the temperature (20°C and 25°C) and relative humidity (between 40% and 60%).
For each protocol performed was registered a file hrm on the heart rate monitor, comprising the periods initial and final rest and the period of the maneuver.
1. Valsalva maneuver12,20
The Valsalva maneuver was performed while seated, this being told to keep the forced expiration against a closed glottis for 15 seconds with an expiratory pressure of 40 mmHg measured by manometer, observing two minutes of rest before performing of the maneuver and two minutes later to complete the same.
2. Maneuver enhancement of Respiratory Sinus Arrhythmia13,20
During the maneuver accentuation of respiratory sinus arrhythmia (RSA), with the subject sitting the same was asked to inhale and exhale deeply and slowly, and is also instructed to monitor the respiratory rate according to the verbal command of the evaluator, allowing themselves to 5-6 breaths per minute in a collect of about 6 minutes, the first two minutes of spontaneous breathing, 3rd and 4th minutes of RSA and 5th and 6th minutes with return to spontaneous breathing.
3. Handgrip20
Also known as static exercise, was the measure of grip strength, three maximal contractions, whichever is the greater of the same. We used 30% of this intensity in an isometric contraction sustained for at least 2 minutes with the patient in the sitting position, observing the periods of two minutes of rest before and after the maneuver. Both the measurement of force, and monitoring for its sustained isometric contraction was performed with the aid of a dynamometer.
4. Paschoal Test17
Finally we performed the Paschoal test, used in protocols of evaluation of the cardiac functional capacity. The volunteers were instructed to pedal on a cycle ergometer horizontal (Movement®H3), the highest possible speed for six minutes without resistance. The speed minimum average for validation was 20 km/h, and at the end of the test, the total distance traveled was recorded.
Between each autonomic maneuver performed inserted itself a period of rest for the HR returned to baseline, but was considered for HRV analysis only the period of the maneuvers.
HRV Analysis
In all protocols of modulation autonomic evaluation was monitored and data recording of the HR beat to beat by Polar® frequencimeter (model S810i, 2001, Finland). Such equipment is validated in the literature to evaluate the autonomic modulation of HR21 and, because of its low cost is available to clinical practice.
Data analysis was performed later to the transfer thereof to a computer using an infrared interface compatible with the frequencimeter model using the software Polar Precision Performance®.
After the transfer of data, HR graphics were analyzed visually and if necessary a digital filter was applied by their own analysis software. Furthermore, it was observed that each signal collected had a minimum of 256 points necessary to sustain the data analysis.
HRV was analyzed considering the indices in the time domain, using simple statistics and frequency domain, which by means of spectral analysis allows to decompose the HRV into its components, defining them by their frequency and amplitude.
In the time domain the indices were used:
RMSSD: represents the square root of the sum of the square of the differences between the iR-R in the registry divided by the number of iR-R at a given time minus one iR-R 22. It is able to provide an indirect measure of parasympathetic activity specifically active in the sino atrial node23.
pNN50: which represents the percentage of the total number of iR-R that have a difference of more than 50 milliseconds relative to the previous R-Ri, also reflecting an indirect measure of parasympathetic tone24.
In the frequency domain were used the indices:
Low frequency (LF): with variation range from 0.04 to 0.15 Hz, which is due to the joint action of vagal and sympathetic components of the heart, being that the sympathetic action is predominant. Therefore, this frequency band has been used as a marker of the sympathetic modulation on heart5,6.
High frequency (HF): with a variation range of 0.15 to 0.4 Hz, which corresponds to the respiratory modulation and is an indicator of the vago action in the heart5,6.
LF / HF ratio: ratio that reflects the absolute and relative interactions between the sympathetic and parasympathetic components of autonomic nervous system in heart25,26.
Statistical Analysis
We used the Kolmogorov-Smirnov test, though there is the normal distribution of variables analyzed.
We compared the data of age, anthropometric characteristics, resting heart rate, systolic and diastolic blood pressure at rest and glucose between groups of volunteers with diabetes and their control groups using the unpaired t test.
The indices obtained by applying the experimental protocols (RMSSD, pNN50, LF, HF, LF/HF) were compared between groups of individuals with diabetes and their respective control groups using the unpaired t test. All statistical tests used in this study had a significance level set at 5%.
