










Serviços Personalizados
artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282
Rev. bras. crescimento desenvolv. hum. vol.23 no.1 São Paulo 2013
ORIGINAL RESEARCH
Language disorders associated with deafness
Letícia Neves de OliveiraI; Bárbara Niegia Garcia de GoulartII; Brasilia Maria ChiariIII
ISpeech-Language Pathologist, Research Technician, Universidade Federal de São Paulo (UNIFESP)
IIResearch Associate, Universidade Federal de São Paulo. Assistant Professor, Universidade Federal do Rio Grande do Sul (UFRGS)
IIISpeech-Language Pathologist, Principal Investigator; Full Professor, Human Communication Disorders, Universidade Federal de São Paulo (UNIFESP)
ABSTRACT
OBJECTIVE: to assess the association between speech-language disorders related to hearing loss and to describe it regarding gender, chief complaint, and type and degree of hearing loss.
METHODS: retrospective study of 482 archives of patients with speech-language disorders between July 1998 and July 2008. Information on age, gender, area of residence, chief complaint / manifestation of language impairment, etiologic diagnosis, and speech-language and hearing impairment was collected.
RESULTS: Most were male patients (56%) aged three to five (32,8%) and six to 11 years (32,8%). Their chief complaints included oral language impairment (57%); sensorineural hearing loss (66,3%); profound hearing loss bilateral (32,8%); and an organic etiology (41,7%). A correlation between language disorder with the level of hearing loss and complaint of language was statistically significant (p < 0,001).
CONCLUSION: the study found an association between language disorder and degree of hearing loss and language complaint.
Key words: speech pathology; epidemiology; deafness; hearing loss; language.
INTRODUCTION
Hearing enables one of the greatest higher brain functions in human beings- communication. Sensory limitations due to hearing impairment may favor the co-occurrence of language disorders and thus impact effective communication1, 2.
Human communication is a predominantly sensory-dependent process carried out through auditory perception and decoding of perceived stimuli opening up the possibility of understanding, which are inherent aspects of human language1, 3.
The impact of hearing loss on the development of speech-language skills can be complex and diverse. Although individuals with hearing loss may show a wide variety of disturbances, the higher the degree of hearing loss and the earlier its onset, the greater the negative impact on development. Thus, diagnosis and intervention as early as possible is required to minimize these impacts4, 5.
In addition to affecting language and communication hearing loss can have an impact on the different biopsychosocial interfaces individuals are exposed to6-8. It is thus crucial to fully understand the many variables involved in language and hearing disorders so that more effective management and treatment actions can be taken to minimize their effects6.
There are few studies in the literature on the prevalence and characteristics of speech-language disorders associated with hearing loss6. The objective of this study was describing the characteristics of patients with speech-language disorders related to hearing loss and to assess their association with gender, chief complaint, and type and degree of hearing loss.
METHODS
Retrospective study conducted in a sample of 536 patients attending an outpatient public clinic in the city of São Paulo, Brazil. Data was collected from archives of patients seen between July 1998 and July 2008.
Patients with archives with information on any language disorder were included in the study. There were excluded archives with more than 20% missing data. There were collected information on age, gender, area of residence, chief complaint (manifestation of language impairment), etiologic diagnosis, and language and hearing impairment.
The variable age was divided by age groups (zero to two; three to five; six to 11; 12 to 19; 20 to 39; 40 to 64; and 65 or more)9. Gender was categorized as male or female. The areas of residence in the city of São Paulo were divided as follows: downtown, North, East, South, West, and other (residents from outside the city of São Paulo).
Data on the chief complaint were categorized based on type of manifestation of language impairment (oral, written, or both). The etiologic diagnosis was divided into organic, functional, and organic and functional.
Language impairment was categorized based on time of disruption of the language process: language acquisition / maturation; development / learning; or encompass / individuation10.
