










Serviços Personalizados
artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282
Rev. bras. crescimento desenvolv. hum. vol.24 no.1 São Paulo 2014
ORIGINAL RESEARCH
Body dissatisfaction among students in brazilian southern city
Ana Caroline Branco Leite; Natália Basso Ferrazzi; Tatiana Mezadri; Doroteia Aparecida Höfelmann
Undergraduate Nutrition Degree, University of Itajai Valley - UNIVALI
ABSTRACT
The body dissatisfaction is associated with eating disorders, interpersonal difficulties and suicidal ideation. The objective was to estimate the prevalence of body dissatisfaction, and its association with infant and maternal variables of school children from 4 and 5 years of municipal schools in Itajai, Santa Catarina. Seven hundred and thirty seven students from 22 urban and rural schools were randomly selected . Data collection included the collection of anthropometric data measures, questionnaires for the child and his guardian. The body dissatisfaction has been identified by the difference between perceived body image and that desired by the school children. Prevalence ratios (PR) and their 95% confidence intervals (95% CI)were calculated and. The response rate was 81.7% (n = 602). The prevalence of body dissatisfaction was 76.9%. Overweight Schoolchildren , and those with abdominal excess of fat showed higher prevalence rates (21% and 30%) of body dissatisfaction. Children of overweight parents had prevalence 12% higher of the outcome. Attempts to lose weight or fat were 23% and 21% higher among weight dissatisfied children . After adjustment, the prevalence of the outcome was lower among girls (PR 0.9 95% 0.8, 1.0) and higher among children with abdominal excess of fat who underwent attempts to lose or gain weight (PR 95 1.2% 1.1, 1.4). The results indicate a high prevalence of body dissatisfaction, especially among boys. Approximately half of the students wanted to weigh less, however, among boys the desire to gain weight was higher. The abdominal fat was strongly associated with the higher prevalence of body dissatisfaction.
Key words: Body image, Nutritional Status, Perception of body weight, abdominal obesity, Obesity, School Health.
INTRODUCTION
The body image is defined as an individual mental representation about their own body. It represents an experience that person lives constantly, deriving from actions, perceptions and impulses. It carries jointly with body own identity, and has relation with physiologic, social and affective aspects. Body image process takes the whole life; its organization is facilitated in early life due to a roll of conditions typical of this life stage¹.
Body self perception is an important aspect of body image, because reflects satisfaction and concerns about body mass. Predominant social cultural patterns may influence body satisfaction2.
Sociodemographic, anthropometric factors, cultural influences, perceptions, parents concerns about children nutritional status and media pressure are factors related with body dissatis-faction3,4.
The media spreads ideas about a kind of corporal perfection, in which slimness symbolizes competency, success and sexual attraction, while obesity represents laziness, self-pity, and lower decision power and life quality5.
Children can overreact to cultural pressure, because they have concerns about body, and appearance in development, and more this body shed to real one, greater will be possibility of conflict, which could generate dissatisfactions with body image, and even initiate eating disorders, frequently related with low self-esteem and limited psychosocial performance6,7.
The eating disorders can be considered phenomenon resulting from interaction of personal, familiar, and sociocultural factors, and are characterized by a intense concern not only with body, but with weight and also with food. The slimness valorization and pressure to lose weight, associated with biologic, familiar, and psychological factors generate a pathologic fear of gain weight8.
Boys are more exposed to muscular figure ideal, conveyed by dolls of superheroes. On the other hand, girls follow beauty ideal of Barbie® doll, tailored in a slim body. Research shows that girls are more dissatisfied with their bodies, wish thinner body, while among boys there is higher prevalence to wish larger bodies4.
In last decades, studies about body image have been increasing, mainly because evidences indicating that body dissatisfaction begins early in life, and is strongly influenced by sociocultural aspects4,9. Furthermore, prospective studies have observed associations between body dissatisfactions and negative outcomes. Among adolescents of both genders body dissatisfaction was considered risk factor to depressive mood, low self-esteem and suicidal ideation, even after adjustment for psychological problems and other variables. Girls in early adolescence and boys in adolescence are considered age groups more susceptible to suicidal intention10,11.
Thus, this study aimed to estimate body dissatisfaction prevalence in association with children and parent variables from 4th and 5th year students of municipal schools of Itajaí, Santa Catarina.
