










Serviços Personalizados
artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282
Rev. bras. crescimento desenvolv. hum. vol.25 no.2 São Paulo 2015
http://dx.doi.org/10.7322/JHGD.103022
ORIGINAL RESEARCH
Laboratory parameters of cerebrospinal fluid in individuals with enterovirus meningitis
Flavio Geraldes AlvesI, II; Rubens WajnsztejnI, II; Camila Almeida Exposto AlvesI, II; Tassiane Cristina MoraisI; Mahmi FujimoriI; Fernando AdamiI; Cicero Macedo CruzI, III; Luiz Carlos de AbreuI
ILaboratório de Delineamento de Estudos e Escrita Científica. Departamento de Ciências Básicas. Faculdade de Medicina do ABC
IIDisciplina de Neurologia da Infância e da Adolescência. Faculdade de Medicina do ABC
IIIDocente do Departamento de pediatria da Universidade Federal do Cariri- UFCA. Barbalha, CE, Brasil
ABSTRACT
INTRODUCTION: Meningitis is the leading infectious syndrome that affects the central nervous system, and most cases are caused by viral infections, mainly enterovirus. The clinical diagnosis for meningitis etiology still presents major challenges. The analysis of polymerase chain reaction (PCR), white blood cells, red blood cells, glucose, protein, and lactate in the cerebrospinal fluid (CSF) provides the first clues to the diagnosis. However, the reference values of some parameters can suffer changes
OBJECTIVE: Analyze the laboratory parameters of CSF in patients with enterovirus meningitis, and then, theirrelationship by age group
METHODS: A descriptive study was conducted based on data from a CSF reference service, located in São Paulo, Brazil, on 202 individuals who had enterovirus meningitis. Data was analysed by the Shapiro-Wilk and Kruskal-Wallis tests (CI = 95%, p < 0.05) and represented by the median and percentile 25 and 75, respectively
RESULTS: The cytological and biochemical parameters of the CSF shows us that proteins had median concentrations of 33.0mg/ dL, glucose of 57.0mg/dl, lactate of 19.0mg/dL and the leukocyte of 119.0 cells/mm3, with a predominance of lymphocytes (42%). It was found that age can cause cytological and biochemical changes in the parameters of CSF. Children younger than 2 years had a range percentage of neutrophils and monocytes different then children aged ≤ 2 and < 6 years, and aged ≤ 6 and < 10 years. The protein concentration range in CSF as well as glucose track can also change according to age
CONCLUSION: The parameters of the CSF in patients with enteroviral meningitis showed similar median concentrations to those found in the literature. Age may lead to changes in cytological and biochemical parameters of CSF. CSF protein and glucose concentrations also change according to age
Key words: enterovirus, cerebrospinal fluid, viral meningitis
INTRODUCTION
Meningitis is the term used to describe the inflammation of the brain meninges, and it is the major infectious syndrome in the central nervous system. Based on its causes, it can be classified into bacterial meningitis and aseptic meningitis1,2.
Aseptic meningitis is the inflammation of the meninges, and does not have a bacterial infection as the cause3-4. Aseptic meningitis may or may not have a viral infection as the most common cause of the disease3,5,13.
Viral meningitis can occur in people of all ages, but it is more common in children5,6. It is a worldwide disease in sporadic and epidemic forms. It often has a benign clinical course, as most viral meningitis are caused by enterovirus. These infections can present high morbidity and low mortality rates. They rarely lead to serious complications, which are observed mainly in immuno-compromised individuals1,3,7.
Enteroviruses are responsible for approximately 90% of cases of aseptic meningitis. They are single-stranded RNA viruses belonging to the Picornaviridae family. There are more than 100 serotypes, including poliovirus, A and B coxsackievirus, and echovirus3,5,8,9,10,11.
The clinical manifestations vary depending on the serotype; however, in most cases the clinical results are not sufficient to allow a specific etiologic diagnosis. The infections may be asymptomatic or present nonspecific symptoms, such as headache, fever, myalgia, malaise, chills, sore throat, abdominal pain, nausea, vomiting, photophobia, neck stiffness, and drowsiness3,5.
It is noteworthy that the initial clinical presentations of viral meningitis and bacterial meningitis are often similar. Therefore, distinguishing the etiologies quickly results in great benefits2 and avoids the inappropriate use of medications2,20.
