










Serviços Personalizados
artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282versão On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.26 no.1 São Paulo 2016
http://dx.doi.org/10.7322/jhgd.113717
ORIGINAL RESEARCH
Communicative indicators, motor and cognitive development of hearing-impaired children
Érica Endo AmemiyaI, *; Alexandra Dezani SoaresII; Brasilia Maria ChiariIII
IFederal University of São Paulo (UNIFESP)
IISpeech pathologist in the Cochlear Implant Team - HSP- UNIFESP
IIIProfessor at the Department of Phonoaudiology (Speech Pathology) - UNIFESP
ABSTRACT
INTRODUCTION: For the assessment of child development in the deaf is effective protocols are needed for this population, as in Brazil, standardized tests for these children are still scarce 4.5. Thus, emphasis is placed on studying child development in deaf so that therapeutic and educational approaches are contemplated in accordance with the needs of each child.
OBJECTIVE: Analyze the performance of children with hearing deficit in different areas: Communications-Issue, Communication-reception, aspects Motors and Cognitive Aspects of Language.
METHODS: We have carried out a comparative study in an institutional clinic with 109 children, divided into 60 hearing individuals with typical development and 49 with hearing loss, severe to profound. The performance index was calculated for each child in these four domains. The index was analysed according to the equation: (number of responses in each area / number of assessed behaviours) x100.
RESULTS: In all age groups, hearing-impaired children had a smaller performance when compared to hearing children in the Communication - Emission domain. The Communication-Reception domain showed significant differences (p < 0.05) from the 12-to-23-months to the 60-to-71-months age groups. The Cognitive Aspects domain demonstrated a significant difference (p < 0.01) between hearing-impaired and hearing children aged 24 to 35 months and onwards. Motor Aspects only had a significant difference (p < 0.01) in the last two age groups, 48-59 months and 60-71 months. The significance level was 5%.
CONCLUSION: In all age groups, hearing-impaired children's performance was worse when compared to hearing children. The intervention made by health professionals ought to take place as soon as possible in order to develop the cognitive, motor and language skills of the hearing-impaired child.
Keywords: hearing loss, child development, language development disorders.
INTRODUCTION
During the process of child development, sensorial ruptures such as hearing loss can worsen language acquisition to a lesser or greater degree. Language acquisition is crucial because language, being a strictly human form of communication, transmits complex information from one person to the other1 and the linguistic code allows us to express language2.
Hearing loss during a child's development can change the relationship between form and content, usage and linguistic levels such as syntactic and semantic vocabulary3,4.This proofs that studying child development is a complex task that demands a systematic, detailed and insightful approach from the researcher.
In order to make the assessment of child's development in hearing-impaired children effective, we need to establish protocols for this population, since in Brazil, standardized tests for these children remain scarce4,5. Therefore, we emphasize studying child development in hearing-impaired children so therapeutic and educational approaches can be carried out according to the necessity of each child.
Having in mind how important this subject is, our objective was to investigate the performance of children with hearing deficit in different domains: Communication-Emission; Communication-Reception; Motor Aspects and Cognitive Aspects of Language and compare them with hearing children.
METHODS
This is a comparative study.
The study group (SG) comprises children with neurosensory hearing loss from a severe degree to profound bilateral and the control group (CG) comprises hearing children with no learning or development complaint.
In total, the study was based on 109 children of both sexes and aged 0 to 71 months. Among them, 60 [55%] were hearing children and 49 [45%] were hearing-impaired children, 58 [53,2%] were female and 61 [46,8%] were male.
Among the female children, 32 [53,3%] were hearing and 26 [53,1%] were hearing-impaired children. When it comes to the figures regarding male children, 28 [46, 7%] were hearing and 23 [46,9%] were hearing-impaired.
60 hearing children came from the children's school of the institution, 11, aged 4 to 6 years old, came from the municipal school and 38 hearing-impaired children, aged 0 to 6 years old, came from ambulatory care.
