










Serviços Personalizados
artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282versão On-line ISSN 2175-3598
Rev. bras. crescimento desenvolv. hum. vol.23 no.2 São Paulo 2013
ORIGINAL RESEARCH
Effect of sedentary lifestyle, nutritional status and sex on the flexibility of school children
Maylli Daiani GraciosaI; Jerusa Jordão CoelhoI; Letícia Miranda Resende da CostaII; Daiane Lazzeri de MedeirosII; Micheli MartinelloIII; Lilian Gerdi Kittel RiesIV
IStudent of Graduation in Physiotherapy / College of Health Science - CEFID / Santa Catarina State University - UDESC
IIStudent of the Master's Program Graduate in Physiotherapy / College of Health Science - CEFID / Santa Catarina State University - UDESC
IIIMaster of Science in Human Movement / College of Health Science - CEFID / Santa Catarina State University - UDESC
IVProfessor of the Graduate Program in Physiotherapy / College of Health Science - CEFID / Santa Catarina State University - UDESC
ABSTRACT
INTRODUCTION: assart-day life habits have led to a more sedentary lifestyle, contributing to increased obesity. In view of these changes, it is necessary to understand whether the flexibility of the individual has also been influenced.
OBJECTIVE: to investigate the influence of sex, sedentary lifestyle and nutritional status on the flexibility of elementary school children.
METHODS: 60 cheldren of both sexes aged five to 14 years were divided into a normal flexibility group (n = 21) and a reduced flexibility group (n = 39). Flexibility was evaluated by photogrammetry using the straight leg raise test, considering the leg angle. The physical activity level was evaluated using the Physical Activity Questionnaire for Older Children, and nutritional status was assessed by Body Mass Index for age and sex.
RESULTS: the normal flexibility group and the reduced flexibility group presented no significant differences regarding age, weight or height (p > 0.05). No differences were found (p > 0.05) in leg angle between the active and sedentary groups, the obese and nonobese or between males and females.
CONCLUSIONS: sex, sedentary lifestyle and nutritional status exercized to influence on the flexibility of students.
Key words: pliability; sex; body mass index; motor activity; child.
INTRODUCTION
Flexibility is a physiological characteristic that allows an individual to execute voluntary movements of maximum joint angular amplitude within morphological limits1, free of pain and restrictions2. This physical attribute results from an interrelationship between ligaments, muscles, tendons, skin and joints3. The shortening of these structures results in a limited range of motion2, and may lead to a number of consequences for individuals with this limitation.
A good flexibility level can greatly impact an individual's quality of life. Among its benefits are: improved skills in daily activities and sports; reduced risk of musculotendinous injuries and incidence of muscle pain, reduced stress and improved posture3. In addition, psychosocial factors and fitness are crucial for stimulating physical activity4, essential for health.
In recent decades, however, constant technological advances5 and an increasing lack of security in urban areas have contributed to a sedentary lifestyle6 in whir by activities such as watching television, playing video games and spending long hours on the computer predominate7,8. This lifestyle, coupled with inadequate diet, has contributed to increased overweight and obesity among children. The increase in these indexes is becoming a public health problem since their consequences affect overall quality of life for these individuals9.
Therefore, a better understanding of the influences that these changes have on flexibility levels is also necessary, since this characteristic plays a fundamental role in everyday life. A number of studies have demonstrated that flexibility is influenced by nutritional status10-12, physical activity levels3 and sex3,10,13,14. However, other studies have reported controversial results regarding nutritional status15-17, physical activity level18 and sex19,20.
There is no consensus as to whether the changes resulting from nutritional transition and increased sedentarism and sex are factors that can influence the physical fitness of children, especially regarding flexibility. Considering the important benefits of flexibility for quality of life during childhood, it is important to investigate the possible influence of the above-mentioned factors on this parameter.
Thus, the objective of this study was to verify whether sex, sedentary lifestyle and nutritional status influence student's flexibility level.
METHODS
Subjects
The sample of this cross-sectional survey included 60 school cheldren's of both sexes between the ages of five and 14 years old who were enrolled in elementary schools in Florianópolis, Brazil. children with special needs, i.e. who participated in any orthopedic treatment and/or physical therapy, were excluded.
The school children were divided into two groups according to leg angle measurement on the straight leg raise test: Group 1 (G1), normal flexibility, included 21 subjects with values > 65°; Group 2 (G2), reduced flexibility, included 39 subjects with values < 65°21.
