










Services on Demand

article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators
Share

 Permalink
PermalinkJournal of Human Growth and Development
Print version ISSN 0104-1282
Rev. bras. crescimento desenvolv. hum. vol.24 no.3 São Paulo 2014
ORIGINAL RESEARCH
Inflammatory breast neoplasms: a systematic review
Naidhia Alves Soares FerreiraI, II; Sionara Melo Figueiredo de CarvalhoI, III; Cintia de Lima GarciaI, II; Grayce Alencar AlbuquerqueI, II; Vitor Engrácia ValentiI; Thaiany Pedrozo Campos AntunesI; Hugo Macedo Jr.I; Luiz Carlos de AbreuI, IV
ILaboratório de EscritaCientífica da Faculdade de Medicina do ABC, Santo André -SP, Brazil
IIFaculdade de Juazeiro do Norte, Juazeiro do Norte - CE, Brazil
IIIUniversidade Federal doCariri, Barbalha-CE, Brazil
IVUniversidade de São Paulo, São Paulo - SP, Brazil
ABSTRACT
OVERVIEW: Inflammatory Breast Cancer (IBC) is a rare and very aggressive type of cancer that tends to develop at a younger age, compared with other subtypes of breast cancer. Because a distinct lump may not be noticeable, correct diagnosis takes longer and, therefore, successful treatment may hinder a patient's prognostics. This study aims to conduct a systematic review of research articles on IBC.
METHODS: This is a systematic review of studies in the PubMed database to April 2013, which fit the eligibility criterion of "Inflammatory Breast Neoplasms" (MeSH Terms), filtered by Languages (English OR Portuguese OR Spanish).
FINDINGS: Of the 119studies identified, 25 complied with the eligibility criterion for the disease, diagnostics, treatment and prognostics.
FINAL CONSIDERATIONS: Despite methodological differences, findings evidence that although IBC presents particular features (lower survival rate and worse prognostics than most types of breast cancer), very few studies examine its epidemiology and specific risk factors in depth and use any other therapeutic approaches than those commonly used for other breast cancer subtypes. Therefore, further investigation of the disease's aggressiveness is still necessary.
Key words: inflammatory breast neoplasms, medical oncology.
INTRODUCTION
Breast cancer is a public health problem, its incidence increases worldwide. While clinical care focuses on the individual health, the public health policies aimed at breast cancer focus the attention on women from various countries. The goal of these policies is to establish collective guidelines to increase health and quality of life through prevention, treatment of disease and health behavior promotion1.
Breast cancer brings number of impacts for women. The challenges and changes resulting from this disease involve many feelings, implying in physical and psychical adaptations2.
Inflammatory Breast Cancer (IBC) is a rare, although highly aggressive and lethal3 type of cancer. Rapid blood and lymphatic spread and breast tumor emboli are the main features ofIBC4. With an average survival rate of three years, IBC accounts for about 2.5% of all breast cancer types in the US. IBC tends to develop at a younger age than the more common form of breast cancer5. Distinct signs and symptoms develop quickly and include redness, thickening (edema/swelling) and ridging or orange-peel like textureof the skin - peaud'orange4 in French.
African-American women appear to be at higher risk of IBC than white women5,6.
The fact that it is a rare form of breast cancer and rarely causes a breast lump, it is harder to diagnose at early stage. Thus, successful prognosis (outlook) and treatment are harder. IBC may be diagnosed by an imaging test and by a breast biopsy of an invasive cancer7.
In the past two decades, a multi-therapy approach has increased the rates of clinical response through neoadjuvant chemotherapy, particularly usinganthracyclinesand taxanes-based combination, surgery, radiotherapy and hormone-based therapy5.
This study is a systematic review of scientific articles on IBC with reference to the diagnosis, treatment, determinants and prognostics of this type of cancer.
METHODS
Given that a systematic literature review is directed by a well-formulated question6, this study attempts to collate all empirical evidence to answer the following: "What has been researched about inflammatory breast neoplasms?"