A hearing examination was performed in both ears separately. Any changes were classified according to type of hearing loss (sensorineural; conductive; mixed; or normal), degree (mild, moderate, severe, and profound); and involvement (unilateral or bilateral).
In the event of missing information or hard to identify data were recorded as "unknown." This study was reviewed and approved by the institutional review board of the Universidade Federal de São Paulo (UNIFESP) (protocol no. 0915/09).
Data were tabulated and then analyzed using the Statistical Package for Social Sciences (SPSS) v. 16.0, Minitab Statistical Software v. 15 and Microsoft Office Excel 2007. The following statistical tests were performed in the analyses: test for equality of two proportions, chi-square test for independence, means and 95% confidence intervals and p-values. The level of significance was set at 5% (p < 0.05).
RESULTS
A total of 536 archives were reviewed but 53 were excluded due to missing data and no reporting of a language disorder. The final sample consisted of data collected from 482 archives.
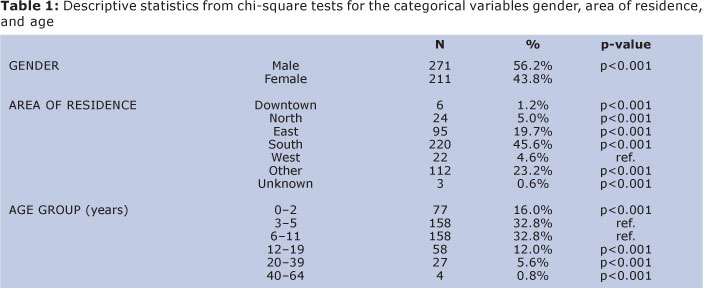
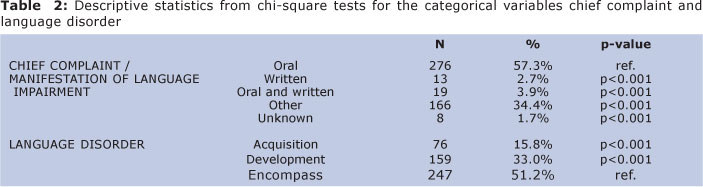
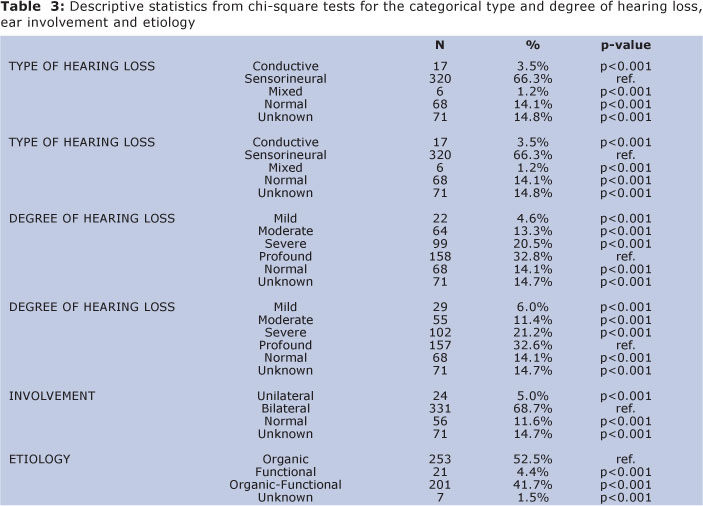
Tables 1, 2 and 3 show the relative frequency distribution (percentages) of all study variables, taking Reference (Ref.) p-values of comparisons of each level of response compared to the most prevalent.