The Human Research Ethics Committee approved this research project in Protocol 165/2011. The participating children's parents or guardians were informed about the objectives and procedures of this study and signed an informed consent form.
Instruments
The instruments used in this study were: anamnesis, the physical activity questionnaire for children (PAQ-C) and photogrammetry. Anamnesis was used to characterize the sample and consisted of anthropometric data and inclusion and exclusion criteria. The body mass and height of the children were used to calculate the Body Mass Index (BMI), which was used to determine nutritional status. On the basis of the BMI adjusted for age and sex. The children were classified, as either underweight (below the fifth percentile), normal weight (between the fifth and 85th percentiles), overweight (between the 85th and 94th percentile) or obese (> the 95th percentile)22. According to this classification, the sample was divided into the following groups for data analysis: an obese group (childrens classified as obese and overweight) and a nonobese group (classified as underweight and normal weight).
The PAQ-C, validated by Crocker et al.23, is a questionnaire used to assess the physical activity level of children and adolescents over the seven previous days. It consists of nine questions about sports, games and physical activities at school and during leisure time. Each question has a value of one to five and the final score is obtained by averaging the value of all the responses. The results range from very sedentary (1) to highly active (5)24. The children were classified as active when they obtain scores > 3 and sedentary when scoring < 324.
The straight leg raise test in conjunction with photogrammetry is considered a useful and reliable method for evaluating flexibility21. In this technique, angular measurements were used to categorize the subjects' flexibility. This analysis was performed using SAPO, a highly reliable software program25.
Procedures
After completing the questionnaires, anamnesis was carried out. The school children were asked to wear appropriate clothes and remain barefoot. Anthropometric measurements were taken with the student in the standing position with feet supported forward and arms relaxed alongside the body. Body weight was measured using a digital scale (Filizola) with 100g precision. A stadiometer was used to measure the height.
The photogrammetry procedure involved a digital camera (SANYO VPC-HD2000) fixed to a tripod on level ground at a height of 85 cm three meters from a gurney measuring 1.82 m in length, 82 cm high and 60.5 cm wide. As a vertical axis reference, a 100 cm plumb line was used. White 1 cm spherical markers were attached bilaterally with double-sided tape to the subjects in order to identify the greater trochanter of the femur and the lateral malleolus as reference points.
After anamnesis, the straight leg raise test was conducted as follows: the child was placed on a stretcher in the supine position with legs extended and arms flexed with the hands behind the head. During the test the thigh of the contralateral limb was secured to stabilize movement. The test was performed on both legs. A photo was taken when the subjects began to feel muscular tension in the posterior region of the leg, before attempting a hip rotation of the limb under evaluation.
Two different, previously trained evaluators took images and calculated the angles so that interrater reliability could be checked. Sagittal plane analysis was carried out by measuring the leg angle (intersection between the leg segment and the horizontal line of the gurney)21 (Figure 1).
Statistical analysis
Descriptive statistics were used for data processing (mean and standard deviation). Interrater reliability for flexibility measurements (leg angle) was assessed using the intraclass correlation coefficient (ICC). The difference between the leg angle measurements of the left and right legs was also evaluated with Student's t-test.
The normality of the data was tested using the Kolmogorov-Smirnov test. Student's t-test for independent samples was used to determine the difference between the average anthropometric characteristics and leg angles of the groups with normal and reduced flexibility. The same test was used to compare the means of the angles of the leg between the active and sedentary groups, between obese and non-obese groups and between males and females. In order to verify the existence of an association between the groups with normal and reduced flexibility factors and physical activity, nutritional status and sex bivariate logistic regression analysis was applied. The effect of the explanatory factors on the occurrence of reduced flexibility was assessed by calculating the odds ratio (OR) with a confidence interval of 95%.
The Statistical Package for the Social Sciences (SPSS) version 17.0 for Windows used for the statistical analysis, and a significance level of 5% (p<0.05) (with a two-tailed distribution) was adopted for all procedures.
