










Serviços Personalizados
artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282versão On-line ISSN 2175-3598
Rev. bras. crescimento desenvolv. hum. vol.23 no.2 São Paulo 2013
ORIGINAL RESEARCH
Body composition and chest expansion of type II and III spinal muscular atrophy patients
Raíssa Christina Mendes de SousaI; Cristina Márcia DiasI; Susana Ortiz CostaI; Arthur de Sá FerreiraI; Carla Peixoto Vinha de SouzaII; Alexandra Prufer de Queiroz Campos AraújoII; Míriam Raquel Meira MainentiI, II
IAugusto Motta University Center (UNISUAM): Postgraduate Program of Rehabilitation Sciences - Praça das Nações, 34, 3º floor Bonsucesso - Rio de Janeiro - Brazil
IIFederal University of Rio de Janeiro (UFRJ): Pediatrics Department, Institute of Child Health and Pediatrics Martagão Gesteira (IPPMG) Rua Bruno Lobo, 50. Cidade Universitária, Campus do Fundão - Rio de Janeiro - Brazil
ABSTRACT
INTRODUCTION: spinal muscular atrophy patients present muscle weakness, orthopedic problems, nutritional complications and respiratory impairment. Lean mass and fat mass modifications are also expected in this population.
OBJECTIVE: to verify the body composition and chest expansion of type II and III spinal muscular atrophy patients.
METHODS: fourteen individuals were evaluated: seven patients in Group I of 9 (7-12) years of age, weighing 29.7 (23.5-60.0) kg; and seven children without the disease in Group II of 9 (9-12) years, weighing 31.0 (27.8-54.1) kg. Patients' monofrequency bioelectrical impedance was used for analyze body composition. Chest, hip and abdominal girths were measured by a flexible steel tape. The SPSS program was used to statistical analysis (p < 0.05).
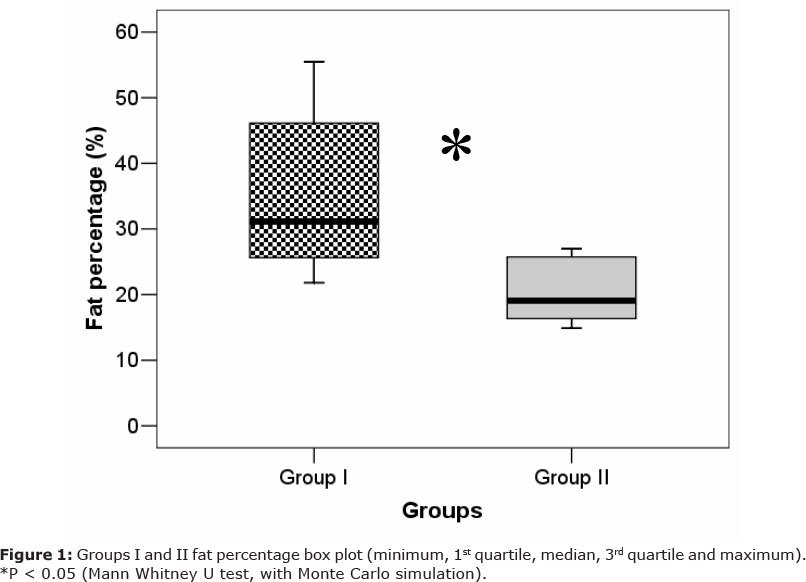
RESULTS: patients presented higher impedance: 1416.9 (850.5-1559.1) vs 788.0 (683.6-853.8), P < 0.05; and fat percentage: 31.2 (23.9-46.6) vs 19.1 (14.9-27.0)%, P < 0.05. The difference between forced inspiration and forced expiration thorax girth was smaller for patients when comparing to Group II: 3.0 (0.8-4.4) vs. 5.0 (3.9-6.5) cm, P<0.05.
CONCLUSIONS: patients with spinal muscular atrophy presented higher adiposity and lower chest expansion.