METHODS
Cross-sectional study with students of public schools from Itajaí/SC, enrolled in 4th and 5th year of basic instruction.
Itajaí is located in Santa Catarina state, and main economic activities of city are connected to merchant port and fishing. The full wholesale trade shows great expression, industrial section is also important, and trade of eating genders. The Port of Itajaí is the largest of Santa Catarina, stands in third position in traffic of containerized load12,13.
According with Brazilian Institute of Geographic and Statistics14, census and estimated population of Itajaí was 163,218 in habitants. Itajaí presented a Gross National Product (GNP) per capita of 38,563 reais15 . In 2000, the poverty prevalence was 29.47% and Human Development Index (HDI) of 0.82516,17. Infant mortality rate was 10.07 per each one thousand children18,19.
The town presented 39 municipal schools, with 4,587 students enrolled in 4th to 5th years. The sampling process was in double stage. In the first, 22 schools were drawn to participate. In each drawn school a roll of enrolled students were performed inway to perform the student draw to data gathering.
Sample size was estimated in software Epi Info 6.04 (EUA - Center for Control of Diseases - CDC). The literature review of studies in studied age band showed body dissatisfaction prevalence ranging 59% to 85%, then we opted to considering expected prevalence of 50% maximizing sample size. Confidence level of 95% and error margin of 5% were considered. A design effect of 1.5 was used due sampling method in double stage (n = 531), to that result 20% were added to compensate losses and refusals, and also 15% to control confound (n = 717).
Estimate to test higher body dissatisfaction prevalence among children with higher income, considered confidence level of 95%, power of 80% and prevalence rate (PR) of 1.3 among exposed, design effect of 1.5, more 35% (losses and/or refusals and control of confounders), resulted 737 children, and was defined as sample size.
In second stage were selected those to be included in study among those enrolled in drawn schools:students were numerated and systema-tically selected through a sample faction (k) obtained by division of total number of enrolled students and sample size.
Data gathering occurred between February to July 2010 and was performed by undergra-duate Nutrition responsible by project, and comprised anthropometric collect data, and children and caregivers questionnaire. A Term of Informed Consent was asked to sign for children caregivers'. Students with signed term were included in the study. Losses considered those children, that after three visits to school were absence, and those without signed term.
Questionnaire have been sent by caregivers up to three days, and included questions about age, schooling (up to 8 years; 9 to 11 years and 12 or more), familiar per capita income (minimum wage R$ 510.00) divided in tertiles: low (0.11 to 0.47), mid (0.48 to 0.78), high (0.79 to 3.27); skin color (white or lighter skinned black and black), lose or gain weight diet habit performing (yes, no), parents perception about children body weight (underweight, normal and overweight), and children health evaluation (very good, good, average/poor/very poor). Considering lower num-ber of caregiver that self-reported their skin color as Asiatic or indigenous (1.39%, n = 7; e 1.19%, n = 2, respectively), those classified in those categories were coded as "missing". Students' skin color classified by research, and followed the same way as parents one.
A questionnaire was applied to students with body image scale - Children's Figure Rating Scale21, comprised by silhouettes with extremes of thinness and fatness. Students selected a drawing compatible with their current body; desire silhouette; opposite gender preference perceived and parents' perception about their body. Additionally, their answered questions coded as yes or no, in relation to performing attempt to lose or gain weight, diet performing and body self-perception (fat, normal or thinner).
For students' nutritional status assessment they were weighted on a digital scale manufac-tured by Kratos-Ca, with a maximum capacity of 150 kg, wearing minimal clothing and no shoes. The scale was fixed in plain surface, away of wall. Student stay in center of scale, barefoot, standing with feed together, arms along the body and stop this position22.
After weighting, height was measured with a compact stadiometer manufactured by Wiso, with scaled 0 to 200 cm, and precision of 0.1 cm. Students were measured barefoot, standing, in plain surface, back to stadiometer, with feet parallel and ankles together22.
The waist circumpherence was measured by means an inextensible anthropometric tape in its narrower perimeter, between students' last rib and iliac crest, without compressing tissues, and was classified according cut of points proposed by Taylor et al.23.
