










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores
Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282
Rev. bras. crescimento desenvolv. hum. vol.22 no.3 São Paulo 2012
ORIGINAL RESEARCH
Mental health awareness intervention in schools
Luísa CamposI, II, III; Filipa PalhaI, III; Pedro DiasI, II; Vânia Sousa LimaI, II; Elisa VeigaI, II; Natália CostaIII; Ana Isabel DuarteIII
IFaculty of Education and Psychology, Catholic University of Portugal, Porto, Portugal
IICenter for Studies in Human Development (CEDH), Catholic University of Portugal (Oporto Regional Center)
IIIENCONTRAR+SE - Association to Support Persons with Severe Mental Disorders - Porto, Portugal
ABSTRACT
The lack of information and stigma associated with mental disorders are major obstacles to the promotion of mental health. The "UPA Makes the Difference: Mental health awareness intervention in schools" project aims to contribute to increase young people knowledge regarding mental health issues. This project is part of the "United to Help Movement", focusing on the combat of mental illness stigma and discrimination.
OBJECTIVES: to describe the psychometric characteristics of the questionnaire UH (United to Help) and to verify the adequacy of action to promote mental health.
METHODS: this study was conducted with 26 students (15-17 year-olds). The mental health intervention is composed by 2 sessions. The questionnaire was administered at the beginning of the 1st session and in the end of the 2nd session.
RESULTS: cronbach'salpha regarding 2 sections of the "Questionnaire UPA" stated poor and acceptable levels of internal consistency (stigmatizing perceptions and perceptions of knowledge, respectively). The post intervention assessment showed a significant increase in the total score of the perceptions of knowledge; no significant differences in stigmatizing perceptions; and a significant decrease in help-seeking intentions when facing a mental health problem, although most participants have come to consider different types of help.
CONCLUSION: the results suggest the need to review the structure of the "stigmatizing perceptions" section of the questionnaire, as well as to conduct new analyses with a larger sample. Furthermore, results show the adequacy of the methodology used in the intervention, particularly in the capacity showed to promote the increase of knowledge regarding mental health issues.
Key words: mental health; social stigma; adolescents; schools.
INTRODUCTION
Mental health problems affect 10 - 20% of children and adolescents worldwide1,2. Apart from the situations identified at these early ages, it is known that a great majority of difficulties of this nature faced by adults had the onset during youth3,4. In this way, the prevention and treatment of mental health problems, and the promotion of mental health and psychological well-being of children and youth is assumed as a priority in terms of public health worldwide, including Portugal. Despite this fact, there are significant barriers to mental health promotion, including the lack of information regarding mental health issues, and mental illness stigma6-9.
Classic social psychological theory support that children are born with no stereotypes, prejudice or discrimination and slowly acquire them through incremental learning processes during interactions with parents, peers and other key people in their lives10.
Research has shown that most children around five years of age have knowledge of stereotypes related to mental illness, and report that they personally believe them9,11. Negative attitudes towards mental illnesses observed tend to be consolidated during adulthood12.
Based on the recognition of the prevalence of mental health problems in childhood and adolescence; on the fact that attitudes towards mental health problems are acquired gradually, starting early in childhood and consolidating into adulthood; and that schools are a privileged context of accessing young people3, 13, in recent decades we have assisted to the development of school-based initiatives aimed at promoting mental health.
Such initiatives can be found in several countries like the United Kingdom, Canada, Germany, USA, Australia and Japan, to mention just a few. They all share the main objectives of promoting young people's mental health literacy, and/or combating the stigma associated with mental health problems 14 (e.g., Crazy? So what?8, MindMatters - Understanding mental illness13; Beyoundblue Schools Research Initiative - Mental Health Literacy Component15; The Science of Mental Illness16; e Mental Health Awareness in Action program17).