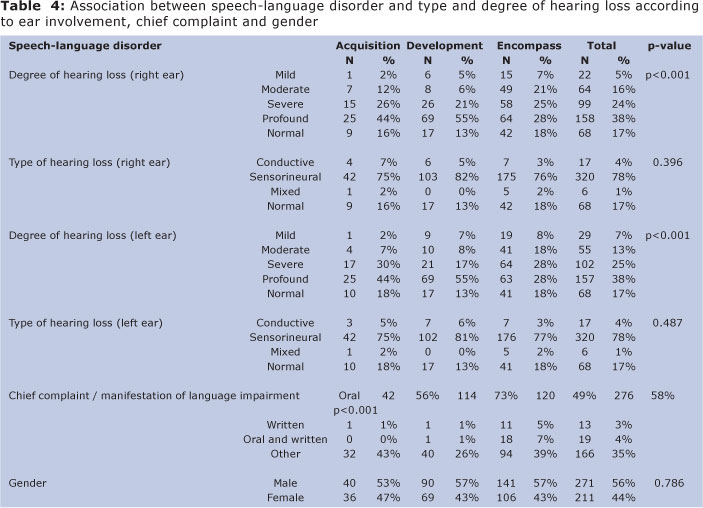
The analysis of the association between the variables type and degree of hearing loss, chief complaint and gender and language impairment is presented in Table 4. A correlation between language impairment and bilateral hearing loss was statistically significant (p < 0.001). In addition, we found a statistically significant association between language impairment and chief complaint (p < 0.001).
DISCUSSION
An intact peripheral and central auditory system is required for the acquisition and development of normal language. It is also crucial for an individual's adequate psychosocial development allowing them to express their thoughts, feelings and desires and acquire life experiences and knowledge11, 12.
It was observed predominance of male patients with language impairment and hearing loss that is in agreement with that reported by other authors13-15. However, this find might be connected with the demand by the service. This study considered that predominance is not associated straightly with the language impairment.
Studies have questioned the association between gender and higher risk of language disorders6, 16 showing that gender is unlikely to affect the type of language disorder. It is a major evidence refuting gender as a risk factor for the occurrence of language disorders, especially when associated with hearing impairment.
The sample studied consisted primarily of residents living in the health service coverage area, which was expected. People tend to seek care within their own area residence17, and only go to seek care elsewhere when have no choice or care services are not available18.
Although age range was wide in this study (1 to 57 years old), there was a greater proportion of preschool and school age patients (3 to 12 years old). At school these children are faced with increased linguistic demands and linguistic differences become more evident19. This finding is corroborated by other studies18, 19.
Language complaints reported by the patients and their family were mostly a of oral language disorder, which is consistent with findings of an earlier study19, 20. These complaints are a manifestation of symptoms and a professional can establish a relationship between the impairment and environmental, social and family factors that can potentially affect their condition6.
The language learning process occurs through biological maturation and interaction within the environment. These two factors are prerequisites for acquisition, development and encompass for satisfactory process of adequate language. Bearing in mind that hearing loss greatly affects one's interaction with the environment, this study found a higher proportion of language disorders observed in encompass stage in the language's process10,21 because we evaluated patients with delayed diagnosis, the same occurs with wearing hearing aids and intervention.
Early diagnosis of hearing loss in children should be made through Universal Newborn Hearing Screening (UNHS) programs but also later hearing screenings of school-aged children because children with hearing loss risk, although with normal hearing at birth, may develop a hearing loss later in life and/or mild hearing loss that is present at birth may progress to more severe forms4, 22.
Complaints of oral language disorders were also seen during the three stages of the language process (acquisition, development and encompass). This is because hearing loss becomes evident when its consequences arise as impaired oral language23. In addition, complaints of oral language disorders may have a greater impact on daily activities regardless of age and are more easily detected even by lay people.
When a language disorder occurs with hearing loss a thorough multidisciplinary evaluation is crucial to accurately determine the type of communication disorder and any impairments associated 2.
The most common type of hearing loss found in this study was profound sensorineural loss bilateral of organic origin, which is corroborated by other studies1, 14. Organic changes may be caused by meningitis, congenital rubella, ototoxic drugs, hyperbilirubinemia, among others24, which can lead to hearing loss with similar characteristics as described in the present study.