RESULTS
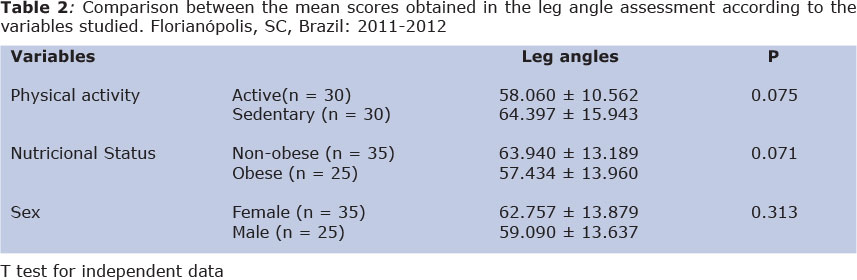
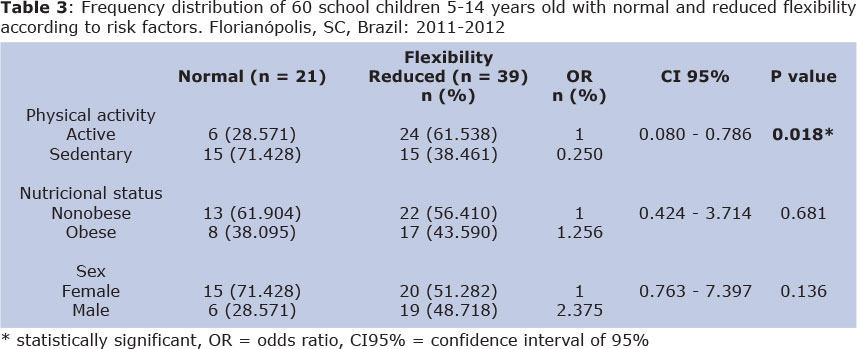
Of the 60 school children assessed, 21 were classified as having normal flexibility and 39 as having reduced flexibility. Table 1 describes the anthropometric characteristics and leg angles of the groups with normal and reduced flexibility. The mean leg angle scores of the active and sedentary groups, nonobese and obese groups and both sexes are compared in table 2. The results of the binary logistic regression are presented in table 3.
DISCUSSION
It was observed that the groups with normal and reduced flexibility were homogeneous. There were no statistically significant differences between the groups in terms of age, weight or height (p>0.05). The results also show that the leg angle was significantly lower in G2 (reduced flexibility) than G1 (the expected results for the groups were divided in accordance with the angle).
Since high reliability for the leg angle measurements was obtained between the two evaluators (ICC>0.960, p<0.000), their arithmetic mean was considered. There were no significant differences (p>0.05) between left and right leg measurements, so an average for the two members was used. No significant differences (p>0.05) in leg angle were observed between the active and sedentary groups, the nonobese and obese or between males and females. A predictive association was observed for the physical activity factor (odds ratio < 1.00). Sedentary students had a 2.5 x greater chance of normal flexibility.
A restricted range of hip motion is related to decreased flexibility of the hamstrings26. In this study, hamstring flexibility was measured with the straight leg raise test. As expected, there was a significant difference in leg angles between the groups with normal and reduced flexibility, with average values of 76° and 53°, respectively. Although the present study used the same classification parameters as Carregaro et al.21, it was observed that the average leg elevation was greater for both groups. The above-mentioned study found mean leg elevation values of 53º and 33º, respectively, for its normal and reduced flexibility groups. However, those values were for individuals between 18 and 35 years old, whereas the subjects evaluated in this study. The different results found in these studies may be due to the chronological age of the participants, since it has been demonstrated that flexibility decreases with advancing age14.
It was expected that the physical activity level would positively influence leg flexibility. Nevertheless, the results of this study did not confirm this hypothesis. Active students had a lower, although not significantly so, leg angle than the sedentary group. Regarding the comparative analysis of factors between children with normal and reduced flexibility, we found an association between physical activity and reduced flexibility.
Flexibility results from the sit-and-reach test in adolescents older than 1527 and an index of seven joints of the human body18 also indicated no differences between individuals with different levels of physical activity. The results of the present study showed that leg flexibility in children between five and 14 years old cannot be differentiated according to physical activity level and therefore must be considered as an independent factor27.
However, the association found between active students and reduced flexibility is curious. It is known that regular physical activity provides physiological and psychological benefits, and the aerobic components, flexibility and muscle overload it entails warrant respect28. Therefore, the importance of including exercises involving physical aptitude during physical education classes must be considered. It is worth mentioning that, at least in Brazil, the content of most physical education classes is limited to teaching the techniques, rules and history of different sports, especially handball, basketball, volleyball and soccer29.
