










Services on Demand
article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Share

 Permalink
PermalinkJournal of Human Growth and Development
Print version ISSN 0104-1282On-line version ISSN 2175-3598
J. Hum. Growth Dev. vol.25 no.3 São Paulo 2015
http://dx.doi.org/10.7322/jhgd.106002
ORIGINAL RESEARCH
Knowledge of health sciences undergraduate students in objective tests on basic life support
Luis Fernando Barbosa TavaresI; Italla Maria Pinheiro BezerraI; Fernando Rocha OliveiraI; Luiz Vinícius de Alcantara SousaI; Rodrigo Daminello RaimundoI; Ednan Cardoso de SousaI; Fernando AdamiI; Luiz Carlos de AbreuI, II
ILaboratório de Delineamento de Estudos e Escrita Cientifica - Faculdade de Medicina do ABC, Santo André, São Paulo - Brasil
IIHarvard T. H. Chan School of Public Health. Department of Environmental Health (MIPS Program). 665 Huntington Avenue - Bulding 1, Roon 1309. Boston, MA
ABSTRACT
INTRODUCTION: Sudden Cardiac Arrest (SCA) is a serious public health problem and represents one of the leading causes of death in the world. In emergency situations the assessment of the victim and care must be effective, to reduce negative outcomes and to increase the survival rate
OBJECTIVE: To analyze graduation students in the Health Sciences through objective testing on Basic Life Support (BLS
METHODS: This is a descriptive, observational and cross sectional study, performed in the State of São Paulo, Brazil. The study population consisted of 664 graduation students in Medicine, Nursing, Physiotherapy, Pharmacy, Nutrition and Occupational Therapy. Data collection occurred through an instrument in the form of objective tests based on the guidelines for Basic Life Support from the American Heart Association. For analysis the Shapiro-Wilk, Chi-square, Mann-Whitney and Kruskal-Wallis tests were used. The adopted confidence level was 95%. The statistical program used was Stata 11.0
RESULT: There was found to be a prevalence of students who were female (82.23%), single (77.56%), on the physiotherapy course (53.16%), in the freshmen year (32.2%) with previous training (54.45%) and with a median age of 22 years old. When the association between the scores was analyzed according to sex, marital status, previous training, course and year of study, the relation between the number of correct answers and previous training, course and year of study showed statistically significant differences (p < 0.001
CONCLUSION: 99.9% of subjects had lower score than the minimum score of 84% of Americam Heart Association, which characterizes insufficient knowledge about the basic support of life theme. Thus, there is need for continued training of health sciences students on the subject, at the undergraduate level
Keywords: basic life support, training, graduate students, knowledge, evaluation, questionnare.
INTRODUCTION
The Sudden Cardiac Arrest (SCA) is a serious public health problem and constitutes one of the main causes of death in the world.1 The population's lack of training and knowledge contributes to the maintenance of the high failure rates in cardiopulmonary resuscitation.2
In emergencies, the assessmentand care of thevictimmust be effective, to reducenegative outcomes and increase survival.3 However, there are differentiated levels of knowledge in the population concerning assistance in cases of SCA, which are specific to inside and outside the hospital, according to available resources and equipment, as well as the individual's knowledge on the action to be taken.
