










Services on Demand
article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Share

 Permalink
PermalinkJournal of Human Growth and Development
Print version ISSN 0104-1282On-line version ISSN 2175-3598
J. Hum. Growth Dev. vol.26 no.1 São Paulo 2016
http://dx.doi.org/10.7322/jhgd.113786
ORIGINAL RESEARCH
http://dx.doi.org/10.7322/jhgd.113786
The trauma from the perspective of caregives of juvenile victims of family violence
Maiara Pereira CunhaI, *; Lucienne Martins BorgesII
IDoutoranda em Psicologia pelo Programa de Pós Graduação em Psicologia pela Universidade Federal de Santa Catarina (UFSC)
IIProfessora do Programa de Pós Graduação em Psicologia pela Universidade Federal de Santa Catarina (UFSC)
ABSTRACT
INTRODUCTION: A child exposed to violent events may go on to develop mental health problems such as post-traumatic stress disorder (PTSD). One of the stressful events that can cause PTSD is family violence.
OBJECTIVES: To describe traumatic events, and to identify the frequency of PSTD and the symptoms in juvenile victims of violence from the perspective of their mothers and caregivers.
METHODS: The Affective Disorders and Schizophrenia for School Aged-Children Present and Lifetime Version (K-SADS-PL) clinical interview was used with the caregivers and children and semi-structured interviews were conducted only with the caregivers. The data from the K-SADS-PL clinical interview were organised in Microsoft Excel. For the analysis of the semi-structured interview data, Atlas/Ti 5.0 software was used.
RESULTS: In total, 20 subjects participated, including 10 children between six and twelve years of age and 10 caregivers. The family composition that predominated was blended and the type of violence was psychological. Of the 10 children who participated in the survey, three were diagnosed with PTSD and four of them showed symptoms, but did not meet all the diagnostic criteria for the disorder. The most common traumatic events experienced by the children were physical abuse, witnessing domestic violence and experiencing trauma. It was found in the semi-structured interviews that trauma, from the perspective of the caregivers, was caused by losses and violence to which the children were exposed.
CONCLUSION: These findings suggest that it is urgent to think of strategies to prevent violence and to perform additional research on PTSD and violence in mental health services
Keywords: family violence, childhood, post-traumatic stress disorder.
INTRODUCTION
Childhood is a period marked by motor, cognitive, affective and social development. The child, in turn, should be able to invest their energy in games and learning, free from the worries of the adult world. However, this is not always possible, since complications, such as family violence, can plague this phase and leave an indelible mark. It is worth mentioning that the developing child is in constant interaction with the environment and has moments of advances, transitions and regressions1. In the period of transition, it is possible that the child may be exposed to risky situations and, depending on the individual and contextual characteristics, present with mental health disorders, such as post-traumatic stress disorder (PTSD).
PTSD is characterised by the American Psychiatric Association (APA)2 as a clinical case belonging to the category of trauma-related disorders and stressors. The person must have been exposed to an extreme traumatic event, i.e. either witnessed or experienced the event. The event may have occurred with a relative or close friend, and may be revived persistently in one or more situations through memories, thoughts, perceptions and/or dreams. When exposed to something that refers to aspects of the traumatic situation, the person can act as if the traumatic situation is occurring again, accompanied by psychological suffering and/or a physiological reaction.
In addition to the symptoms described above, the person constantly dodges stimuli that refer to the event, which may lead to general numbness or increased excitability that were not present before the trauma. The symptoms need to be present for more than one month, and the subject must demonstrate suffering in their occupational and social spheres, as indicated by the DSM2. The disturbance does not occur due to physiological effects arising from for example, medicines, alcohol, or other medical conditions.
One of the events that can cause PTSD is violence. Violence is defined as intentional use of physical force or power against a person or a group, and the consequences of that relationship may include death, harm, deprivation and/or psychological suffering3. Violence committed against children and adolescents in Brazil is monitored by the Grievances and Notifications Information System (GNIS/SISAN). In 2011, it was found that female children were the most affected by violence, and the main place where this occurred was in the victim's residence. With respect to the type of violence, it was found that 40.5% of cases experienced physical violence, 20% sexual violence, 17% psychological violence and 16% negligence4.
In Brazil, the prevalence of PTSD in childhood is approximately 6.5%, and at that frequency, psychological and social damage will affect both the victims and their families2. In this sense, Cunha and Malik-Borges5 indicated the importance of professionals sensitised to the problem of PTSD, as well as making support and psychological care available soon after the traumatic event or the appearance of the first symptoms, in addition to being able to perform proper diagnostics.
Thus, the objective of this study was to describe the traumatic events, identify the frequency of PTSD and symptoms found in children who are victims of violence from the perspective of mothers and stepmothers.
METHODS
The present research, of an exploratory and transverse nature, with predominantly qualitative measures, was carried out at the Psychosocial Attention Centre for the Child (PACC/CAPSi) which, since 2000, assists children who present with psychological problems.
