










Serviços Personalizados
artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282versão On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.26 no.2 São Paulo 2016
http://dx.doi.org/10.7322/jhgd.119262
ORIGINAL RESEARCH
Psychomotor development screening of children from kindergarten units of Belém, Pará, Brazil
Talitha Buenaño França GuerreiroI; Lília Iêda Chaves CavalcanteI; Elson Ferreira CostaI; Mário Diego Rocha ValenteII
ILaboratório de Ecologia do desenvolvimento, Universidade Federal do Pará, Belém, PA - Brasil
IIDepartamento de Trânsito do Estado do Pará
ABSTRACT
INTRODUCTION: Child development is considered a sequence of changes in behaviour and underlying processes that are influenced by biological and environmental factors. The screening and monitoring of neuropsychomotor development (NPMD) procedures have been shown to be effective in the early identification of different diseases in childhood.
OBJECTIVE: relate the condition of the NPMD in children aged 36-48 months attending Early Childhood Education Units (ECEU) in Belém, Pará, Brazil to certain personal characteristics and variables of their ecological environment.
METHODS: The following instruments were applied: Questionnaire of the biopsychosocial characteristics of the child, the Instrument for Measuring Urban Poverty Level, and finally, Developmental Screening Denver II Test.
RESULT: The study revealed that of the 319 children evaluated, 77.74% had probable delays in development. The variables that were statistically significant were paternal education (0.000**), the child's primary caregiver (0.039*) and pregnancy planning (0.007*). Regarding the instrument of measurement for the level of urban poverty, the scores ranged from 28 to 52 points, and showed a statistically significant relation with the outcome (0.003)*
CONCLUSION: The high prevalence of probable developmental delays seen in children of the city's ECEU showed the need to introduce early stimulation programs, encouraging the monitoring of child development through the screening, and, in addition, to alert for the issue of negative interference of socioeconomic factors related to family condition and city they reside in on child growth and development.
Key words: child development, Denver II test, level of urban poverty.
INTRODUCTION
Child development is a complex term that comprises definitions originated in several areas, such as paediatrics, physiotherapy and psychology. The most recent studies emphasize development as a process of change and permanence, demonstrating that the acquisition and use of skills integrate various systems and functions of the individual in constant interaction with the physical and social environment.1-6
There are many factors that influence the child's health and development, which may be related to heredity and biological adaptation, in addition to environmental conditions (experience and sensory-motor stimulation, nutrition, socioeconomic conditions, affective disorders). The impact of these factors on child development has been the subject of many studies in recent decades, pointing out that identification and early intervention are key to the prognosis of children with development disorders.7-9
It is important to note that the assessment of the child's development seems inefficient when it is based only on clinical impressions. Less than 30% of children with mental retardation, language disorders or other developmental problems had such situations detected by the clinical trial.7-10 With the purpose of promoting some form of early intervention for the so-called deviations of development, the use of standardized instruments have been indicated and recommended by experts and institutions2-6 since it enables the action of anticipatory recommendations to parents, caregivers and professionals.
In this sense, several studies have investigated the impact of socio-economic and environmental conditions, lifestyle and health conditions on child development. In Brazil, until the present, are rare population-based studies about social inequalities in the development of children and the risk factors for late, functional limitations and disabilities2.7 -11. In the North, such studies are rarer still, not to say no. Faced with this situation, the need for more studies that can recognize the influence of the ecological aspects in populations, beyond the urgency of producing greater understanding around the Northern Brazilian population, is still little discussed in this regard.
Thus, the objective of this study is to relate the neuropsychomotor development of children with personal characteristics and their eco-environmental variables.
METHODS
This is a exploratory and descriptive cross-sectional study, with a quantitative approach of the data held in the city of Belém, Pará, Brazil. A total of 319 children participated in the study, with inclusion criteria being children of both sexes, aged 36 to 48 months, that degree early childhood education units (ECEU) linked to the City Department of education, of city of Belém. Children that presented disorders affecting expression of speech, sensory changes, auditory and/or visual and sequelae of central nervous system involvement were excluded.
For sample size calculation, a conglomerate sampling procedure was used. The margin of error of the sample calculation was within 5% and the confidence level represented 95%. In this sense, as the population of the study consisted of 1201 individuals, the ideal sample size was established with 300 subjects. However, a percentage of 7% of subjects was added in anticipation of possible losses, which totalled 320.
ECEU involved in the research were distributed proportionally by the eight administrative districts by drawing lots, depending on the number of existing education institutions in each of them, as well as the number of children evaluated in each district.
To register the information of each child, a Biopsychosocial Features Questionnaire for Children (BFQC) consisting of 48 questions was applied, addressing the following categories: identification, pre, peri and postnatal history and socioeconomic and environmental conditions. The questionnaires were answered after the Free and Enlightened consent form was signed by the persons responsible. The research was approved as CAAE 05177512.5.0000.5172 Protocol.
