










Services on Demand
article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Share

 Permalink
PermalinkJournal of Human Growth and Development
Print version ISSN 0104-1282
Rev. bras. crescimento desenvolv. hum. vol.24 no.1 São Paulo 2014
ORIGINAL RESEARCH
Growth parameters of Sri Lankan children during infancy: a comparison with World Health Organization multicentre growth reference study
Priyantha Julian PereraI; Meranthi Preethika FernanadoII; Nayomi RanathungaIII; Wikum SampathIV; Rohini SamaranayakeV; Sachith MeththanandaVI
IConsultant Paediatrician/Senior Lecturer, Department of Paediatrics, Faculty of Medicine, University of Kelaniya, Sri Lanka
IILecturer, Department of Paediatrics, Faculty of Medicine, University of Kelaniya, Sri Lanka
IIIMedical Officer, Teaching Hospital Ragama, Sri Lanka
IVDepartment of Tropical Health, Faculty of Medicine, University of Kelaniya, Sri Lanka
VClinical skills lab, Faculty of Medicine, University of Kelaniya, Sri Lanka
VIDepartment of paediatrics, Faculty of Medicine, University of Kelaniya, Sri Lanka
ABSTRACT
OBJECTIVES: growth monitoring (GM) is an important intervention ensuring wellbeing of children. If GM to be meaningful it is essential to have reference standards appropriate for that population. In Sri Lanka growth charts based on WHO multi centre growth reference study (MGRS) are used for GM. This study was carried out to ascertain the appropriateness of MGRS charts for GM in Sri Lankan children.
METHODS: out of a birth cohort of 2215 children, 250 from each sex were invited for a followed up. Children were examined at 2, 4, 6, 9 and 12 months, to measure weight and length. Statistical characteristics of weight and length for each sex were calculated and compared with MGRS data.
RESULTS: out of babies invited to participate in the study 244 boys and 241 girls responded initially. Out of this 85% of boys and 86% of girls completed the follow up. Weight and length of both sexes deviated significantly at all ages from MGRS data.
CONCLUSION: MGRS data seems to be inappropriate for monitoring growth of Sri Lankan children
Key words: growth monitoring, growth charts, weight, length, growth centiles.
INTRODUCTION
Growth monitoring (GM) is an important intervention ensuring wellbeing of children. Medical, nutritional, social and emotional problems have a negative effect on physical growth of a child. Thus, GM is an effect on screening tool to pick up children with problems early. For meaningful GM not only accurate measurements are important, but having accurate reference standards to compare is important. Over the years different growth charts have being used for GM. The WHO Multi centre Growth Reference Study (MGRS) was undertaken between 1997 and 2003, to generate new growth curves for assessing the growth and development of infants and young children around the world1.
The objective of the MGRS was to devise reference growth charts applicable to all communities. MGRS was based on the concept, growth of children from birth to five years depends mainly on nutrition, feeding practices, environment and health care than genetics or ethnicity. MGRS was conducted in six different areas of the world, i.e. New York, Brazil, Norway, Ghana, New Delhi and Bahrain. To ensure children with highest growth potentials included, only children brought up under optimum conditions were selected for MGRS. MGRS curves are expected to provide a single international standard representing physiological growth of all children from birth to five years1.
In Sri Lanka, growth charts based on MGRS are used for GM since 2008 2. Over the years it has been our observation that most of the Sri Lankan children are having their height and weight close to mean minus one standard deviation on MGRS charts than the mean. In a study done in 2010 in the Gampaha district, Sri Lanka, growth parameters at birth were studied. According to this study statistical characteristics for weight, length and head circumference of Sri Lankan children, significantly deviated from MGRS. Means of Sri Lankan children at birth were falling near mean minus one standard deviation of MGRS growth charts3.
Two other studies, on birth weight of Sri Lankan babies have showed a similar tendency4,5. Results of these studies have raised concerns about the appropriateness of using MGRS growth charts for GM in Sri Lanka. To date there are no studies comparing post natal growth of Sri Lankan children with MGRS data.