A total of 20 participants took part in this research: 10 mothers or guardians and 10 children between six and twelve years of age. Participants were selected according to the following inclusion criteria: (1) had entered the children's mental health service between 2010 and 2013; (2) a minimum of six and maximum of twelve years of age to join the children's mental health service; (3) have been victims of some kind of family violence, whether it be physical, psychological, sexual and/or neglect, at least one month after the event; (4) attended the children's mental health service at the time of the study and (5) the parents or guardians have knowledge of the traumatic event experienced by the child. It is worth noting that the criterion relating to age is based on the Statute of the Child and Adolescent, in which a child is any person up to twelve years of age6. Favourable opinion: on 301,464.
Data collection instruments
Depending on the goals, a semi-structured interview was applied in order to access information and offer to mothers or stepmothers a chance to talk about the situations experienced by the children, on the basis of the following questions: a) to discuss the traumatic event experienced by the child; and b) to check if there had been modifications to the behaviour of the child.
To investigate the symptoms of PTSD, the clinical interview Affective Disorders and Schizophrenia for School-Aged Children Present and Lifetime Version (K-SADS-PL) was used with their mothers or guardians and with the children. The K-SADS-PL was drafted by Kaufman et al.7. Is a clinical interview that should be carried out with the parents or guardians and/or with children. Based on the diagnostic criteria of DSM-III/R (1987) and DSM-IV (1994), it seeks to identify disorders in childhood and adolescence. In Brazil, Bordin and Brasil8 validated the instrument. The authors translated the English version into Portuguese (back-translation), assessed its content validity, construct validity and convergence. In addition, the reliability between evaluators and the test-retest score were evaluated in a sample of 78 children and their respective guardians who sought care at a mental health clinic for children.
In the application of this test in a clinical interview, it must be completed; this means that even is the researcher has interest only in the section corresponding to PTSD, the full test that investigates all the abovementioned disorders must be done. With respect to the section on PTSD, it consists of structured questions, which can be shown to the respondent to read them, or the researcher can interpret the question in their own words. In cases of the presence of symptoms of PTSD in the current diagnostic, the information must be entered as a current episode (CE). Otherwise, if there is a history of symptoms, but the participants have not experienced them for at least two months, the information will refer to a more serious episode that occurred in the past (MSEP). At the end of the instrument, and on the basis of the responses, it will be up to the researcher to assess the criteria in the DSM-IV (1994) regarding evidence of PTSD in children.
Analysis of the data
The interviews were fully transcribed and organised with Atlas/Ti 5.0 software, which enabled the construction of the analysis categories9. To calculate the frequencies and percentages of the K-SADS-PL clinical interview, the descriptive analysis of the data was performed in Microsoft Excel.
RESULTS AND DISCUSSIONS
Participants' characteristics
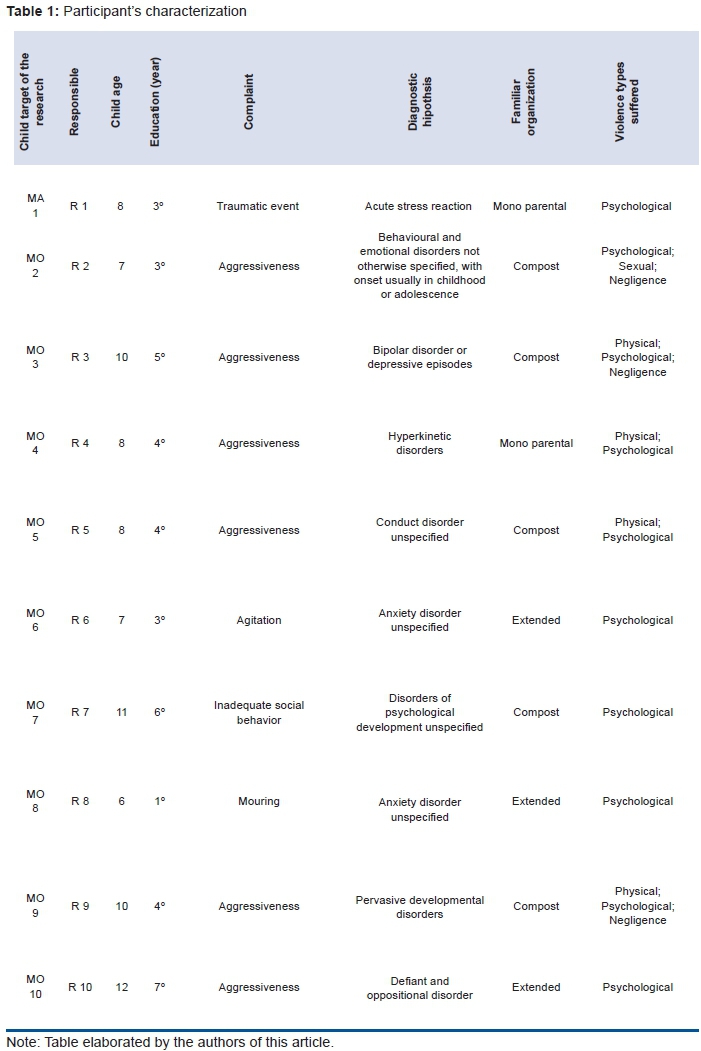
Table 1 presents the demographic information of the participants, such as age, education, the complaint that prompted the referral of the child to the service, diagnostic hypothesis upon admission of the child into mental health care, family composition and the type of violence suffered. (Table 1).