The main method used for differentiation is based on clinical findings, but in clinical suspicion of meningitis, cerebrospinal fluid (CSF) analysis is mandatory. The results of CSF analysis form the basis for the objectives of the therapy and allows the request of other necessary examinations, according to the diagnosis and identification of the etiologic agent1,12,13.
Given the considerable genetic variability of enterovirus, the detection of RNA viruses in clinical samples has proven usefulness to streamline the diagnosis and improve assistance to patients, particularly newborns9. The Gram stain test, biochemical tests (such as protein, glucose, and lactate), and differential counting of leukocytes in the CSF are important for establishing an etiological cause of meningitis7,14.
In the CSF viral infection analysis, there is generally a predominance of lymphocytes and absence of bacterial agents1. In aseptic meningitis, mononuclear cells are predominant, while in bacterial meningitis, polymorphonuclear cells are predominant. An important fact is that the predominant cell population in aseptic meningitis can be changed within 24 hours, and this can lead to the uncertainty of diagnosis and of the treatment programme13.
Due to doubts about the etiology of meningitis, medical management usually includes hospital observation, which increases the number of hospitalisations2. Thus, early detection of enterovirus can result in benefits to the health system. In addition to reducing the occupation of hospital beds, the risk of contamination by contact and inappropriate use of antibiotics can also be avoided. Unfortunately, it is still a major challenge to differentiate types of meningitis only based on clinical characteristics and initial parameters of CSF2,7,9,15.
Studies addressing this topic are essential to establishing etiological identification parameters, thus contributing to an accurate diagnosis. The generation of a set of reference values for CSF parameters, especially in children, is an important area of discussion among health professionals16.
The objective of this study was to analyze the laboratory parameters of CSF in patients with enterovirus meningitis, and then, their relationship by age group.
METHODS
This is a descriptive study, based on data of a reference service of CSF analysis, located in São Paulo, Brazil. Data were collected in August 2014, from the database inserted in Tasy Management System - Philips Healthcare®, during the period from 1 August 1st of 2011 to July 31th of 2012.
The study included examinations of individuals submitted to CSF puncture who were diagnosed with enterovirus meningitis. The study included only those individuals whose results were 100% negative in Gram stain tests and culture, along with the confirmation of viral infection by positivity on enterovirus panel by polymerase chain reaction (PCR) in real time, totaling 202 individuals.
The variables analysed were age, bacterioscopy, culture, enterovirus panel, global cytology and differential, protein, glucose, and lactate. Bacterioscopy uses the Gram stain method. The culture is carried out by identifying by manual techniques under specific conditions. The enterovirus panel is analysed by real time PCR. The global cytology is performed using Fuchs-Rosenthal chamber scoring; cytology differential microscopy using Leischmann staining method; protein, glucose and lactate are analysed by an enzymatic method.
A Shapiro-Wilk test (p <0.05) was performed, and we decided to present the data based on median values, percentile 25 and 75. The biochemical and cytological variables were compared by age in years (<2 years; > 2 and <6 years; ≥ 6 and < 10 years; ≥ 10 and < 20 years; ≥ 20 years), using the Kruskal-Wallis test and analysis by confidence interval (95% CI). The statistical software used was Stata® version 11.0.
RESULTS
The average age of the individuals was 7.7 years, and the median age was 5 years. The youngest verified individual was 10 months, and the oldest was 42 years. Among those surveyed, 10.4% (n = 21) were individuals aged < 2 years, 40.1% (n = 81) aged ≤ 2 and < 6 years, 26.7% (n = 54) aged ≤ 6 and < 10 years, 15.4% (n = 31) aged ≥ 10 and < 20 years, and 7.4% (n = 15) aged over 20 years.
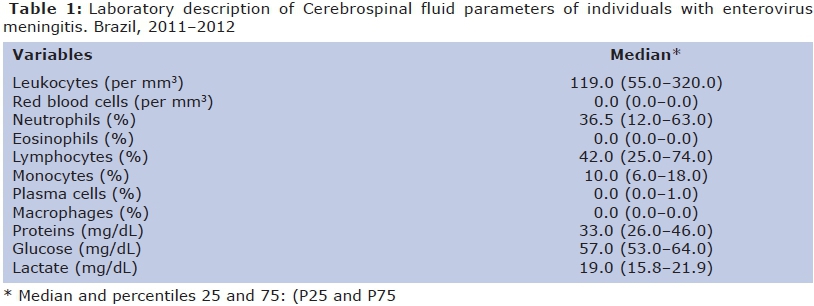
Laboratory CSF parameters of patients with enterovirus meningitis are described in Table 1, presented based on median values and percentiles 25 and 75, respectively. The following median values were observed: protein 33.0 mg/dL, glucose 57.0 mg/dL, lactate 19.0 mg/dL, and leukocyte 119.0 cells/mm3. Among these, lymphocytes were prevalent (42%), followed by neutrophils (36.5%). Eosinophils, plasma cells, and macrophages obtained median values of zero. There were no red blood cells.
