










Serviços Personalizados
artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282
Rev. bras. crescimento desenvolv. hum. vol.24 no.1 São Paulo 2014
ORIGINAL RESEARCH
Moiré topography: an alternative to scoliosis evaluation in student's health
Júlio Guilherme SilvaI; Márcia Santos de AlmeidaII; Carolina Gomes da CostaII; Aline Fraga RochaII; Priscila Moreira da SilvaII; Rodrigo Teixeira Gomes da SilvaII; Miriam Raquel Meira MainentiIII
IPhysiotherapist, Doctor in Mental Health/Motor learning - IPUB/UFRJ, Professor of Masters Program in Rehabilitation Sciences- Augusto Motta University Center- UNISUAM-RJ
IIScientific Initiation Program (PIBIC) - Augusto Motta University Center- UNISUAM-RJ, Human Movement Analysis Lab (LAMH)
IIIPhysiotherapist, Doctor in Science - FM/UFRJ, Professor of Masters Program in Rehabilitation Sciences - UNISUAM-RJ
ABSTRACT
Moire's Topography (MT) is a method that detects scoliosis through shadows assymetry arised in the back. Few studies have discussed time of application, interpretation and operating cost. The aim of this study was to analyze operating aspescts of MT in students and to verify postural alterations by MT in the same group. 58 boys were analyzed in this study and through MT, the presence of shadow (fringes) in the back were evaluated where each assymetry corresponds to about 10o in Cobb's angle. MT marks were used to determine possible deviation. Data of interest received descriptive statistic analysis in variables such as total body mass, body mass index (BMI), weight, scoliosis, average time of analysis and diagnostic, and also the operation cost evaluation of equipment. Subjects (9,91 ± 0,79 years) showed total body mass of 37,83 ± 10,45kg, stature 1,42 ± 0,11m and BDI 18,53 ± 4,15 kg/m2. The average time of analysis was 3,25 ± 0,29min. Among subjects 75% had deviation of one fringe in toracolumbar region that shows a scoliosis less than 10º. MT represented a fast method and of low operation cost that could be an important instrument in the screening of scoliosis. We concluded that MS confirmed to be practical and of easy handling where 94,6% subjects showed scoliosis. Our data suggests that the MSP insertion in the students' health care program of scoliosis identification is possible.
Key word: scoliosis, moire topography, student, posture, postural evaluation.
INTRODUCTION
Scoliosis is a three-dimensional deformity of the spine where there is one or more curves in the frontal plane, axial rotation of the vertebrae and misalignment in the sagittal1 plane. This type of orthopedic deformity is frequent in students between 11 and 18 years of age, where 85% of cases in teenagers are of idiopathic origin2,3. At this age, the initiation and progression of scoliosis happen quickly, so there is a great need for early detection4,5. A rapid diagnosis can prevent the emergence of possible musculoskeletal complications, besides respiratory changes due to chest deformity6 .
There is a range of possibilities of analysis of musculoskeletal alterations in the image evaluation of scoliosis. So far, the X-ray is the gold-standard exam used for evaluation of scoliosis, by calculating the Cobb angle4,6. Panoramic radiography enables highly reliable monitoring of progression and / or stabilization of the deviation of the spine7,8.
However, in very young patients, there is a major concern related to the fact that x-ray exposes subjects to radiation and due to the cumulative effect in the body, it can represent a threat to health6,9 .
Thus, several investigations encourage non-invasive methods and that have high levels of reliability, so that they can become alternative to radiologic examination10,11.
Another discussion on the search for new tests for early detection of scoliosis is the cost. In our country, the price of a panoramic examination of the spine is still expensive, especially for the needy population. According to the Brazilian Institute of Geography and Statistics (IBGE) 12, there are 37 millions of Brazilians living in the poverty line, without access to a good quality of health.
As far as children are concerned, it is estimated to be 13.4 million in need of health care for various reasons12.
Given this context, it is necessary to intervene increasingly early in the detection of the deformities such as scoliosis. Thus, children of school age should be evaluated in health programs in which scoliosis would be a great object of interest.
Among the techniques for evaluation of scoliosis, we can highlight the Moiré topography, which bases its analysis through a phenomenon of shadow projection derived from optical, wherein the light projected on the back, passes through a plate and this way lines are formed, first in a reference plane, and then on the body surface, delineating surface topographically9,13. Through "fringes"and according to the asymmetry of the shadows, scoliosis is detected. In spite of being an easy technique to apply , it's still not widely used in clinical practice13-14 , especially in the health of school children.