Within the scope offirst aid, basic life support (BLS) should be part of community-wide efforts, which include prevention, cardiopulmonary resuscitation, prompt access to emergency services, advanced life support in paediatrics (ALSP), followed by integrated post-resuscitationcare. Ofthese five links in the survival chain of the American Heart Association, the first three form BLS.4
Thus, in thecontextof the BLS action knowledge, people are considered to be laypersons or not laypersons. Non-graduates in any health science area or those who have not had training in BLS are considered laypersons, and not laypersons are graduates in the health sciences or trained professionals working in the health area.2
It is widely accepted that in the case of collapse due to cardiac arrest, those who are assisted quickly and effectively have a greater chance ofsurvival and absence of negative outcomes. However, individuals who suffer sudden cardiac arrest depend on basic life support because the chances of survival decrease by 7-10% every minute elapsed after a cardiac arrestwithout defibrillation if indicated.2 In this sense, the training of laypersons to provide early care in emergencies is crucial to saving lives and preventingnegative outcomes.2
There is consensus that early training favours the retention of knowledge and reinforces the concept of social obligation to help others.6 In addition, the continuing education process is a great strategy to reach a wide audience and to increase survival from cardiac arrest witnessed by bystanders in the community.5,6
Training in BLS promotes specific skills (cognitive) that enable the identification of SCA by members of the publicand contributestothe process of interventions before this sudden event. Studies indicate that educating the public (potential witnesses) to intervene in SCA cases increases the survival rate of victims by two to three times compared to those who do not receive inter-vention.7,8
According to the guidelines for cardiopulmo-nary resuscitation and emergency cardiovascular care of the Brazilian Society of Cardiology, it can be estimated that 200,000 cardiac arrest so ccur per year in Brazil, with half of the cases occurring outside hospital.2 According to Meissneretal,5 people sufferingh eart failure depend on available basic life support which increases the chance of survival by 2 to 3 times, but studies show that in less than a third of cases of cardiac arrest, where a witness was present, the victim received CPR.5
The biggest challenge, especially in Brazil, is to increase access to CPR education, establishing processes for continuous improvement in quality, while minimizing the time between CPR and the application of the first defibrillator shock.2
The better understanding of potential barriersfor performing CPR can generate actions that increase its rates, especially in the extra-hospital environment2 so in view of there levance of the data, it was decided to investigate the knowledge of students in the health sciences on BLS.
Thus, the objective of this research is to analyze the knowledge of graduate students in the health sciences on basic life support.
METHODS
The study was approved by the Ethics Committee of the ABC's Medical School, number 557-716 on 03.12.2014.
This is andescriptive, observational and cross sectional study conducted in São Paulo, Brazil. The study population consisted of undergraduates of medical, nursing, physiotherapy, pharmacy, nutrition and occupational therapy schools in seven institutions located in Sao Paulo, Santo André, Sorocaba and Jundiaí, all in the state of São Paulo, Brazil.
The data collection instrument was a ques-tionnaire developed by the researcher based on the guidelines for basic life support of the American Heart Association (2010).
The objective questionnaire applied was prepared for respondents with a health professional degree or trained on this topic (considered not a layperson), but the researcher applied this instrument considering the students as a laypublic. It was composed of 20 objective questions and each question contained four alternatives, with one correct answer. The questionnaire had an open question on the demographics, asking if the student hadanyprior training in basic life support, and if a positive response, for how long.
A total of 1,300 tests using the objective questionnaire model were applied. In the final sample, 664 tests were included for results analysis, occurring a loss of nearly 50% of the sample due to not completing the demographic data or not fully completing the questionnaire.
The questionnaire was administered ona single occasion. The individuals received a password with a number to identify the questionnaire documents, a feedback sheet and a free and informed consent form. This option was offered in order to preserve the anonymity of research participants.
The number of correct responses considered ideal for data analysis was 84%, based on the amount of necessary adjustments in the BLS American Heart Association course, on which the guidelines for this study werebased.
As for statistical analysis, for the qualitative variables we used absolute and relative frequency and for quantitative variables, median and percentiles 25 and 75%, respectively, by non-normal distribution observed by Shapiro-Wilk test (p < 0.05).
To analyze the association between previous training, respondent's sex, course of study and year of study we used the chi-square test; and to evaluate the difference of right answers between groups, we used confidence interval of the median and the Mann-Whitney test. To assess the difference between the amount of right answers and courses, years of education and marital status, we used confidence intervals of the median and Kruskal-Wallis. The adopted confidence level test was 95%. The statistical program used was Stata 11.0.