The sample in this study had enough statistical power (95%). 102 individuals would be necessary to carry out this study, according to the statistical program GPower, having a sample proportion of 1:1 and not having any loss in terms of samples.
Hearing-impaired children (GE) complied with the following inclusion criteria: having prelingual hearing loss, in other words, the hearing loss occurred before the age of 3; aged between 0 and 71 months and neurosensory hearing loss from a severe degree to deep bilateral6. Hearing children, on the other hand, complied with following criteria: not presenting any hearing complains or complaints related to communication or learning, and being between the age of 0 and 71 months.
The criteria for exclusion, both for hearing-impaired children as well as hearing children, were: children that have cognitive, visual, psychiatric, neurologic and motor impairments noticed by the assessor, free and clarified consent form and/ or an approval form not signed by the parent or guardian responsible for the child's participation in the research.
We took into account the samples by spontaneous demand of hearing-impaired 0-to71-months children in the ambulatory care when they attended the service to receive the audiological diagnosis and the indication of electronic devices.
The instrument used to gather the data was "Proposal of data systematization of phonoaudiological assessment through the observation of 0-to-6-year-old children's behaviour"4. It is composed of four domains: Communication-Emission; Communication-Reception; Motor Aspects and Cognitive Aspects of Language. Each domain addresses expected behaviour for each age, taking into account the presence or absence of each one of them. The participants underwent similar procedures in the three places where samples were collected.
We have carried out a brief anamnesis and afterwards we started activities that allowed us to notice or not the presence of expected behaviours according to the age. Playful materials were used during the entire assessment (paper, black and colour pencils, scissors, glue, cardboard box, pieces of tissue, mirror, nylon thread, play dough, plastic throw rings, cardboard or plastic cones, rattle, wooden cubes, bench, balls, plastic animals, trucks, dolls, family puppets, wooden beads, miniatures of kitchen utensils, animals, means of transportation, fruits, house, hairbrush, comic books, children stories, plastic letters and numbers, boards with geometric shapes, boards with incomplete drawings to fill out, incomplete human figure, puzzles and different pictures).
The assessment was recorded with a digital Sony camera, Cyber-shot DSC-W30 model, and the footage was analysed afterwards. The sessions lasted approximately 40 minutes.
The protocols were filled out by three speech pathologists at the same time while the video of the child was presented. The three of them had experience in assessing hearing-impaired children. The behaviour was only considered present or absent when there was a consensus of at least two of the assessors. When there was no consensus among the assessors, a third opinion was consulted.
The data collected was analysed by the statistic programme SPSS version 19.0.
Furthermore, the analysis of the answers in the behaviour of hearing and hearing-impaired children is presented based on the median distribution divided by age.
The performance in Communication-Emission; Communication-Reception; Motor Aspects and Cognitive Aspects of Language performance index was calculated to each child.
The indexes were analysed in regards to the presence of answers in each domain, according to the calculation: number of present behaviours/ total of analysed items. The significance level adopted was 5%.
RESULTS
The study group (SG) was formed by children with neurosensory hearing loss from a severe degree to profound bilateral and the control group (CG) comprises hearing children with no learning or development complaints.
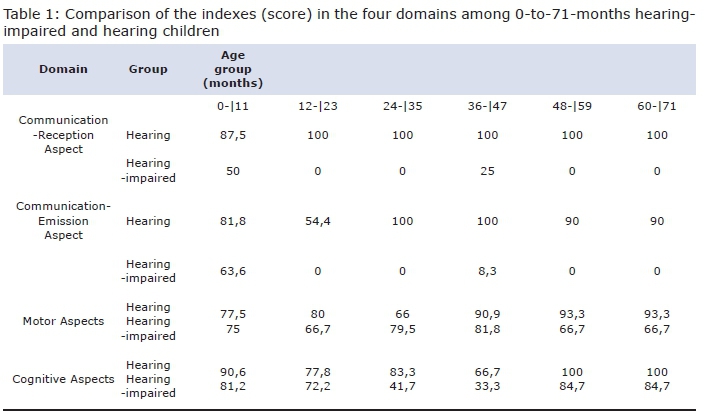
"Table 1: Comparison of the indexes in the four domains among 0-to-71-months hearing-impaired and hearing children" describes the median of indexes in each large domain of the ages that vary from 0 to 71 months. These indexes indicate hearing and hearing-impaired children's presence of answers.