A systematic search was conducted on the PubMed MEDLINE database, from its inception to April 2013, originally using the field "MeSH Terms" and Boolean operators (AND; OR) in "PubMed Advanced Search Builder" tool with the following search terms and field:
# 1 "Inflammatory Breast Neoplasms" (MeSH term);
# 2 Languages (English OR Portuguese OR Spanish [field]);
The following search was performed: #1 AND #2.
Articles were assessed as per their compliance with previously set eligibility criteria, as follows: a) manuscripts written in English, Portuguese or Spanish; b) articles about inflammatory breast neoplasms; c) original articles with online accessible full text; d) prospective or retrospective observational (analytical or descriptive, except case reports), experimental or quasi-experimental studies. Exclusion criteria were: a) other designs, such as case reports, series of cases, review of literature and commentaries; b) non-original studies, including editorials, reviews, prefaces, brief communications and letters to the editor.
Subsequently, every sample was thoroughly examined and data were entered into a matrix for multivariate analysis of author, publication year, description of the study sample and main findings. Studies that dealt with types other than inflammatory breast neoplasms, the focus of this study, were discarded. For each sample, data were extracted independently if co-authored and discrepancies were resolved by consensus. Finally, for heuristic reasons, articles were grouped for discussion in four major themes: profile epidemiology, treatment, factor of prognosis and survival.
RESULTS
The search strategies initially led to 119 references. After browsing the title and abstract of the retrieved articles for eligibility compliance with inclusion criteria, 94 articles were discarded and 25 articles were further retrieved and included in the final sample (Figure 1).
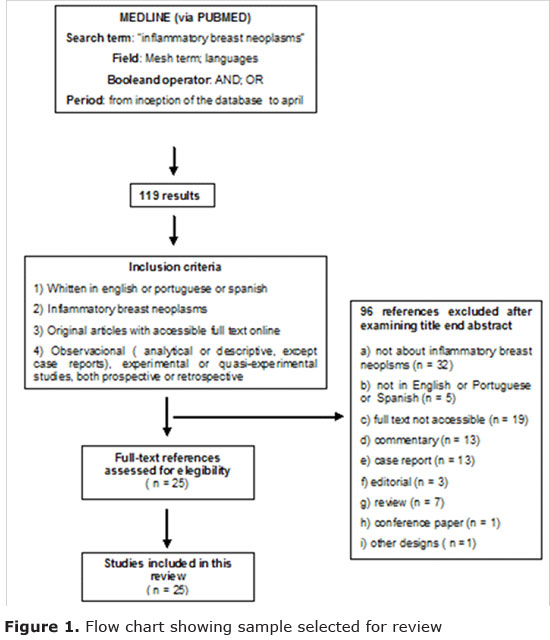
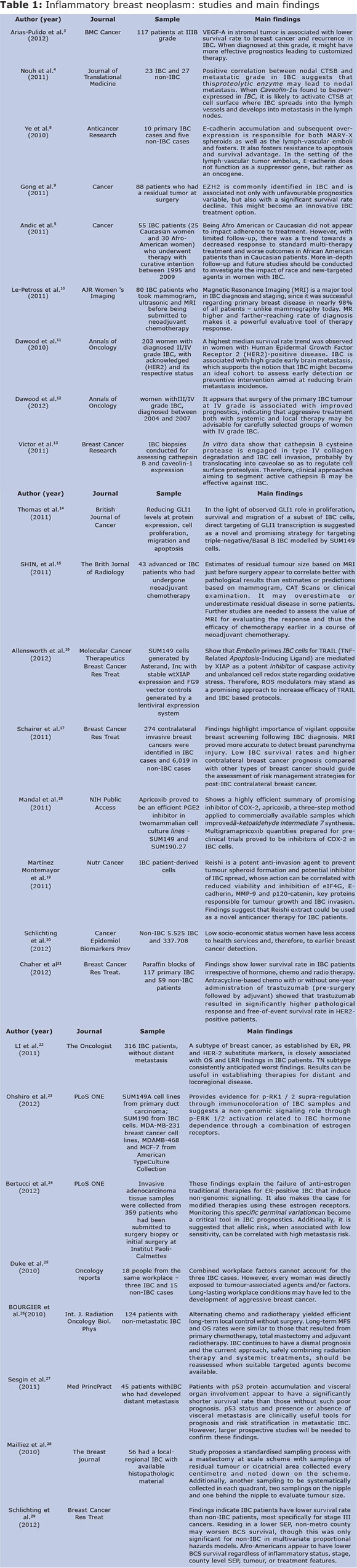
Table 1 provides an overview of the sample selection process which resulted in the 25 studies of the final sample. Such studies were grouped into the three previously set themes: diagnosis and treatment features4,10,12-19,21,23,26,28 (14 studies), determinants5,20,25 (three studies) and prognostics3,8,9,11,22,24,27,29 (eight studies).