RESULTS
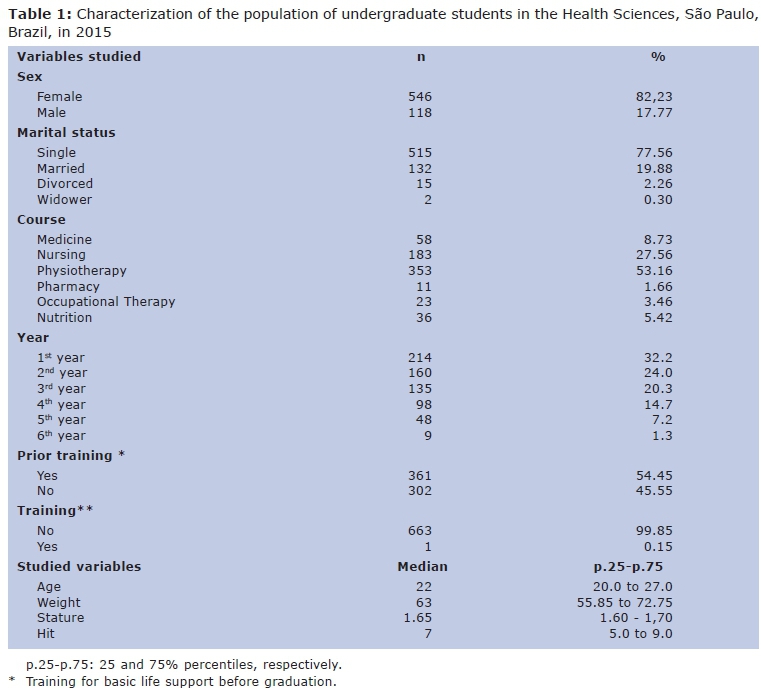
The sample consisted of 664 individuals, of which there was a prevalence of students who were female (82.23%), single (77.56%), from the physiotherapy course (53.16%), in their first year of study (32.2%) with previous training (54.45%) and the median age was 22 years (Table 1).
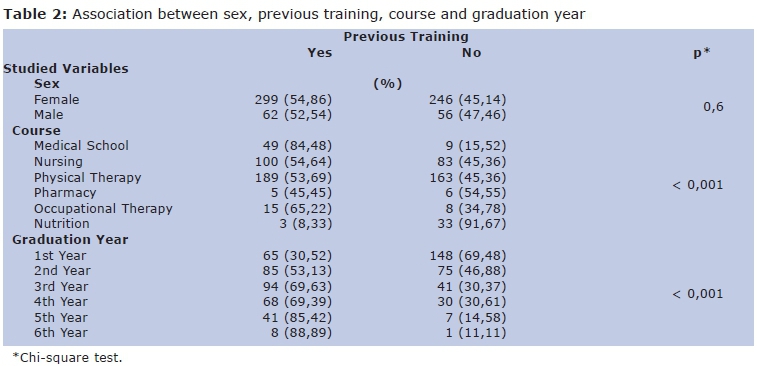
I relation to previous training, it was associated to course and year of study, in which statistically significant differences (p < 0.001) were found. Comparing the courses, 84.8% of students on a medical course had previous training and, comparing the year of study, 88.89% of students in their 6th year had previous training (Table 2).
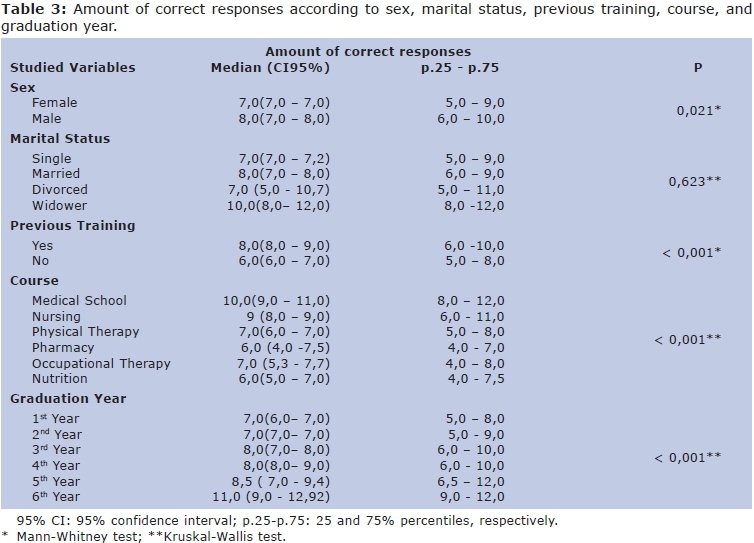
There was association between the number of correct responses and the variables of prior training, course of study and year of study showed statistically significant differences (p < 0.001). Between the sexes, male respondents obtained the highest number of correct answers ranging between 7.0 and 8.0, high lighting also the widowed individuals who scored between 8.0 and 12.0. Participants who had prior training had scoresrangingfrom 8.0 to 9.0. When taking into consideration the current course and year of study, the medical school was between 9.0 and 11.0 and 6th grade obtained scores of between 9.0 and 12.92 (Table 3).