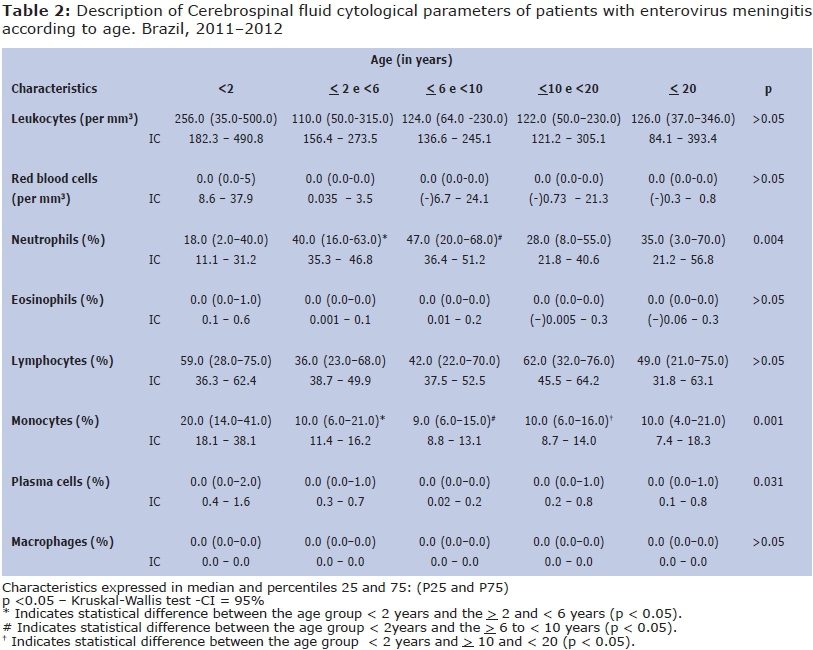
The cytological parameters according to age group are described in Table 2. A statistically significant difference was observed in neutrophil count in those aged < 2 years in relation to those aged ≥ 2 and < 6 years (p <0.05) and ≤ 6 and < 10 years (p < 0.05).
The values of monocytes also showed variations in their concentration according to age group. This parameter shows the difference among the age group < 2 years and the following age groups: ≤ 2 and < 6 years (p < 0.05), > 6 and < 10 years (p < 0.05), and ≤ 10 and < 20 years (p < 0.05).
There were also significant differences in the analysis of the confidence intervals in relation to the percentage of plasma cells among individuals aged ≤ 6 and < 10 years (p < 0.05) and the groups aged < 2 years and ≤ 10 and < 20 years ( p < 0.05). This result, however, might not be used as a parameter, as the percentage of the general data of plasma cells in the researched subjects is approximately 0%.
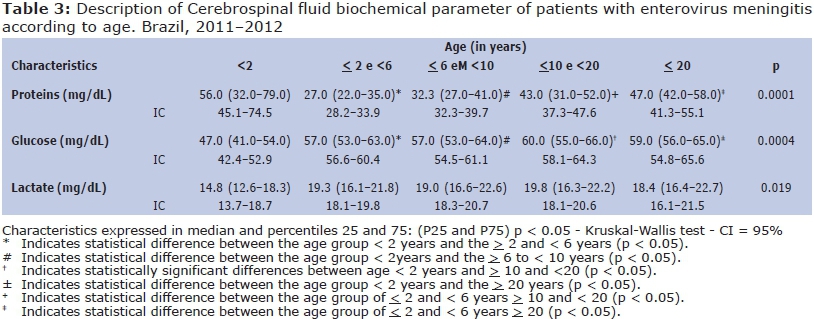
The concentrations of biochemical parameters also presented statistically significant variations according to age, as shown in Table 3.
Protein concentrations fluctuated in the group aged < 2 years when compared to the groups aged of ≥ 2 and < 6 years (p < 0.05) and ≥ 6 and < 10 years (p < 0.05). The groups aged ≥ 2 and < 6 years also showed significant differences when compared with individuals in the group aged ≥ 10 and < 20 years (p < 0.05) and the group aged with ≥ 20 years (p < 0.05).