Key words: neuromuscular diseases; electric impedance; body fat distribution; anthropometry; lung.
INTRODUCTION
Spinal muscular atrophy (SMA) is a recessive, autosomal neuromuscular disease characterized by degeneration of anterior horn spinal cord motor cells and brain stem neurons1-5. It is classified by disease severity and the age at on set of symptoms, namely type I for the most severe cases and type IV for those presenting few complications1,3,6-8. Type II SMA infants get to three point of sitting independent and present thoracic deformity because of muscle weakness, whide causes postural deviations. Type III SMA onset occurs in older children. Patients with type III get to three point of walking, wether or not they maintain this ability throughout adulthood1-3,6,7. SMA patients present progressive symmetrical proximal weakness and hypotonia1-4,6,8, but there is no sensory abnormality7. Besides muscle weakness, respiratory9, orthopedic5, and nutritional10-12 problems are particularly note wortley.
Among the methods used to evaluate body composition in children, bioelectrical impedance stands out as a noninvasive and painless method, which has already been adopted by other authors while evaluating SMA patients13, or children and adolescents without the disease14-16. Body girth measurements are frequently used in clinical practice17,18 due to their practical character and low price. Thoracic girth has already been associated with pulmonary function19, without any intention of replacyng the standard spirometry measurements, used for a more frequent follow up of patients' pulmonary function.
SMA children suffer from stunted development due to nutritional, muscular, postural and respiratory alterations. Body composition assessment in these patients is proposed by Caromano et al.20, since they state that there is a correlation between fat percentage and muscle strength in neuromuscular patients. There are few studies assessing neuromuscular patients with more specific methods than bioelectrical impedance and anthropometric measurements. Therefore, the aim of this study is verify the body composition and chest expansion of type II and III spinal muscular atrophy patients.
METHODS
Study Protocol and Sample
Seven SMA patients (five with type II and two with type III) were recruited (Group I) from the neuropediatric outpatient clinic of the Institute of Child Health and Pediatrics Martagão Gesteira (IPPMG), Federal University of Rio de Janeiro (UFRJ) and were evaluated at the Postgraduate Program of Rehabilitation Sciences laboratories, Augusto Motta University Center (UNISUAM). To compare data, seven individuals without the disease (Group II, control) had already participated in a previous research project at UNISUAM were selected from Rui Barbosa School (Bonsucesso - Rio de Janeiro, RJ), who had their age, sex, weight and height characteristics being paired with those of the patients (Table 1).
Assessments
Weight
Total body mass measurement was performed with an analog scale (R110, Welmy - Santa Bárbara d'Oeste, São Paulo, Brazil) to the nearest 0.1 kg. The subject was instructed to maintain both feet on the platform, without support and with the entire weight divided between both lower limbs21. For those that could not maintain the upright posture, this measurement was done with another person's help (supporting the patient) and subtracting the weight of the assistant from the total weight measured.
Height
Height was estimated for all participants (Groups I and II) by the equation proposed in the literature for brazilian data22 because a great number of patients could not stand up and had lower limb deformities:
Height (cm) = 63.525
3.237* (S)-0.06904* (A)+1.293*(HS)
Where S = sex (boys = 1; girls = 2); A = age (years) and HS = half span (cm, distance between the sternum and the distal phalange of the third finger, with the flexible steel tape parallel to the clavicle23).
Bioelectrical Impedance
Body composition analysis was performed using a monofrequency bioelectrical impedance analyzer (BIA 310e, Biodynamics, Seattle, Washington, USA). Two electrodes were applied to the dorsal surface of the right hand and two electrodes were placed on the dorsal surface of the right foot. The exam was performed in the supine position and the subjects received standardized recommendations: 1) no alcohol consumption or exercise within 24 hours prior to the test; 2) no caffeine or food consumption for four hours prior to the test; 3) the consumption of two-four glasses of water within the two hours prior to the test; 4) bathroom use within the 30 minutes prior to the assessment. Resistance and reactance values provided by the analyzer were used to estimate the fat-free mass (kg), in a child-specific equation14,15: FFM = 2.33 + 0.588*(H2/I) + + 0.211*W, where FFM = fat-free mass (kg); H = height (cm); I = impedance (Resistance2 + + Reactance2)1/2 (W); W = weight (kg)14. Fat percentage was calculated by the following equations: FM = W - FFM; and %F = (FM/W)*100, where FM = fat mass (kg), W = weight (kg), FFM = fat-free mass (kg), and % F = fat percentage (%).