Determining features
Only three of the study samples5,20,25 investi-gated determining features of the disease. For Andicet al.5, no difference was assessed between races at middle age, tumour size and receptor grade and status. However, a trend emerged for pathologic response, which was slightly higher in Caucasian than in Afro-American women (P = 0,23) - a generally higher survival rate (three years) in Caucasian than in Afro-American women (P = 0,09) and higher survival rate of distant metastasis (P = 0,19). Racial features did not seem to affect adherence to treatment.
Two studies 5, 20suggest that low socio-economic status is associated with higherIBC incidence, irrespective of a patient's age/race/ethnic group at diagnosis, and possibly associated with lower educational level and poor access to health services.
Duke et al.25investigated three specific cases of IBC in the workplace within a time-span of 10 months, suggesting that oral contraceptives, hormone replacement therapy, overweight and exposure topesticides and herbicides might have combined to result in such an unordinary number ofIBC cases in the workplace. However, they did not explain how combined workplace factors affected the three people.
Diagnostics and treatment
Several studies investigated diagnosis and treatment4,10,12-19,21,23,26,28, two of which10,15 show that MRI (Magnetic Resonance Imaging) is significantly more accuracy for diagnosing IBC. Le-Petross9 argues that MRI has a 98% accuracy rate in targeting IBC when compared with ultrasonic imaging (94%) and a mammogram (65%). MRI may also aid in assessing response to therapy. The samples contradict current practices to track breast cancer, of which the mammogram is the most commonly used. Vigilant opposite breast screening using MRI should be considered given the low IBC survival rates and higher contralateral breast cancer prognosis compared with other types of breast cancer17.
With reference to treatment options, primary grade IV IBC surgery is associated with better prognostics, suggesting that systemic or local therapy may be advisable for carefully selected objects13. Nevertheless, Bourgieret al.26 monitored 124 women from the time their non-metastasis IBS was diagnosed and suggest alternating chemo and radiotherapy as an effective method for long-term control without surgery. Chaher et al.21, however, observed worse survival conditions in IBC patients, irrespective of their being submitted to chemo, radio or hormone therapy.
Some studies suggest novel treatments using biological markers4,13. Victor et al.13 contend that cathepsin B cysteine protease is engaged in type IV collagen degradationand IBC cell invasion, probably by translocating into caveolae so as to regulate cell surface proteolysis. These in vitro findings are supported by significant cathepsin B and caveolin-1 co-expression in IBC cell samples. Theirs is one of the few studies which show that cathepsin B, associated with caveolin-1, plays a role in aggressive phenotype of IBC.
Two studies investigated plant active principles. Martínez-Montemayor et al19 examined the use of Reishi extract, a potent anti-invasion agent to prevent tumour spheroid formation and potential inhibitor of IBC spread and action can be correlated with reduced viability and inhibition of eIF4G, E-cadherin, MMP-9 and p120-catenin - key proteins responsible for tumour growth and IBC invasion. It is suggested that Reishi extract could be used as a novel anticancer therapy for IBC patients. Allensworth et al.16 described the role played by apoptosis inhibitor related to X when embelin, derived from a plant, is used in combination withTRAIL - a proapoptotic receptor agonist - to catalyse the death of this receptor. Cell viability was lowered and TRAIL proved to be a novice approach to higher IBC protocol.
GLI1 is a protein-coding gene that is able to regulate cell proliferation, survival and differentiation. Thus, Thomas et al.14 suggested direct targeting of GLI1 transcription as a promising strategic therapy for IBC patients.