The objective of this study is to ascertain the appropriateness of multi centre growth reference study (MGRS) charts for Growth monitoring (GM) in Sri Lankan children.
METHODS
Study setting
In contrast to being a low middle income country, Sri Lanka has impressive health statistics. Maternal mortality ratio of Sri Lanka is 33.4 per 100,000 live births6 and neonatal mortality rate is 10 per 1000 live births7. Sri Lanka is divided in to 25 administrative districts. Gampaha district is the 2nd most populous district with a population of 2,066,096. This is about 12% of the total Sri Lankan population8. In socio-economic standards, Gampaha district is only second to Colombo district. Gampaha district had 9.2% of poor households in 20029. Other than for Colombo and Gampaha all other districts has percentages of poor households well above 15%. Around 99% of deliveries taking place in the district occur in hospitals.
Study designand Subject Selection
A descriptive cross-sectional study was conducted between September and October 2012 to assess growth parameters at birth of babies born in Gampaha district. All normal term babies born in both government and private hospitals were recruited for the study. A total of 2215 babies were included in this study. At recruitment parents were informed that a follow up study will be conducted and if their baby is selected they will be informed.
Out 2215 babies 250 boys and 250 girls were randomly selected using computer generated numbers. Parents of selected babies were informed via telephone or by post. Babies were followed up at two, four, six, nine and twelve months. These ages were selected because they are the ages at which immunizations are carried out in Sri Lanka. A special clinic was conducted at the University Paediatric Unit of North Colombo Teaching Hospital for the follow up. Participation in the study was voluntary and informed written consent was obtained from mothers at the first visit.
Data collection
Weight and length of children were measured by a medical graduate, assisted by a medical student. To avoid inter observer error, same medical graduate and medical student did measurements at all clinics. Both these investigators had one week training under the principle investigator. Weight was measured to the second decimal in kilograms using a beam balance scale, standardised once a week. The length was measured to the first decimal in centimetres using a foldable infantometer. Measurements were randomly repeated by the first investigator to ensure accuracy. Kappa scores of one and0.95 were obtained for weight and length respectively, indicating strong agreement between the principle investigator and the medical graduate.
At each visit babies were also examined by a consultant Paediatrician or a Senior Registrar in Paediatrics. Any medical problems detected were attended to. Next date of clinic visit was informed to the parents during each visit and reminders were sent via telephone and post. Children who missed a scheduled clinic were given a new appointment on the same week. Children who failed to turn up at a particular age were not followed up further.
Data analysis
Descriptive statistics and frequency tabulations were generated using statistical package for social sciences, version 16. Mean, mode, median, standard deviation and centiles were calculated for weight and length at each age. Socio demographic data of children who completed the follow up and those who dropped out were calculated separately. Growth data of children who dropped out were also compared with that of children who completed the study.
Ethical issues
Ethical clearance was obtained from the ethics committee of Faculty of Medicine, University of Kelaniya. Informed written consent was obtained from mothers. Appropriate action was taken for babies with medical or surgical problems. Correct feeding advice was given to mothers and EBF was promoted at all times. Apart from travelling expenses, there were no additional expenses to the parents.
RESULTS
Out of babies invited to participate in the study 244 boys and 241 girls responded initially. Despite our attempts to encourage participation, there was a gradual decrease in attendance with 85% of boys and 86% of girls completing the follow up till one year. Number of babies presented at each age is depicted in table 1.

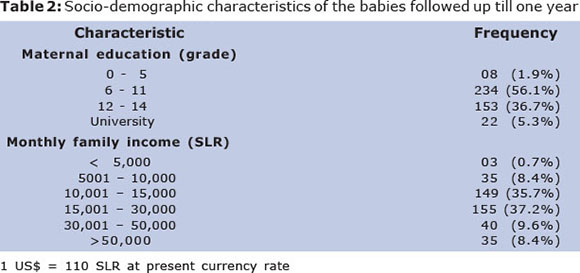
Children included in the study were from a reasonably good socio-economic background, where more than 98% of the mothers had secondary education.Maternal Education level and monthly family income of the babies followed up till one year is depicted in table 2.