Additionally, body mass index (BMI = W/H2), fat-free mass index (FFMI = FFM/H2) and fat mass index (FMI = FM/H2) were calculated as previously described11.
Girths
A flexible steel tape (Terrazul, Cambuci, São Paulo, Brazil) was used to measure the body girths. The abdomen measurement was made at umbilical level 24 and the hip girth, at the greatest girth, proximately to pubic symphysis21. For those that could not maintain the upright posture, measurements were taken with another person's help, supporting the patient's weight while the examiner performed the measurement. For thoracic girth, the flexible steel tape was placed at the level of the mesosternum, with arms abducted21. For those that could not maintain posture, the measure the upright was performed in a sitting position, preferentially without the use of chair back. Three measure were taken: 1) standard after a normal expiration (Thorax)21; 2) maximal inspiration after a forced inspiration (ThoraxInsp); and 3) maximal expiration after a forced expiration (ThoraxExp). The difference between maximal inspiration and maximal expiration girths was called 'chest expansion'.
Ethical Aspects
Informed consent was obtained from the childrens' parents and the protocol was approved by UNISUAM Ethics Committee before being applied (CAAE: 0028.0.307.000-11).
Statistical Analysis
Nonparametric descriptors and tests with resampling methods were selected because of the small sample size. Data were expressed as median (interquartile range). The Mann Whitney U test was used to compare groups, and the Monte Carlo simulation with 10,000 bootstrap samples was applied. All analyses were realized on the SPSS program, version 13.0, considering a 5% level of significance.
RESULTS
Table 1 summarizes demographic, body composition and girth variables separated by group. The age of Group I was 9 (7-12) years old, similar to Group II: 9 (9-12) years old (P = 0.509). The groups were also comparable for weight, height and BMI: 29.7 (23.5-60.0) vs. 31.0 (27.8-54.1) kg, P = 0.618; 1.45 (1.40-1.58) vs. 1.55 (1.45 - - 1.63) m, P = 0.262; and 15.3 (9.8 - 21.3) vs. 14.0 (12.9-18.8) kg/m2, P = 0.905, respectively.
Group I presented higher values of resistance, impedance and fat percentage. Lower values of chest expansion, fat-free mass and FFMI were also observed, though the last two variables presented no statistical difference (Table 1, Figure 1).
DISCUSSION
Group I composed of SMA patients exhibited higher body adiposity (with both high impedance and body fat percentage) than Group II. Leroy-Willig et al.25 applied magnetic resonance and anthropometric measures to study the body composition of 11 children with neuromuscular diseases. Those authors observed an average of 35.9% of fat (skinfold thickness method), similar to the median values of the present study (31.2%). However, those authors included only three patients with SMA type II and did not investigate the thoracic expansion of their sample.
Higher values of body fat percentage and FMI as compared to regional normative data (paired by sex, age, and ethnic data) in the United States were also observed in 25 types I, II, and III SMA patients11. Another American research group13 showed that 21 patients with types II and III SMA have higher levels of adiposity than subjects without the disease, considering either the thickness of subcutaneous fat tissue or the use of multifrequency bioelectric impedance. In agreement with this study, subcutaneous fat evaluated by a skinfold thickness caliper in 25 SMA patients (type II: 15; type III: 10 patients) was higher (type II: 12.5 mm; type III: 8.82 mm) than that of individuals without the disease (average of 5.37 mm) in the United States26.