On one hand, the Communication-Emission domain presented significant differences in all age groups. On the other hand, the Communication-Reception domain presented significant differences only at the 12- to-23-months age group. The 24-to-47-months age group had significant differences in the domains: Communication-Reception, Communication-Emission and Cognitive Aspects of Language. The 48-to-71-months age group had significant differences in all four domains (p<0, 05).
DISCUSSION
The first age group analysed, 0 to 11 months, corresponds to the beginning of development and the first year of life. We can notice the first communicative resources used by children, which are already experiencing a large influence of hearing loss. The Communication - emission domain was the only one that showed a significant difference (p < 0,05). In this domain, the behaviour "Vocalization with a variation in intonation after various stimuli" was the most affected one.
Studies in the literature7,8 confirm this, because 0-to-11-months children with hearing loss may present alterations in prosody, which are noticed since the beginning of vocalizations9 . The latter are resources used by children to call the adult's attention. The development of prosody is compromised in hearing-impaired children due to the hearing difficulty to notice prosodic traces, which results in alterations of vocalization, absence of consonants and modifications in the sound of vowels 7.
In the 12-to23-months age group, we noticed significant differences in the Communication-Reception and Emission domains10,11. Studies affirm that a child aged 12 to 16 months with moderate to profound degree hearing loss are underdeveloped in terms of receptive and expressive language skills when compared with children with mild hearing loss. Thus, it emphasizes the importance of hearing feedback in language development10,11.
The 24-to-25-months age group showed significant differences in three domains: Communication - Reception and Emission and cognitive aspects of language. Regarding Communication - Reception and Emission, all the behaviours were absent. When hearing-impaired children grow up without auricular electronic devices and with no multidisciplinary support, the deficit becomes more prominent5.
In case of medium otitis between 26 to 28 months, we notice a negative impact in the perception of speech, which influences both reception and emission, especially for consonants such as /s/ and /z/, compromising learning11,12.
Hearing-impaired children aged 36 to 47 months who use an Individual Sound Expansion Device (ISED) have a performance that is compatible to normality when it comes to expressive vocabulary. This, however, did not occur in the results seen in this study, because children had a compatible performance only in motor aspects3. The Cognitive Aspects of Language domain presents significant differences. Behaviours such as "joining part 2 and 3 to form the whole", "combining 1 to 1, 3 or more objects" and "memorizing pictures (the child is capable of selecting a stimulus among others)" are altered, which means that the hearing-impaired child's symbolic thinking is already underdeveloped compared with hearing children8.
After the initial development phase, the first years of life, in which motor actions to know and organize the world prevail, is followed by a phase in which leaning is based on the senses13. Having hearing deficits in this age group makes it difficult to understand ambiguous messages, jokes, ironies and suspense, voice control, and causes the production of phonetic and articulating mistakes throughout the language development12. Children with hearing loss in the 48-to-71-months age group in this study were lagging behind in regards to language development14. In the reality of hearing-impaired children, the use of syntax similar to that of adults, the expansion of adjectives and phrasal verbs, negative sentences and yes and no question are hardly reached. This demonstrates that the child with hearing loss dos not have the opportunity to socially develop language and speech skills, since these are built through conversation and personal reports15-17.
In order to making it possible for a child with hearing loss to reach good performance in language acquisition, one needs technological and educational apparatus and a healthy family environment, as well as cognitive skills13,18-20. Cognitive functions such as attention, categorization, learning and memory can influence the way the cognitive system processes a sensory entrance coming from electronic devices, such as cochlear implant13.