Ohshiro et al.23 explored non-genomic signalling of several estrogen and anti-estrogen agents in IBC SUM149 and SUM190 cell lines and identified a variant estrogen receptor (EEI), ERa36, in SUM149 and SUM190 cells and a substantial increase in cell migration and invasion of SUM149 cells when these ligands were used. Such findings suggest a non-genomic signalling role through p-ERK1/2 activation related to IBC hormone dependence through a combination of estrogen receptors, and explain the failure of anti-estrogen traditional therapies for ER-positive IBC.
Mailliezet al.28compared the Complete Pathologic Response(CPR) in 56 non-metastasis IBC patients and assessed a possible correlation betweenCPR and global survival. Initial biopsies and mastectomy at scale scheme with samplings of residual tumour or cicatricial area were revised by the same pathologist. A 75% clinical response was found, but no correlation between clinical and pathological response. Neither response was predictive of global relapse-free survival.
Prognostics
Prognostics-oriented studies explore mainly biological factors that are good prognostics markers3,8,9,11,22,24,27,29.
Seszinet al.27assessed prognostics markers of IBC by examining resection samples of 45 IBC patients who had developed distant metastasis. Patients with p53 protein accumulation and visceral organ involvement appear to have a significantly shorter survival rate than those without such poor prognosis.
EZH2, Enhancer of homolog zester2, is a Polycomb protein that regulates cell cycle progression and which is associated with many malign tumours, including breast cancer. It is associated not only with unfavourable prognostics variable but also with a significant survival rate decline9. Therefore, it might become an innovative IBC treatment option.
Expression of VEGF-A, Vascular endothelial growth factor A, in stromal tumour, is associated with lower survival rate to breast cancer and recurrence in IBC. When diagnosed at this grade, it might have more effective prognostics leading to customised therapy.
In the research of Para Ye et al.8, E-cadherin accumulation and subsequent over-expression is responsible for both MARY-X spheroids and the lymph-vascular emboli and fosters. It also fosters resistance to apoptosis and survival advantage. In the setting of the lymph-vascular tumor embolus, E-cadherin does not function as a suppressor gene, but rather as an oncogene.
Two studies assessed hormone receptors11,24. Dawoodet al.11 studied 203 women with diagnosed II/IV grade IBC, with acknowledged (HER2) and its respective status and cumulative incidence or brain metastases. A highest median survival rate trend was observed in women with Human Epidermal Growth Factor Receptor 2 (HER2)-positive disease. IBC is associated with high grade early brain metastasis, which supports the notion that IBC might become an ideal cohort to assess early detection or preventive intervention aimed at reducing brain metastasis incidence.
Between 1989 and 2008, Li et al.22analysed the records of 316 patients without distant metastasis, most of whom were submitted to neoadjuvant chemotherapy, mastectomy and post-mastectomy radiotherapy. These objects were grouped according to the status of the estrogen receptor, progesterone and human epidermal growth factor receptor -2. They found that the disease triple-negative is associated with lower global and locoregional relapse survival, thus showing the need to develop therapies for distant and locoregional disease.
Bertucciet al.24 suggested, initially described as a low susceptibility locus and penetrance forcolorectal and prostate cancer, seems to be associated with high IBC metastasis risk. New prognostic tools, currently based on histoclinic and somatic mutation factors, may benefit from monitoring the specific IBC patient germinative variations. As this was the first study to present such findings, the authors suggested further investigation to verify this association.
Although IBC risk factors remain unknown, some studies have shown diverse features for IBC and non-IBC patients. Few studies have examined the rarest pathologies of this type of cancer and are thus inaccurate in assessing consistently inherent risk factors.
Therefore, it is paramount that early IBC diagnosis is implemented, especially for low socioeconomic groups, who are likely to have less access to healthcare and early detection programmes, as early diagnosis is viewed as possibly having a direct positive effect on prognostics.
It should be noted that the mammogram remains the most commonly used method to detect breast cancer. However, evidence shows that MRI is a more accurate diagnostic tool as IBC clinical features are taken into account.