In Table 1, the complaint is the reason why the child was transferred to the service, while the traumatic event refers to situations where the child's routine was affected by exposure to scenes of physical and psychological violence between the father and the mother, accompanied by intense fear and horror on the part of the child. Aggressiveness includes verbal and physical aggression directed toward peers (other children) and authority figures (parents and teachers). The agitation category relates to certain behaviours, both motor and verbal. The complaint agitation refers to intense verbal and motor behaviours. The complaint inappropriate social behaviour is related to situations in which the child lies and steals objects. The complaint mourning is related to the loss of a significant person to the child. Finally, the complaint withdrawn behaviour refers to children who are timid or socially isolated at school.
The diagnostic hypothesis of this study was recorded according to the ICD-1010, which is the classification used in the records of the service. With respect to the diagnostic hypothesis, four participants arrived at reception with indications of emotional and behavioural disorders with onset usually occurring in childhood and adolescence. The most common disorders observed were anxiety or mood disorders. The same occurred in a study by Hoffmann, Saints and Mota11 which looked at the records of seven CAPSi sites, including emotional and behavioural disorders with onset usually occurring in childhood and adolescence; these disorders were observed in 44.5% (n = 648) of users. Delvan et al.12, published in 2010 the characterisation of the user profile and noted that 146 users were referred as a result of mental health problems, such as learning disorders, aggression, problems in relationships, or additional conditions that could be the focus of clinical attention.
In view of the predominance of males, Delfini, Dombi-Barbosa, Fonseca Tavares and Reis13 investigated 63 Records Centres (CAPSi) in the greater São Paulo and found that 25.4% (n = 16) of boys had emotional and behavioural disorders, with onset usually occurring in childhood and adolescence. In female subject, 27.5% (n = 11) of records did not include information on the diagnostic hypothesis.
According to Pedrini, Frizzo14, males often have outsourced behaviours, which are characterised by intrusive behaviours in the environment such as breaking the rules and aggressive behaviour. In turn, females tend to demonstrate internalised behaviours, i.e. behaviours linked to depression, withdrawal and anxiety. Thus, it was observed that the present research agrees with previous data on the male predominance in the mental health service. This information demonstrates that not only boys present distress, but also girls. However, as girls tend not to outsource their behaviour, they are taken less frequently to the mental health service. Boys, predominantly due to outsourced behaviours, are directed to mental health service more often than girls.
It is worth mentioning that information about the complaints and diagnostic hypotheses found in the CAPSi were obtained from the records of the interviews. Therefore, it is assumed that the diagnosis has been defined at the time the child began attending and, in many cases, lasted throughout the treatment period. According to Hoffmann et al.11, CAPSi tend to disregard comorbidities and possible changes in psychopathological cases, whose information records would be relevant.
The terminology used in the family composition was considered based on the document of the United Nations15 and mentions that a residence consisting of a single-parent family is composed of a parent, either the father or the mother, and their children. It is possible to have a home with extended family, where the nuclear family (parents and children) reside with other relatives such as grandparents, uncles, cousins, etc. Finally, a compound residence is characterised by the presence of a parent (father or mother), companion (stepmother or stepfather) and their respective children. It is noteworthy that, in this study, the family composition excelled with five participants.
Clinical Interview K-SADS-PL
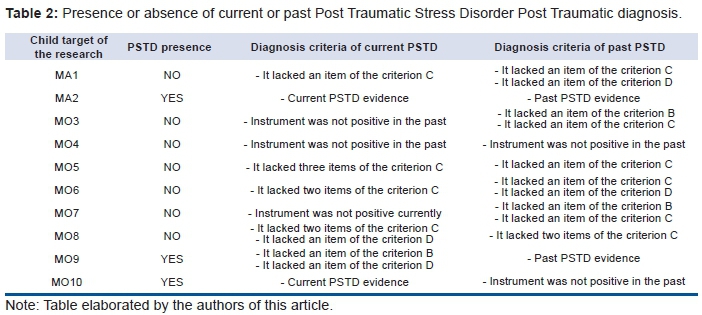
Table 2 was drafted with the aim to indicate the presence of the diagnosis and symptoms of PTSD in the participants. (Table 2).
In this study, 30% (n = 3) of participants showed evidence of current or past PTSD (MA2, MO9 and MO10). It is noteworthy that these participants also demonstrated the criteria of duration and suffering significant or functional impairment. With participants MO3 MO4, and MO7, the instrument was not positive for this determination. This indicates that, according to the clinical interview, the investigated traumatic events did not cause harm to these children. The same occurred in the past for MO4 and MO10. With the other participants, i.e. MA1, MO5, MO6 and M08, it was noted that they did not have all necessary diagnostic criteria for the presence of symptoms of criteria B (revival), C (persistent avoidance) and D (pronounced excitability).
