










Services on Demand
article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Share

 Permalink
PermalinkJournal of Human Growth and Development
Print version ISSN 0104-1282
Rev. bras. crescimento desenvolv. hum. vol.24 no.1 São Paulo 2014
ORIGINAL RESEARCH
Analisys of the prevalence of overweight and obesity and the level of physical activity in children and adolescents of a southwestern city of São Paulo
Thays Fernanda Castilho CabreraI; Ingrid Fernandes Leite CorreiaI; Daiane Oliveira dos SantosI; Francis Lopes PacagnelliI; Maria Tereza Artero PradoI, II; Talita Dias da SilvaII, III; Carlos Bandeira de Mello MonteiroII, III; Deborah Cristina Gonçalves Luiz FernaniI, II
IFaculdade de Ciências da Saúde, Universidade do Oeste Paulista (UNOESTE), Presidente Prudente/SP
IILaboratório de Delineamento de Estudos e Escrita Científica, Faculdade de Medicina do ABC, Santo André/SP
IIIEscola de Artes, Ciências e Humanidades, Universidade de São Paulo (USP), São Paulo/SP. Study carried out at Universidade do Oeste Paulista, Presidente Prudente/SP
ABSTRACT
This study aimed to verify the prevalence of overweight, obesity and physical activity level according to the sex of children and adolescents from public schools city of Nantes, São Paulo, Brazil. The sample consisted of 170 children and 232 adolescents with a mean age of 8.04±1.31 and 13.2±1.83 years, respectively, of both sex and frequenters of two schools. Anthropometric measurements were collected: body mass index by age (BMI/age) and abdominal circumference. The BMI/age was classified according to the Sistema de Vigilância Alimentar e Nutricional (SISVAN) (2007) and a modified, adapted and suggested questionnaire by Silva (2009) was used to analyze the physical activity level. An unpaired t test was used and p-values < 0.05 were considered significant. The prevalence of 30.59% of the overweight or obese individuals, most of them adolescents, was verified. A higher media was also found with a significant value difference of the abdominal circumference in the females sex in the children group. It was observed that 62.68% of the sample was inactive or inadequately active and that most were female. Those facts demonstrate the sizable risk that these individuals may present for cardiovascular and musculoskeletal complications throughout life. The importance of the early educational and nutritional programs in schools should be emphasized with the prevention and treatment of overweight and low physical activity level individuals.
Key words: prevalence, overweight, obesity, child, adolescent, exercise.
INTRODUCTION
According to the World Health Organization (WHO)1, overweight and obesity are described as an excessive or unnatural accumulation of fat that affects health. The fundamental cause is an imbalance between consumed and spent calories, generally the result of inappropriate eating patterns, with ingestion of highly energetic food rich in fat and physical inactivity, known as sedentary. In 2011 there were more than 40 million overweight children younger than five years in the world.
Knowing that those indexes are rising and that the gain of weight is associated with mortality and morbidity risk, and consequently, the reduction of life expectation, it is the causal factor for the higher costs in health care during the life of these individuals2.
Among the health problems that these individuals can present are cardio-metabolic as dyslipidemia, insulin resistance (type 2 diabetes) and high blood pressure3, besides other problems as depression4, compromised quality of life5 and low self-esteem6.
Worldwide searches verified that excessive weight (overweight and obesity) has increased globally with alarming rates. In Taiwan, China the prevalence of overweight during childhood almost doubled between 1986 (13%) and 2009 (27.7%)7. Also, a study conducted in the United States revealed that 31.8% of the children between 2 and 19 were overweight or obese8. In New Zealand, a study evaluating 9107 adolescents' students verified that 31.7% of the students presented overweight or obesity and 2.5% severe obesity9.
In Brazil, the prevalence in young people has increased in the last decades in all regions and social classes. Information about the nutritional status of the Brazilian children show the prevalence of excess weight in children from 5 to 9 years in the North and Northeast region of the country ranged from 25% to 30% and in Southeast, South and Midwest regions, from 32% to 40%. But in the population from 10 to 19 years, the increases were more intense: from 3.7% to 21.7% for boys, and from 7.5% to 19.4% for girls between the periods of 1974-1975 to 2008-200910.