The Body Mass Index (BMI) was calculated dividing weight to squared height, the result of which is given in kg/m². The nutritional profile was determined through World Health Organization24 criteria. Students were characterized from underweight to overweight, following the BMI to age indicator.
The data entry was performed in Epidata software, in which data enter protection have been created. The questionnaires were reviewed, coded, double-entered and conferred in Epi Info software by research.
To describe quantitative variables were calculated means and standard deviation, minimum, maximum and median values. Categorical variables were described through their absolute (n) and relative (%) frequencies, and 95% Confidence Intervals (95% CI).
The body dissatisfaction was identified by the difference between current perceived silhouette and that desired by students. The association among variables and outcome were analyzed by qui-squared Pearson test, with design effect adjustment. Correlation among continuous variables was evaluated by Pearson's correlation.
The body dissatisfaction prevalence was additionally compared with exposition variables through PR and respective 95% CI. The adjusted analysis was performed through Poisson's Regression, with adjustment for complex design. We included in adjusted analysis those variables that kept confidence level of 25% in bivariate analysis. The input variables process in adjusted analysis initiated by children's variables followed by caregivers' variables. The p < 0.0525 was considered in analysis. Analyses were performed through Microsoft Excel and Stata SE9 software.
The research project was submitted and approved by the Committee of Ethic in Research of University of Vale of Itajaí (UNIVALI), under protocol numbered 373/09A. The results were informed to children's caregivers and Secretary through main findings description and deliver of individual reports in each evaluated school.
RESULTS
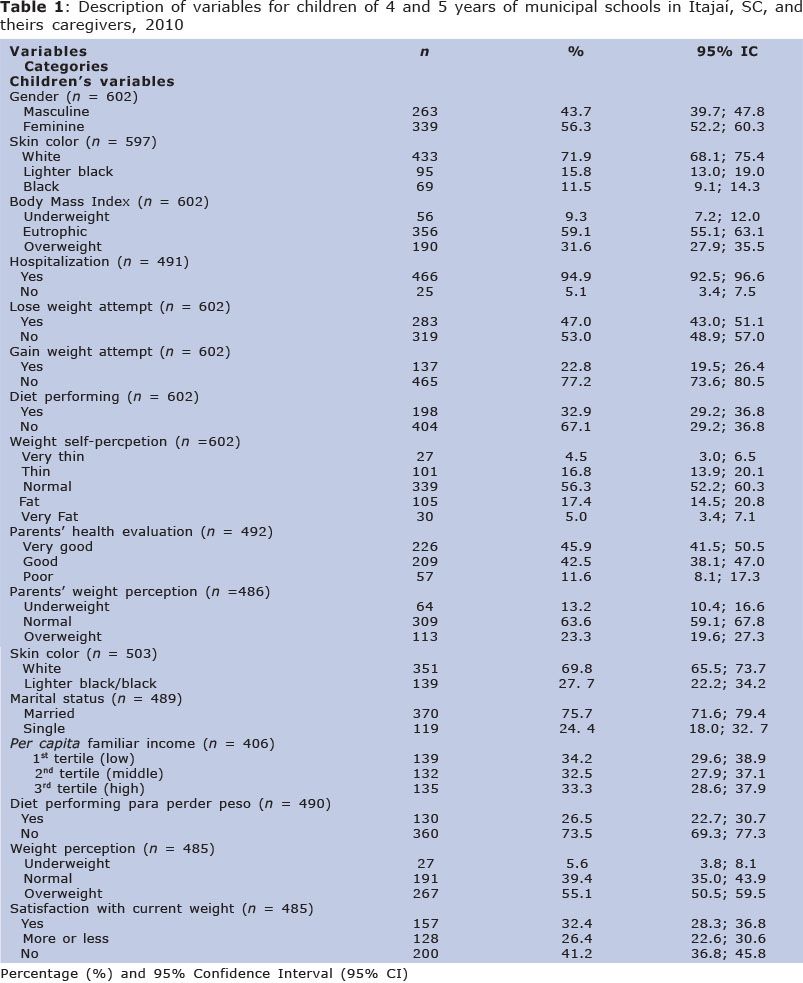
Six hundred and two consent terms were signed by parents or caregivers of investigated students from 737 that we have sent (81.7%). Questions completeness rate ranged to 67.4% to 100% for income variable and those collected in questionnaire replied by children (Table 1).