Specifically with participants who have PTSD, a predominance of males was observed, with an average age of 9.6 years and average schooling of 4.6 years. The children were taken to the service with complaints of withdrawn behaviour (n = 2) and aggression (n = 1); two of them were exposed to three types of violence and one to one type of violence. With respect to the family composition, the most frequent type was compound, while the third participant was from an extended family. The data from this study corroborate with the information of Graham-Bermann et al.16 and Ximenes et al.17, who mentioned that the accumulation of traumatic situations acts like a facilitator factor for the development of PTSD. Regarding the familial setting, Poletto and Koller18 stated that the family can be understood as a risk factor and/or protection, depending on the quality of the relationship between those involved, as well as the communication between the members and the context in which it is located.
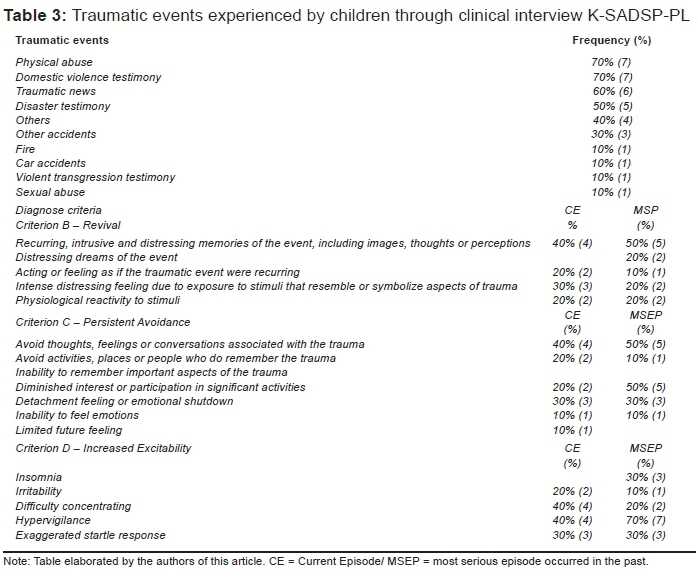
Table 3 presents the traumatic events and the symptoms most often experienced by the participants of this study. (Table 3).
Semi-structured interview
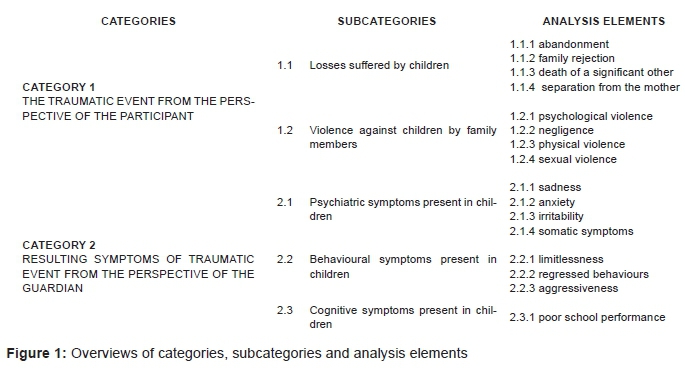
Figure 1 shows the categories and subcategories and the elements of analysis that informed the results and discussion of the data, which will be described. (Figure 1).
In category 1 - Traumatic event, from the perspective of the participant, it was sought to understand this category based on reports of events experienced by the children. To this end, two subcategories were analysed: losses suffered by children and violence against children by family members. In subcategory 1.1, losses suffered by children were identified on the basis of the perspective of mothers and stepmothers. In subcategory 1.1.1, abandonment was cited by four guardians as a traumatic event.
I abandoned everything when I met (referred to the name of the current companion) and did not look back. I grabbed my things and said goodbye (R3).
Based on the narratives, it was found that the traumatic event, from the perspective of the guardians, was related to abandonment. The life history of these children showed negligence throughout childhood that culminated in abandonment on the part of those responsible. It was concluded that the abandonment situation faced by children was linked to trauma, due to the presence of the element of surprise and despair, evidenced by MO9 and MO3.19
Another kind of loss, 1.1.2 family rejection, was reported by four participants:
My dad fights with my grandmother when I go there, because I am there. Over and over and over again he (referring to child) called me to talk: "Why doesn't Daddy like me? Did I do something to him? Why doesn't Daddy want to see me? Why doesn't he come to visit me? Why doesn't he come and get me? Why won't he talk to me when I go see Grandma?" It was so complicated. After that, his father didn't want contact with us, it's gone. There was a worse phase, because before there were fights they had their good moments, but from that moment on his father was gone. Finally, after we separated, his father went a long time without seeing him again." (R6).
Tinoco and Franco20 mentioned that successive losses, as alluded to by R6, tend to destabilise the emotional development of the child. In addition, an aggravation is the child not having someone who assumes their care and welcomes their questions and emotions. Despite these circumstances, MO6 possessed a support network that may have taken on a protective function. Thus, the impact of the traumatic event does not seem to have compromised the overall development of the child, as for example, proper school performance.
Yet, in the same subcategory, the analysis element 1.1.3: death of a significant other, was cited by three guardians:
MO7 cried a lot because of the death of his uncle who passed away. When he remembers, he cries, talks, but nowadays no longer speaks. I forgot how, but last year he remembered him enough. [...] When his uncle died, he was pretty scared. He is afraid to die. Because we took a scare at the time and MO7 witnessed that scare. I yelled a lot, my mother yelled a lot and I have not recovered. He was like a father to us (R7).