Flexibility can be influenced by the type of exercise performed, i.e., the type of movement most often employed in certain activities can result in better mechanical efficiency and specific perfor-mance18. However, the evaluation methodology in this study was limited in that it did not distinguish between the type of physical activity in which the subjects were involved. Thus, to evaluate such influence, it would be necessary to consider the type of physical activity performed as well as specific categories of movements and the joints most involved in such activity. The study was limited to assessing flexibility by means of the hip flexion angle with the leg extended. It was assumed that those who achieved a better score in the test participated in activities involving large movements of this joint.
In agreement with other studies19,20, no difference in the leg angles was observed between the sexes. Although some authors have reported such a difference10,13,14, these results are controversial. Bim and Nardo10 assessed the flexibility of adolescents 16 to 17 years old with the sit-and-reach test and concluded that male performance was better. Penha and João13 found the same result when evaluating children seven to eight years old by the fingertip-to-floor test. Pagnussat & Paganotto14, using the hamstring length test with a group of six- to 13-year-olds, reported that females were more flexible than males. Further studies are necessary to determine whether sex influences flexibility. Other sex-factors could affect this parameter and should be considered. Sex differences could be due to anatomical and physiological differences2, genetic variation and sociocultural factors19.
There was no difference in leg angle values between the obese and nonobese students, which corroborated Contel et al., Kim et al. and Minato et al.15-17. On the other hand, other studies using the sit-and-reach test found different results11,12,30. It was observed that in cases of overweight and obesity, fat accumulation at the joints could increase friction and reduce myoarticular stretching ability19.
In the present study, the only classification method used to categorize the subjects' nutritional profile was BMI adjusted for age and sex, which cannot discriminate between lean and fat mass. Thus, it was not possible to determine fat percentage. For this reason, some students classified as having reduced flexibility could have had a BMI similar to those considered to have normal flexibility, although with different percentages of fat. However, it is impossible to confirm this hypothesis, since this component was not assessed in this study.
Furthermore, it is known that flexibility can be influenced by factors such as biological individuality, somatotype17, the type of physical activity in which the individual is involved and age3. It could be presumed, therefore, that flexibility is influenced by the sum of all these factors. Thus, when the actual existence of these influences is verified, it becomes necessary to control all the variables that could affect flexibility levels.
More than half of the children in the present study were classified as having reduced flexibility according to the classification parameters of Carregaro et al21. Pelegrini et al31. assessed 7507 children aged seven to 10 years from all the regions of Brazil with the sit-and-reach test and also found that the majority did not attain the minimum fle-xibility criteria established for health. Other studies10,32,33 have also found the same results, so it may be that there is a trend among brazilian children and adolescents towards low levels of physical fitness.
Some authors have stated that this tendency may be related to increasing physical inactivity in children31,33, but the present study found that a sedentary lifestyle cannot be considered a risk factor for flexibility deficits. Nevertheless, what we can take into account are the types of activities that predominate in these individuals' routines.
It is known that due to the constant advances in technology in recent decades, children have become accustomed to remaining seated in front of computers, television and video games for extended periods of time7,8. Moreover, the sitting posture also predominates during the school day. One study found that individuals who spend much of their time seated have lower overall flexibility of the posterior chain34. This occurs because such a posture tends to shorten the posterior muscles of the lower limbs, especially the hamstrings and gastrocnemius34. Thus, it is assumed that the subjects evaluated in this study who had low levels of flexibility may be spending too much time in this position.
The flexibility results presented in this study merit attention, since this component is important for promoting better health and reducing pain levels, risk of injury and stress3. Furthermore, when there is limited range of motion, sports performance and activities of daily living may be impaired35. Moreover, lower levels of physical fitness among children can contribute to inactivity, leading to reduced participation in physical activity and games36 and resulting in a less healthy lifestyle.
Thus, the need to include physical fitness as an essential component of physical education classes should be emphasized. Such programs, besides addressing social aspects and motor coordination skills, should also include exercises to improve flexibility, muscle strength and cardiorespiratory endurance. By improving fundamental movement skills, it is likely that children will be more willing to participate in activities that involve physical fitness components36. Thus, when designing an exercise program for this population, activities that promote improved levels of all physical fitness components should be included so that children are encouraged to develop a more physically active and healthy lifestyle37.
In conclusion, sex, sedentary lifestyle and nutritional status were did not found to influence the fle-0xibility of the children we studied and that reduced flexibility was prevalent.