Convincing information has been reported showing that the practice of physical activity during childhood could be related to a reduced risk of developing overweight and obesity, being an extremely important health element, because it has positive effects beyond well-being, addressing cardiovascular and musculoskeletal health11.
Behavioral factors are already known to be acquired during childhood and adolescence and persist for life, and as such, owing to the constant increase of these individuals with excess of weight and the emergence of precociously chronic degenerative diseases, research that evaluates the excess of weight and the physical activity level of these individuals has become essential to enable creating prevention strategies, intervention and better habits for better quality of life in the short and long-term12,13.
Other studies that cover this topic were predominantly conducted with the population from major centers. However, this study had emphasizes to determinate the existence of overweight and obesity previously described, but in a small metropolitan region. Thus, the aim of this study was to verify the prevalence of overweight, obesity and the physical activity level according to the sex of the children and adolescents from public schools city of Nantes, São Paulo, Brazil.
METHODS
This was a transversal study approved by the Ethics Committee of the Universidade do Oeste Paulista in Presidente Prudente, São Paulo state, under the protocol number 1203/12. This study was conducted in both schools of Nantes, São Paulo state, both in the public school system, after authorization by the municipal educational department of the city.
The sample was composed of 402 students aged between 6 and 17, and from both sexes, and were divided into two groups: the children group (CGr) with 170 individuals, aged between 6 and 11 years and the adolescents group (AGr) with 232 individuals aged between 12 and 17 years. The inclusion criteria included individuals to be currently enrolled and attending one of the two selected schools and authorization from the parent or person responsible for the individuals to participate in the study by signing an informed consent form. Individuals who presented neurological and metabolic diagnostic were excluded from the study. Evaluations were conducted during school hours (morning and afternoon in the schools during the period from September 2012 to February 2013. To verify anthropometric measurements: body mass index by age (BMI/age) and abdominal circumference (AC), were taken based on the methodology stated by Moser et al. (2011)14.
First, information as to the sex, age, weight and height of the students was collected. Weight measurement was made with Plena® digital scale (Minneapolis, MN, USA) with maximum capacity of 160 kg and increments of 100 grams. The individual was positioned standing on the center of the platform, barefooted and with arms free alongside the body. Clothing worn by the students consisted of a school uniform (shorts and T-shirt).
The height assessment, in meters (m), was made with a tape measure fixed onto a flat wall, with increments of 0.1m. The individual was positioned in orthostatism, on barefoot, with a occipital region, scapular waist, pelvic and the posterior region of the heel in contact with the wall, while the head remained on a Frankfurt horizontal plane.
AC was measured in centimeters (cm) with a cloth measuring tape with increments of 0.1cm, placed on the umbilicus scar and at the same time to the ground, while the individual was kept in orthostatism, with the feet together, relaxed stomach and with the arms free alongside the body.
To establish a nutritional diagnosis, the classification of BMI/age according to the Sistema de Vigilância Alimentar e Nutricional (SISVAN)15, was used, which has been used in the Brazilian population and adapted to WHO cutoff points by the analyses of the growth curves, in which the classifications are the following: percentile < 0.1 corresponds to extremely underweight; percentile ≥ 0.1 to < 3 = underweight; percentile ≥ 3 to < 85 = healthy weight; percentile > 85 to 97 = over-weight; percentile > 97 to < 99.9 = obesity and percentile > 99.9 = severe obesity.
A modified and adapted questionnaire suggested by Silva (2009)16 was used, formulated from the most used questionnaires to verify physical activity17-19. To analyze the physical activity level, this questionnaire approaches the ways of displacement and the physical activities realized in and out the school, and sedentary time, which includes the time of watching television, playing on the computer or video-games and speaking on the phone.
After the students answer the questionnai-re with an interview from the study, they were classified according to the frequency and intensity of the exercises realized: inactive (students who did not realize any physical activity); inadequately active (students who realized physical activity on a frequency of twice or less, or with an inferior duration of one hour per week); active (students who realized physical activities three times or more per week and with a superior duration of one hour).
Each item collected in this study (weight, height, AC, physical activity level questionnaire) was made by the same interviewer in all of the evaluated students.
Statistical analyses were elaborated by an electronic database (Excel®) and the data were expressed in absolute and relative numbers. To verify the differences between the sexes of the groups, unpaired t test was used, p-values < 0.05 were considered significant.