According to Franco and Mazorra21, the death of a significant person triggers a feeling of emotional and physical threat, which tends to mobilise the members of the family, as alluded to in the interview of R7. A family that experiences the impact of a loss usually presents difficulties in tackling this subject with children. Thus, the phase of development of the child, the type of death, the relationship of the family before and after the death, the way the family carried on after the death, i.e. whether the child was reassured about death and how it happens, become difficult or facilitators of mourning.
With regard to the traumatic event, in this case the death of a relative, Freud22 mentions that, for children, death does not bring the same feelings and values that are observed in adults. In a way, this infers that the impact of death on children is more connected to the way the family behaves before death rather than a direct experience with the same. Therefore, it is not the death of a loved one that characterises the traumatic event. The trauma observed here is related to psychological impacts, because of the suffering presented by family members and by changes in family dynamics.
Finally, one participant mentioned 1.1.4: separation from the mother
They (referring to the paternal grandmother and father of the child) went to the school and sought her (the child). I (mother of the child) walked out of the Forum in a state of shock. The bailiff cried of despair. I do not remember everything. I remember the pain that I felt, that I grabbed her (referring to the daughter). I then hurt him (referring to the bailiff), and ended up with scratch marks from my daughter on my shoulder (R2).
In this case, the child lived with her mother, but for judicial enforcement due to the dispute between the parents, the child went to live with relatives in a different city. Therefore, she changed to a new school and had to adapt to new family members. The traumatic event in this excerpt is in the separation of mother and daughter, and the deprivation of a mother. Even returning to living with the mother, the child showed fear and horror with the possibility of being removed again. This example shows one of the criteria of PTSD, which is to live constantly with the feeling that the traumatic situation is about to happen again.
Subcategory 1.2 violence against children by family members describes the types of family violence to which the children were exposed, including psychological violence, neglect, physical violence and sexual violence. Seven participants made reference to 1.2.1: psychological violence
Had once when I won it (MO4's sister) and my mother (MO4), he I remember to this day that he (referring to the child's stepfather) grabbed me by the neck and said he was going to kill me. Then I started throwing up and he rubbed my face on the floor in the room and my mother (MO4) saw it. MO4 talked to many people about this (R4).
According to the Ministry of Health3, psychological violence includes acts of humiliation, depreciation and ridicule, as noted in the quote of R4, in that the child's mother is sentenced to death and undervalued by his companion. Even with R4, it was observed that the child was exposed to violence since his stepfather had assaulted his wife. In this case, the child was exposed directly and indirectly to violence. Durant et al.23, indicate that the suffering of the mother can have an impact on the children.
In the same subcategory, three participants reported 1.2.2: negligence
She (referring to the paternal grandmother) took my daughter to go out at night (referring to night parties). [...] R2 got pneumonia because her grandmother put her in sandals and a dress for a walk on the Boardwalk [...] (R2).
In the narrative of R2, negligence was characterised by the fact that the child be exposed to unsuitable situations for their age and development. This is aligned with Martins and Jorge24 who showed that the practices of neglect are often related to female figures.
The next element of analysis, 1.2.3: physical violence, was cited by three participants:
When he was little and still wet his pants, his father got angry and filled his underwear with worms and after that, did he wear underwear. MO5 cried a lot, a lot, and was forever afraid of putting on underwear [...] Once, MO5 did mess of child, and his father beat him using a strap with such force that he was full of brands of girdled (R5).
The quote of R5 shows that physical violence was characterised by the use of physical force, which involved hitting with straps and slippers. The narratives of the participants agree with Martins and Jorge24 and Waiselfisz4, who showed that the predominant type of family violence is physical violence.
The last element of the analysis subcategory violence, 1.2.4: sexual violence, appeared once:
…when her grandmother went out to work, the uncle called her to go to the bathroom and asked her to examine his penis, claiming that he was hurt. Her grandmother bought a nurse kit for her to play with the uncle, then she also played with the uncle's penis (R2).
In the case of R2, in addition to sexual violence, the child was exposed to neglect and psychological violence. As pointed out by the literature referring to this issue, the presence of various types of violence of concomitant form tends to be frequent, which can increase the vulnerability to PTSD.
With category 1, it appears that the narratives showed trauma through losses and the violence to which children were exposed and that led to psychological suffering. With regard to losses, it is assumed that the traumatic event is related to the breach of a significant link to the child. In the case of death, there seems to be a particularity, because the loss is not related to the loved one who died, but to the family structure. In relation to the subcategory violence, a predominance of psychological violence was observed, which to some extent contradicts the literature. This shows how the actions and behaviours of the participants are perceived as violence and many are transmitted among generations. With category 1, the inter actuation of the types of violence and the presence of the traumatic event from the perspective of the participants was verified.
Category 2 - Symptoms resulting from the traumatic event from the perspective of the guardian investigated symptoms resulting from exposure to traumatic events, through the following sub-categories: psychological symptoms present in children, behavioural symptoms present in children, and cognitive symptoms present in children.