There are few studies related to the time of analysis, interpretation and diagnosis of scoliosis using the MT. Mainly on the discussion of the operating cost and the possibility of their massification in postural analysis of school children.
This way, the objectives are: to verify postural deviations through Moiré topography in schoolchildren and, analyze the operational aspects of the application of this procedure in school children.
METHODS
Sample
This is an observational study, where 58 boys were chosen at random, students from the Rio de Janeiro public schools aged between 10 and 12 years old. As all the subjects were underage, their respective legal guardians signed a free and informed consent form, after being told the nature of the study and the protocol being carried out.
Besides that, the individuals were also aware of the benefits of participating in the survey and the absence of any kind of chemical or biological hazard in the use of MT. The evaluations took place at the Human Movement Analysis Lab (LAMH), of the post-graduation program in Rehabilitation Sciences- Augusto Motta University Center- UNISUAM-RJ. The study was approved by the Ethics Committee and Research of the Municipal Health Secretary and Civil Defense of Rio de Janeiro under # 46A/2011.
The sample size was determined by the minimum value of 58 individuals, because a confi-dence level of 95% was considered, with a power test of 80%, the population standard deviation of 0.5 and an estimated margin of error of 13%.
Subjects who did not have any type of musculoskeletal injury were eligible for the study, those who were not under any type of physical therapy for injuries and / or disorders of the musculoskeletal system and subjects without any nervous system disorders that affected the voluntary movement and muscle tone.
The excluded subjects were those who had undergone orthopedic surgery of medium/high complexity in the spine and lower limbs, children who had a shortening of the lower limbs greater than or equal to 1 cm, subjects that at the time of study had pain, acute stage of involvement of the vestibular system and musculoskeletal injuries that do not allow the permanence in the upright position unattended for five minutes.
Instrumental
The anthropometric characteristics of the sample were made using a scale with precision of 0.1 kg, with a stadiometer (0.005 m) coupled (R110, Welmy, São Paulo, Brazil).
To perform a MT, we used a room with low light, to allow identification of the Moiré effect (appearance of fringes), allowing the evaluation of possible asymmetries in the fringes and, consequently, the detection of scoliosis13. The material used consisted of: a digital camera (at least 3.0 megapixel); a moiré plate and a 500W lamp.
Procedures
For the measurement of total body mass (TBM), the student was instructed to keep both feet on the platform, unsupported and with the weight divided into the lower limbs. The height (H) was measured with the subject standing, with the subject's head in the Frankfurt plane and the end of a deep inspiration15. The Body Mass Index (BMI) was calculated by the ratio between the total body mass (kg) and squared height (m): BMI = TBM /H2, according to the World Health Organization (WHO) 16.
To perform the postural evaluation, the machine was positioned opposite the Moiré plate to a distance of 1.70 m and the slide projector with a 500W lamp was positioned to 70cm laterally. The light fell on the Moire plate at 45o (Figure 1). All components of MT respected the Takasaki equation9,13.
H= N dL/D

Where H is the distance of the individual from the plate (which is zero in this case, since the subject touches the plate ), N is the number of fringes; L is the distance of the plate to the camera and D is the inclination of the light source in the center of the plate 45 o.
The MT plate consists in an acrylic plate with black stripes, 1mm thick separated from each other by 1mm. The subjects were positioned with shoulders, arms relaxed, eyes fixed on the horizon and with the back leaning against the plate (fig. 1).
According to Knackfuss et al.13, the shadows in the back create figures called "O" superior, "M1", "W", "M2" e "O" inferior that represent the scapular regions, upper back, thoracolumbar, lumbar and glutes respectively (figure 2).

Any asymmetry in these figures showed a postural deviation. The interest alterations in that study were in figures "M1", "M2", "W1" e "W2". The pictures were analysed in the computer and for the evaluation of possible deviations, a straight line starting at C7 prominence to the intergluteal (PQ) line was drawn in the picture.
In the fringe that deviates more, we marked its minimum point (X). A perpendicular line to line PQ passes by limit X. In the other hemibody, we marked the Y point, equidistant of X. If the back is symmetric, X and Y will be situated in the same fringe. In case they aren't, the deviation value will be the same as the number of fringes situated between the one that has point X and to the one that has point Y, including the line with Y13.
Data analysis
Descriptive analyzes were performed on the following variables: total body mass , height, BMI, appearances or not of scoliosis, type and segment of scoliosis, the average time for analysis and diagnosis, as well as analysis of the operating cost of the equipment.
The numerical variables were presented as mean ± standard deviation and categorical variables as absolute frequency (n) and relative (%). For processing of the data a SPSS program version 20 was used.