RESULTS
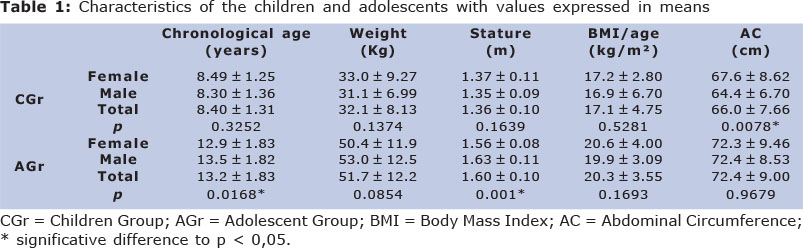
From the 402 students in the current study, 210 (52.2%) were girls and 192 (47.8%) were boys. The total mean in the chronological age of the evaluated individuals in CGr was 8.40±1.31 years and in AGr was 13.2±1.83 years, and in the AGr, there was a significant difference between sex in relation to chronological age (p=0.0168) and the stature of the individuals (p=0.001). The values referring to mean AC in CGr was 66.0±7.66 cm and in AGr was 72.4±9.00 cm, but in CGr there was a significant difference between sex (p=0.0078) (Table 1).
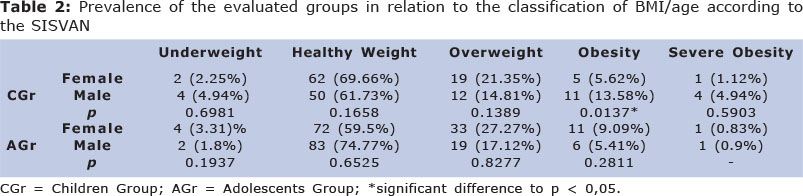
In relation to the diagnosis of BMI/age according SISVAN, 123 (30.59%) of the total evaluated sample had weight above the appropriate limit for the age, in other words, obtained an overweight, obesity or severe obesity classification. From these 30.59% of the individuals with weight excess, 52 (12.93%) are from CGr and 71 (17.66%) were from AGr. The values corresponding to each classification of BMI/age in relation to sex in CGr and AGr are shown in Table 2. There was a significant difference only in CGr in relation to sex in the obesity classification (p=0.0137).
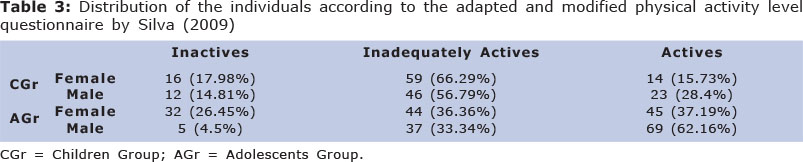
On the assessment of physical activity, 133 (78.24%) of the individuals in CGr and 118 (50.86%) in AGr were verified to be inactive or inadequately active, in other words, 251 (62.44%) of the total sample did not realize physical activity accordingly. It was observed that females showed physical activity in lower proportion than males for both groups (Table 3).
DISCUSSION
This study observed an expressive value (30.59%) of the evaluated individuals that presented weight above that appropriate for age, most of these individuals were from group AGr, but only the obesity classification by SISVAN15 for CGr in relation to sex obtained a significant difference. A higher mean and a significant difference in the value of AC for females in relation to males for CGr were found and there was a significant difference in the chronological age and stature for AGr. In relation to the physical activity, more than half of the sample, 251 students (62.44%), were observed to be inactive or inadequately activity and that most of these individuals were from the female sex in both groups.
Chen et al.20, evaluating the relation between the perinatal factors and social demographic, familiar environment, behavior, with the risk of obesity and overweight in individuals from 9 to 14 years in Taiwan, verified that 49.8% of its sample presented weight excess (32.3% overweight and 17.5% obesity), as these values were superior to those found in our study in which 123 individuals (30.59%) of the sample presented overweight, obesity or severe obesity.
It is possible to observe the percentage differences in relation to the excess of weight (overweight or obesity) comparing female and male sex in our study. In relation to the classification of overweight, the female sex was verified to present a higher number with overweight than male sex, in the CGr (21.35% girls and 14.81% boys) as much as the AGr (27.27% girls and 17.12% boys).