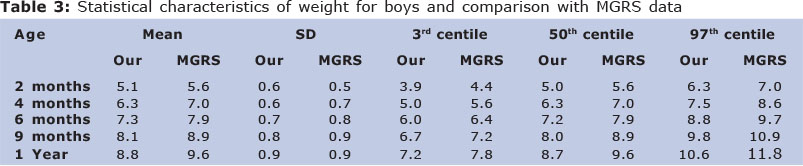
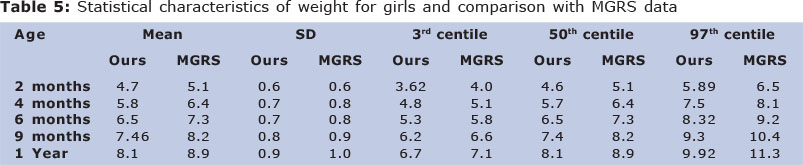
Weight and length of both sexes in the study population showed significant deviation from MGRS data. At all ages mean of weight and length of the study population were falling on or near mean minus one SD of the MGRS curves.
As with other biological parameters weight and length of both sexes exhibited a normal distribution at all ages. Statistical characteristics of weight and length for boys and girls are depicted in table 3, 4, 5 and 6 respectively. For the purpose of comparison relevant figures from MGRS is also given in these tables.
Available data from children who were lost to follow were compared with data from children who completed the follow up. We did not find a significant difference.
DISCUSSION
GM is an important component of the child welfare activity in a country. However, if inappropriate growth charts are used GM will be useless andharmful in many ways. If reference standards used for GM are higher than the population concerned, growth will be underes-timated and vice versa. Though MGRS was based on the theory that genetics and ethnicity do not play an important role in physical growth of a child, there are studies which have proven genetic influence on growth10,11.
As a principle, growth charts are based on data from children having maximum growth potentials. In our study, only normal-term babies, without congenital abnormalities were included. Babies born in private hospitals were also recruited to ensure babies from the higher socio-economic stratum were also included in the study. Yet according to our study, at all ages during infancy means of height and weight were falling close to the mean minus one standard deviation according to MGRS data. As the Gampaha district is socio-economically advanced than most of the districts and socio-economic factors also influence the physical growth of children, national figures can be expected to be lower than derived from our study.
Therefore, using MGRS growth curves for GM tend to underestimate growth of our children.´
This has serious repercussions. Even a child. This growing well within his genetic potentials will be considered failing to thrive, leading to unnecessary investigations and treatments. Most worrying effects would be on exclusive breast feeding.
Exclusive breast feeding is considered as the best way to feed an infant during first six months. When a child on exclusive breast feeding show a poor growth according to growth charts, mothers tend to panic and start formula milk thinking breast milk is inadequate. This trend has been demonstrated in Sri Lanka by a previous study12. Due to overfeeding with formula milk some of these babies demonstrate an inappropriate weightgain, pushing them up in the growth charts. This can give a negative impression that exclusive breast feeding is not capable of supporting growth during early infancy. Sri Lanka has a very high exclusive breast feeding rates at present, but this issue might have a negative impact on it13.
In later part of infancy, when growth parameters tend to fall down according to growth charts mothers resort to force feeding their babies which is often resisted by babies. This often leads to a vicious cycle and child starts to refuse food even at sight, causing mental trauma to both child and parent. On the other hand overfeeding a child merely to catch up with the growth chart which may not be appropriate for the child might end up producing an overweight child.
At present in Sri Lanka we are facing an alarming rise in overweight and Obesity among school children. Overfeeding during preschool years is going to add to this problem. All these problems could be avoided by developing our own growth charts appropriate for our children.