RESULTS
Among the 58 students evaluated (average 0.79 ± 9.91 years old) had a total body mass of 37.83 ± 10.45 kg, height 1.42 ± 0.11 me BMI of 18.53 ± 4.15 kg/m2. About the average time for evaluation of the photos, the average time spent by the evaluators was 3.35 min. Another point was that during the research there were no sample losses.
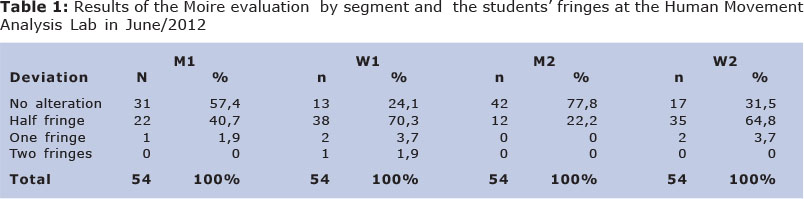
In the evaluation using MT, the data pointed to asymmetries in the points of interest in 76% of "W1", 65% in "W2", 42.6% of "M1" and 22% of "M2" (Table 1).
DISCUSSION
There was a group of students that showed low angular value Scoliosis (half fringe) in the figures of "M" and "W". Such information is of great importance, because it has been already proved in the literature the high level of reliability of the MT with just a 3% margin of error in relation to the gold standard that is the Cobb angle17-18. Despite this fact, the technique encourages discussions and remains being improved through computational resources for the standardization of application and decrease of the margin of error13,19-20.
The postural analysis of individuals in school age proposes the detection of idiopathic scoliosis common in this age group10,21, the bone growth accelerated in this stage of life promotes the rapid increase of the angle of scoliosis and it may lead to irreversible complications and if there is no early intervention6,20.
The results support to alert the need of a rapid method of analysis of scoliosis and the MT can fill this gap. Especially, in the applicability in the health of school children, being an important vector in attention to primary health23. The MT can facilitate the introduction of a routine in postural evaluation in Brazilian schools, promoting early diagnosis, reliable, low cost, without exposing the child to radiation24-25.
According to the results found in our study, we can affirm that individuals who showed half fringe deviation have approximately scoliosis of less than 10 ° of the Cobb angle17-18. Such fact shows that the process of vertebral rotation is present and the low angular value is the beginning of a scoliosis.
As scoliosis below 10 o are imperceptible to physical examination, the MT confirmed to be a method of easy detection of low angular value scoliosis and the data are in accordance to the literature9-13, which deviation of half-fringe in region W1 was detected in 70.3% of subjects.
In the contribution of Ueno et al20, 3.424 subjects presented scoliosis. (N=250.000 children evaluated). When compared to the X-ray, 65% of children had the Cobb angle above 10º and prevalence of scoliosis curves were in the range of 10º - 19º. The results show that a slight increase in prevalence rates of children with a higher magnitude curve (e"20°), in relation to the last epidemiological study conducted in Japan by Ohtsuka et al26. Furthermore, 35% of the subjects had a scoliosis lower than 10 °, it means, a deviation of no more than one fringe at MT.
The tracking of postural deviations in students is a big challenge in Brazil, since there are few health programs in schools that has as a scope the evaluation and monitoring of scoliosis. Based on this premise, there are only programs of prevalence study. Souza Junior et al27 evaluated the prevalence of scoliosis in schoolchildren in the city of Juazeiro do Norte, Ceará - Brazil.
In a universe of 2,432 students enrolled in public schools, 670 students between 11 and 19 years were randomly selected. In the methodology we used only the observation of spinal deformity in the back during flexion of the trunk and the asymmetry of the shoulders and pelvis. The results showed a prevalence of 8.8% with deviation of the spine, especially thoracolumbar. We emphasize that in this study there was no quantification of the degree of deviation, and as low angular scoliosis values, lower than 10º, are imperceptible to the naked eye, there were probably underestimated negative cases. Such fact corroborates with our results with a high prevalence of scoliosis, 94.4% as the data of Ueno et al20 that found scoliosis in more than 65% of japanese while 35% of this with low angular value.
The high prevalence of our results can be explained by the great power of MT in detecting scoliosis in the initial phase of low angular value. This may put into question the methodology of most studies on the prevalence of scoliosis since, according to Andersen et al28 and Wong et al29, showed a world prevalence of scoliosis between 1 and 2%. In Brazil, the data are similar where Leal et al30 showed from 1 to 4%. In another Brazilian study, Nery et al31showed that the prevalence of lateral deviation of the spine was 1.4%.