DISCUSSION
The results reveal that 84.48% of medical students had previous training and that 88.89% of 6th year medical students had previous training. Between the sexes, male students obtained the highest scores. Participants who had prior training scored similarly well. However, while most students claimed to have some previous training, perfor-mance was unsatisfactory in the majority relative to the desired level, since only one student had a percentage score above 84% in the questionnaire.
We know that education is a dynamic process that involves multiple aspects, from actual human (such as cognition and skills development) to social (cultural and political).9 The educational methodthat is usedin health care is currently grounded on developing students' skills so that they can deal with the eventualities of clinical practice.
With regard to assistance to victims of sudden cardiac arrest (SCA), little knowledge or incorrect knowledge on Basic Life Support (BLS) can compromise the survivalof the victim.3 Thus, this study demonstrates that the percentage scored was lower than expected, according to the amount of necessary adjustments in the BLS course of the American Heart Association (2010). These results converge with the study of Pergola and Araújo,3 when performed with a lay population.
In the same study of Pergola and Araújo,3 over 90% of health professionals asserted that they wereable to perform BLS procedures, although less than 40% performed themcorrectly.
Regarding previous BLS training, more than 50% of students said they went through training. However, although theystatedthat they had com-pleted prior training, when compared to students who hadnot, both produced unsatisfactory results, below the level expected.
The medical school students reported having had more previous training, also students of the sixth year of its course were those who showed greater knowledge. It was evident too that as thenumber of years of study increased the obtained results, although poor, were progressively better. This shows improvement in learning over the years of study.
Although it is not known what these students understand as previous training and what kind of training they have undergone, it is known that the adequate preparation of these future health professionals is of immense importance, for the proper implementation of BLS toincrease survival ratesand reduce negative outcomes of victims.
Regarding the number of correct answers in the BLS questionnaire, students of medical school had greater success than the nursing course, which in turn had greater success than the physical therapy course students and these were significantly higher than the other courses studied.
Maybe because of the greater opportunity toapproach this issue in universities, medical, nursing and physical therapy students showed greater theoretical knowledge of this subject, since it is an area where the professional works directly with the patient and thus has greater opportunity to witness the sudden collapse of expertise in providing BLS.
However, unsatisfactory results are probably related to the greater number of survey responses by first-year undergraduate students, although students from other years also did not obtain satisfactory results, which can demonstrate the need for training that favours the construction of this knowledge.
Knowledge is considered the starting point for decision-making in an attempt to ensure the quality of procedures performed with the victim at the scene, in order to promote and maintain the victim's life.10,11
Medical schools are taking on the challenge of modifying their curriculum, as current trends in education aim at a comprehensive education, seeking the integration between basic and biomedical sciences with clinical science to reduce thehigh burden of unnecessary expertise.12
The importance of acquiring skills to support scientific knowledge is undeniable, ensuring greater efficiency in a situation where the good use of time is paramount. Thus, it is probable that a doctor who in his or herundergraduate studieshad training in basic life support techniques, can naturally develop better basic skillsin emergency situations.10,11
Therefore, the curriculum/extracurricular of medical undergraduates must also have as its mainstay BLS training in all contexts inside and outside the health services. A proper introduction to knowledge and skills in first aid and CPR should be considered an essential aspect of the medical curriculum.13
However, students must acquire capabilities in realistic contexts, which facilitate knowledge and skills acquisition, or improve these through the process. Among the capabilities, those that are theoretical and practical present better results, as they offer better returns of knowledge and skills construction.14,15
On the other hand, it is still considered important to encourage research in this area, so that visibility is given to situations like these. However, while scientific production has been increasingin Brazil, it would significantly increase with the proper training of health professionals who work with management projects research.16,18
According to the BLS course of the American Heart Association (2010), individuals are considered qualified when scores of 84% are obtained in a questionnaire similar to that in Annex 1. However, of the 664 subjects who completed the questionnaire on BLS, just one achieved a scoregreater than or equal to 84% and the others had lowerresults in this American Heart Association's indicator.