Despite the fact that in the Portuguese National School Health Program 18 "mental health" is considered a priority area for the promotion of an healthy lifestyle, it is not clear how it is expected to approach these issues. To our knowledge, there are no systematic interventions specifically focusing on mental health issues, and/or on combating mental illness stigma amongst young people. It is in this context that the "UPA Makes a Difference" project was developed by ENCONTRAR+SE - Association to Support Persons with Severe Mental Disorders - an NGO focused on mental health issues. The project aims to contribute to young peoples' (15-18 year-olds) increase of mental health literacy.
Considering the complexity of developing an intervention about these themes for a young public, during the first year of the project a pilot study was carried out (August 2009 - July 2010).
Thus, to describe the psychometric characteristics of the questionnaire UH (United to Help) and to verify the adequacy of action to promote mental health.
METHODS
Participants
Twenty-six students from 2 classes of private secondary schools (57.7% in 10th grade and 42.3% in 11th grade) were included in this study. Students were aged between 15 to 17 year-olds (M =15.77; SD = 0.15). Regarding gender, 10 were male and 16 female. All students were single and Portuguese. Ten students were enrolled in the area of Social-economics Studies, 8 in Science and Technology, 7 in Languages and Humanities, and 5 in Visual Arts.
In what concerns to social-economic status, according to Graffar's classification19, 88.5% were included in level 1 (high SES), 7.7% in level 2 (medium-high SES), and 3.8% in level 4 (medium-low SES).
Parents' educational level ranged between secondary school to PhD (most parents graduated from college). Regarding parental professional status, 69.2% of mothers and 80.8% of fathers were employed.
In what refers to contact with people with mental health problems, 21 (80.8%) participants knew someone with mental health problems and only four (15.4%) mentioned not to know someone with these problems. Mental health problems identified by students included mood disorders (N=7; 26.9%), dementias (N=3; 11.5%), eating disorders (N=2; 7.7%), and mental retardation (N=2; 7.7%). Regarding the degree of proximity, 5 students (23.8%) mentioned the selected person to be a first degree family member, 7 students (33.3%) indicated a distant family member, 5 students (23.8%) pointed out a friend, and one student (4.8%) referred him(her)self.
Measures
Questionnaire UPA Makes the Difference: Students' perceptions of mental health problems
Questionnaire "UPA Makes the Difference: Students' perceptions of mental health problems" was developed taking into account: a) literature review on knowledge and attitudes towards mental health problems; b) discourse content from 10 focus group sessions held with 15-18 years old students, parents and teachers20,21. The questionnaire comprises a social-demographic form and three sections, encompassing a) stigmatizing perceptions; b) perceptions of knowledge; and c) behavioral intentions.
Social-demographic form
This form allows data collection on students and families' social-demographic features. Students data includes: age; civil status; nationality; city/town; occupation; school year; school failure history; scientific area; leisure activities; contact and degree of proximity with people with mental health problems. Family data refers to family composition; family members' ages, educational level, professions and occupational status, and 5 SES indicators, using Graffar's classification (occupation and educational level of parents, neighborhood appearance; housing conditions, and major family income sources).
Stigmatizing perceptions
This section comprises 19 items (11 of which were translated and adapted from PHS-AMI - Public Health Scale - Attitudes Toward Mental Illness22), organized in a 5-point Likert scale (0 = completely disagree; 4 = completely agree).
Perceptions of Knowledge
This section comprises questions regarding the perception of knowledge on 14 mental health problems (depression, bipolar disorder, phobias, panic disorder, obsessive-compulsive disorder, PTSD, personality disorders, schizophrenia, anorexia nervosa, bulimia nervosa, addictions, alzheimer's dementia, autism spectrum disorders, disruptive behavior and attention deficit disorders) in a 5-point scale (0=don't know at all; 4=know very well); causes of mental health problems - with 8 cumulative possible answers; and one item evaluating their belief regarding the possibility of people with mental disorders "having a life similar to other people's" - in a 4-point scale (0 = impossible; 4 = possible).