Most studies of prevalence of scoliosis detected scoliosis higher than 10º and used the Adams test30-31. Besides that, Leal et al30 exposed the subjects to X-ray.This point reinforces the possibility of contribution of MT in the investigation of scoliosis. Especially for the easy implementation, little expertise is needed to carry out the examination and there is no exposure to x-ray. Referring to the Adams test used by Leal et al30 e Nery et al.31, the spinal deformity will be detected in scoliosis with higher angular value, which limits early intervention of professionals of health, because what determines the scoliotic process, regardless of question, is the vertebral rotation. Among the methods available, the most sensitive to this factor is the MT13.
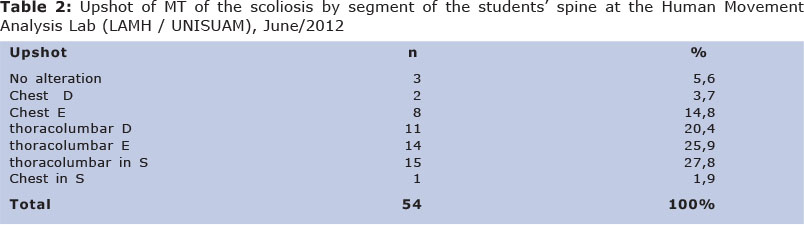
Referring to the findings (Table 1 and 2), it is confirmed that the MT is a fast method, that added to its low operating cost (approximately one thousand reais - plate, 12 pixels digital camera, tripod and 500W lamp) makes it easier to use in scoliosis detection programs scoliosis.
Thus, it is concluded that the MT confirmed to be a fast method of analysis with an average of 3.2 min to capture and analysis of the photograph. Low angular value scoliosis was detected in 94.4% of the sample and only for a prevalence of 5.6% of subjects without changes. The easy handling appears as a great feature of the method and it can be applied to large samples, in detection scoliosis projects.
REFERENCES
1. Nowakowski A, Dworak LB, Kubaszewski L, Kaczmarczyk J. Spinal alignment in surgical, multisegmental, transpedicular correction of adolescent idiopathic scoliosis. Med Sci Monit. 2012; 18(12): 181-187. [ Links ]
2. Döhnert MB, Tomasi E. Validade da fotogra-metria computadorizada na detecção de escoliose idiopática adolescente. Rev Bras Fisioter 2008; 12(4) 290-7. [ Links ]
3. Fernandes L, Crescentini MCV, Poletto PR, Gotfryd AO, Yi LU. Qualidade de vida e funcionalidade em adolescentes com escoliose idiopática: es-tudo piloto. Fisioter Mov 2012; 25 (1): 73-8 [ Links ]
4. Fletcher ND, Bruce RW. Early onset scoliosis: current concepts and controversies. Curr Rev Musculoskelet Med. 2012; 5 (2): 102-10. [ Links ]
5. Lenke LG. Commentary: Continuing the quest for identifying specific criteria for the progression of adolescent idiopathic scoliosis. Spine J. 2012;12(11): 996-7 [ Links ]
6. Minghelli B. Rastreio escolar: a importância na detecção precoce de posturas escolióticas em adolescentes das escolas de Silves, Algarve. Rev. Port. Sau. Pub. 2008; 26 (2): 61-8. [ Links ]
7. Adobor RD, Riise RB, Sørensen R, Kibsgård TJ, Steen H, Brox JI Scoliosis detection, patient characteristics, referral patterns and treatment in the absence of a screening program in Norway. Scoliosis; 2012; 7 (1): 18. [ Links ]
8. Cardoso LR, Gonçalves C, Bonvicine C; Barboza MAI. Análise clínica e radiográfica pré e pós-tratamento conservador na escoliose idiopática do adolescente: Estudo de caso. ConScientiae Saúde 2011, 10(1):166-74. [ Links ]
9. Porto F, Gurgel JL, Russomano T, Farinatti PTV. Moiré topography: Characteristics and clinical application. Gait Posture. 2010; 32: 422 - 424. [ Links ]
10. Ferreira DMA, Suguikawa TR, Pachioni CAS, Fregonesi CEPT, Camargo MR. Rastreamento escolar da escoliose: medida para o diagnóstico precoce. Rev Bras Crescimento Desenvolvimento Hum. 2009; 19 (3): 357-68. [ Links ]
11. Morita AK, Faria CRS, Pachioni CAS, Ferreira DMA. Mensuração da gibosidade e a sua correlação com medidas radiológicas na esco-liose. Colloquium Vitae 2011; 3(1): 27-31. [ Links ]
12. IBGE - Instituto Brasileiro de Geografia e Estatística. Indicadores sociais: uma análise das condições de vida. Estudos & Pesquisas - Informação Demográfica e Socioeconômica nº 27, 2010. [ Links ]