One limitation of this study was thatthe individuals did not have training in BLS techniques, which reinforces the need for mass training of these procedures, especially in university healthcare.
The results imply that efforts should be made for the Basic Life Support techniquesto be introduced into the curriculum from the first year of undergraduate studies and for subsequent years, so that knowledge and skills are enhanced, and in turn, can be effectively implemented. On the other hand, continuing education is of even more importance so that the developed practices are increasingly implemented properly tomeet the needs of individuals.
Students had insufficient knowledge in Basic Life Support, emphasizing the need to provideand enhanceinformation on this topicduring under-graduate studies, andthrough continuous education, providing trainingat different timeswhich would helpin the retentionof knowledge andencourage intervention by students faced with are al situation of cardiac arrest.
CONCLUSION
Conclusion: 99.9% of subjects had lower score than the minimum score of 84% of Americam Heart Association, which characterizes insufficient knowledge about the basic support of life theme. Thus, there is need for continued training of health sciences students on the subject, at the under-graduate level.
Acknowledgments: The author thanks Professor Dr. Luiz Carlos de Abreu and all scientific methodology group in the relevant contributions to this article.
REFERENCES
1. Swor R, Khan I, Domeier R, Honeycutt L, Chu K, Compton S. CPR training and CPR performance: do CPR-trained bystanders perform CPR? AcadEmerg Med. 2006; 13(6): 596-601. DOI: http://dx.doi.org/10.1197/j.aem.2005.12.021 [ Links ]
2. Gonzalez MM, Timerman S, Gianotto-Oliveira R, Polastri TF, Canesin MF, Schimidt A, et al. I Guideline for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care - Brazilian Society of Cardiology: Executive Summary. ArqBrasCardiol. 2013;100(2):105-13. DOI: http://dx.doi.org/10.5935/abc.20130022 [ Links ]
3. Pergola AM, Araujo IE. Laypeople and basic life support. Rev Esc Enferm USP. 2009; 43(2): 335-42. DOI: http://dx.doi.org/10.1590/S0080-62342009000200012 [ Links ]
4. Berg MD, Schexnayder SM, Chameides L, Terry M, Donoghue A, Hickey RW, et al. Part 13: pediatric basic life support: 2010 American Heart Association Guidelines for Cardiopul-monary Resuscitation and Emergency Cardiovascular Care. Circulation. 2010;122(18 Suppl 3):S862-75. DOI: http://dx.doi.org/10.1161/CIRCULATIONAHA.110.971085 [ Links ]
5. Meissner TM, Kloppe C, Hanefeld C. Basic life support skills of high school students before and after cardiopulmonary resuscitation training: a longitudinal investigation. Scand J Trauma ResuscEmerg Med. 2012;20:31. DOI: http://dx.doi.org/10.1186/1757-7241-20-31 [ Links ]
6. Roppolo LP, Pepe PE. Retention, retention, retention: targeting the young in CPR skills training! Crit Care. 2009;13(5):185. DOI: http://dx.doi.org/10.1186/cc7997 [ Links ]
7. Fredriksson M, Herlitz J, Nichol G. Variation in outcome in studies of out-of-hospital cardiac arrest: a review of studies conforming to the Utstein guidelines. Am J Emerg Med. 2003; 21(4): 276-81. [ Links ]
8. Perkins GD, Brace SJ, Smythe M, Ong G, Gates S. Out-of-hospital cardiac arrest: recent advances in resuscitation and effects on outcome. Heart. 2012;98(7):529-35. DOI: http://dx.doi.org/10.1136/heartjnl-2011-300802 [ Links ]
9. Maia JA. Metodologias problematizadoras em currículos de graduação médica. RevBrasEduc Med. 2014;38(4):566-74. DOI: http://dx.doi.org/10.1590/S0100-55022014000400018 [ Links ]
10. Vieira LJES, Carneiro RCMM, Frota MA, Gomes ALA, Ximenes LB. Actions and possibilities of accidents prevention with children in daycare at Fortaleza, Ceara State. CiencSaude Coletiva. 2009;14(5):1687-97. DOI: http://dx.doi.org/10.1590/S1413-81232009000500010 [ Links ]