Glucose concentrations in CSF also varied according to age, significantly in individuals aged < 2 years, in relation to all other categorised age groups (p < 0.05).
In lactate analysis, there was statistical significance (p = 0.019), but the confidence intervals among the age groups were quite homogeneous.
DISCUSSION
Viral diseases that affect the central nervous system represent a significant burden to human health throughout the world. The complexity of these diseases is influenced by the great variety of existing viruses and their variable forms of infection that affect the central nervous system4. Because of this, it is so important to have precision in etiologic diagnosis, especially when it comes to individuals in special age groups. In these cases, especially in newborns, viral meningitis may be high-risk diseases, as far as bacterial meningitis16.
It is a challenge to distinguish serious and benign bacterial and viral infections, especially in pediatric subjects17. The analysis of some of the CSF laboratory parameters (PCR, leukocytes, erythrocytes, glucose, and proteins) is often the first clue to the diagnosis16,18.
The number of CSF leukocytes may vary with the infectious agent. In healthy individuals, the CSF may present up to 4 leucocytes/mm3, whereas this number can reach up to 1000 leukocytes/mm3 with viral infections, or even exceed 1000 leukocytes/ mm3 with bacterial infections1.
This study found a median concentration of 119.0 leucocytes/mm3, with a predominance of lymphocytes (42%), followed by neutrophils (36.5%). A study of enterovirus meningitis found 149 leucocytes/mm3 as an average concentra-tion6. This difference may be related to the fact that the study subjects were all children, while in our study both children and adults were evaluated. An approximate value was also found in a study of aseptic meningitis in individuals positive for enterovirus, with a concentration of 159 leukocytes/mm3 and 40% neutrophils8. The predominant type of leukocyte is important to know in order to assist in the diagnosis. There is a predominance of neutrophils in bacterial meningitis, while in viral meningitis lymphocytes are usually predominant1,13.
In this study, red blood cells were not observed in the CSF. In a study of patients with meningitis, a concentration of 15 erythrocytes/mm3 was observed in patients with aseptic meningites, and a higher value (53 erythrocytes/mm3) in patients with bacterial meningitis13.
The values of CSF biochemical parameters are also key. Noteworthy are mainly protein, glucose, and lactate. In this study, there was a median dosage concentration of 33.0 mg/dL for proteins, 57.0 mg/dL for glucose and 19.0 mg/dL for lactate.
A protein concentration of 56.9 mg/dL and a glucose concentration of 64.5 mg/dL were found in a study on enterovirus detection in pediatric patients with aseptic meningitis6. In a study of viral meningitis in Korea, it was found that individuals with enterovirus infections showed a protein concentration with a median value of 39 mg/dL and glucose of 59 mg/dL19, which is similar to this study findings.
Glucose and protein concentrations also serve as a parameter to the etiology differential. In a CSF study in aseptic and bacterial meningitis, it was found that the glucose concentrations are low and the protein concentration rises in bacterial meningitis13.
The CSF lactate levels are among the most useful tests to distinguish bacterial and viral meningitis1. In this study, a lactate concentration of 19.0 mg/dL was observed. The increase in CSF lactate is a potential marker for bacterial meningitis, and can provide early diagnosis information. It is produced by bacterial anaerobic metabolism and is unaffected by blood lactate concentration. The lactate level is elevated in cases of bacterial meningitis, and a concentration of 35 mg/dL may be a cutoff value to distinguish aseptic and bacterial meningitis14.
It was found that age is a factor that can lead to changes in concentrations of some of the CSF parameters for leukocyte, glucose, and protein concentrations.
For leukocyte differential, it was found that the age group < 2 years had a range of less neutrophil counts (CI = 11.1-31.2) compared to the groups aged ≥ 2 and < 6 years (p < 0.05) and ≥ 6 and < 10 years (p <0.05). Monocytes also fluctuated in their concentration according to age; higher scores were observed at age < 2 years (CI = 18.1-38.1) when compared to the ages > 2 and < 6 years (p < 0.05), ≥ 6 and < 10 years (p < 0.05) and ≥ 10 and < 20 years.
The CSF protein concentration was lower in individuals aged < 2 years when compared to those aged ≥ 2 and < 6 years (p < 0.05), and > 6 and < 10 years (p < 0.05). The group aged ≥ 2 and < 6 years had a lower concentration range than individuals aged ≥ 10 and < 20 years (p < 0.05) and with ≥ 20 years (p < 0.05).