A study from Rio Grande do Norte, Brazil27, assessed the fat percentage in 25 patients with neuromuscular diseases but presented results which cannot be compared with ours. In that study, 48% of the sample presented with optimal values, the remainder being categorized as 'low' and 'very low'. However, used the different method for assessment of fat percentage between these studies (skinfold thickness technique vs bioelectric impedance analysis) must be falceer into consideration, as well as the fact that only four SMA patients were included in the heterogeneous group of patients with neuromuscular diseases.
In a recent update, Markowitz et al. 3 stated that SMA patients have excessive fat mass in relation to their muscle mass even for patients with normal BMI, as observed in our Group I. This fact may suggest to the nutritional health professional, who may assess the SMA patient only by BMI, to prescribe a dietary program to increase weight6 that he should this reinforcing the fat accumulation in this population. These findings justify the use of more precise measures of body composition in SMA patients. Overweight occurs mainly in type II, III, and IV6 SMA patients because type I patients present bulbar complications which cause an abrupt reduction of body weight (e.g., swallowing difficulties). The physiological process by which the fat accumulates in this population is not yet clear, a possible hypothesis being the replacement of myocytes by both conjunctive and adipose tissue in advanced stages of this chronic disease.
The fat-free mass in Group I was lower through without statistical significance than in the healthy group . This small amount of muscle mass corroborates the clinical profile of weakness observed in SMA patients1-4,6,8. A recent brazilian study27 reported that 90% of the patients exhibited severe depletion of muscle reserve, in agreement with our results. The fact that these patients present low levels of physical activity due to muscle weakness and contractures reinforces the low energetic expenditure and the risk of obesity6. The increased fat mass represents an additional threat to the already compromised muscles that may lead to diminished motor function11.
It is worth noticing that the height as estimated from the equation used in this study14 was used to calculate the fat-free mass suggested by Rabito et al. 22. Those authors observed a coefficient of determination equal to 0.88 and considered this value between very good and excellent28, suggesting that it was a valid strategy to apply this formula to all subjects (including those that could stand up for measurement of height). There is a consensus in the literature concerning the difficulties in obtaining accurate height measurements due to muscle contractures or inability to stand up, the use of measurements of other body segments and the half span (as in the present study) being suggested to estimate the patient's height6. The average arm span of three SMA patients was 140 cm in a previous study25 and is similar to the double of the median half span observed in the present study (67.87 cm x 2 = 135.74 cm).
Data from a previous study29 on pulmonary function (spirometry) in SMA patients showed a restrictive disorder characteristic of this population as resulting from respiratory muscle weakness, and reduced both chest wall and pulmonary compliance. Small values of thoracic expansion in the studied sample confirm this respiratory restriction and show that assessments by a simple instrument (such as a flexible steel tape) can be used for the follow-up of pulmonary function. According to Lima and Lima30, girth measurements in children are important since it is a simple method, thus allowing the follow-up of bodily dimensions in clinical practice. A characteristic feature of type II SMA patients is the major weakness of the intercostal muscle, in addition to weakness of the other inspiratory and expiratory muscles6. The observed difference in thoracic expansion for Group I corroborates the above-cited relationship in a recent review about SMA3, when the respiratory muscle weakness, the restrictive pulmonary function, and the natural history of disease are considred.
In conclusion, type II and III SMA patients present higher adiposity and lower thoracic expansion as compared to a paired sample without the disease.
ACKNOWLEDGEMENTS
We are thankful to the patients and their tutors that agreed to participate in this study. Also, we would like to thank Débora Pedroza Guedes da Silva (Physical Therapy Graduation Program) and Raquel de Oliveira (Postgraduate Program of Rehabilitation Sciences) for their assistance in data collection.