11. Vieira JE, Tamousauskas MRG. Avaliação das resistências de docentes a propostas de renovações em currículos de graduação em medicina. RevBrasEduc Med. 2013; 37(1): 32-8. DOI: http://dx.doi.org/10.1590/S0100-55022013000100005 [ Links ]
12. Quintero GA. Medical education and the healthcare system-why does the curriculum need to be reformed? BMC Med. 2014;12:213. DOI: http://dx.doi.org/10.1186/s12916-014-0213-3 [ Links ]
13. Tan EC, Hekkert KD, van Vugt AB, Biert J. First aid and basic life support: a questionnaire survey of medical schools in the Netherlands. Teach Learn Med. 2010; 22(2): 112-5. DOI: http://dx.doi.org/10.1080/10401331003656538 [ Links ]
14. Alves TS, Cogo ALP. Searching for evidences for Training in Basic Life Support - a systematic literature review.Online Braz J Nurs. 2006; 5(2). [ Links ]
15. Bezerra IMP, Machado MFAS, Souza OF, Lima Antão JYF, Dantas MNL, Reis AOA, et al. Professional activity in the context of health education: a systematic review. J Hum Growth Dev. 2014;24(3):255-62. DOI: http://dx.doi.org/10.7322/jhdg.88909 [ Links ]
16. Monteiro CBM, Almeida Junior ÁDd, Wajnzstejn R. Project management in health and medical research. J Hum Growth Dev. 2014; 24(3): 239-242. DOI: http://dx.doi.org/10.7322/jhdg.88895 [ Links ]
17. Ferreira M, Ferreira C, de Abreu LC, Valenti VE, Murad N, Meneghini A, et al. Myocardium tissue changes caused by electrical transthoracic discharges in rats. IntArch Med. 2009;2:31. DOI: http://dx.doi.org/10.1186/1755-7682-2-31 [ Links ]
18. Herrero D, Gallo PR, Fujimori M, Monteiro CBM, Valenti VE, Tavares CM, et al. Motor development of infants exposed to maternal human immunodeficiency virus (HIV) but not infected. Int Arch Med. 2013;6:45. DOI: http://dx.doi.org/10.1186/1755-7682-6-45 [ Links ]
Manuscript submitted Oct 22 2014
Accepted for publication Dec 19 2014.
Corresponding author: Luis Fernando Barbosa Tavares. E-mail: luisfbt@hotmail.com
Appendix
Faculdade de Medicina do ABC
Departamento de Saúde da Coletividade
Disciplina de Metodologia Científica
Serviço do Prof. Dr. Luiz Carlos de Abreu
APPENDIX 1. Objective questionnaire
Name: _____________________________________________________________________________
Signature: _________________________________________________________________________
Age: Sex: Marital
Status:______________ Weight: Height: ______________Course: ______________
ave you had a Basic Life Support lesson: Yes ( ) / No ( )
If you did, for how long: _____________________________________________________________________________
Abbreviations and definitions of interest to answer the questionnaire:
Abbreviations of interest in the questions:
CPR (cardiopulmonary resuscitation) / SCA (Sudden Cardiac Arrest) / AED (automatic electric defibrillator) / BLS (basic Life support)
Definitions of interest for interpreting the questions:
- Definition of Basic Life Support: Sequence of procedures provided to a person in the event of cardiac arrest outside the hospital.
According to the World Health Organization:
- Infant is defined as: Individuals from 28 days to 24 months
- Child is defined as: Individuals from 24months to under 10 years of age
- Teenager is defined as: Individuals from 10 years to 20 years of age
- For the purposes of this guideline (Part 13: Pediatric Basic Life Support: 2010 American Heart Association Guidelines Cardiopulmonary Resuscitation for Emergency and Cardiovascular care) and responses to this questionnaire, use the following classification:
- BLS guidelines for infants: Less than 1 year old.
- BLS guidelines for kids: This applies to children of about 1 year of age up to puberty. Puberty for educational purposes is defined as the development of breasts in women and the presence of axillary hair in men.
- BLS guidelines for adults: Applied to individuals from puberty and beyond.