For glucose, it was observed that there was difference between < 2 years age group in relation to other age groups. Its concentration was lower in this age group (p < 0.05).
In children, the establishment of reference values in laboratory tests in the literature has been a field of discussion among health professionals. It is known that the values observed for CSF cell numbers, glucose, and protein in individuals less than 60 days old tend to be different from those observed in older children and adults16.
In studies of children with aseptic meningitis, the enterovirus positive group showed an increase in the concentration of leukocytes according to age. Children under 2 years of age had values of 38 leukocytes/mm3, while children aged 6 to 10 years showed a concentration of 156.6 leukocytes/ mm.3 No leukocyte differential percentages were reported. There was also an inverse relationship between the concentration of protein and age6.
In a study on CSF features in febrile children in the emergency department, it was observed that blood cells and CSF protein concentration decrease with increasing age. No clear relationship with increasing age was observed for glucose16.
Importantly, children under 6 years of age were the ones that showed the most changes in some parameters when compared to other age groups in these studies6,16, which may increase the difficulty in diagnosing this group. The establishment of an early etiological diagnosis, especially in infants, is essential for targeting interventions that save lives17. Therefore, studies that seek to show changes in the CSF settings according to the type of infection and age are necessary for the development of health strategies, especially in pediatrics.
This study has some limitations. It is a local study, referring to the city of São Paulo. Its retrospective design allows us only to analyze the CSF exams in subjects with PCR positive for Enterovirus. There is no data of the patient's clinical course or of the onset date of their symptoms, only the data of the CSF parameters during the hospital observation period. Despite, we believe that the results are relevant and clinicallyimportant , especially in this sample , compared to the published studies in the literature.
The primary health care should always be considered in the diagnosis and treatment of diseases
. Basic care and public health measures such as breastfeeding , hands washing and up to date vaccines can prevent the onset of diseases such as meningitis, decreasing the morbidity and mortality of these diseases21.
CONCLUSION
Age may lead to changes in cytological and biochemical parameters of CSF. The < 2 years age group presents an different range of percentage of neutrophils and monocytes of children aged > 2 and < 6 years and ≥ 6 and < 10 years. CSF protein and glucose concentrations also change according to age. These data show the importance of studies that can clarify the changes by age in CSF constituents, and the usefulness in creating reference parameters for enterovirus meningitis.
REFERENCES:
1. Almeida SM, Nogueira MB, Raboni SM, Vidal LR. Laboratorial diagnosis of lymphocytic meningitis. Braz J Infect Dis. 2007;11(5):489-95. DOI: http://dx.doi.org/10.1590/S1413-86702007000500010 [ Links ]
2. Mohseni MM, Wilde JA. Viral meningitis: Which patients can be discharged from the emergency department J Emerg Med. 2012; 43(6): 1181-7. DOI: http://dx.doi.org/10.1016/j.jemermed.2012.03.021 [ Links ]
3. Kumar R. Aseptic Meningitis: Diagnosis and Management. Indian J Pediatr. 2005;72(1):57-63. [ Links ]
4. Swanson PA, McGavern DB. Viral diseases of the central nervous system. Curr Opin Virol. 2015; 11: 44-54. DOI: http://dx.doi.org/10.1016/j.coviro.2014.12.009 [ Links ]
5. Rice P. Viral meningitis and encephalitis. Medicine. 2013; 41(12): 678-82. DOI: http://dx.doi.org/10.1016/j.mpmed.2013.09.005 [ Links ]
6. Shaker OG, Abdelhamid N. Detection of enteroviruses in pediatric patients with aseptic meningitis. Clin Neurol Neurosurg. 2015; 129: 67-71. DOI: http://dx.doi.org/10.1016/j.clineuro.2014.12.004 [ Links ]