The classification of obesity in CGr (5.62% girls and 13.58% boys) the highest percentage values are in relation to boys, yet in the AGr in relation to the girls (9.09% girls and 5.41% boys). On the severe obesity both groups (CGr: 1.12% girls and 4.94% boys; AGr: 0.83% girls and 0,9% boys) the highest percentage values were for the boys.
The research of Bac et al.21 had the objective to analyze the index of overweight and obesity in boys and girls, from 6 to 13 years, that live in rural and urban environment and found the overweight level for girls in rural areas was 16.49% and in the urban areas 16.9%, but boys from rural areas had the value 28.14% and from urban areas 27.31%. In relation to obesity, the authors verified the reverse: 4.12% of obese girls were from rural areas and 3.44% from urban, while 3.52% of the boys were from rural areas and 7.78% from urban areas.
The findings of Bac et al.21 differs from this search in two ways.The first is that those authors analyzed the excess weight in relation to the area in which the children lived (rural and urban) and the other is that the boys represented the highest proportion of overweight and obesity.
Although social economics variables were not analyzed in this study and the two evaluated schools were public in a small town in the countryside of São Paulo state, the children and adolescents showed the elevated level of overweight and obesity. Studies suggest that the families of the children and adolescents that attend private schools are the ones who belong to the social economic group with the higher purchasing power and in these groups, the studies have found a prevalence in overweight and obesity when comparated to the group with lower purchasing power22-24.
Moser et al.14 evaluated the frequency of high blood pressure in boys and girls from 10 to 16 years of age and analyzed its association with the excess of body weight and abdominal obesity.
Analyzing the measures of the AC in relation to sex, it was revealed that abdominal obesity was more frequent in girls (37.1%; n=148) than in boys (28.8%; n=105), with significant difference (p=0.0146), as this finding partly collaborates with the findings of this study, in which in the CGr girls presented a higher value of AC (67.6±8.62 cm) than boys (64.4±6.70 cm) with a significant difference (p<0.0078), but in the AGr the values are very similar and there was no difference according to sex (female: 72.3±9.46 cm and male: 72.4±8.53 cm).
Studies have verified the increased proportion of abdominal obesity in American25 and British26 children and adolescents, while a growth in frequency was also found, especially in the female sex.
Klein-Platat et al.11, analyzing if physical activity was related to AC in adolescents, observed that 20.2% of the sample presented overweight and there was no difference in relation to sex.
However, verifying that boys presented a higher AC than girls (67.6±9.1 and 65.7±8.9 cm respectively, p<0.0001).This fact, as well as the CGr to the AGr, directly differers from this study, has previously been mentioned. In that same study, AC was also observed to be negatively associated to structured physical activity and positively associated to sedentary in girls and boys. Beyond reporting the high measurements in AC are in indications of abdominal fat and suggests that a structured physical activity could have a beneficial effect on the cardiovascular and metabolic risks in particular with the presence of excess weight11. Besides this, Gonçalves et al.27 showed in your study that obese children perceived themselves as less competency to school, sport, low self-esteem, inadequate acceptance of physical appearance and social.
The individuals evaluated in this study showed a low level of physical activity, where 78.24% of the CGr and 50.86% of the AGr were inactive or inadequately active (total of 62.44% of the sample), which means that more than half of the individuals evaluated did not exercise or did not exercise enough. According to the analysis by sex, we could see that there was a predominance of girls inactive or inadequately active in both groups (GrC= 75 and GrA= 76).
According to Hallal et al.28, who studied the prevalence of sedentary and associated factors between 4452 children with ages from 10 to 12 years old in Pelotas (Rio Grande do Sul state), they verified that the prevalence of sedentary was 58.2%, being positively associated to female sex, social economic level, having an inactive mother and daily hours of television watching and negatively associated with the daily time playing videogames.
The authors also affirm the importance to realize strategies to fight sedentary in adolescents, due to the high prevalence and for being associated to adult physical inactivity. Additionally, Baruki et al.29 verified in his studies that eutrophic chindren are more active, as they practice more intense exercises and dedicate less time watching television and playing videogames than overweight children.
Shokrvash et al.30 described that evaluated adolescents did not show appropriated time to physical activity. However, there was a significant difference related to physical activity between sex, where girls presented higher risk of low level of physical activity. This result was also observed in this study, where there were a higher number of girls who were inactive or inadequately active compared to boys.