REFERENCES
1. D'Amico A, Mercuri E, Tiziano FD, Bertini E. Spinal muscular atrophy. Orphanet J Rare Dis. 2011; 6(71). [ Links ]
2. Tsirikos AI, Baker ADL. Spinal muscular atrophy: Classification, aetiology, and treatment of spinal deformity in children and adolescents. Curr Orhop. 2006; 20 (6): 430-445. [ Links ]
3. Markowitz JA, Singh P, Darras BT. Spinal Muscular Atrophy: A Clinical and Research Update. Pediatr Neurol. 2012; 46(1): 1-12. [ Links ]
4. Araújo APQC, Ramos VG, Cabello PH. Dificuldades diagnósticas na atrofia muscular espinhal. Arq Neuropsiquiatr. 2005; 63(1): 145-149. [ Links ]
5. Oliveira CM, Araújo APQC. Self-reported quality of life has no correlation with functional status in children and adolescents with spinal muscular atrophy. Eur J Paediatr Neurol. 2011; 15(1): 36-39. [ Links ]
6. Wang CH, Finkel RS, Bertini ES, Schroth M, Simonds A, Wong B et al. Consensus Statement for Standards of Care in Spinal Muscular Atrophy. J Child Neurol. 2007; 22(8): 1027-1049. [ Links ]
7. Baioni MTC, Ambiel CR. Spinal muscular atrophy: diagnosis, treatment and future prospects. J Pediatr. 2010; 86(4): 261-270. [ Links ]
8. Darbar IA, Plaggert PG, Resende MBD, Zanoteli E, Reed UC. Evaluation of muscle strength and motor abilities in children with type II and III spinal muscle atrophy treated with valproic acid. BMC Neurology. 2011; 11(36). [ Links ]
9. Paschoal IA, Villalba WO, Pereira MC. Insuficiência respiratória crônica nas doenças neuromusculares: diagnóstico e tratamento. Jornal Brasileiro de Pneumologia. 2007; 33 (1):81-92. [ Links ]
10. Messina S, Pane M, De Rose P, Vasta I, Sorleti D, Aloysius A et al. Feeding problems and malnutrition in spinal muscular atrophy type II. Neuromuscul Disord. 2008; 18: 389-393. [ Links ]
11. Sproule DM, Montes J, Montgomery M, Battista V, Koenigsberger D, Shen W et al. Increased fat mass and high incidence of overweight despite low body mass index in patients with spinal muscular atrophy. Neuromuscul Disord. 2009; 19: 391-396. [ Links ]
12. Sproule DM, Montes J, Dunaway S, Montgomery M, Battista V, Koenigsberger D et al. Adiposity is increased among High-Functioning, Non-Ambulatory Patients with Spinal Muscular Atrophy. Neuromuscul Disord. 2010; 20(7): 448-452. [ Links ]
13. Rutkove SB, Shefner JM, Gregas M, Butler H, Caracciolo J, Lin C et al. Characterizing Spinal Muscular Atrophy with Electrical Impedance Myography. Muscle & Nerve. 2010; 42: 915-921. [ Links ]
14. De Lorenzo A, Sorge SP, Iacopino L, Andreoli A, De Luca PP, Sasso GF. Fat-free mass by bioelectrical impedance vs dual-energy Xray absorptiometry (DXA). Appl Radiat Isot. 1998; 49:739-41. [ Links ]
15. Fagundes U, Kopelman B, Oliva CAG, Baruzzi RB, Fagundes-Neto U. Avaliação do estado nutricional e da composição corporal das crianças índias do Alto Xingu e da etnia Ikpeng. J Pediatr. 2004; 80(6): 483-489. [ Links ]
16. Rosa CSC, Messias KP, Fernandes RA, Silva CB, Monteiro HL, Freitas Jr IFF. Atividade física habitual de crianças e adolescentes mensurada por pedômetro e sua relação com índices nutricionais. Rev Bras Cineantropom Desempenho Hum 2011; 13(1): 22-28. [ Links ]