7. Chadwick DR. Viral meningitis. Br Med Bull. 2006;75-76:1-14. DOI: http://dx.doi.org/10.1093/bmb/ldh057 [ Links ]
8. Giulieri SG, Chapuis-Taillard C, Manuel O, Hugli O, Pinget C, Wasserfallen J-B, et al. Rapid detection of enterovirus in cerebrospinal fluid by a fully-automated PCR assay is associated with improved management of aseptic meningitis in adult patients. J Clin Virol. 2015;62:58-62. DOI: http://dx.doi.org/10.1016/j.jcv.2014.11.0 01 [ Links ]
9. Hong J, Kim A, Hwang S, Cheon DS, Kim JH, Lee JW, et al. Comparison of the genexpert enterovirus assay (GXEA) with real-time one step RT-PCR for the detection of enteroviral RNA in the cerebrospinal fluid of patients with meningitis. Virol J. 2015;12:27. DOI: http://dx.doi.org/10.1186/s12985-015-0258-8 [ Links ]
10. Kumar A, Shukla D, Kumar R, Idris MZ, Misra UK, Dhole TN. Molecular epidemiological study of enteroviruses associated with encephalitis in children from India. J Clin Microbiol. 2012; 50(11):3509-12. DOI: http://dx.doi.org/10.1128/JCM.01483-12 [ Links ]
11. Tapparel C, Siegrist F, Petty TJ, Kaiser L. Picornavirus and enterovirus diversity with associated human diseases. Infect Genet Evol. 2013; 14:282-93. DOI: http://dx.doi.org/10.1016/j.meegid.2012.10.016 [ Links ]
12. Bremell D, Mattsson N, Wallin F, Henriksson J, Wall M, Blennow K, et al. Automated cerebrospinal fluid cell count-new reference ranges and evaluation of its clinical use in central nervous system infections. Clin Biochem. 2014;47(1-2):25-30. DOI: http://dx.doi.org/10.1016/j.clinbiochem.2013.11.010 [ Links ]
13. Negrini B, Kelleher KJ, Wald ER. Cerebrospinal fluid findings in aseptic versus bacterial meningitis. Pediatrics. 2000;105(2):316-9. DOI: http://dx.doi.org/10.1542/peds.105.2.316 [ Links ]
14. Sakushima K, Hayashino Y, Kawaguchi T, Jackson JL, Fukuhara S. Diagnostic accuracy of cerebrospinal fluid lactate for differentiating bacterial meningitis from aseptic meningitis: a meta-analysis. J Infect. 2011;62(4):255-62. DOI: http://dx.doi.org/10.1016/j.jinf.2011.02.010 [ Links ]
15. Chadwick DR, Lever AM. The impact of new diagnostic methodologies in the management of meningitis in adults at a teaching hospital. QJM. 2002; 95(1):663-70. DOI: http://dx.doi.org/10.1093/qjmed/95.10.663 [ Links ]
16. Chadwick SL, Wilson JW, Levin JE, Martin JM. Cerebrospinal fluid characteristics of infants who present to the emergency department with fever: establishing normal values by week ofage. Pediatr Infect Dis J. 2011; 30(4):e63-7. DOI: http://dx.doi.org/10.1097/INF.0b013e31820ad2ba [ Links ]
17. Messacar K, Breazeale G, Wei Q, Robinson CC, Dominguez SR. Epidemiology and clinical characteristics of infants with Human Parechovirus or Human Herpes Virus-6 detected in cerebrospinal fluid tested for Enterovirus or Herpes Simplex Virus. J Med Virol. 2015; 87(5): 829-35. DOI: http://dx.doi.org/10.1002/jmv.24119 [ Links ]
18. White K, Ostrowski K, Maloney S, Norton R. The utility of cerebrospinal fluid parameters in the early microbiological assessment of meningitis. Diagn Microbiol Infect Dis. 2012;73(1):27-30. DOI: http://dx.doi.org/10.1016/j.diagmicrobio.2012.02.010 [ Links ]
19. Seo J, Yeom JS, Youn H, Han T, Chung J. Prevalence of human parechovirus and enterovirus in cerebrospinal fluid samples in children in Jinju, Korea. Korean J Pediatr. 2015; 58(3):102-7. DOI: http://dx.doi.org/10.3345/kjp.2015.58.3.102 [ Links ]
20. Zeleke A, Chanie T, Woldie, M. Medication prescribing errors and associated factors at the pediatric wards of Dessie Referral Hospital, Northeast Ethiopia. Inter Arc Med. 2014;7:18. DOI: http://dx.doi.org/10.1186/1755-7682-7-18 [ Links ]
21. Atrash H, Carpentier R. The evolving role of public health in the delivery of health care. J Hum Growth Dev. 2012; 22(3): 396-399. [ Links ]
Manuscript submitted: jun 12 2015
Accepted for publication: aug 10 2015
Corresponding author: fg.flavio@gmail.com


{kind=link}
{kind=link}
{kind=link}