QUESTIONS
1. We can sequence the survival chainof the infant and child asbeing?
a) prevention, call, airways,cardiopulmonary resuscitation, post-resuscitation care
b) prevention,cardiopulmonary resuscitation, call, advanced life support, post-resuscitation care
c) prevention, airways, cardiopulmonary resuscitation, call, advancedlife support
d) prevention, airways, call, cardiopulmonary resuscitation, post-resuscitation care
2. What are the sequential clinical parameters that shouldbe used to recognize a cardiac arrest?
a) not responsive, apnoeaorgasping, no palpable peripheral pulse within 3 seconds
b) responsive, not only with gasping, without palpable peripheral pulse within 10 seconds
c) apnoea, not responsive, with out central pulse palpable inup to 3 seconds
d) not responsive, apnoea or just with gasping, without central pulse palpable within 10 seconds
3. You're alone and find a child of 3 years unconscious and know that the child was not a victim of trauma. What is the sequence of actions that must befollowed?
a) check out the responsiveness, check the breathing for10 seconds, cry for help, start cardiopulmonary resuscitation by 1 minute and after leaving the victim and ask for help and an AED
b) check responsiveness, cry for help, check the breathing up to 10 seconds, start CPR for 2 minutes and cardiopulmonary after leaving the victim and ask for help and an AED
c) cry for help, check out the responsiveness, check the breathing up to 4 seconds, after leaving the victim and ask for help and an AED and start cardiopulmonary resuscitation
d) check the breathing up to 10 seconds, check responsiveness, cry for help, start vents for 2 minutes and after leaving the victim and ask for help and an AED
4. Once cardiopulmonary arrest has been diagnosed, cardiopulmonary resuscitation must be carried out in the following sequence:
a) air vents opening, thoracic compressions
b) airway opening, chest compressions, ventilations
c) chest compressions, airway, openingvents
d) chest compressions, ventilations, airway opening
5. During high quality cardiopulmonary resuscitation, how many compressions should be done for a minute?
a) at least 60 compressions
b) at least 80 compressions
c) at least 150 compressions
d) at least 100 compressions
6. With regards to chest compressions during high quality cardiopulmonary resuscitation, we should compress the chest to a depthof:
a) at least 1/3 of the anterior-posterior diameter of the chest in children (5 cm) and 1/3 in infants (4cm)
b) at least 1/2 of the anterior-posterior diameter of the chest in children (7 cm) and 1/3 in infants (4cm)
c) at least 1/3 of the anterior-posterior diameter of the chest in children (5 cm) and 1/2 in infants (6cm)
d) at least 1/2 of the anterior-posterior diameter of the chest in children (7 cm) and 1/2 in infants (6cm)
7. During cardiopulmonary resuscitation with 2 first responders, we must:
a) allow the total return of the chest wall between compressions and do not change the functions of the first responders after 2 minutes
b) allow the partial return of the chest wall between compressions and do not change the functions of the first responders after 2 minutes
c) allow the total return of the chest wall between compressions and change the functions of the first responders after 2 minutes
d) allow the partial return of the chest wall between compressions and change the functions of the first responders after 2 minutes
8. During the re-evaluation of the patient every 2 minutes in cardiopulmonary resuscitation, we should:
a) try to limit interruptions in chest compressions to less than 3 seconds
b) try to limit interruptions in chest compressions to less than 10 seconds
c) try to limit interruptions in chest compressions to less than 15 seconds
d) try to limit interruptions in chest compressions to less than 20 seconds
9. On checking pulses during a suspicion of cardiopulmonary arrest, we should preferably opt for:
a) check central pulse (femoral or brachial) in infants and carotids in children and teenagers
b) check central pulse (femoral or carotid) in infants and brachial children and teenagers
c) check central pulse (femoral or brachial) in infants and brachial children and teenagers
d) check central pulse (femoral or carotid) in infants and carotids in children and teenagers
10. The correct manoeuvre for opening the airway is:
a) just lifting the chin for patients who have been the victims of trauma
b) head tilt and chin lift for patients who have not been victims of trauma
c) head tilt and chin lift for patients who have been victims of trauma
d) inclination of the head only to patients who have been victims of trauma
11. During cardiopulmonary resuscitation, with out aguaranteed advanced air route, the relationship between compressions-vents must be:
a) 30 compressions to 2 breaths in any age group with 2 rescuers
b) 15 compressions to 2 breaths only for children with 1 rescuer