A limitating factor of this study can be the cross-sectional design of the study, despite feedback to those responsible in the participating schools. Even so, Mascarenhas et al.31 emphasized in your study the importance of defining references for each region and constantly updating them to follow up the temporal trends of BMI.
In conclusion, higher levels of AC was found in girls in the CGr and results similar between sex in AGr that show an elevated health risk to those people exposed. Additionally, there was a high prevalence of overweight and obesity in both sex, in the children and adolescents measured. According to sex, there was a higher rate of: overweight in female in the CGr and AGr; obesity in male in the CGr and female in AGr, and severe obesity in boys between both groups. Related to the level of physical activity, a major part of the sample was verified to be inactive or inadequately active with predominance of the female sex.
Those facts show the high risk of cardiovascular and musculoskeletal complication that those individual can present during life. The importance of realization of an early educational program and nutritional at school has to be emphasized to prevent and treat those individuals overweight and with low levels of physical activity.
REFERENCES
1. World Health Organization - WHO. Obesity and Overweight. [online] 2013. [cited 2013 May 15]. Available from: http://www.who.int/mediacentre/factsheets/fs311/en/. [ Links ]
2. Wang G, Dietz WH. Economic burden of obesity in youths aged 6 to 17 years: 1979-1999. Pediatrics. 2002;109: 81-1. [ Links ]
3. Lambert M, Delvin EE, Levy E, O'Loughlin J, Paradis G, Barnett T, et al. Prevalence of cardiometabolic risk factors by weight status in a population-based sample of Quebec children and adolescents. Can J Cardiol. 2008; 24, 575-83. [ Links ]
4. Needham B, Crosnoe R. Overweight and depression during adolescence. J Adolesc Health. 2004;36:48 - 55. [ Links ]
5. Schwimmer JB, Burwinkle TM, Varni JW. Health-related quality of life in severely obese children and adolescents. JAMA. 2003; 289: 1813 - 9. [ Links ]
6. French SA, Story M, Perry CL. Self esteem and obesity in children and adolescents: A literature review. Obes Res. 1995;3:479 - 90. [ Links ]
7. Chen LJ, Fox KR, Haase A, Wang JM. Obesity, fitness and health in Taiwanese children and adolescents. Eur J Clin Nutr. 2006; 60: 1367 - 75. [ Links ]
8. Ogden CL, Carroll MD, Kit BK, Flegal KM . Prevalence of obesity and trends in body mass index among US children and adolescents, 1999-2010. JAMA. 2012; 307(5): 483 - 90. [ Links ]
9. Farrant B, Utter J, Ameratunga S, Clark T, Fleming T, Simon D. Prevalence of severe obesity among New Zealand adolescents and associations with health risk behaviors and emotional well-Being. J Pediatr. 2013; 25: 1 - 7. [ Links ]
10. Friedrich RR, Schuch I, Wagner MB. Effect of interventions on the body mass index of school-age students. Rev Saúde Pública. 2012; 46(3): 551 - 60. [ Links ]
11. Klein-Platat C, Oujaa M, Wagner A, Haan MC, Arveiler D, Schlienger JL, et al. Physical activity is inversely related to waist circumference in 12-y-old French adolescents. Int J Obes. 2005; 29: 9 - 14. [ Links ]
12. Sichieri R, Souza RA. Strategies for obesity prevention in children and adolescents. Cad Saude Publica. 2008; 24: 209 - 23. [ Links ]
13. Feferbaun R, Leoni C, Nogueira RC, Cavalcanti PN, Cardoso EB, Serra M. A 10-month anthropometric and bioimpedance evaluation of a nutritional education program for 7 - to 14-year-old students. J Hum Growth Dev. 2012; 22(3): 283 - 290. [ Links ]
14. Moser DC, Milano GE, Brito LMS, Titski ACK, Leite N. Pressão arterial elevada, excesso de peso e obesidade abdominal em crianças e adolescentes. Rev Educ Física/UEM. 2011; 22(4): 591 - 600. [ Links ]