Girls participated more in this study than boys (56.3% vs 43.7%) (Table 1). The mean of age was 9.9 years and ranged 7.7 to 14.3 years, with standard deviation wish to gain weight was higher among boys (30.8% vs 21.83%) (p = 0,003).
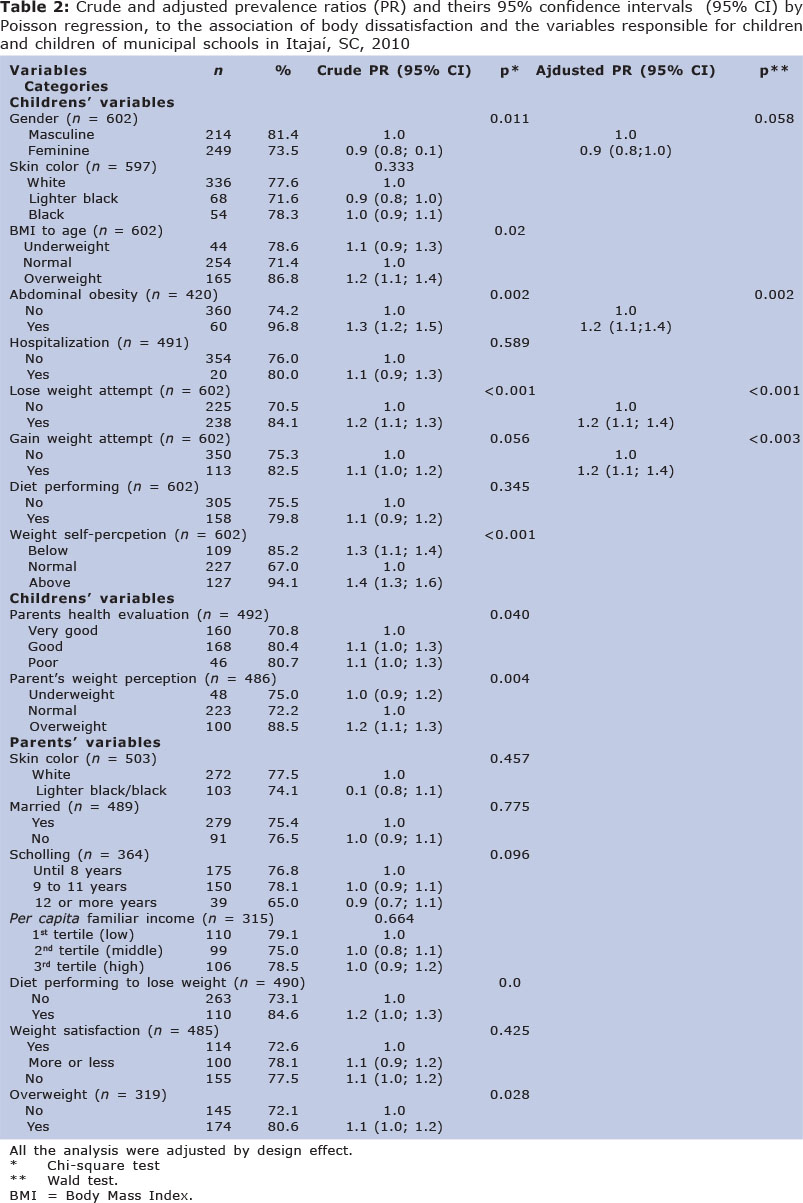
Girls presented lower prevalence of body dissatisfactions than boys. Children with BMI considered higher than ideal showed prevalence 21% higher of body dissatisfaction than those in normal range. Body perception as "overweight" represents an increase of 40% to outcome, while body image as underweight contributes with 27%. Among those that reported performing attempts to lose or gain weight, body dissatisfaction prevalence was 19% and 10% higher, respectively. Among scholars with excess of fat in abdominal region prevalence of outcome was 1.21 time higher. Children of parents with overweight had prevalence 12% higher of body dissatisfaction. Unsatisfied children parents their health rated as worst (Tables 2).
Despite that was not found difference in nutritional status classification according gender (p=0.884), girls presented lower prevalence of abdominal obesity than boys (PR = 0.76; 95% CI = 0.54; 1.08, p = 0.040). While body dissatisfaction was higher among boys, diets realization were higher among girls (36.58% vs 28.14%, p = 0.032).