RESULT
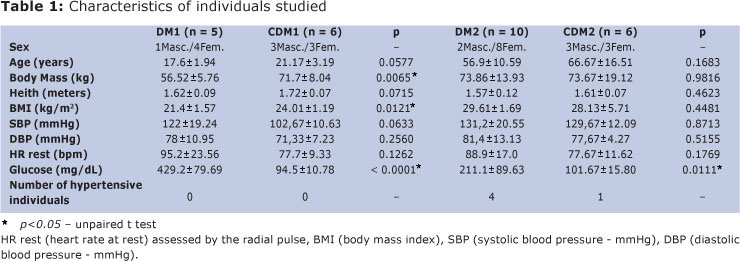
The results of this study are presented in Tables 1 and 2, on average and standard deviation. It is noted in Table 1 that the group of individuals with DM had higher blood glucose levels (p<0.05) when compared to their respective control groups. In addition, body weight and body mass index (BMI) were lower in DM1 patients group when compared to CDM1.
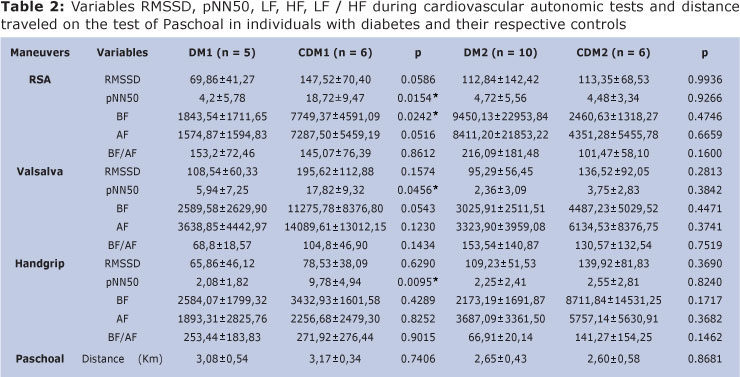
In Table 2, of the variables considered during the cardiac autonomic tests, the variable pNN50 was lower in DM1 compared to the group CDM1 in all maneuvers. Furthermore, the variable LF was lower in DM1 group compared to the CDM1 during ASR.
There were no statistical differences in the comparisons of the indices in the time and frequency domain when compared the DM2 and CDM2 groups.
We also found no statistically significant differences when comparing the distances traveled during the Paschoal test.
DISCUSSION
In the present study, we used HRV to evaluate autonomic modulation of heart rate, because it is a noninvasive method, effective and low cost.
Studies report significant changes in HRV as a function of age, fitness level27 and the presence of risk factors for coronary artery disease (CAD)28 or established CAD29.
Besides these factors, the literature also shows that heart rate (HR) and systolic blood pressure (SBP) and diastolic (DBP) at rest is influenced by: genetic characteristics, anthropometric measurements (weight and height), gender, hormonal and emotional factors, body position, environmental influences, level of physical fitness, clinical condition, among others9.
In this study, the values related to body mass and BMI were significantly lower in DM1 compared to CDM1. However, for both groups the values were situated in the normal range18. HR, SBP and DBP at rest showed no significant difference between groups. As expected, blood glucose levels in groups with a diagnosis of diabetes mellitus was higher when compared to their respective controls, confirming the presence of a primary disorder, either in liberation or capture of insulin or both mechanisms, leading to high blood glucose levels found .
In relation to the indices in time domain, the values of RMSSD showed no statistically significant differences in comparisons between the groups with diabetes and their respective controls. However, the DM1 group had significantly lower pNN50 variable when compared to the control group CDM1 in all autonomic maneuvers performed, thus suggesting lower vagal activity in DM1 group.
According to the data of pNN50 variable, the results of this study are consistent with previous studies that found a reduction in vagal activity in patients with diagnosis of DM130,31.
Considering the RMSSD values obtained in this study, lower mean values are observed in individuals with DM1 although not statistically significant. But it may be noted that there is great dispersion of data, observed by the high standard deviation in all maneuvers used, may explain the absence of statistical difference.