With regard to the socioeconomic condition of the families of the children participating in the study, we used an instrument of measurement in order to determine the level of urban poverty (LUP). This instrument allowed us to take a range of analysis for elements of socioeconomic condition descriptors of poor urban populations, with the goal of generating a measure capable of calculating its variability, but not limited to the family income. The instrument is composed of 13 items,with each item's score on a scale ranging from zero to four, and the sum obtained in each one of these items establishing the urban poverty level of the family.12
To evaluate the development, was used the Denver Developmental Screening Test II - DDST II.6,13 In general, the Denver II Test consists of 125 items, arranged in four dimensions: a) personal/social, b) thin/adaptive motor function, c) language and d) gross motor function; features good reliability indexes, with 0.99 inter-observer and 0.9 in test re-test. The validity of the test is based on its standardization and not on its correlation with other tests, once all the other consist of slightly different way of working14. The test also stands out as one of the most widely used instruments in Brazilian research10-11 and stands out as the most globally applied test.2,3,6 After the assessment, were classified in the test with the development: Normal, when the child did not present any kind of delay or at most one item of caution; and were considered indicative of suspected cases of delay in development when indicated two or more items of caution or one or more items.
The team of BFQC data collection was composed by the researcher responsible for the study and two students of the Master Post Graduation in Theory and Research of Behaviour program - (MPGTRB). It comprised one student of physiotherapy, one of social service and five more of occupational therapy. The whole team was previously qualified for the application of BFQC and MPGTRB researchers were trained on the basis of the previously established methodology in its DDST II manual. Once the test required active cooperation of the child, every effort was made to gain their confidence and stimulate their participation by, for example, asking to the teachers to introduce the researchers to the child earlier and stay a while to adapt and to the child to feel more comfortable.
The program Statistical Package for the Social Sciences (SPSS) was used to analyze the data. Initially, a frequency distribution analysis of several variables was used, and we then conducted a comparative study between the variables and the condition of suspected delay in development, using the Chi-square test for this analysis. All analyses were considered significant when p values < 0.05.
RESULTS
The sample totalled 319 children: 141 female and 178 male. Most children lived in families that receive from 1 to 3 minimum wages, with the parents' having primary responsibility for the income and given that more than half of them received some social benefit, usually in the form of financial assistance paid by the Programa Bolsa Família (PBF). Regarding the characteristics of the parents, most were married and own a home. In general, the mothers were within the age range of 20 years, with 12 years or more of study, performing some sort of regular job, while among the parents, men were predominately age 30 years or more, with 9 to 11 years of study, and performing informal job. In the sample, it was observed that 65.83% of families lived in homes with three or more rooms, inhabited by two to five residents (74.92%). It was pointed out that slightly over half of families inhabited masonry houses (59.56%), with a significant percentage of people residing in households of mixed wood. With regard to housing conditions, most of the family homes featured running water (86.62%), with its own bathroom (79.94%), regular electric power connection (80.25%) and regular garbage collection (97.5%).
It was observed that a large part of the population studied was not born of a planned pregnancy, with this characteristic representing 70.53% of the total group. However, prenatal care was successfully accomplished by 96.23% of women. In the aspect of gestational age there was a predominance of children born to term (87.47%), with 12.53% of children born pre-term. As regards to the type of childbirth, most children were born by caesarean delivery (53.92%). In relation to the consumption of substances, most mothers mentioned that they did not consume any substance (alcohol, tobacco, abortion drug) during pregnancy (86.2%).
Among families evaluated, 87 were classified within the poverty level (27.27%), 132 families in low level lower (41.38%), and over 100 families in the low level higher (31.35%), as shown in the graph in Figure 1. The calculated average stood at 44 points and sets of 45 points, with a standard deviation of 4.54 points.

Table 1 shows the results of the DDST II scores of children in the study. It is observed that 77.74% presented a suspected developmental delay and only 22.26% presented a score compatible with the status of normality.
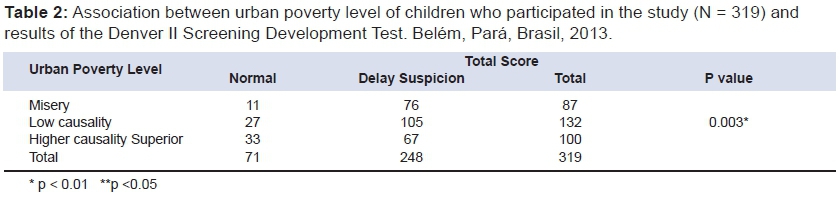
The results indicated a significant correlation (p 0.003*) between poverty level and the developmental condition of children, as can be seen in Table 2. The following variables showed significant association with suspected delay in NPMD in bivariate analysis: paternal schooling (0.000**), primary caregiver of the child (0.039*), planning of pregnancy (0.007*) (Table 3).
DISCUSSION
Analysis of the results showed that a significant part proportion of the three-year-olds showed results indicative of a suspected delay in this population. However, in this study, the percentage of children who presented with this condition proved to be superior when compared to those who represent this condition in the population, according to under file screens made in the country over the last 15 years.