REFERENCES
1. Dantas EHM. Alongamento & flexionamento. 4ª ed. Rio de Janeiro: Shape; 1998. 33p. [ Links ]
2. Polachini LO, Fuzasaki L, Tamaso M, Tellini GG, Masieiro D. Comparative study between three methods for evaluating of hamstring shortening. Rev. bras. fisioter. 2005;9(2):187-93. [ Links ]
3. Glaner MF. The importance of health-related physical fitness. Rev Bras Cineantropom Desempenho Hum. 2003;5(2):75-85. [ Links ]
4. Juzwiak CR, Paschoal V, Lopez FA. Nutrition and physical activity. J. pediatr. 2000; 76(3): 349-358. [ Links ]
5. Giugliano R, Carneiro EC. Factors associated with obesity in school children. J. pediatr. 2004; 80(1): 17-22. [ Links ]
6. Reilly JJ. Physical activity, sedentary behaviour and energy balance in the preschool child: opportunities for early obesity prevention. Proc Nutr Soc. 2008;67:317 - 325. [ Links ]
7. Lazzoli JK, Nóbrega ACL, Carvalho T, Oliveira MAB, Teixeira Jac, Leitão MB et al. Position statement of the Brazilian Society of Sports Medicine: physical activity and health in children and adolescents. Rev. bras. med. esporte. 1998;4(4):107-109. [ Links ]
8. Cardon G, Van Cauwenberghe E, De Bourdeaudhuij I. What do we know about physical activity in infants and toddlers: a review of the literature and future research directions. Sci. sports. 2011;26:127-130. [ Links ]
9. Pereira LO, Francischi RP, Lancha AH. Obesity: Dietary Intake, Sedentarism and Insulin Resistance. Arq Bras Endocrinol Metab. 2003;47(2):111-127. [ Links ]
10. Bim RH, Junior NN. Fitness related to health of the adolescent trainees of the State University of Maringá. Acta Sci Health Sci. 2005;27(1): 77- 85. [ Links ]
11. Deforche B, Lefevre J, Bourdeaudhuij I, Hills AP, Duquet W, Bouckaert J. Physical Fitness and Physical Activity in Obese and Nonobese Flemish Youth. Obes Res. 2003;11(3):434-441. [ Links ]
12. Gouveia ER, Freitas DL, Maia JA, Beunen GP, Claessens AL, Marques AT, Thomis MA, Almeida SM, Sousa AM, Lefevre JA. Physical activity, fitness and overweight in children and adolescents: the Madeira Growth Study. Rev Bras de Educ Fís Esp. 2007;21(2):95-106. [ Links ]
13. Penha PJ, João SMA. Muscle flexibility assessment among boys and girls aged 7 and 8 years old. Fisioter e Pesq. 2008; 15(4): 387-91. [ Links ]
14. Pagnussat AS, Paganotto KM. Study of lumbar curvature in the structural development phase. Fisioter Mov. 2008;21(1):39-46. [ Links ]
15. Contel M, Gonçalvez A, Aragon F, Padovani CR. Influence of body weight on fitness in adolescents: study in high school students in Sorocaba/SP. Rev. bras. med. esporte. 2000;6(2):44-49. [ Links ]
16. Kim J, Aviva M, Garrett MF, Matthew WG, Virginia C, Ellen K, Robert M, Karen EP. Relationship of physical fitness to prevalence and incidence of overweight among schoolchildren. Obes Res. 2005;13:1246 - 1254. [ Links ]
17. Minatto G, Ribeiro RR, Junior AA, Santos KD. Influence of age, sexual maturation, anthropometric variables and body composition on flexibility. Rev Bras Cineantropom Desempenho Hum. 2010;12(3):151-158. [ Links ]
18. Melo FAP, Oliveira MF, Almeida MB. Physical activity level does note identify flexibility level. Rev Bras Ativ Fis Saúde. 2009;14(1):48-54. [ Links ]
19. Silva DJL, Santos JAR, Oliveira BMPM. Flexibility among adolescents - A contribution to global evaluation. Rev Bras Cineantropom Desempenho Hum. 2006;8(1):72-79. [ Links ]
20. Okano AH, Altimari LR, Dodero SR, Coelho CF, Almeida PBL, Cyrino ES. Comparisons between the motor performance of children of different sex and ethnic groups. Rev. Bras. Ciên. e Mov. 2001;9(3):39-44. [ Links ]