Subcategory 2.1 - psychological symptoms in children was mentioned, based on the participants' narratives. Five guardians alluded to subcategory 2.1.2: sorrow:
In the past she (referring to daughter) cried like….how can I tell you…a sentimental child, I couldn't say anything to her because she would cry. And now, it is a cry of sadness. I noticed that we see her crying in sorrow, due to something that she feels, that hurts her, something you know, is different [...] (R1)
Note that R1 asserts that the present crying is due to sorrow, and therefore is different from previous situations. This is aligned with a study by Gava, Silva and Dell'Aglio25 which, after searching expert reports on children who were victims of violence, found that these children experienced the symptoms of depression, including sadness, a depressed mood and crying.
Four participants reported 2.1.2: anxiety:
The change that I perceived was a fear of dying, he (the child) had that trauma, a fear of dying. Every time, he thought he was going to die. I stayed with that and he did too. Do you understand me? (R7).
In the quote from R7, one senses the presence of symptoms of PTSD, as recurrent, intrusive and afflictive remembrances of the event, including images, thoughts or perceptions, due to reports of an intense fear of dying. The impact of the traumatic event in the mother can also impair the child.
Three guardians cited 2.2.3: irritability:
That is what I said to you (referring to the teacher), he became more agitated, [...], more rude, because he automatically isolated the family he had, he says no one is related to me. Do you understand? (R10).
Lopez-Soler et al.26, observed that children exposed to violence demonstrate aggressiveness, showing hostile behaviours, irritability as well as difficulties and inadequate control of aggressive strategies. Therefore, it is understandable that irritability can arise as a symptom to communicate situations of profound dissatisfaction. In the case of MO10, after obtaining knowledge of its biological origin, the child went on to express excitement and frustration with more intensity.
The last analysis element of the psychological symptoms subcategory, 2.1.4: somatic symptoms, was referred to by two participants:
I had already made some previous queries with the doctor about six months ago. There were some medical tests, and she had the same symptoms (chest pain, shortness of breath and pain in the belly). Then the doctor told me to do all the tests, and asked me to return. Then I returned and she said there was nothing in the tests. Six months later, I came back and said she was feeling the same symptoms. Then she said to me, her mother: there is nothing, there is nothing (R1).
As illustrated by R1, after traumatic events, children can present with somatic symptoms, such as chest pain, shortness of breath and pain in the belly. As pointed out by Marcelli and Cohen27, traumatic events can trigger anxiety, causing discomfort that can often be manifested in the body by means of somatic symptoms. The above reports are in line with the research of Kugler, Bloom, Kaercher, Truax and Storch28, who noted the presence of somatic symptoms in children who were victims of family violence.
With the subcategory 2.2 - Behavioural symptoms in children - participants reported the main behavioural symptoms.
Family have cited the analysis 2.2.1 lack of limits:
[...] behaving in a while here, this thing of not having limits, and does not respect anyone, not the teacher, or Grandma, or the mother, or the aunt, or anyone and will be very rude towards them, always wanting to have the last word, even if you don't have anything else to discuss and call you that, silly! (R6).
According to Maercelli and Cohen27, frustration intolerance is often characterised by the difficulty of the child in discerning the boundaries between the outside world and the inner world28. As well as irritability, the lack of limits seems to indicate vulnerability in relation to the outside world, a world that appears as an element that frustrates and threatens.
Two participants cited 2.2.2: regressed behaviours:
She (child) returned there, sucking, bedwetting, afraid of the dark, drinking from a bottle, she was not my girl (crying) (R2).
Regressed behaviours are seen as behaviours inconsistent with the developmental stage and the age of the child and which had already been acquired and integrated into previous steps of its development, as shown by R2. As pointed out by Graham-Bermann et al.16, children exposed to family violence tend to have regressed behaviours, which in turn interfere in the child's development.
One participant referred to 2.2.3: aggression
(Child's name) came to (mental health service) because he was aggressive with two children in high school. He hit two children. He said he would hit by anything, he said he wanted. Complicated! (R3).
The above narrative shows the difficulty of MO3 in dealing with conflict at school, which led to physical aggression. It is assumed that the violence experienced by MO3 at home has been reproduced in the school environment.
In the case of the aggressive acts presented here, they seem to denote a line of communication from bitter frustration. A child or an adult who does not work on their frustrations will express them through aggressive gestures, according to Martins-Borges et al.29.
In subcategory 2.3 - cognitive symptoms in children, two guardians cited 2.3.1: poor performance in school
[...] The Director said to me: MO4 has failed this year. He got a 2, he got 0. He refuses to do the activities. I (the child's mother) mentioned this to the psychiatrist last time [...] (R4).
Based on R4, difficulties related to the teaching-learning process as well as cognitive symptoms point to the impact of family violence in the school context. These data are in line with Preto and Moreira30, who compared school averages between the children of victims and non-victims; the former showed poorer performance in school. In addition, when the mothers of the children were exposed to physical and psychological violence, the children of victims demonstrated difficulties in the teaching-learning process.
In general, after traumatic events, children/participants showed various symptoms, which had an impact on their integral development. Such symptoms were not restricted to psychological manifestations, but also left a mark on behaviour and the learning process as elucidated by the participants.
It was found that the 10 children who participated in the research came to the services because of aggressiveness. At the time of the survey, the children lived mostly with their families. The most common type of violence mentioned in their reports and in the reports of their guardians was psychological.