Hearing and language are correlated interdependent functions, and this study showed a statistically significant association between degree of hearing loss and language impairment. It was found a greater prevalence of profound hearing loss during the stages of language acquisition, development and encompass. A direct impact of profound hearing loss on language was reported in a previous study that found more significant language impairment with profound than mild, moderate and severe loss2, 23.
However, the type of hearing loss was not associated with language impairment. Changes in the auditory pathway directly affect language acquisition, development, and encompass4. Conductive abnormalities result in a reduction of the sound intensity that reaches the cochlea, and sounds are perceived as low and muffled lacking in depth, richness, and dimension. All these factors show that this condition may also have a great impact on language acquisition and development11.
In conclusion, our results show that language impairment is directly associated with the degree of hearing loss and language complaints. The profile of patients with language impairment related to hearing loss includes profound sensorineural hearing loss bilateral by organic origin; chief complaint of an oral language disorder; and higher prevalence among male children aged three to five and six to 11 years, corresponding to the stages of language development and linguistic ability.
REFERÊNCIAS
1. Silva LPA, Queiros F, Lima I. Etiology of hearing impairment in children and adolescents of a reference center APADA in the city of Salvador, state of Bahia. Braz J Otorhinolaryngol. 2006;72(1):33-6. http://dx.doi.org/10.1590/S0034-72992006000100006 [ Links ]
2. Psillas G, Psifidis A, Antoniadou-Hitoglou M, Kouloulas A. Hearing assessment in pre-school children with speech delay. Auris Nasus Larynx. 2006;33(3):259-63. http://dx.doi.org/10.1016/j.anl.2005.11.013 [ Links ]
3. Zocoli AMF, Riechel FC; Zeigelboim BS, Marques JM. Audição: abordagem do pediatra acerca dessa temática. Rev. Bras. Otorrinolaringol. 2006;72(5):617-623. http://dx.doi.org/10.1590/S0034-72992006000500007 [ Links ]
4. Vieira ABC, Macedo, LR. O diagnóstico da perda auditiva na infância. Pediatria (São Paulo). 2007;29(1):43-49. [ Links ]
5. Fernandes DMZ, Lima MCMP, Gonçalves VMG, Francozo MFC. Acompanhamento do desenvolvimento da linguagem de lactentes de risco para surdez. Rev. Soc. Bras. Fonoaudiol. 2011;16(1):30-36. http://dx.doi.org/10.1590/S1516-80342011000100007 [ Links ]
6. Goulart BNG, Chiari BM. Prevalência de distúrbios de fala em escolares e seus fatores associados. Rev Saúde Pública. 2007;41(5):726-31. http://dx.doi.org/10.1590/S0034-89102007000500006 [ Links ]
7. Neuber LMB, Do Valle TGM, Palamin MEG. O adolescente e a deficiência auditiva: as relações familiares retratadas no teste do desenho em cores da família. Rev Bras Crescimento Desenvolv Hum [online]. 2008;18(3):321-338. [ Links ]
8. Barker DH, Quittner AL, Fink NE, Eisenberg LS, Tobey EA, Niparko JK; CDaCI Investigative Team. Predicting behavior problems in deaf and hearing children: the influences of language, attention, and parent-child communication. Dev Psychopathol. 2009;21(2):373-92. http://dx.doi.org/10.1017/S0954579409000212 [ Links ]
9. Papalia DE, Olds SW, Feldman RD. Desenvolvimento Humano. Bueno D, trad. 8 nd ed. Porto Alegre: Artmed; 2006. [ Links ]