Behavioral intentions
The section regarding behavioral intentions includes 3 questions: seeking help intention facing a mental health problem, organized in a 5 - point Likert scale (0 = definitely wouldn't seek help; 4 = definitely would seek help); type of help, with four options; intention of helping a close person with mental health problems (yes/no/I don't know).
A think aloud procedure was carried out with the preliminary version of the questionnaire, which allowed for the reappraisal of several items, making them more adequate for the participants' age range.
Mental health awareness intervention - structure and goals
The mental health awareness intervention were developed taking into account: a) literature review on school-based mental health promotion programs; b) discourse content from 10 focus group sessions held with 15-18 years old students, parents and teachers; material produced during the "UPA'08" campaign [anti-stigma campaign implemented by ENCONTRAR+SE (www.encontrarse.pt/upa08)].
The intervention is composed by 2 sessions, 120 minutes each, one-week interval, conducted by two trained psychologists. Topics are addressed taking into account developmental characteristics of the participants. Sessions follow an interactive methodology, using group dynamics and music, group discussions and disclosure regarding participants' emotional well-being.
Intervention specific goals, influencing sessions' structure, are: First Session: a) to present UPA Makes the Difference project; b) to establish group rules; c) to explore students' cognitive-emotional experience; d) to discuss the meaning of mental health problems; e) to understand the cross-line between mental health and mental disorders; f) to identify mental disorders causes and risks. Second session: a) to explore the impact of mental disorders; b) to discuss treatment and prognosis of mental disorders; c) to address behavioral intentions related to mental health problems; d) to discuss the concept of mental health; e) to raise students' awareness of mental health promotion; f) to promote non-stigma behaviors towards mental disorders.
Intervention general goals, specific session's goals, structure, contents, materials, methodologies and activities are manualized, allowing for its replicability.
Procedures
The Portuguese Ministry of Education (DGIDC - Direcção Geral de Inovação e Desenvolvimento Curricular, a governmental agency responsible for authorizing research projects in school settings) gave permission for this project to take place.
Informed consent was given by students' parents and by students in the beginning of the intervention.
The intervention was implemented in two classes of a private secondary school and the questionnaire was filled out by students in the beginning of the first session and at the end of the second session.
Data analysis
Data was analyzed with SPSS 17.0. Descriptive statistics were used for social-demographic characterization, stigmatizing perceptions and knowledge regarding mental health problems; Wilcoxon test was performed in order to assess pre-post intervention differences.
Ten stigmatizing perceptions items were recoded (items 1, 3, 5, 7, 9, 11, 13, 15, 17, 19). A total score was obtained using the average score for each item. Higher scores refer to less stigmatizing perceptions (more positive perceptions).
In order to assess perceptions of knowledge regarding mental health problems, a total score was obtained by adding the scores of each mental disorder; higher scores indicate higher perceptions of knowledge.
A p < 0.05 was used for statistical significance.
RESULTS
- Psychometric properties of the Questionnaire UPA Makes the Difference: Students' perceptions of mental health problems
Preliminary results concerning the internal consistency of the questionnaire "UPA Makes the Difference: Students' perceptions of mental health problems", showed a Cronbach's alpha of 0.52 in the stigmatizing perceptions' section, and 0.74 in the perceptions of knowledge section.
- Pre-intervention
Stigmatizing Perceptions
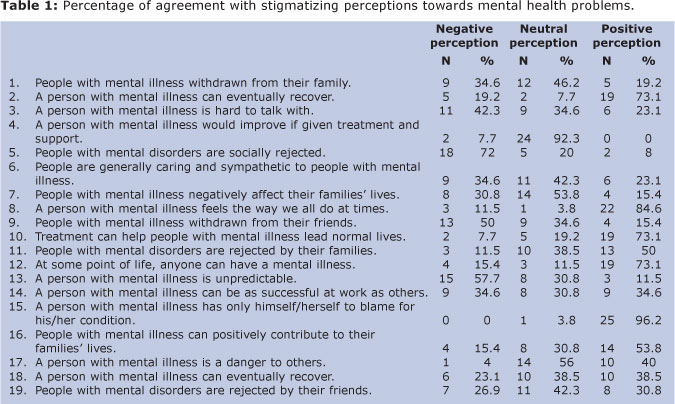
Regarding the stigmatizing perceptions section, in a 5 - point scale (0 = completely disagree; to 4 = completely agree), participants show neutral perceptions (M=2.29; SD = 0.27).