Urban or rural school localization was not associated with body dissatisfaction (76.7% vs 80.0%) (p = 0.797).
The BMI were not applied in adjusted analysis, based in strong correlation with waist circumference (r=0.91), furthermore, in crude analysis BMI presented lower magnitude of association with the outcome.
After adjusted analysis children variables (gender, desire to lose or gain weight, and abdominal obesity), parents variables (overweight, schooling, and realizations of diets), lost their associations with body dissatisfaction in studied population. Girls presented 9% lower body dissatisfaction than boys. Attempts to lose or gain weight were 23% and 21% higher respectively, in children unsatisfied with their body weight (Table 2).
Due to expressive difference in comple-teness rate of questions from questionnaire replied by parents additional analysis were performed, comparing outcome prevalence with missing categories in each variable. Prevalence exhibited by "missing" group was higher than those observed to reference categories by following variables: parents rating about children weight, overweight, skin color, schooling, marital status, performing diets and parents´ satisfaction with weight (data not presented).
DISCUSSION
Prevalence of body dissatisfaction in this study was 76.91%. Therefore higher than that observed in study performed by Triches and Giugliani 4 with schoolchildren between 8 and 10 years in Dois Irmãos and Morro Reuter, in Rio Grande do Sul (63.9%). Vilela et al. 20 also verified lower prevalence of body dissatisfaction (59.0%) among students with 7 to 19 years in Minas Gerais. Explanations by those differences could not be find in relation our sample gender or nutritional status, once in both studies4,20 most part of students was from feminine gender. Among children from Rio Grande do Sul 4 prevalence of eutrophic (58.2%) was lower than those observed in students of this study (82.0%).
In most part of studies which included students of same age group studied, prevalence of body dissatisfaction was higher among girls26, finding that also found among adolescents9 and adults27-28. However, among studied children, boys presented prevalence 10% higher of body dissatisfaction than girls. Similar findings were found by Conti et al. 29 among adolescents between 10 and 14 years in São Paulo, boys presented higher prevalence of body dissatisfaction than girls (40.0% and 18.5%, respectivally).
In analyzing differences between genders for investigated variables were not found significant differences for major part of investigated variables (data not presented for all variables). Prevalence of overweight was similar among them, but abdominal obesity was found more frequently in boys.
In last decades, abdominal obesity became an important health concern, mainly in relation to metabolic abnormalities associated with future cardiovascular disease. Among pre-school children overweight can anticipate puberty in girls and delay in boys. Obesity in girls in pre-pubertal period can also be associated with hyperandrogenemia and higher risk of polycystic ovaries. Despite underlying biologic mechanisms are not fully understood, insulin resistance, and compensatory hyperinsulinemia represents cues to pubertal changes associated with children obesity30.
The excess of fat in abdominal region is recognized, mainly, with risk factor to cardiovascular disease, diabetes, dyslipidemia and metabolic syndrome31,32.
In study performed with students from Santo André3, they detected among boys statistically significant association among overweight and body dissatisfaction, in regions in which were observed accumulation of fat (stomach and waist), well as in relation to body weight; in girls, for areas as hair, buttocks, hip, thighs, legs, stomach, shoulders/back, muscular tone, body weight and general aspects, i.e., boys and girls reported dissatisfaction with stomach and body weight 3.
Nearly half of investigated students in both genders would like to lose weight, but, desire to gain weight was virtually twice higher among boys. These behaviors also can be noticed by other research, which observed that boys desired larger silhouette than current, indicating stronger bodies4,5. Boys can interpret larger drawings as more muscular or older.
The desire to lose weight as similar among boys and girls, but performing diets was more frequently observed in girls (36.58%). Those findings reinforce those of Vilela et al.,20 in which 40% of students performed some kind of diet, mainly among girls.
Fear to gain weight and persistent desire to lose weight can initiate an excessive concern with food, and consequently, an alteration of eating behaviors, with dietetic restrictions, joint with physical activity planned to reduce weight33.
Nunes et al.34 pointed out that body image dissatisfaction can be strongly associated with possible eating disorders, fact that deserves attention especially because of its consequences in individual life.