In relation to results obtained in the frequency domain, were found significantly higher values of the BF band for the individuals of the group CDM1 during the maneuver of accentuation of the respiratory sinus arrhythmia. However, these individuals also tended to have larger values of the AF band, even if no present statistically significant difference, so that there was no significant difference in LF / HF ratio, but with a tendency to lower values in CDM1.
Some studies have shown that a better way to characterize the sympathetic-vagal balance is the use of LF/HF ratio, which reflects the absolute and relative interactions between the sympathetic and parasympathetic components of autonomic nervous system in the heart 5.
The results for the frequency domain, in DM1group, are discordant from other previous studies that found a statistically significant difference, showing a diabetic autonomic neuropathy in the early stage of onset of the disease28,31,32.
The possible explanation for the absence of significant differences in the present work is the time of diagnosis of disease. As was not standardized the time of diagnostic of DM1 for inclusion of individuals in the study, this data was heterogeneous and may be the reason for the large dispersion of data and lack of significant difference.
In relation to subjects with DM2 were not statistically significant differences in any of the indices evaluated for autonomic maneuvers.
This result is similar to the results of previous studies that assessed HRV during autonomic maneuvers. In a recent study of HRV tests were used as the Valsalva maneuver and deep breathing and are not statistically significant differences between healthy subjects and those with early diagnosis of diabetes33. Another study in 2008 evaluated healthy and obese women with and without DM2 during Handgrip maneuver, finding no statistically significant differences between groups34.
The results of this study differ from others found in the literature, where individuals with T2DM have increased sympathetic tone compared to healthy subjects35,36,37.
The values of the distance traveled during the performance of Paschoal test showed no statistically significant difference. This test offers a graduation of the physical capacity from the distance traveled on a cycle ergometer17 in submaximal intensity (level of activity of daily living).
According to the literature it is expected under aerobic capacity in individuals diagnosed with diabetes mellitus38,39. One possible explanation for the results of this study in relation to functional capacity, is that the assessment protocol applied, using submaximal intensity of effort. Therefore, it is possible that the functional limitations resulting from the DM occurs in levels of physical exercise levels higher, not limiting the activities of daily living of individuals with DM.
The sample size and the lack of records regarding the duration of the disease can be identified as limiting factors in this study. We can still consider the difficulty of selecting a sample that fully meets the criteria inclusion, taking into consideration the high percentage of subjects with DM in association with other diseases such as hypertension and concomitant use of drugs, such as channel blockers calcium or beta-blockers, which greatly affect the autonomic modulation.
The variable pNN50 was significantly lower in subjects with diabetes mellitus type 1 in all cardiovascular autonomic tests performed, showing a reduction of parasympathetic activity in these individuals when compared to the control group. Already, the functional capacity assessed at submaximal levels were similar between subjects with and without Diabetes Mellitus, thereby inferring that the activity limitations due to the change in HRV found, occurs at higher levels of physical activity in the sample considered.
ACKNOWLEDGMENTS
The authors wish to thank Fundação de Amparo à Pesquisa de Minas Gerais FAPEMIG/PIBIC for financial support to the project (Process: APQ00595-08).