When an item-analysis was conducted on each of the 19 items (see Table 1), the most negative stigmatizing perceptions (completely disagree and disagree) are found in items 5 (social rejection), 13 (unpredictability), 9 (withdrawal from friends), and 3 (difficult to speak to); less stigmatizing perceptions (completely agree and agree) are found in items 15 (person is to blame for the situation), 8 (normalization of cognitive and emotional experience of mental disorders), 2 (possibility of recovery), 10 (positive impact of treatment), and 12 (possibility of someone having a mental disorder)
Perceptions of knowledge
The mean result of the perceptions of knowledge regarding listed mental disorders is positive (M = 2.09; SD = 0.61) in a 4 - point Likert scale (0 = impossible to 4 = possible).
A detailed analysis of the values obtained for each mental disorder indicate that participants have less knowledge perceptions about Autism spectrum disorders (M = 1.38; SD = 1.20) and about Disruptive behavior and attention deficit disorders (M = 1.46; SD = 1.24). Addictions (M = 3.08; SD = 0.76) and Anorexia nervosa (M = 3.12; SD = 0.91) are the disorders students refer as having a better knowledge.
The causes of mental health problems most referred by participants are negative life events (N = 24; 92.3%), drugs and/or alcohol abuse (N=21, 80.8%), heredity (N = 21, 80.8%) and family problems (N = 18, 69.2%).
Finally, only two (7.7%) participants consider to be possible that people with mental disorder have a "life similar to other people" (on a scale from 0 = impossible to 4 = possible).
Behavioral intentions
Most participants state that probably or definitely would seek help (N = 20, 77%) if they had a mental health problem.
Regarding the type of help, eight (38.1%) participants report that they would seek their parents' help, and, in the same proportion (N=8, 38.1%), other students would appeal to a variety of types of help (e.g., parents' help and specific services); two participants (9.5%) would seek a specific service (e.g., psychologist or psychiatrist); and three participants (14.3%) don't know what type of help they would seek.
Finally, 25 participants (96.2%) have the intention of helping a close person (e.g., family, friend, colleague) with a mental health problem.
- Post-intervention
Stigmatizing Perceptions
There are no significant differences between the total score of stigmatizing perceptions before (M = 2.29; SD = 0.27) and after (M = 2.37; SD = 0.34) the mental health awareness intervention (Z = -1.06; p = 0.29).
A detailed analysis shows significant differences in four items of the stigmatizing perceptions section. Perceptions are more positive (less stigmatizing) in items 2 (M = 2.69; SD = 1.09 - pre-test; M = 3.35; SD = 0.80 - post-test; Z = 2.29; p = 0.02), 12 (M = 2.81; SD = 1.20 - pre-test; M = 3.54; SD = 0.65 - post-test; Z= - 2.44; p = 0.02), 14 (M = 2.00; SD = 0.98 - pre-test; M = 2.58; SD = 0.95 - post-test; Z = -2.70; p = 0.007), and 18 (M = 2.15; SD = 0.93 - pre-test; M = 2.92; SD = 0.98 - post-test; Z = -2.80; p = 0.005).
Perceptions of Knowledge
There is a significant increase between pre (M = 2.09; SD = 0.61) and post-intervention (M = 2.49; SD = 0.73) students' perceptions of knowledge (Z = -3.70; p = 0.000).