In this study, the prevalence of body dissatisfaction was 79.8% among students that admitted performing diets. According Salles e Fiates 35 the practice of diets is already part of life of a significant number of pre-adolescents. Feminine gender is often more vulnerable to social, economic, cultural pressure, associated with esthetic patterns. There is evidence in literature about higher mother sensibility to girl's body weight. Mothers showed higher concern with weight gain and higher probability to adopt food intake restrictions to their daughters 36.
Children of overweight parents presented prevalence 12% higher of body dissatisfaction. Several studies found association among familiar context aspects before and after child's birth and children overweight 37, among their parents´ overweight stands out 38, 39, 40. Beyond the risk to have overweight (factor strongly associated with body dissatisfaction), the coexistence with mothers concerned about their body weight can promote a less favorable vision about children own body image 41.
Among limitations of this study we can point out the cross-sectional design. Children were evaluated once, in this way, it is not possible to determine temporal direction of observed associations among investigated variables and outcome, i.e., define if they represent cause or consequence of body dissatisfaction. Association analysis of exposition variables and outcome can be harm by refuses, related to absence of consent term by parents. Furthermore, relative homogeneity of evaluated, all from public municipal schools, probably be the principal reason for absence of association among socioeconomic variables and the outcome. Inclusion of children of urban and rural area and analysis of outcome prevalence in not completely questionnaires represents important advantages of this study.
CONCLUSIONS
The findings of this study indicated high prevalence of body dissatisfaction among the evaluated children, mainly among boys. Nearly half part of the students of both genders desired to have lower weight, however among boys desire to gain weight was higher. The abdominal obesity was strongly associated with higher prevalence of body dissatisfaction among the evaluated children. Those results must be considered by caregivers and health professionals.
Contributions:
Leite, ACB: study concep-tion, data collect, paper writing; Ferrazzi, NB: study conception, data collect, paper writing; Mezadri, T: study conception, critical review of paper; Höfelmann, DA: study conception, data analysis, paper writing.
Acknowledgements:
Those responsible for Secretary of Education from Itajaí and school employees for allowing the research. To students and their parents for taking part in data gathering. We thanks to UNIVALI and Santa Catarina State Government for research grant.
REFERENCES
1. Tavares MCGCF. Imagem corporal: conceito e desenvolvimento. São Paulo: Manole; 2003. [ Links ]
2. Tessmer CS, Silva MC, Pinho MN, Gazalle, FK, Fassa AG. Insatisfação corporal em freqüentadores de academia. R. bras. Ci e Mov. 2006; 14:07-12. [ Links ]
3. Conti MA, Frutuoso MFP, GambardellaAMD. Excesso de peso e insatisfação corporal em adolescentes. Rev Nut Camp. 2005; 18: 491- 97. http://dx.doi.org/10.1590/S1415-52732005000400005 [ Links ]
4. Triches RM, Giugliani ERJ. Insatisfação corporal em escolares de dois municípios da região Sul do Brasil. Rev Nutr. 2007; 20:119-28.http://dx.doi.org/10.1590/S1415-52732007000200001 [ Links ]
5. Pereira EF, Graup S, Lopes AS, Borgato AF, Daraonco LSE. Percepção da imagem corporal de crianças e adolescentes com diferentes níveis socio-econômicos na cidade de Florianópolis, Santa Catarina, Brasil. Rev Bras Saúde Matern Infant. 2009; 9:253-62. http://dx.doi.org/10.1590/S1519-38292009000300004 [ Links ]