Few studies have examined IBC molecular biology as it is rare. Nevertheless, as we consider this disease's high aggressiveness, low survival rate and resistance to treatment, further investigation must be pursued. The sample of this study has not identified different and effective types of treatment, but found new proposed ways to enhance IBC treatment using novice biological markers, as discussed above.
REFERENCES
1. Hani K. Atrash 1, Richard Carpentier The evolving role of public health in the delivery of health care. Journal of Human Growth and Development, 2012; 22 (3): 396-99. [ Links ]
2. Ariana Machado Toriy, EditKrawulski, Jaqueline de Souza Viera Brasiliense, Clarissa Medeiros da Luz, Fabiana FlowersSperandio. Perceptions, feelings and physical and emotional experiences of woman after breast cancer. Journal of Human Growth and Development, 2013; 23 (3): 303-08. [ Links ]
3. Arias-Pulidoet al. Tumor stromal vascular endothelial growth factorA is predictive of poor outcome in inflammatory breast cancer BMC Cancer 2012, 12:298. [ Links ]
4. Nouh, M. A. et al. Cathepsin B: a potential prognostic marker for inflammatory breast cancer. Journal of translational medicine9, 1, doi:10.1186/1479-5876-9-1 (2011). [ Links ]
5. Andic, F. et al. Treatment adherence and outcome in women with inflammatory breast cancer: does race matter? Cancer117, 5485-5492, doi:10.1002/cncr.26187 (2011). [ Links ]
6. Hance KW, A. W., Devesa SS, et al. Trends in, the, i. b. c. i. a. s., surveillance, e., and end results program at the, 2005;97:966-, N. C. I. J. N. C. I. & 975. [ Links ]
7. Moher D, L. A., Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097. [ Links ]
8. Ye, Y., et al. (2010). E-cadherin accumulation within the lymphovascular embolus of inflammatory breast cancer is due to altered trafficking.Anticancer Research, 30(10), 3903-10. [ Links ]
9. Gong, Y. et al. Polycomb group protein EZH2 is frequently expressed in inflammatory breast cancer and is predictive of worse clinical outcome. Cancer117, 5476-5484, doi:10.1002/cncr.26179 (2011). [ Links ]
10. Le-Petross, H. T. et al. MRI features of inflammatory breast cancer. AJR. American journal of roentgenology197, W769-776, doi:10.2214/AJR.10.6157 (2011). [ Links ]
11. Dawood, S. et al. Incidence of and survival following brain metastases among women with inflammatory breast cancer. Annals of oncology: official journal of the European Society for Medical Oncology / ESMO21, 2348-2355, doi:10.1093/annonc/mdq239 (2010). [ Links ]
12. Dawood, S. et al. Identifying factors that impact survival among women with inflammatory breast cancer. Annals of oncology : official journal of the European Society for Medical Oncology / ESMO23, 870-875, doi:10.1093/annonc/mdr319 (2012). [ Links ]
13. Victor, B. C., Anbalagan, A., Mohamed, M. M., Sloane, B. F. & Cavallo-Medved, D. Inhibition of cathepsin B activity attenuates extracellular matrix degradation and inflammatory breast cancer invasion. Breast cancer research : BCR13, R115, doi:10.1186/bcr3058 (2011). [ Links ]
14. Thomas, Z. I. et al. Targeting GLI1 expression in human inflammatory breast cancer cells enhances apoptosis and attenuates migration. British journal of cancer104, 1575-1586, doi:10.1038/bjc.2011.133 (2011). [ Links ]
15. Shin, H. J. et al. Comparison of mammography, sonography, MRI and clinical examination in patients with locally advanced or inflammatory breast cancer who underwent neoadjuvant chemotherapy. The British journal of radiology84, 612-620, doi:10.1259/bjr/74430952 (2011). [ Links ]