The deficit in this functions occurred in all the 4-to-6-months age group children in this study. We noticed a relationship between hearing and sight21, because both work together in a child's normal development to provide information on the environment. However, the integration between hearing, visual and motor development suggests that hearing alteration contributes to motor underdevelopment in hearing-impaired children associated to the lack of opportunities in experiencing everyday activities, later insertion in school learning, among others22.
Knowing which are the most compromised domains in the development process allows us to ensure professional care in the three most important steps of assessment: diagnosis, intervention and evaluation of results, allowing information to be shared among all the professionals in the team 22.
CONCLUSION
The analysis of behavioural indicators in the Communication - Reception and Emission, Motor Aspects and Cognitive aspects of language domains made it possible for us to build up a profile of hearing-impaired children. In all age groups, we have found that hearing-impaired children have inferior development when compared with hearing children in the Communication-Emission domain. The later multidisciplinary interventions in the hearing-impaired child take place, the more severe will be his cognitive, motor and linguistic performance.
ACKNOWLEDGEMENTS
Sincere gratitude is extended to the following:
CAPES
Hearing-impaired person Centre (Centro do Deficiente Auditivo - CDA) - UNIFESP. Paulistinha School of education (Escola Paulistinha de Educação) - UNIFESP. Helen Keller Especial Municipal School (Escola Municipal de Educação Especial Helen Keller)
REFERENCES
1. Kandel ER. Uma visão global. In: Kandel ER, Schwartz JH, Jessel TM. Fundamentos da neurociência e do comportamento. Rio de Janeiro: Guanabara Koogan; 1997; p.505-6. [ Links ]
2. Soares AD, Chiari BM. Caracterização da narrativa oral de deficientes auditivos. Rev Soc Bras Fonoaudiol. 2006;11(4):272-8. [ Links ]
3. Costa MCM, Chiari BM. Verificação do desempenho de crianças deficientes auditivas oralizadas em teste de vocabulário. Pró-Fono R Atual Cient. 2006;18(2):189-96. DOI: http://dx.doi.org/10.1590/S0104-56872006000200008 [ Links ]
4. Chiari BM, Basilio CS, Nakagawa EA, Cormedi MA, Silva NSM, Cardoso RM, et al. Proposta de sistematização de dados da avaliação fonoaudiológica através da observação de comportamentos de criança de 0 a 6 anos. Pró-Fono R Atual Cient. 1991;3(2):29-36. [ Links ]
5. Sandri MA, Meneghetti SL, Gomes E. Perfil comunicativo de crianças entre 1 e 3 anos com desenvolvimento normal de linguagem. Rev CEFAC. 2009;11(1):34-41. DOI: http://dx.doi.org/10.1590/S1516-18462009000100006 [ Links ]
6. World Health Organization (WHO). Deafnes and Hearing loss. 2015. [Cited 2015 sep 02] Available from: http://www.who.int/mediacentre/factsheets/fs300/en/ [ Links ]
7. Schirmer CR, Fontoura DR, Nunes ML. Language and learning disorders. J Pediatr (Rio J). 2004;80(2 Suppl.0):S95-103. DOI: http://dx.doi.org/10.1590/S0021-75572004000300012 [ Links ]
8. Lyxell B, Wass M, Sahlén B, Samuelsson C, Asker-Arnason L, Ibertsson T, et al. Cognitive development, reading and prosodic skills in children with cochlear implants. Scand J Psychol. 2009;50(5):463-74. DOI: http://dx.doi.org/10.1111/j.1467-9450.2009.00754.x [ Links ]