15. Sistema de Vigilância Alimentar e Nutricional (SISVAN). Curvas de Crescimento da Organização Mundial da Saúde (OMS). [online] 2007. [cited 2013 Apr 8]. Available from: http://nutricao.saude.gov.br/sisvan.php?conteudo=curvas_cresc_oms. [ Links ]
16. Silva BO. Questionários de Avaliação da Atividade Física e do Sedentarismo em Crianças e Adolescentes. Rev Derc. 2009;15(45):14 - 18. [ Links ]
17. Aaron DJ , Kriska AM , Dearwater SR, Anderson RL , Olsen TL , Cauley JA, et al. The epidemiology of leisure physical activity in an adolescent population. Med Sci Sports Exer. 1993; 25: 847-53. [ Links ]
18. Booth ML, Okely AD, Chey T, Bauman A. The reliability and validity of the physical activity questions in the WHO health behaviour in schoolchildren (HBSC) survey: a population study. Br J Sports Med. 2001; 35: 263-7. [ Links ]
19. National Health and Nutrition Examination Survey (NHANES). Codebook for data release (2001-2002). Physical activity section of the SP and MEC CAPI questionnaires (PAQ-B). [cited 2013 May 4]. Available from: http://www.pop.psu.edu/data-archive/codebooks/nhanes/01_02/quest/paq_b_cbk.pdf. [ Links ]
20. Chen YC, Chen PC, Hsieh WS, Portnov BA, Chen YA, Lee YL. Environmental factors associated with overweight and obesity in taiwanese children. Paediatr Perinat Epidemiol. 2012; 26(6): 561 - 71. [ Links ]
21. Bac A, Wozniacka R, Matusik S, Golec J, Golec E. Prevalence of overweight and obesity in children aged 6-13 years- alarming increase in obesity in Cracow, Poland. Eur J Pediatr. 2012;171:245 - 251. [ Links ]
22. Leão LSCS, Araújo LMB, Moraes LTLP, Assis AM. Prevalência de obesidade em escolares de Salvador, Bahia. Arq Bras Endocrinol Metab. 2003; 47(2): 151 - 7. [ Links ]
23. Ronque ERV, Cyrino ES, Dorea VR, Junior HS, Galdi EHG, Arruda M. Prevalência de sobrepeso e obesidade em escolares de alto nível socioeconômico em Londrina, Paraná, Brasil. Rev Nutr. 2005; 18(6): 709 - 17. [ Links ]
24. Balaban G, Silva GAP. Prevalência de sobrepeso e obesidade em crianças e adolescentes de uma escola da rede privada de Recife. J Pediatr. 2001; 77(2): 96 - 100. [ Links ]
25. Lee S, Bacha F, Arslanian SA. Waist circumference, blood pressure, and lipid components of the metabolic syndrome. J Pediatr. 2006; 149: 809 - 16. [ Links ]
26. McCarthy HD, Ellis SM, Cole TJ. Dramatic increases in central overweight and obesity in British children aged 11 - 16 year: cross-sectional surveys of waist circumference. Br Med J. 2003; 326: 624 - 7. [ Links ]
27. Gonçalves S, Silva D, Antunes H. Psychosocial correlates of overweight and obesity in infancy. J Hum Growth Dev. 2012; 22(1): 179-186. [ Links ]
28. Hallal PC, Bertoldi AD, Gonçalves H, Victora CG. Prevalence of sedentary lifestyle and associated factors in adolescents 10 to 12 years of age. Cad Saude Publica. 2006; 22: 1277-87. [ Links ]
29. Baruki SB, Rosado LE, Rosado GP, Ribeiro RC. Association between nutritional status and physical activity in Municipal Schools in Corumbá - MS. Rev Bras Med Esporte. 2006;12:90-4. [ Links ]
30. Shokrvash B, Majlessi F, Montazeri A, Nedjat S, Rahimi A, Djazayeri A, Shojaeezadeh D. Correlates of physical activity in adolescence: a study from a developing country. Glob Health Action. 2013;6:203-27. [ Links ]
31. Mascarenhas LPG, Smolarek AC, Bozza R, Boguszewski MCS, Prati FS, Stabelini Neto A, et al. Cutoff for body mass index in adolescents: comparison with national and international reference standards. J Hum Growth Dev. 2011; 21(3): 798 - 807. [ Links ]
Manuscript submitted Aug 01 2013
Accepted for publication Dec 28 2013
Corresponding author: deborah@unoeste.br
Funding institution: Universidade do Oeste Paulista (Unoeste), Protocol 1203/12.

{kind=link}
{kind=link}
{kind=link}