Limitations
Main limitation in our study was the drop outs during the progress of the study. This is a known phenomenon in this type of study design. Socio-demographic criteria and growth data of children who completed the study and who dropped out were compared to ascertain the impact of drop outs on outcome of the study.
Our study sample consisted of children living in a limited geographical area, so that findings of this study may not represent the entire country. Considering the higher socio-economic standards of the study population, national figures could be expected to be lower than from this study.
In conclusion, the Statistical characteristics of this study population deviated significantly from MGRS data, arousing serious concerns about its use for GM in Sri Lanka.
Conflicts of interest
All authors declare no conflicts of interest in conducting this study or publishing these data.
Funding
No funds were obtained to conduct the study.
Author contribution
PJP was involved in planning & supervising the study and preparation of the manuscript. MPF was involved in planning the study, data collection and preparation of the manuscript. NR,RSWS were involved in data collection & analysis and preparation of the manuscript. SM was involved in planning and conducting the studyand preparation of the manuscript.
REFERENCES
1. de Onis M, Onayongo A, Broeck J, Chumlee C, Matorell R. Measurement and standerdi-zationprotocalls for anthropometry used in the construction of a new international growth refference. Food and nutrition bulletin, vol 25. No 1 ( suppliment) 2004, The United Nations University. [ Links ]
2. Child Health Developmental Record. Ministry of Health. 2012. Colombo. Sri Lanka. [ Links ]
3. Perera PJ, Fernando M, Warnakulasuriya T, Ranathunga R, Wickramasinghe R. Growth Parameters at birth for Sri Lankan babies. WHO South-East Asia Journal of Public Health 2013; 2(1): 49-54 [ Links ]
4. WHO 1984. Perinatal mortality & morbidity including low birth weight. South East Asian regional organization. No 3, New Delhi [ Links ]
5. Abeysena C, Payawardana P, Senevitathne R. Maternal sleep deprivation is a risk factor for small for gestational age: A cohort study. Australian and New Zeeland journal of Obstetrics and Gynecology 2009; 49: 382 - 387 [ Links ]
6. Ministry of Healthcare and Nutrition, Family Health Bureau. Maternal Mortality Review for 2008. Colombo. 2010. [ Links ]
7. UNICEF - Sri Lanka - Statistics 2012. Available through www.unicef.org/infobycountry/sri_lanka_statistics.html. last viewed on 10.9.13 [ Links ]
8. Department of disaster management, Government of Sri Lanka 2012. Available through http://www.dmc.gov.lk/DistrictSection/Gampaha/Gampaha_P6DivisionalInfo.html last viewed on 10.9.13 [ Links ]
9. Department of Census and Statistics. Poverty Statistics/Indicators for Sri Lanka. Colombo, Sri Lanka. 2002. [ Links ]
10. Johnson L, Llewellyn CH, van Jaarsveld CH, Cole TJ, Wardle J. Genetic and environmental influences on infant growth: prospective analysis of the Gemini twin birth cohort. PLoS One. 2011;6(5):e19918 [ Links ]
11. Rona RJ, Chinn S.Genetic and environmental influences on growth. J Med Screen. 1995;2(3):133-9 [ Links ]
12. Perera PJ, Ranathunga N, Fernando M P, Sampath W, Samaranayake G B. Actual exclusive breast feeding rates and factors influencing them, among a cohort of children living in Gampaha district Sri Lanka: A prospective observational study. Int Breastfeed j; 2012, 7:21 [ Links ]
13. Perera PJ, Fernando M, Warnakulasuria T, Ranathunga N. Feeding practices among Children attending child welfare clinics in Ragama MOH area: a descriptive cross-sectional study. Int Breastfeed J; 2011; 6: 18 [ Links ]
Manuscript submitted Nov 16 2013
Accepted for publication Dec 28 2013
Corresponding author: priyanthaprr@gmail.com

{kind=link}
{kind=link}
{kind=link}
{kind=link}