Specifically, there are significant differences in the perceptions of knowledge regarding the following disorders: obsessive-compulsive disorder (M = 1.50; SD = 1.20 - pre-test; M = 2.28; SD = 1.10 - post-test; Z = -3.02; p = 0.003); personality disorders (M = 1.81; SD = 1.10 - pre-test; M = 2.42; SD = 1.17 - post-test; Z = -2.97; p = 0.003), disruptive behavior and attention deficit disorders (M = 1.46; SD = 1.24 - pre-test; M = 2.08; SD = 1.20 - post-test; Z = -2.69; p = 0.007), depression (M = 2.62; SD = 0.90 - pre-test; M = 3.23, SD = 1.03 - post-test; Z = - 2.65; p = 0.01), bipolar disorder (M = 2.16; SD = 1.34 - pre-test; M = 2.73; SD = 1.04 - post-test; Z = -2.43; p = 0.02), panic disorder (M = 1.54; SD = 1.17 - pre-test; M = 2.15; SD=1.12 - post-test; Z = -2.29, p = 0.02), and schizophrenia (M = 1.50; SD = 1.07 - pre-test; M = 2.00; SD = 1.13 - post-test; Z = -2.1; p = 0.04) (see Figure 1).

Regarding causes associated with the onset of mental health problems, there are no significant changes between pre and post-intervention.
Finally, in the question regarding the possibility of people with mental disorder having a life similar to "other people's", results are significantly higher in the post-intervention (M = 3.81; SD = 0.90) when compared to the pre-intervention (M = 3.23; SD = 0.91) (Z = -2.51; p = 0.01).
Behavioral intentions
The results show a significant decrease of the intention to seek help (M = 4.04; SD= 1.04 - pre-test; M = 3.77; SD = 0.95 - post-test; Z = -2.33; p = 0.02).
Regarding the type of help that participants would seek in case they would have to deal with a mental health problem, in the post-intervention assessment most of them consider using different types of help (N = 11, 42.3%). On the other hand, exclusive demand of parents' help decreases (N = 2, 7.7%).
There are no differences in the intention of helping a close person with a mental health problem (X2 = 0.04; p = 0.84).
DISCUSSION
Assuming the current emphasis on the importance of promoting mental health in young people, this study has an innovative character for the Portuguese context, setting the foundations for a research field with high impact on personal, familiar, social and economic levels. This occurs, on one hand, through the development of an assessment measure directed to evaluate students' perceptions towards mental health issues, and, on the other hand, by developing an intervention program directed to promote mental health in this population.
Results regarding the psychometric properties of the "Questionnaire UPA Makes the Difference: Students' perceptions of mental health problems" show adequate internal consistency of items about perceptions of knowledge on mental disorders (α = 0.74), and poor levels of internal consistency in what concerns to items related to stigmatizing perceptions (α = 0.52).
These results highlight the relevance of this measure in what regards to the assessment of perceptions of knowledge on mental disorders; however, the structure of the section related to stigmatizing perceptions should be revised and subject to further analysis using a larger sample.
Discussion about the appropriateness of the intervention designed to promote mental health is organized as follows: a) pre-intervention results on 26 participants regarding perceptions of knowledge, stigmatizing perceptions, and behavioral intentions; b) post-intervention results, allowing the assessment of the intervention's impact.
Pre-intervention results discussion requires taking into account the participants and families' social-demographic features, as well as the school setting where the intervention took place. Most of the participants come from a high social-economic background, with parents schooling ranging from secondary school to PhD. These factors, combined with a school setting that emphasized mental health promotion, should be considered for discussion.
Results from the pre-intervention assessment indicate high levels of perceptions of knowledge about mental health problems. Most participants revealed a reasonable perception of knowledge regarding the 14 mental disorders considered in the questionnaire, as well as an adequate identification of mental health problems' causes. These data can be better understood considering the social-demographic and school setting characteristics presented23,24.