16. Allensworth, J. L., Aird, K. M., Aldrich, A. J., Batinic-Haberle, I. & Devi, G. R. XIAP inhibition and generation of reactive oxygen species enhances TRAIL sensitivity in inflammatory breast cancer cells. Molecular cancer therapeutics11, 1518-1527, doi:10.1158/1535-7163.MCT-11-0787 (2012). [ Links ]
17. Schairer, C., Brown, L. M. & Mai, P. L. Inflammatory breast cancer: high risk of contralateral breast cancer compared to comparably staged non-inflammatory breast cancer. Breast cancer research and treatment129, 117-124, doi:10.1007/s10549-010-1324-y (2011). [ Links ]
18. Mandal, P. K., Freiter, E. M., Bagsby, A. L., Robertson, F. M. & McMurray, J. S. Efficient synthesis of apricoxib, CS-706, a selective cyclooxygenase-2 inhibitor, and evaluation of inhibition of prostaglandin E2 production in inflammatory breast cancer cells. Bioorganic & medicinal chemistry letters21, 6071-6073, doi:10.1016/j.bmcl.2011.08.050 (2011). [ Links ]
19. Martinez-Montemayor, M. M., Acevedo, R. R., Otero-Franqui, E., Cubano, L. A. & Dharmawardhane, S. F. Ganoderma lucidum (Reishi) inhibits cancer cell growth and expression of key molecules in inflammatory breast cancer. Nutrition and cancer63, 1085-1094, doi: 10.1080/01635581.2011.601845 (2011). [ Links ]
20. Schlichting JA, et al. Association of inflammatory and noninflammatory breast cancer with socioeconomic characteristics in the Surveillance, Epidemiology, and End Results database, 2000-2007.Cancer Epidemiol Biomarkers Prev 21, 155.doi: 10.1158/1055-9965 2012 [ Links ]
21. Chaher, N. et al. Molecular and epidemiological characteristics of inflammatory breast cancer in Algerian patients. Breast cancer research and treatment131, 437-444, doi:10.1007/s10549-011-1422-5 (2012). [ Links ]
22. Li, J. et al. Triple-negative subtype predicts poor overall survival and high locoregional relapse in inflammatory breast cancer. The oncologist16, 1675-1683, doi:10.1634/theoncologist.2011-0196 (2011). [ Links ]
23. Ohshiro K, Schwartz AM, Levine PH, Kumar R .Alternate Estrogen Receptors Promote Invasion of Inflammatory Breast Cancer Cells via Non-Genomic Signaling. PLoS ONE 7(1): e30725. doi:10.1371/journal.pone.0030725 (2012). [ Links ]
24. Bertucci, F. 8q24 cancer risk allele associated with major metastatic risk in inflammatory breast cancer. PLoS One 7(5),doi:10.1371/journal.pone.0037943.t001 (2012) [ Links ]
25. Duke T J, Nasreen C. Jahed, C C. Veneroso, R R, Owen J, Daniel H. et al. A cluster of inflammatory breast cancer (IBC) in an office setting: Additional evidence of the importance of environmental factors in IBC etiology. Oncology reports24, doi:10.3892/or_00000983 (2010). [ Links ]
26. Bourgier C et al. Exclusive Alternating Chemotherapy and Radiotherapy in Nonmetastatic Inflammatory Breast Cancer: 20 Years of Follow-Up. International Journal of Radiation Oncology, Biology, Physics 82(2) 690-695, (2012). [ Links ]
27. Sezgin C et al. p53 protein accumulation and presence of visceral metastasis are independent prognostic factors for survival in patients with metastatic inflammatory breast carcinoma.Med PrincPract 20(2):159-64. doi: 10.1159/000319916. (2011). [ Links ]
28. Mailliez et al. Is there a reliable method to assess the complete pathologic response on the tumor after eo-adjuvant chemotherapy in inflammatory breast cancer toward recommendations for the pathologic process? Experience in 56 patients treated in a single institution. Breast J 16(5):464-71. doi: 10.1111/j.1524-4741.2010.00957 (2010). [ Links ]
29. Schlichting JA, et al. Inflammatory and non-inflammatory breast cancer survival by socioeconomic position in the Surveillance, Epidemiology, and End Results database, 1990-2008.BreastCancer Res Treat 134(3), 1257-68(2012). 29 [ Links ]
Manuscript submitted Sep 10 2014
Accepted for publication Nov 21 2014