In view of the objectives of this article, the most frequent traumatic events are physical abuse, witnessing domestic violence, traumatic news and hearing about a disaster. This last event is a regional feature given the history of flooding, because the region is recurrently devastated by floods. Regarding the identification of the frequency of post-traumatic stress disorder, 30% of the participants demonstrated all of the diagnostic criteria of PTSD.
Considering the symptoms, other children showed other symptoms and signs of suffering. With regard to symptoms that appeared often, criterion B - revival - appeared in 50% of cases in the past, with recurrent, intrusive remembrances of a grievous event, including images, thoughts and perceptions. In turn, criterion C - persistent avoidance - predominated. Avoiding thoughts, feelings or conversations associated with the trauma and decreased interest or participation in important activities, both with 50% for the past. With respect to criterion D - increased excitability - 70% of participants demonstrated the symptom of hypervigilance in the past.
Thus, it was found that, in addition to diagnosis, the situations of violence and the losses to which children were exposed also left marks. This infers that suffering was expressed by the participants of this research in different ways, both through the body, expressed in relationships that were controversial or even aggressive, and also affecting cognition and the learning process, as shown in reports of the participants of this research.
The semi-structured interview technique, essential to give voice to participants, allowed access to traumatic events - in the form of losses and violence - according to the perspective of those responsible. The reported losses were dropouts, rejection, death of a loved one and separation. Violence consisted of psychological violence, neglect, physical violence and sexual violence. It should be noted that the data of the interview dialogue was combined with the findings of the K-SADS-PL clinical interview.
After exposure to these traumatic events, the children presented psychological symptoms, cognitive and behavioural. Sadness, anxiety, irritability and somatic symptoms were named and psychological symptoms expressed by children or reported by their responsible. To characterise the behavioural symptoms, participants mentioned a lack of boundaries, regressive conduct and aggressiveness. The only cognitive symptom listed by participants was poor school performance.
With respect to the limitations of this study, it should be noted that the definition of childhood was made according to the Statute of the Child and Adolescent; the chronological age established for children differs from the criteria used by the United Nations.
REFERENCES
1. Marinho-Araujo CM. A ciência do desenvolvimento humano: para além de uma Psicologia do Desenvolvimento. Psicol Esc Educ. 2006;10(1):135-6. DOI: http://dx.doi.org/10.1590/S1413-85572006000100013 [ Links ]
2. Associação de Psiquiatria Americana (APA). Manual diagnóstico e estatístico de transtornos mentais: DSM-5. Porto Alegre: Artmed; 2014. [ Links ]
3. Brasil. Ministério da Saúde. Violência intrafamiliar: orientações para a prática em serviço. Brasília: MS; 2002. [cited 2015 Aug 12] Available from: http://bvsms.saude.gov.br/bvs/publicacoes/cd05_19.pdf. [ Links ]
4. Waiselfisz JJ. Atendimento por violências no SUS. In: Waiselfisz JJ. Mapa da violência 2012: crianças e adolescentes do Brasil. Rio de Janeiro: FLACSO Brasil; 2012; p.62-73. [ Links ]
5. Cunha MP, Martins-Borges L. Transtorno de estresse pós-traumático (TEPT) na infância e adolescência e sua relação com a violência familiar. Bol Acad Paulista Psicol. 2013;33(85):312-29. [ Links ]
6. Brasil. Estatuto da Criança e do Adolescente: Lei 8.069/90, de 13 de Julho de 1990. Brasília: Senado Federal; 1990. [ Links ]
7. Kaufman J, Birmaher B, Brent D, Rao U, Flynn C, Moreci P, et al. Schedule for Affective Disorders and Schizophrenia for School-Aged Children Present and Lifetime Version (K-SADS-PL): initial reliability and validity data. J Am Acad Child Adolesc Psychiatry. 1997;36(7):980-8. DOI: http://dx.doi.org/10.1097/00004583-199707000-00021 [ Links ]
8. Brasil HH, Bordin AI. Convergent validity of K-SADS-PL by comparison with CBCL in a Portuguese speaking outpatient population. BMC Psychiatry. 2010;10:83. DOI: http://dx.doi.org/10.1186/1471-244X-10-83 [ Links ]
9. Cantero DSM. Teoría fundamentada y Atlas.ti: recursos metodológicos para la investigación educativa. REDIE. 2014;16(1):104-22. [ Links ]