Regarding stigmatizing perceptions, participants showed neutral perceptions towards people with mental disorders which, combined with the presumably good level of knowledge, are consonant with international data suggesting that higher levels of knowledge about mental disorders are associated with less negative attitudes9.
Only two of the 26 participants considered to be possible for someone with a mental disorder to have "a life similar to other people's". This result cannot be differentiated from a general belief about mental disorders - the unfeasibility of recovery. This belief is related to item 2 from stigmatizing perceptions section (possibility of recovery), where less stigmatizing perceptions were obtained. In this sense, students considered to be possible that someone presenting a mental disorder could "eventually" recover (which is congruent with their level of knowledge), even though the amplitude of the recovery is not enough for these people to have a life like most people do.
Finally, in what regards to the results from the behavioral intentions section, most students would be willing to seek help (from their parents and from unspecified services) and almost every participants would be willing to provide help to significant other who presented mental health problems. These results correspond to the congruence between behavioral intentions and the level of knowledge these students present, as well as to their neutral stigmatizing perceptions.
Focusing on the post-intervention assessment, results indicate: (1) a significant increase of the global score regarding perceptions of knowledge; (2) no significant differences on the global score regarding stigmatizing perceptions; and (3) significant decrease of participants' intention to seek help, although most participants moved to considering different types of help.
In what concerns to the significant increase of the global score of the section regarding perceptions of knowledge, analyzing separately these data by mental disorder, increased results were observed in disorders in which during pre-intervention student's presented lower levels of knowledge, suggesting a positive impact of the intervention on this domain.
No differences were found between pre and post intervention in what regards to mental health problems causes, suggesting that an appropriate level of knowledge was already present before intervention.
Regarding the item related to the possibility of "someone with mental disorders having a life similar to other people", a significant increase from pre to post intervention was observed. This result reinforces the appropriateness of the intervention - challenging the social representation of people with mental disorders not having a life like other people do, although no significant differences were found on the global score of stigmatizing perceptions.
Furthermore, the absence of significant differences on the global score of stigmatizing perceptions is in line with previous research8,21 showing that changes in attitudes are expected to occur in longer interventions, when compared to briefer ones8,25.
Participants showed a significant decrease, from pre to post intervention, in one's intention to seek help but, on the other hand, most students moved to considering different types of help. Both results can be better explained considering the 2nd session contents. Specifically, during session 2 students were asked to adopt proactive attitudes in promoting their own and other people's mental health. Then, it can be considered that decrease in post-intervention regarding one's intention to seek help reflects students' ability ant proactivity on promoting their own mental health. Additionally, session 2 focused on students' awareness of specific services (e.g., psychology service at school), and significant others (e.g., a teacher) from whom they can seek help. In this sense, the fact that students, after the intervention, moved to considering different types of help is considered a positive outcome. These results highlight the role of knowledge in designing interventions to promote mental health, in the sense that problems' early detection and appropriate help seeking only occur if students and significant others (family, teachers and friends) are informed about mental disorders symptoms and available resources25.
In what concerns students' willingness to help significant others presenting a mental problem, there were no significant differences between pre and post-intervention, probably due to the fact that at pre-intervention assessment 96.2% already revealed that they would.
In conclusion, both the questionnaire and the intervention developed appear to be adequate to the purposed goals, which is rather significant considering the fact that both resulted from students' discourse. On the other hand, it should be emphasized that intervention's contents and strategies were dynamic, appealing and reflexive, which are fundamental characteristics to the success of this type of interventions26.
Despite the fact that most interventions aimed at promoting mental health (including UPA Makes the Difference project) are brief25, efforts should be made in order to develop long-lasting interventions25,27, considering that change of attitudes and behaviors take time, and could be increased through booster sessions28.