REFERENCES
1. Davidson MB, Defrozon RA, Drash A, Raskin P. Report of the Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Diabetes Care. 2003;26:5-20. [ Links ]
2. Torres HC, Hortale VA, Schall V. A experiência de jogos em grupos operativos na educação em saúde para diabéticos. Cad. Saúde Pública. 2003;19(4):1039-1047. [ Links ]
3. Ortiz MCA, Zanetti ML. Levantamento dos fatores de risco para diabetes mellitus tipo 2 em uma instituição de ensino superior. Rev Latino-am Enfermagem. 2001;9(3):58-63. [ Links ]
4. Maser RE, Lenhard MJ. Cardiovascular Autonomic Neuropathy Due to Diabetes Mellitus: Clinical Manifestations, Consequences, and Treatment. J Clin Endocrinol Metab. 2005; 90(10):5896-5903. [ Links ]
5. Task Force of European Society of Cardiology of the North American Society of Pacing Electrophysiology. Heart rate variability. Standars of mensurement, physiological interpretation and clinical use. Circulation. 1996;93:1043-65. [ Links ]
6. Longo A, Ferreira D, Correia MJ. Variabilidade da Freqüência Cardíaca. Rev Port Cardiol.1995;14(3):241-262. [ Links ]
7. Akselrod S, Gordon D, Ubel FA, Shannon DC, Berger AC, Cohen RJ. Power spectrum analysis of heart rate fluctuaction: a quantitative probe of beat-to-beat cardiovascular control. Science. 1981;213:220-222. [ Links ]
8. Pomeranz B, Macauley RJ, Caudill MA, Kutz I, Adam D, Gordon D. Assessment of autonomic function in humans by heart rate spectral analysis. Am J Physiol. 1985;248: H151-H153. [ Links ]
9. Marães VRFS, Santos MDB, Catai AM, Moraes FR, Oliveira L, Gallo Jr L, et al. Modulação do sistema nervoso autonômico na resposta da freqüência cardíaca em repouso e à manobra de valsalva com o incremento da idade. Rev Bras Fisioter. 2004; 8(2): 97-103. [ Links ]
10. Marães VRFS. Estudo da variabilidade da freqüência cardíaca durante exercício físico dinâmico em voluntários sadios [dissertação de mestrado]. Campinas: Universidade Estadual de Campinas. Instituto de Biologia, 1999. [ Links ]
11. Ribeiro TF, Azevedo GD, Crescêncio JC, Marães VRFS, Papa V, Catai AM. Heart rate variability under resting conditions in postmenopausal and young women. Braz J Med Biol Res. 2001;34(7):871-7. [ Links ]
12. Martinelli FS. Resposta da freqüência cardíaca e da pressão arterial sistêmica às manobras posturais passivas e de Valsalva, em indivíduos sedentários e atletas corredores de longa distância [dissertação de mestrado]. Campinas: Universidade Estadual de Campinas, 1996. [ Links ]
13. Santos MDB, Moraes FR, Marães VRFS, Sakabe DI, Takahashi ACM, Oliveira L, et al. Estudo da arritmia sinusal respiratória e da variabilidade da freqüência cardíaca de homens jovens e de meia idade. Rev. Soc. Cardiol. 2003;13(3):15-26. [ Links ]
14. Perini R, Milesi S, Biancardi L, Pendergast DR, Veicsteinas A. Heart rate variability in exercising humans: effect of water immersion. Eur Appl Physiol 1998;77:326-332. [ Links ]
15. Perini R, Milesi S, Biancardi L, Veicsteinas A. Effects of high altitude acclimatization on heart rate variability in resting humans. Eur J Appl Physiol. 1996;73: 521-528. [ Links ]
16. Vinik AI, Ziegler D. Diabetic Cardiovascular Autonomic Neuropathy. Circulation. 2007;115:387-397. [ Links ]
17. Paschoal MA. Avaliação cardiorrespiratória de esforço e programa de recondicionamento aeróbio em cicloergômetro para pacientes com doença pulmonar obstrutiva crônica. Rev Bras Fisioter. 2002; 6(3):119-25. [ Links ]
18. Sociedade Brasileira de Diabetes. Atualização Brasileira sobre Diabetes, 2005. [ Links ]
19. V Diretrizes Brasileiras de Hipertensão Arterial. Arq. Bras. Cardiol. São Paulo Sept. 2007; 89(3). [ Links ]
20. Castro CLB, Nóbrega ACL, Araújo CGS. Testes Autonômicos Cardiovasculares. Uma Revisão Crítica. Parte I e II. Arq Bras Cardiol. 1992;59:75-83/151-158. [ Links ]