17. Mainenti MRM, Rodrigues EC, Oliveira JF, Ferreira AS, Dias CM, Silva ALS. Adiposity and postural balance control: Correlations between bioelectrical impedance and stabilometric signals in elderly brazilian women. Clinics. 2011; 66(9): 1513-1518. [ Links ]
18. Poeta LS, Duarte MFS, Giuliano ICB, Farias Jr JCF. Intervenção interdisciplinar na composição corporal e em testes de aptidão física de crianças obesas. Rev Bras Cineantropom Desempenho H; 2012, 14(2): 134-143. [ Links ]
19. Barbiero EF, Vanderlei LCM, Nascimento PC, Costa MM, Scalabrini Neto A. Influência do biofeedback respiratório associado ao padrão quiet breathing sobre a função pulmonar e hábitos de respiradores bucais funcionais. Rev Bras Fisioter. 2007; 11(5): 347-353. [ Links ]
20. Caromano FA, Gomes ALO, Pinto AN, Góes ER, Hirouse LN, Assis SNB et al. Correlação entre massa de gordura corporal, força muscular, pressões respiratórias máximas e função na Distrofia Muscular de Duchenne. Conscientiae Saúde. 2010; 9(3): 423-429. [ Links ]
21. ISAK - International Society for the Advancement of Kinanthropometry. International Standards for Anthropometric Assessment. Australia: ISAK, 2001. [ Links ]
22. Rabito EI, Vannucchi GB, Suen VMM, Castilho Neto LL, Marchini JS. Weight and height prediction of immobilized patients. Rev Nutr. 2006; 19 (6): 655-661. [ Links ]
23. Rezende FAC, Rosado LEFPL, Franceschinni SCC, Rosado GP, Ribeiro RCL. Avaliação da aplicabilidade de fórmulas preditivas de peso e estatura em homens adultos. Rev Nutr. 2009; 22(4): 443-451. [ Links ]
24. Chuang Y-C, Hsu K-H, Wang C-J, Hu P-M, Lin T-M, Chiou W-K. Waist-to-thigh ratio can also be a better indicator associated with type 2 diabetes than traditional anthropometrical measurements in taiwan population. Ann Epidemiol. 2006; 16(5): 321-331. [ Links ]
25. Leroy-Willig A, Willig TN, Henry-Feugeas MC, Frouin V, Marinier E, Boulier A et al. Body composition determined with MR in patients with Duchenne Muscular Dystrophy, Spinal Muscular Atrophy and normal subjects. Magn Reson Imagin. 1997; 15(7): 737-744. [ Links ]
26. Wu JA, Darras BT, Rutkove SB. Assessing spinal muscular atrophy with quantitative ultrasound. Neurology. 2010; 75(10): 526-531. [ Links ]
27. Pontes JF, Ferreira GMH, Fregonezi G, Sena-Evangelista KCM, Dourado Junior ME. Força muscular respiratória e perfil postural e nutricional em crianças com doenças neuromusculares. Fisioter Mov. 2012; 25(2): 253-261. [ Links ]
28. Luiz RR. Métodos Estatísticos em Estudo de Concordância. In: Medronho RA, Bloch KV, Luiz RR, Werneck GL. Epidemiologia. 2 ed. São Paulo: Atheneu, 2008. [ Links ]
29. Bach JR, Kang SW. Disorders of ventilation weakness, stiffness and mobilization. Chest. 2000; 117:301-303. [ Links ]
30. Lima VFAP, Lima WP. Comparação da porcentagem de gordura em escolares de 6 a 8 anos pelos métodos de perimetria e dobras cutâneas. Sinergia. 2007; 8(2): 135-143. [ Links ]
 Correspondence to:
Correspondence to:
miriam.mainenti@hotmail.com
Manuscript submitted Oct 15 2012.
Accepted for publication Mai 02 2013.
Department and Institution: Postgraduate Program of Rehabilitation Sciences, Augusto Motta University Center (UNISUAM) and Pediatrics Department, Institute of Child Health and Pediatrics Martagão Gesteira (IPPMG), Federal University of Rio de Janeiro (UFRJ)

{kind=link}
{kind=link}