13. Knackfuss IG,Silva JG, Reis FJJ, Paula BM, A, Cardoso FGC, Omena TP et al. A utilização da estereofotografia de moiré na detecção de escolioses. Rev Fisioter Brasil. 2004; 5(5): 357-61. [ Links ]
14. Porto F, Gurgel JL, Farinatti PTV. Topografia de Moiré como Método de Avaliação Postural: Revisão do Estado da Arte. Rev. Bras. Geriatr. Gerontol 2011; 14(3): 567-577. [ Links ]
15. ISAK - International Society for the Advancement of Kinanthropometry. International Standards for Anthropometric Assessment. Australia: ISAK, 2001. [ Links ]
16. WHO - World Health Organization. Obesity - Preventing and Managing the Global Epidemic. 1998;1-158. [ Links ]
17. Lu D, Xu C, Sun J. Application of image processing technique in scoliosis detection. Sheng Wu Yi Xue Gong Cheng Xue Za Zhi. 2012; 29 (4):663-8. [ Links ]
18. Luk KD, Lee CF, Cheung KM, Cheng JC, Ng BK, Lam TP et al. Clinical effectiveness of school screening for adolescent idiopathic scoliosis: a large population-based retrospective cohort study. J. Spine. 2010; 35 (17): 1607-14. [ Links ]
19. Illés T. Comparison of classical 2D measurement of scoliosis and 3D measurement using vertebral vectors; advantages for prognosis and treatment evaluation. Bull Acad Natl Med. 2011; 195(3):629-42 [ Links ]
20. Ueno M, Takaso M, Nakazawa T, Imura T, Saito W, Shintani R et al. A 5-year epidemiological study on the prevalence rate of idiopathic scoliosis in Tokyo: school screening of more than 250,000 children. J Orthop Sci. 2011;16(1):1-6. [ Links ]
21. Lee CF Fong DY, Cheung KM, Cheng JC, Nig BK , Lam TP et a.Referral criteria for school scoliosis screening: assessment and recommendations based on a large longitudinally followed cohort. Spine 2010; 35(25) 1492-8. [ Links ]
22. Minghelli B, Abílio FDG, Góis AA, Timóteo AL, Florença HA, Lóia NH et al. Prevalência de alterações posturais em crianças e adolescentes em escolas do Algarve. Rev. Saúde e Tecnologia 2009; 4: 33 - 37. [ Links ]
23. Linker B. A dangerous curve: the role of history in america's scoliosis screening programs. American Journal of Public. 2012; 102(4): 606-616. [ Links ]
24. Wilczyñski J. The most common faulty postures among boys aged 13-16 years measured by Moiré's photogrammetric method. Med Pr. 2006; 57(4): 347-52. [ Links ]
25. Parent EC, Damaraju S.,Hill DL, Lou E, Smetaniuk D. Identifying the Best Surface Topography Parameters for Detecting Idiopathic Scoliosis Curve Progression. Stud Health Technol Inform. 2010; 158: 78-82. [ Links ]
26. Ohtsuka Y, Yamagata M, Arai S, Kitahara H, Minami S. School screening for scoliosis by the Chiba university medical school screening program-results of 1.24 million students over an 8-year period. Spine. 1988;13:1251 - 6. [ Links ]
27. Souza Junior JV, Sampaio, RMM, Aguiar, JB, Pinto FJM. Perfil dos desvios posturais da coluna vertebral em adolescentes de escolas públicas do município de Juazeiro do Norte - CE Fisioter pesqui 2011; 18(4): 311-316. [ Links ]
28. Andersen MO, Thomsen K, Kyvik KO. Adolescent idiopathic scoliosis in twins: a population-based survey. Spine. 2007;32(8):927-30. [ Links ]
29. Wong HK, Hui JHP, Rajan U, Chia HP. Idiopathic Scoliosis in Singapore schoolchildren. A prevalence study 15 years into the screening program. Spine 2005; 30(10): 1188-96. [ Links ]
30. Leal JS, Leal MCPS, Gomes CER, Guimarães MDC. Inquérito epidemiológico sobre escoliose idiopática do adolescente. Rev Bras Ortop 2006; 41(8): 309-19. [ Links ]
31. Nery LS, Halpern R, Nery PC, Nehme KP, Stein AT. Prevalence of scoliosis among school students in a town in southern Brazil. São Paulo Med. J. 2010;128(2):69-73. [ Links ]
Manuscript submitted Aug 01 2013
Accepted for publication Dec 28 2013
Corresponding author: jglsilva@yahoo.com.br

{kind=link}
{kind=link}
{kind=link}