21. Vanderlei LCM, et al. Comparison of the Polar S810i monitor and the ECG for the analysis of heart rate variability in the time and frequency domains. Braz J Med Biol Res. 2008; 41(10):854-859. [ Links ]
22. Antila K. Quantitativa characterization of heart rate during exercise. Scand J Clin Lab Invest. 1979; 80:153-155. [ Links ]
23. Kleiger RE, Stein KP, Bosner MS, Rottman JN. The time-domain mensurements of heart variability. Armonk, Futura. 1995: 33-46. [ Links ]
24. Pumprla J, Howorka K, Groves D, Chester M, Nolan J. Functional Assessment of Heart Rate Variability: Physiological Basis and Practical Applications. Int. J. Cardiol. 2002; 84:1-14. [ Links ]
25. Lombardi F, Malliani A, Pagani M, Cerutti S. Heart rate variability and its sympatho-vagal modulation. Ospedale L. Sacco, Università di Milano, Italy. 1: Cardiovasc Res. 1996; 32(2): 208-216. [ Links ]
26. Pagani M, Lucini D, Pizzinelli P, Sergi M, Bosisio E, Mela GS, et al. Effects of aging and of chronic obstructive pulmonary disease on RR interval variability. J Auton Nerv Syst. 1996; 59:125-132. [ Links ]
27. Melo RC, et al. Effects of age and physical activity on the autonomic control of heart rate in healthy men. Braz J Med Biol Res. 2005;38(9):1331-38. [ Links ]
28. Pavy-Le Traon A, Fontaine S, Tap G, Guidolin B, Senard JM, Hanaire H. Cardiovascular autonomic neuropathy and other complications in type 1 diabetes. Clin Auton Res. 2010; 20(3): 153-60. [ Links ]
29. Günther A, Witte OW, Hoyer D. Autonomic dysfunction and risk stratification assessed from heart rate pattern. Open Neurol J. 2010; 15(4): 39-49. [ Links ]
30. Evans JM, Ziegler MG, Patwardhan AR, Ott JB, Kim CS, Leonelli FM, et al. Gender differences in autonomic cardiovascular regulation: spectral, hormonal, and hemodynamic indexes. J Appl Physiol. 2001; 91(6): 2611-8. [ Links ]
31. Waden J, Forsblom C, Thorn LM, Saraheimo M, Rosengård-Bärlund M, Heikkilä O, et al. Adult stature and diabetes complications in patients with type 1 diabetes: the FinnDiane study and the diabetes control and complications trial. Diabetes. 2009;58:1914-1920. [ Links ]
32. Boysen A, Lewin MAG, Hecker W, Leichter HE, Uhlemann F. Autonomic function testing in children and adolescents with diabetes mellitus. Pediatric Diabetes. 2007; 8: 261-264. [ Links ]
33. Cabezas-Cerrato J, Hermida RC, Cabezas-Agrícola JM, Ayala DE. Cardiac Autonomic Neuropathy, Estimated Cardiovascular Risk, and Circadian Blood Pressure Pattern in Diabetes Mellitus. Chronobiol Int. 2009; 26(5):942-957. [ Links ]
34. Franklin RM, Baynard T, Weinstock RS, Goulopoulou S, Carhart Jr R, Ploutz-Snyder R, Figueroa A, Fernhall B, Kanaley JA. Autonomic responses to physiological stressors in women with type 2 diabetes. Clin Auton Res. 2008; 18: 66-73 [ Links ]
35. Barbosa FJ, Barbosa PRB, Cordovil I. Modulação autonômica do coração na Hipertensão Arterial Sistêmica. Arq Bras Cardiol. 2002;78(2):181-188. [ Links ]
36. Balcioglu S, Ugur A, Turkoglu S, Ozdemir M, Çengel A. Heart Rate variability and Heart Rate Turbulence in Patients With Type 2 Diabetes Mellitus With Versus Without Cardiac Autonomic Neuropathy. Am J Cardiol. 2007;100:890-893. [ Links ]
37. Masi CM, Hawkley LC, Rickett EM, Cacioppo JT. Respiratory sinus arrhythmia and diseases of aging: Obesity, diabetes mellitus, and hypertension. Biological Psychology. 2007;74: 212-223. [ Links ]
38. Gregoire J, Tuck S, Yamamoto Y, Hughson RL. Heart rate variability at rest and exercise: influence of age, gender, and physical training. Can J Appl Physiol. 1996;21(6):455-470. [ Links ]
39. Lyerly GW, Sui X, Lavie CJ, Church TS, Hand GA, Blair SN. The association between cardiorespiratory fitness and risk of all-cause mortality among women with impaired fasting glucose or undiagnosed diabetes mellitus. Mayo Clin Proc. 2009; 84(9): 776-779. [ Links ]
 Corresponding author:
Corresponding author:
lunovais@yahoo.com.br
Manuscript submitted Feb 16 2012
Accepted for publication Aug 10 2012

{kind=link}
{kind=link}