10. Perissinoto J, Chiari BM. A avaliação como ação precursora do diagnóstico. In: C R F Andrade. (Org.). Fisioterapia, fonoaudiologia e terapia ocupacional em pediatria. 3 nd ed. São Paulo: 2003 [ Links ]
11. Bauer, ILB. Consequências da perda auditiva leve versus diagnóstico precoce (Tese). Porto Alegre: CEFAC, 1999. [ Links ]
12. Nogueira JCR, Mendonça MC. Assessment of hearing in a municipal public school student population. Braz. J. Otorhinolaryngol. 2011;77(6):716-720. http://dx.doi.org/10.1590/S1808-86942011000600007 [ Links ]
13. Lima BPS, Guimarães JATL, Rocha MCG. Características epidemiológicas das alterações de linguagem em um centro fonoaudiológico do primeiro setor. Rev Soc Bras Fonoaudiol. 2008;13(4):376-80. http://dx.doi.org/10.1590/S1516-80342008000400013 [ Links ]
14. Uus K, Bamford J. Effectiveness of population-based newborn hearing screening in England: ages of interventions and profile of cases. Pediatrics. 2006;117(5):e887-93. http://dx.doi.org/10.1542/peds.2005-1064 [ Links ]
15. Pinto MM, Raimundo JC, Samelli AG, Carvalho ACM, Matas CG, Ferrari GMS, et al. Idade no diagnóstico e no início da intervenção de crianças deficientes auditivas em um serviço público de saúde auditiva brasileiro. Arq. Int. Otorrinolaringol. 2012; 16(1): 44-49. http://dx.doi.org/10.7162/S1809-48722012000100006 [ Links ]
16. Rabelo ATV; Alves CRL; Goulart LMHF; Friche AAL; Lemos SMA; Campos FR; et al. Speech disorders in students in Belo Horizonte. J Soc Bras Fonoaudiol. 2011; 23(4): 344-50. http://dx.doi.org/10.1590/S2179-64912011000400009 [ Links ]
17. Baille MF, Arnaud C, Cans C, Grandjean H, du Mazaubrun C, Rumeau-Rouquette C. Prevalence, aetiology, and care of severe and profound hearing loss. Arch Dis Child. 1996;75(2):129-32. http://dx.doi.org/10.1136/adc.75.2.129 [ Links ]
18. Costa RG, Souza LBR. Perfil dos usuários e da demanda pelo serviço da clínica-escola de fonoaudiologia da UFBA. Rev. ciênc. méd. biol. 2009;8(1):53-59. [ Links ]
19. Diniz RD, Bordin R. Demanda em Fonoaudiologia em um serviço público municipal da região sul do Brasil. Rev. Soc. Bras. Fonoaudiol. 2011;16(2):126-131. http://dx.doi.org/10.1590/S1516-80342011000200004 [ Links ]
20. Goulart BNG, Henckel C, Klering CE, Martini M. Fonoaudiologia e promoção da saúde: relato de experiência baseado em visitas domiciliares. Rev CEFAC. 2010;12(5):842-49. http://dx.doi.org/10.1590/S1516-18462010005000095 [ Links ]
21. Carvalho JF, Homem, FCB. A influência do meio na aquisição da linguagem. Fono atual. 2001;4(17):14-16. [ Links ]
22. Vieira EP, Miranda EC, Azevedo MF, Garcia MV. Ocorrência dos indicadores de risco para a deficiência auditiva infantil no decorrer de quatro anos em um programa de triagem auditiva neonatal de um hospital público. Rev. Soc. Bras. Fonoaudiol. 2007; 12(3): 214-220. http://dx.doi.org/10.1590/S1516-80342007000300009 [ Links ]
23. Gatto CI, Tochetto TM. Deficiência auditiva infantil: implicações e soluções. Rev. CEFAC. 2007;9(1):110-115. http://dx.doi.org/10.1590/S1516-18462007000100014 [ Links ]
24. Dunmade AD, Segun-Busari S, Olajide TG, Ologe FE. Profound bilateral sensorineural hearing loss in nigerian children: any shift in etiology? J Deaf Stud Deaf Educ. 2007;12(1):112-8. http://dx.doi.org/10.1093/deafed/enl019 [ Links ]
 Correspondence to:
Correspondence to:
leticianeoli@gmail.com
Manuscript submitted Jul 06 2012,
Accepted for publication Dec 22 2012.

{kind=link}
{kind=link}
{kind=link}
{kind=link}