The development of effective school-based interventions targeting young people should consider: their views on mental health; how they construct their knowledge about this topic; as well as their interests and concerns regarding mental disorders. In this way, the focus groups with different stakeholders (students, parents and teachers), the assessment both of the psychometric properties of the questionnaire "UPA Makes the Difference: Students' perceptions of mental health problems" and the impact of the mental health awareness intervention, resulted to be an appropriate methodology to reach the purposed goals.
Acknowledgements: The "UPA Makes the Difference" project was sponsored by the Portuguese High Comission for Health; the Calouste Gulbenkian Foundation; BPI bank, and by an unrestricted educational grant from Lilly Portugal. The project also had the scientific support from the Center for Studies in Human Development (CEDH) of Catholic University of Portugal (Oporto Regional Center). The authors would like to thank the contributions received from Sofia Moura Faria, Teresa Mansilha, Lígia Gomes, Sílvia Magalhães, Sónia Mesquita e Joana Batouxas.
REFERENCES
1. Kieling C, Baker-Henningham H, Belfer M, Conti, G, Ertem, I, Omigbodun, O, et al. Child and adolescent mental health worldwide: evidence for action. Lancet. 2011: 378;1515-1525. Doi: 10.1016/S0140-6736(11)60827-1 [ Links ]
2. World Health Organization . The World health report. Mental health: new understanding, new hope. [online document]. 2001 [cited 2011 Jan 30]. Available from: http://www.who.int/en/ [ Links ]
3. Murray C, Lopez A. The global burden of disease. A comprehensive assessment of mortality and disability from diseases, injuries and risk factors in 1990, and projected to 2020. Cambridge, Massachusetts: Harvard University Press; 1996. [ Links ]
4. U.S. Department of Health and Human Services. Mental Health: A Report of the Surgeon General-Executive Summary. Rockville, MD: U.S. Department of Health and Human Services, Substance Abuse and Mental Health Services Administration (SAMHSA), Center for Mental Health Services, Centre for Disease Control and Prevention (CDC); and National Institutes of Health, National Institute of Mental Health; 1999. [ Links ]
5. Kelly CM, Jorm AF, Wright A. Improving mental health literacy as a strategy to facilitate early intervention for mental disorders. Medical Journal of Australia. 2007;187:S26-S30. [ Links ]
6. Patel V, Flisher A, Hetrick S, McGorry P. Mental health of young people: A global public-health challenge. Lancet. 2007;369:1302-13. [ Links ]
7. Dwight E, Foa E, Gur RE, Hendin H, O'Brien CP, Seligman MEP, et al. Treating and preventing adolescent mental health disorders: What we know and what we don't know. A research agenda for improving the mental health of our youth. Oxford: Oxford Press; 2005. [ Links ]
8. Schulze B, Richter-Werling M, Matschinger H, Angermeyer MC. Crazy? So what? Effects of a school project on student's attitudes towards people with schizophrenia. Acta Psychiatrica Scandinavica. 2003;107:142 - 50. [ Links ]
9. Stuart H. Reaching Out to high school youth: The effectiveness of a video-based antistigma program. Canadian Journal of Psychiatry. 2006;51:647 - 653. [ Links ]
10. Corrigan P, Watson A. How children stigmatize people with mental illness. International Journal of Social Psychiatry. 2007:53(6);526 - 546. Doi: 10.1007/s10597-007-9084-9 [ Links ]
11. Augoustinos M, Rosewarne D. Stereotype knowledge and prejudice in children. British Journal of Developmental Psychology. 2001;19:143-56. Doi: 10.1348/026151001165912 [ Links ]
12. Wahl O. Children's views of mental illness: a review of the literature. Psychiatric Rehabilitation Skills. 2002:6;134-158. Doi: 10.1080/10973430208408430 [ Links ]