21. Carregaro RL, Silva LCCB, Gil Coury HJC. Comparison between two clinical tests for evaluating the flexibility of the posterior muscles of the thigh. Rev. bras. fisioter. 2007;11(2):139-145. [ Links ]
22. Center for Disease Control and Prevention - CDC. National Center for Chronic Disease Prevention and Health Promotion - Nutrition and Physical Activity. Body mass index-for-age (children). Disponível em: <http://www.cdc.gov/nccdphp/dnpa/bmi-for-age.htm> Acesso em: 08/5/2012. [ Links ]
23. Kowalski KC, Crocker PRE, Faulkner RR. Validation of the Physical Activity Questionnaire for Older Children. Pediatr Exerc Sci. 1997;9:174-186. [ Links ]
24. Silva RCR, Malina, RM. Level of physical activity in adolescents from Niterói, Rio de Janeiro, Brazil. Cad Saúde Pública. 2000; 16(4): 1091-1097. [ Links ]
25. Guariglia DA, Pereira LM, Pereira HM, Cardoso JR. Reliability and usability assessment of three different softwares for photogrammetric analysis of hip flexion angle. Fisioter e Pesq. 2011;18(3):247-251. [ Links ]
26. Magnusson SP, Simonsen EB, Aagaard P, Boesen J, Johannsen F, Kjaer M. Determinants of musculoskeletal flexibility: Viscoelastic properties, cross-sectional area, EMG and stretch tolerance. Scand J Med Sci Sports. 1997;7:195 - 202. [ Links ]
27. Guedes DP, Guedes JERP, Barbosa DS, Oliveira JA. Habitual physical activity and health-related physical fitness in adolescents. Rev. Bras. Ciên. e Mov. 2002;10(1):13-21. [ Links ]
28. Carvalho T, Nóbrega ACL, Lazzoli JK, Magni JRT, Rezende L, Drummond FA, et al. Position statement of the Brazilian Society of Sports Medicine: physical activity and health. Rev. bras. med. esporte. 1996;2:79-81. [ Links ]
29. Ferreira MS. Fitness and health in physical education: enlarging the focus. Rev. Bras. de Ciênc. Esporte. 2001; 22(2):41-54. [ Links ]
30. Andreasi, Michelin E, Rinaldi AEM, Burini RC. Physical fitness and association with anthropometric measurements in 7 to 15 year-old school children. J. pediatr. 2010; 86: 497-502. [ Links ]
31. Pelegrini A, Silva DAS, Petroski EL, Glaner MF. Health-Related Physical Fitness in Brasilian Schoolchildren: Data From The Brazil Sport Pro-gram. Rev Bras Med Esporte 2011;17(2):92-6. [ Links ]
32. Bergmann GG, Araújo MLB, Garlipp DC, Lorenzi TDC, Gaya A. Annual alteration in the growth and health-related physical fitness of the school children. Rev Bras Cineantropom Desempenho Hum 2005;7(2):55-61. [ Links ]
33. Burgos MS, R CP, Tornquist L, Piccin AS, Reckziegel MB, Pohl HH, Burgos LT. Health-related physical fitness profile of children and adolescents aged 7-17. J Health Sci Inst. 2012; 30(2): 171-5. [ Links ]
34. SACCO, I. C. N. et al. The influence of occupation on overall flexibility and lower limb and lumbar range of motion. Rev Bras Cineantropom Desempenho Hum. 2009; 11(1): 51-58. [ Links ]
35. Almeida TT, Jabur NM. Myths and trues about flexibility: reflections about the stretch training in the health of human being. Motricidade. 2007; 3(1): 337-344. [ Links ]
36. Berleze A, Haeffner LSB, Valentini NC. Motor performance of obese children: An investigation of the process anda product of basic motor abilities. Rev Bras Cineantropom Desempenho Hum. 2007; 9(2): 134-144. [ Links ]
37. Greguol M, Rose Júnior DD. Health physical fitness of blind adolescents in regular and special schools. Rev Bras Crescimento Desenvolvimento Hum. 2009; 19(1):42-53. [ Links ]
 Correspondence to:
Correspondence to:
maygraciosa@gmail.com
Manuscript submitted Oct 20 2012., a
Accepted for publication Mar 20 2013.

{kind=link}
{kind=link}
{kind=link}
{kind=link}