9. Nikolopoulos TP, Vlastarakos PV. Treating options for deaf children. Early Hum Dev. 2010;86(11):669-74. DOI: http://dx.doi.org/10.1016/j.earlhumdev.2010.10.001 [ Links ]
10. Vohr B, Jodoin-Krauzyk J, Tucker R, Johnson MJ, Topol D, Ahlgren M. Early language outcomes of early-identified infants with permanent hearing loss at 12 to 16 months of age. Pediatrics. 2008;122(3):535-44. DOI: http://dx.doi.org/10.1542/peds.2007-2028 [ Links ]
11. Moeller MP, Hoover B, Putman C, Arbataitis K, Bohnenkamp G, Peterson B, et al. Vocalizations of infants with hearing loss compared with infants with normal hearing: Part I- phonetic development. Ear Hear. 2007;28(5):605-27. DOI: http://dx.doi.org/10.1097/AUD.0b013e31812564ab [ Links ]
12. Alzahrani M, Tabet P, Saliba I. Pediatric hearing loss: common causes,diagnosis and therapeutic approach. Minerva Pediatr. 2015;67(1):75-90. [ Links ]
13. Barnard JM, Fisher LM, Johnson KC, Eisenberg LS, Wang NY, Quittner AL, et al. A Prospective Longitudinal Study of U.S. Children Unable to Achieve Open-Set Speech Recognition 5 Years After Cochlear Implantation. Otol Neurotol. 2015;36(6):985-92. DOI: http://dx.doi.org/10.1097/MAO.0000000000000723 [ Links ]
14. Fortunato CAU, Bevilacqua MC, Costa MPR. Análise comparativa da linguagem oral de crianças ouvintes e surdas usuárias de implante coclear. Rev CEFAC. 2009;11(4):662-72. DOI: http://dx.doi.org/10.1590/S1516-18462009000800015 [ Links ]
15. Sarant JZ, Holt CM, Dowell RC, Rickards FW, Blamey PJ. Spoken language development in oral preschool children with permanent childhood deafness. J Deaf Stud Deaf Educ. 2009;14(2):205-17. DOI: http://dx.doi.org/10.1093/deafed/enn034 [ Links ]
16. McCann DC, Worsfold S, Law CM, Mullee M, Petrou S, Stevenson J, et al. Reading and communication skills after universal newborn screening for permanent childhood hearing impairment. Arch Dis Child. 2009;94(4):293-7. DOI: http://dx.doi.org/10.1136/adc.2008.151217 [ Links ]
17. Gândara JP, Befi-Lopes DM. Tendências da aquisição lexical em crianças em desenvolvimento normal e crianças com alterações específicas no desenvolvimento da linguagem. Rev Soc Bras Fonoaudiol. 2010;15(2):297-304. DOI: http://dx.doi.org/10.1590/S1516-80342010000200024 [ Links ]
18. Kane MO, Schopmeyer B, Mellon NK, Wang NY, Niparko JK. Prelinguistic communication and subsequent language acquisition in children with cochlear implants. Arch Otolaryngol Head Neck Surg. 2004;130(5):619-23. DOI: http://dx.doi.org/10.1001/archotol.130.5.619 [ Links ]
19. Sharma A, Gilley PM, Dorman MF, Baldwin R. Deprivation-induced cortical reorganization in children with cochlear implants. Int J Audiol. 2007;46(9):494-9. DOI: http://dx.doi.org/10.1080/14992020701524836 [ Links ]
20. Holzinger D, Fellinger J, Beitel C. Early onset of family centred intervention predicts language outcomes in children with hearing loss. Int J Pediatr Otorhinolaryngol. 2011;75(2):256-60. DOI: http://dx.doi.org/10.1016/j.ijporl.2010.11.011 [ Links ]
21. Wiegersma PH, Van der Velde A. Motor development of deaf children. J Child Psychol Psychiatry. 1983; 24(1): 103-11. [ Links ]
22. Yoon PJ. Hearing loss and cochlear implantation in children. Adv Pediatr. 2011;58(1):277-96. DOI: http://dx.doi.org/10.1016/j.yapd.2011.03.013 [ Links ]
Manuscript submitted: Oct 22 2015
Accepted for publication Dec 19 2015.
* Corresponding author: Érica Endo Amemiya - E-mail: erica_ea@yahoo.com.br


{kind=link}