13. Wyn J, Cahill H, Holdsworth R, Rowling L, Carson S. MindMatters, a whole-school approach promotion mental health and wellbeing. Australian and New Zealand Journal of Psychiatry. 2000;34:594-601. [ Links ]
14. Bourget Management Consulting for the Canadian Alliance on Mental Illness and Mental Health. Mental Health Literacy: A Review of the Literature [online document]. 2007 [cited 2010 Nov 03]. Available from: http://www.camimh.ca/files/literacy/LIT_REVIEW_MAY_6_07.pdf [ Links ]
15. Spence S, Burns J, Boucher S, Glover S, Craetz B, Kay D, et al. The beyondblue schools research initiative: Conceptual framework and intervention. Child and Adolescent Psychiatry. 2005;13(2):159-164. [ Links ]
16. Watson A, Otey E, Westbrook A, Qardner A, Lamb T, Corrigan P, et al. Changing middle schoolers' attitudes about mental illness through education. Schizophrenia Bulletin. 2004;30(3):563-572. [ Links ]
17. Pinfold V, Stuart H, Thornicroft G, Arboleda- Flórez J. Working with young people: The impact of mental health awareness programmes in schools in the UK and Canada. World Psychiatry. 2005;4(1):48-52. [ Links ]
18. Ministério da Saúde e Divisão de Saúde Escolar. Programa Nacional de Saúde Escolar. [online document]. 2006 [cited 2010 Nov 03]. Available from: http://www.min-saude.pt/NR/rdonlyres/4612A602-74B9-435E-B720-0DF22F70D36C/0/ProgramaNacionaldeSa%C3%BAdeEscolar.pdf. [ Links ]
19. Amaro F. Escala de Graffar Adaptada. In: Costa AMB et al. Currículos Funcionais. Lisboa: IIE; 1996. [ Links ]
20. Magalhães S. UPA Faz a Diferença - Estudo piloto sobre conhecimentos, estigma e necessidades relativas a questões de saúde mental, num grupo de agentes educativos de alunos do ensino secundário privado [thesis]. Porto: Faculdade de Educação e Psicologia da Universidade Católica Portuguesa; 2010. [ Links ]
21. Gomes L. UPA Faz a Diferença - Estudo piloto sobre conhecimentos, estigma e necessidades relativas a questões de saúde mental, num grupo de alunos do ensino secundário público [thesis]. Porto: Faculdade de Educação e Psicologia da Universidade Católica Portuguesa, 2010. [ Links ]
22. Kobau R, DiIorio C, Chapman D, Delvecchio P. Attitudes about mental illness and its treatment: Validation of a generic scale for public health surveillance of mental illness associated stigma. Community Mental Health Journal. 2010;46:164-176. [ Links ]
23. Pinfold V, Toulmin H, Thornicroft G, Huxley P, Farmer P, Graham T. Reducing psychiatric stigma and discrimination: Evaluation of educational interventions in UK secondary schools. British Journal of Psychiatry. 2003;182:142 - 146. [ Links ]
24. Burns R, Rapee R. Adolescent mental health literacy: Young people's knowledge of depression and help seeking. Journal of Adolescence. 2006;29:225-239. [ Links ]
25. Patton G, Glover S, Bond L, Butle H, Godfrey C, Di Pietro G, et al. The Gatehouse Project: A systematic approach to mental health promotion in secondary schools. Australian and New Zealand Journal of Psychiatry. 2000;34:586-593. [ Links ]
26. Jorge-Monteiro F, Madeira T. Considerações sobre doença mental e comunicação social. Análise Psicológica. 2007; 25:97-109. [ Links ]
27. Sartorius N. Lessons learned from a 10-year programme against stigma and discrimination because of an illness. Psychology, Health & Medicine. 2006;11(3),383-388. [ Links ]
28. Botvin G, Renick N, Baker E. The effects of scheduling format and booster sessions on a broad-spectrum psychosocial approach to smoking prevention. Journal of Behavioral Medicine. 1983;6(4):359-379. [ Links ]
 Corresponding author:
Corresponding author:
mcampos@porto.ucp.pt
Manuscript submitted Jul 02 2011
Accepted for publication Apr 30 2012

{kind=link}