c) 30 compressions to 2 breaths in any age group with 1 rescuer
d) 15 compressions to 2 breaths only for infants with 2 rescuers
12. In a child in cardiopulmonary arrest with advanced airway, we must:
a) perform 30 compressions to 2 breaths in any age group with 2 rescuers
b) no longer synchronize vents with compressions, perform 130 compressions per minute and do 20 breaths per minute
c) no longer synchronize vents with compressions, performat least 100 compressions per minute and do10 breaths per minute
d) perform 30 compressions to 2 breaths in any age group with 1 rescuer
13. You are walking in a park and witnessed a sudden collapse in a teenager, and there's no one else around but you and the victim. What is the sequence of actions that should be followed:
a) check responsiveness, checking breathing for 10 seconds, cry for help, start compressions for 2 minutes and after leaving the victim ask for help and an AED
b) check responsiveness, check breathing and if there is no response and no breath, do not abandon the victim, gotoaphone and ask for help and an AED, return to the victim and check her pulse, and if there is no pulse, begin CPR
c) quickly check wrists, if there is no pulse, begin CPR and after 2 cycles of compressions/vents 30:2 leave the victim and ask for help
d) check out the responsiveness, check the breathing until 4 seconds, check the pulse, cry for help, start vents for 2 minutes and after leaving the victim ask for help and an AED
14. With respect to the use of theAED:
a) cannot be used ininfants
b) use only in children and adolescents and the children's paddles should be used until 5 years of age
c) use the paddles AED for children up to 1 year of age
d) can be used in any age group and the paddles infant AED must beused up to 8 years of age if available
15. During high quality CPR,effective vents mean:
a) vents that produce visible chest rise
b) vents that produce chest hyper expansibility
c) vents that don't necessarily produce visible chest rise
d) vents that alternate with chest's hyper expansibility and hypo expansibility
16. The characteristics of high quality CPR are:
a) start compressions in the first 20 seconds, compress with force and speed, allowing the total return of the thorax, minimize interruptions in compressions to less than 5 seconds, administer effective vents, avoid excessive ventilation
b) start compressions in the first 15 seconds, compress with little strength and slowly allow the total return of the thorax, minimize the interruption in compressions toless than 5 seconds, administer effective vents, avoid excessive ventilation
c) start compressions in the first 20 seconds, compress with force and speed, allowing the total return of the thorax, minimize interruption in compressions to less than15 seconds, administer effective vents, producing excessive ventilation
d) start compressions in the first 10 seconds, compress with force and speed, allowing the total return of the thorax, minimize the interruption in compressions to less than 10 seconds, administer effective vents, avoid excessive ventilation.
17. The basic life support consists of:
a) airway opening intubation, orotracheal ventilation, thoracic compressions, vascular access, use of adrenaline
b chest compressions, airway, ventilation, defibrillation (AED)
c) chest compressions, tracheal intubation, ventilation, defibrillation (AED), vascular access
d) vascular access, opening of airway, ventilation, chest compressions, adrenaline, manual defibrillation
18. With respect to ventilation of the patient in BLS, tick the correct alternative:
a) must be asyn chronous with the compressions during CPR
b) in the case of having initially only a respiratory failure, we should ventilate the child 30 time sper minute
c) each ventilation should last about 5 seconds and we must promote a large thoracic expand ability
d) each vent must have a duration of about 1 second and promote visible chest rise
19. With respect to defibrillation with an AED, select the correct answer:
a) we should use the paddles AED for children up to 1 year of age
b) the use of AED is not indicated for children under 1 year of age
c) after each shock immediately restart the chest compressions
d) after each shock should check the responsiveness, breathing, and if necessary, restart thoracic compressions
20. The steps to use an AED are:
a) turn on the unit, place electrodes on the chest, wait for the AED to analyze the pace, move away from the victim, release for the shock if indicated
b) turn on the unit, analyze the rhythm, place electrodes on the chest, release for the shock if indicated, move away from the victim
c) put electrodes, call the appliance, check the pulse, analyze the rhythm, release for the shock if indicated
d) call the appliance, check the pulse, put electrodes on the chest, move away from the victim, a wait the AED to analyze the rhythm, release for the shock if indicated


{kind=link}
{kind=link}
{kind=link}