6. Branco LM, Hilario MOE,Cintra IP. Percepção e satisfação corporal em adolescentes e a relação com seu estado nutricional. Rev Psiq Clín. 2006; 33:292-96. [ Links ]
7. Pinheiro AP, Guigliani ERJ. Quem são as crianças que se sentem gordas apesar de terem peso adequado? J Pediatr. 2006; 82:232-35.http://dx.doi.org/10.2223/JPED.1477 [ Links ]
8. Souto S, Ferro-Bucher JSN. Práticas indiscriminadas de dietas de emagrecimento e o desenvolvimento de transtornos alimentares. Rev Nutr. 2006; 19: 693-704. http://dx.doi.org/10.1590/S1415-52732006000600006 [ Links ]
9. Corseuil MW, Pelegrini A, Beck C,Petroski EL. Prevalência de insatisfação com a imagem corporal e sua associação com a inadequação nutricional em adolescentes. R.da Educação Física/UEM. 2009; 20:25-31. DOI: 10.4025/reveducfis.v20i1.3496 [ Links ]
10. Paxton SJ, Sztainer DN, Hannan PJ, Eisenberg ME. Body Dissatisfaction Prospectively Predicts Depressive Mood and Low Self-Esteem in Adolescent Girls and Boys. J Clin Child Adolesc Psychol. 2006; 35:539-49. [ Links ]
11. Kim DS. Body image dissatisfaction as an important contributor to suicidal ideation in Korean adolescents: gender difference and mediation of parent and peer relationships. J Psychosom Res. 2009; 66: 297-303. [ Links ]
12. PMI (Prefeitura municipal de Itajaí). Perfil de Itajaí. http://www.itajai.sc.gov.br/sedeer/Perfil_de_itajai_2006.doc. (acessado em 25/07/2009). [ Links ]
13. SEDR (Secretaria de Estado de Desenvolvimento Regional). Itajaí. 2009. http://www.iai.sdr.sc.gov.br/index.php?option=com_content&task=view&id=70&Itemid=187. (acessado em 25/07/2009). [ Links ]
14. IBGE (Instituto Brasileiro de Geografia e Estatística). População recenseada e estimada, segundo os municípios - Santa Catarina - 2007. http://www.ibge.com.br/home/estatistica/populacao/contagem2007/contagem_final/tabela1_1_22.pdf (acessado em 25/06/2009). [ Links ]
15. IBGE (Instituto Brasileiro de Geografia e Estatística). Cidades: Santa Catarina - Itajaí - Produto Interno Bruto dos Municípios 2006. http://www.ibge.com.br/cidadesat/topwindow.htm?1 (acessado em 25/06/2009). [ Links ]
16. IBGE (Instituto Brasileiro de Geografia e Estatística). Cidades: Santa Catarina - Itajaí - Mapa de Pobreza e Desigualdade - Municípios Brasileiros 2003. http://www.ibge.com.br/cidadesat/topwindow.htm?1 (acessado em 25/06/2009). [ Links ]
17. PNUD (Programa das Nações Unidas para o Desenvolvimento Brasil). Índice de Desenvolvimento Humano - Municipal 1991 e 2000. http://www.pnud.org.br/atlas/ranking/IDHM%2091%2000%20Ranking%20decrescente%20 (pelos%20dados%20de% 202000).htm. (acessado em 19/06/2009). [ Links ]
18. Datasusa. Nascidos vivos - Santa Catarina. http://tabnet.datasus.gov.br/cgi/tabcgi.exe?sinasc/cnv/nvSC.def (acessado em 19/06/2009). [ Links ]
19. Datasusb. Óbitos infantis - Santa Catarina. http://tabnet.datasus.gov.br/cgi/tabcgi.exe?sim/cnv/infSC.def (acessado em 19/06/2009). [ Links ]
20. Vilela JE, Lamounier JA, Filho MAD, Neto JRB, Horta GM. Eating disorders in school children. J Pediatr. 2004; 80:49-54. http://dx.doi.org/10.2223/JPED.1133 [ Links ]
21. Tiggemann M, Wilson BE. Children's Figure Rating: relationship to self-estem and negative stereotyping. Int J Eat Disord. 1998; 23:83-88. [ Links ]
22. Barros FC, Victora CG. Epidemiologia da saúde infantil: um manual para diagnósticos comunitários. 2 ed. São Paulo: Hucitec - UNICEF; 1994. [ Links ]
23. Taylor RW, Jones IE, Williams SM, Goulding A. Evaluation of waist circumference, waist-to-hip ratio, and the conicity index as screening tools for high trunk fat mass, as measured by dual-energy X-ray absorptiometry, in children aged 3-19 y. Am J Clin Nutr. 2000; 72:490 -95. [ Links ]