10. Organização Mundial da Saúde (OMS). Classificação de transtornos mentais e de comportamento da CID-10: descrições clínicas e diretrizes diagnósticas. Porto Alegre: Artmed; 1993. [ Links ]
11. Hoffmann MCCL, Santos ND, Mota ELA. Caracterização dos usuários e dos serviços prestados por Centros de Atenção Psicossocial infantil-juvenil. Cad Saúde Pública. 2008;24(3):633-42. DOI: http://dx.doi.org/10.1590/S0102-311X2008000300017 [ Links ]
12. Delvan JS, Portes JRM, Cunha MP, Menezes M, Legal EJ. Crianças que utilizam os serviços de saúde mental: caracterização da população em uma cidade do Sul do Brasil. Rev Bras Desenvolvimento Hum. 2010;20(2):228-37. [ Links ]
13. Delfini PSS, Dombi-Barbosa C, Fonseca FL, Tavares CM, Reis AOA. Perfil dos usuários de um centro de atenção psicossocial infanto-juvenil da grande São Paulo, Brasil. Rev Bras Desenvolvimento Hum. 2009;19(2):226-36. [ Links ]
14. Pedrini JR, Frizzo GB. Avaliação de indicadores de problemas de comportamento infantil relatados por pais e professores. Aletheia. 2010;(33):223-33. [ Links ]
15. Organização das Nações Unidas (ONU). Principles and recommendations for population and housing censuses. New York: United Nations; 2008. [ Links ]
16. Graham-Bermann SA, Castor LE, Miller LE, Howell KH. The impact of intimate partner violence and additional traumatic events on trauma symptoms and PTSD in preschool-aged children. J Trauma Stress. 2012;25(4):393-400. DOI: http://dx.doi.org/10.1002/jts.21724 [ Links ]
17. Ximenes LF, Oliveira RVC, Assis SG. Violência e transtorno de estresse pós traumático na infância. Ciênc Saúde Coletiva. 2009;14(2):417-33. DOI: tp://dx.doi.org/10.1590/S1413-81232009000200011 [ Links ]
18. Poletto M, Koller SH. Contextos ecológicos: promotores de resiliência, fatores de risco e de proteção. Estud Psicol. 2008;25(3):405-16. DOI: http://dx.doi.org/10.1590/S0103-166X2008000300009 [ Links ]
19. Meshulam-Werebe D, Andrade MGO, Delouya D. Transtorno de estresse pós-traumático: o enfoque psicanalítico. Rev Bras Psiquiatr. 2003;25(Suppl. 1):37-40. DOI: http://dx.doi.org/10.1590/S1516-44462003000500009 [ Links ]
20. Tinoco V, Franco MHP. O luto em instituições de abrigamento de crianças. Estud Psicol. 2011;28(4):427-34. DOI: http://dx.doi.org/10.1590/S0103-166X2011000400003 [ Links ]
21. Franco MHP, Mazorra L. Criança e luto: vivências fantasmáticas diante da morte do genitor. Estud Psicol. 2007;24(4):503-11. DOI: http://dx.doi.org/10.1590/S0103-166X2007000400009 [ Links ]
22. Freud S. Luto e melancolia. In: Freud S. Introdução ao narcisismo, ensaios e metapsicologia e outros textos. São Paulo: Companhia das letras; 1917; p.171-194. [ Links ]
23. Durant JG, Schraiber LB, França-Junior I, Barros C. Repercussão da exposição à violência por parceiro íntimo no comportamento dos filhos. Rev Saúde Pública. 2011;45(2):355-64. DOI: http://dx.doi.org/10.1590/S0034-89102011005000004 [ Links ]
24. Martins CBG, Jorge MHPM. Violência física contra menores de 15 anos: estudo epidemiológico em cidade do sul do Brasil. Rev Bras Epidemiol. 2009;12(3):325-37. DOI: http://dx.doi.org/10.1590/S1415-790X2009000300004 [ Links ]
25. Gava LL, Silva DG, Dell'Aglio DD. Sintomas e quadros psicopatológicos identificados nas perícias em situações de abuso sexual infanto- juvenil. Psico. 2013; 44(2): 235-44. [ Links ]
26. López-Soler C, Fernández MV, Prieto M, Alcántara MPMV, Castro M, López-Pina JA. Prevalencia de las alteraciones emocionales en una muestra de menores maltratados. Anales Psicol. 2012;28(3):780-788. DOI: http://dx.doi.org/10.6018/analesps.28.3.140441 [ Links ]
27. Marcelli D, Cohen D. Os transtornos de ansiedade, os sintomas e a organização de aparência neurótica. (Murad, Fátima. Trad.). In: Marcelli D. Manual de psicopatologia da infância de Ajuriaguerra. Porto Alegre: Artmed; 2010; p. 298-332. [ Links ]
28. Kugler BB, Bloom M, Kaercher LB, Truax TV, Storch EA. Somatic symptoms in traumatized children and adolescents. Child Psychiatry Hum Dev. 2012;43(5): 661-73. DOI: http://dx.doi.org/10.1007/s10578-012-0289-y [ Links ]
29. Martins-Borges L, Mayorca DS, Livramento MS. Atendimento psicológico em situações de violência conjugal. In: MC Zurba. Psicologia e Saúde Coletiva. Florianópolis: Tribo da Ilha; 2011; p. ;157-168. [ Links ]
30. Preto M, Moreira PAS. Autoregulação da aprendizagem em crianças e adolescentes filhos de vítimas de violência doméstica contra mulheres. Psicol Reflex Crít. 2012;25(4):730-7. DOI: http://dx.doi.org/10.1590/S0102-79722012000400012 [ Links ]
Manuscript submitted: Jan 28 2016
Accepted for publication Feb 21 2016.
* Corresponding author: Maria Pereira Cunha - Email: maiara_pereira@yahoo.com.br


{kind=link}
{kind=link}
{kind=link}
{kind=link}