24. WHO (World Health Organization). Child Growth Standards: Métodos e desenvolvimento. Índice de massa corporal para idade. Geneva: WHO; 2006/2007. [ Links ]
25. Kirkwood B. Essentials of medical statistics. Oxford: Blackwell, 1988. [ Links ]
26. Graups S, Pereira EF, Lopes AS, Araújo VC, Legnani RFS, Borgatto AF. Associação entre a percepção da imagem corporal e indicadores antropométricos de escolares. Rev Bras Educ Fís Esp. 2008; 22: 129-38. [ Links ]
27. Cachelin FM, Rebeck RM, Chung GH, Pelayo E. Does ethnicity influence bodysize preference? A comparison of body image and body size. Obes Res. 2002; 10:158 -66. [ Links ]
28. Araújo DSMS, Araújo CGS. Autopercepção e insatisfação com o peso corporal independem de frequência de atividade física. Rev Bras de Cardiol. 2003; 80:235-42. [ Links ]
29. Fernandes AER. Avaliação da imagem corporal, hábitos de vida e alimentares em crianças e adolescentes de escolas públicas e particulares de Belo Horizonte [Dissertação de Pós graduação]. Minas Gerais: Faculdade de Medicina, Universidade Federal de Minas Gerais, 2007. [ Links ]
30. Pinheiro AP. Insatisfação com o corpo em escolares de 8 a 11 anos de Porto Alegre: prevalência e fatores associados [Dissertação de Pós graduação]. Porto Alegre:Faculdade de Medicina, Universidade Federal do Rio Grande do Sul, Porto Alegre, 2003. [ Links ]
31. Solorzano CM, McCartney CR. Obesity and the pubertal transition in girls and boys. Reproduction. 2010; 140: 343-45. [ Links ]
32. Martins IS, Marinho SP. O potencial diagnóstico dos indicadores da obesidade centralizada. Rev Saúde Pública. 2003; 37: 760-67. http://dx.doi.org/10.1590/S0034-89102003000600011 [ Links ]
33. Olinto MTA, Nácul LC, Gigante DP, Dias JSC, Menezes AMB, Macedo S. Waist circumference as a determinant of hypertension and diabetes in Brazilian women: a population-based study. Public Health Nutr. 2004; 7:629-35. [ Links ]
34. Alves E, Vasconcelos FAG, Calvo MCM, Neves J. Prevalência de sintomas de anorexia nervosa e insatisfação com a imagem corporal em adolescentes do sexo feminino do Município de Florianópolis, Santa Catarina, Brasil. Cad Saúde Pública. 2008; 24:503-12. http://dx.doi.org/10.1590/S0102-311X2008000300004 [ Links ]
35. Nunes MA, Olinto MTA, Barros FC, Carney S. Influência da percepção do peso e do índice de massa corporal nos comportamentos alimentares anormais. Rev Bras Psiquiatr. 2001; 23:21-27. http://dx.doi.org/10.1590/S1516-44462001000100006. [ Links ]
36. Salles RK, Fiates GMR. Fatores de risco para o desenvolvimento de distúrbios alimentares: um estudo em universitárias. Rev Nutr. 2001;14:3-6. http://dx.doi.org/10.1590/S1415-52732001000400001 [ Links ]
37. Tiggemann M, Lowes J. Predictors of maternal control over children's eating behaviour. Appetite. 2002; 39:1-7. [ Links ]
38. Kitsantas P, Gaffney KF. Risk profiles for overweight/obesity among preschoolers. Early Hum Dev. 2010; 86: 563-68. [ Links ]
39. Giugliano R, Carneiro E. Fatores associados à obesidade em escolares. J Pediatr. 2004; 80:17-22. http://dx.doi.org/10.2223/1128 [ Links ]
40. Guimarães LV, Barros MBA, Martins MSAS, Duarte EC. Fatores associados ao sobrepeso em escolares. Rev. Nutr. 2006; 19: 05-17. http://dx.doi.org/10.1590/S1415-52732006000100001 [ Links ]
41. Suñé FR, Dias-da-Costa JS, Olinto MTA, Pattussi MP. Prevalência e fatores associados para sobrepeso e obesidade em escolares de uma cidade no Sul do Brasil. Cad Saúde Pública. 2007; 23:1361-71. http://dx.doi.org/10.1590/S0102-311X2007000600011 [ Links ]
42. Davison K, Markey CN, Birch LL. Etiology of body dissatisfaction and weight concerns among 5-year-old girls. Appetite. 2000; 35: 143-51. [ Links ]
Manuscript submitted Aug 01 2013
Accepted for publication Dec 28 2013
Corresponding author: doroaph@yahoo.com.br

{kind=link}
{kind=link}