Among Brazilian studies that used a similar research procedure and presented results that most closely match those reported in this study is one that was conducted by Caon and Ries14 that pointed out the existence of 86.2% of children with questionable performance; that is, with suspected delays in development. In this sense, it calls attention to the fact that the results obtained in this study differ from most Brazilian studies done thus far to assess the development of children through the DDST II.2-3 In some Brazilian research studies,7,10 approximately 40% to 46% of children presented development that was assessed as at risk and/or suspected of delay, but most research reveals a percentage close to the 20% range.19-20
Among possible explanations for this variation could be the particular characteristics of the study population in Belém, Pará, Brazil. In this study, the selection of the sample involved children belonging to public and municipal services networks, which are generally comprised of children from lower-income families and living in unfavourable socio-economic conditions; therefore, presumably, these children are under the effects of poverty, which brings with it limitations to insuring their proper development. According to information collected by the coordinators of the ECEU visited throughout the research, there is an extensive waiting list for schoolchildren, as well as a wait period of effectuation of registration. Faced with the impossibility of ECEU meeting this growing demand, a selection of children is usually made at the beginning of the year to fill the vacancies.
These children are selected by teachers from information gathered based on visits made to the home where they live with their responsible. From what was discovered, the ECEU uses the degree of social vulnerability presented by their families as a criterion for the selection of children for admission, which includes consideration of socioeconomic factors (especially the income of the primary caregivers) and other situations that tend to increase the chance of being exposed to any form of violence or negligence (use of alcohol and other drugs, history of mental disorder, etc.).
Teachers and coordinators of the ECEU admit that families with very low incomes generally have a higher likelihood of neglecting basic care in terms of the health and education of their children, since they have several layers of difficulty, such as offering proper nutrition in the first three years of a child's life, this being a condition of vulnerability that should receive priority treatment and be met by the institution whenever possible. From this perspective, the more precarious the conditions of family health and the environment in which the child lives (e.g., with the absence of basic sanitation and/or drinking water), the more the child may be exposed to disease, and higher should be the priority given by ECEU in order to include socially. Likewise, other indicators of social vulnerability of the children's families are usually considered by ECEU coordination at the time of student selection, such as parental involvement with illegal substances, family violence, and parents or family members serving time in seclusion.
The school can and should work as a positive and proactive factor in the protection and promotion of child development. However, access to services maintained by the early childhood education policy in these areas can be given from the preference given to families with a higher level of social risk, seems to be seen as a measure of protection important, it is not possible, however, because of the limits placed by the objectives of this study, check how much staying in the school environment has represented or may represent for children new stimuli and opportunities for growth and learning at the end of the childhood.
According to the child protection legislation, in exceptional situations registration in an ECEU is achieved through an explicit request made by juvenile services with operations in the region. An example of this situation is the case of a child evaluated in the study: the child was apparently healthy, but could barely speak, having shown up on all aspects of development evaluated by DSDT II, although these were not identified as evidence of physical or mental limitations or disabilities. The child in question was attending ECEU a few months prior the evaluation, having been referred at the time of research by child protective services. There was information indicating that the child spent the rest of the day in the company of his mother (who has a mental illness), wandering the streets and circulating around town, aiming to sell candy and other goodies.
It is also important to highlight how much is still unknown about the development of children living off the country's East, where axis was held most studies using DDST II.21,22 It is assumed that environmental conditions in which children are being raised in other regions, such as northern Brazil, can be more damaging to child development due to social and regional inequalities which the country features historically. According to Issler and Giugliani,12 children, because of their vulnerability, are the ones suffering the damaging effects of poverty and lack of education. This position is shared by other authors.23,24,25
In developing countries many children, their parents and caregivers are victims of social inequalities that limit access to basic goods and services that are essential to survival and social learning.19 In the present study, the level of poverty of households showed a statistically significant association to the outcomes achieved among children who live and study in different administrative districts of Belém, corroborating the findings of other investigations that have applied the DDST II. Such studies demonstrate that there is an association between socioeconomic level predictors' variables of family and child development milestones.5,6,24,25
The poverty level may cause the child to present serious health problems, including those associated with delays in neuropsychomotor development, as they are subject to less stimulation and increased exposure to risk factors. One can therefore assume that there is evidence that children of low socioeconomic status tend to be continuously exposed to multiple adverse factors, thereby constituting a major risk group for delays in development. It is also important to mention that not all studies that explore the relationship between social class and child development have used the same indicators to mark this specific condition; some use family income as the principal - or, sometimes the only - predictor.
In the present study, family income is not a strong risk factor for developing classified as suspect of delay. Other studies have also shown this result.11,23 Such a finding can be justified by the fact that the sample introduced relatively homogeneous income levels, with 65% of the families showing gains of 1 to 3 minimum wages.
In any case, in descriptive terms, it is clear that the condition of low income is a feature that is presented not only as predominant in the population studied. This data is important because, historically, the economic factor has been associated with (and even limited to) the income of individuals, families and populations to an extent that says a lot about the level of access to basic goods and services for the promotion of development (e.g., food, housing and sanitation).1, 4, 5, 24.25
Child development studies highlight that monthly family income produces an effect on the quality of the conditions that impact directly on the neuropsychomotor development of the child, such as feeding and basic attention to maternal and child health.1,24 Therefore, deficiencies in this variable result in unfavourable situations within the framework of the child's health care, in the ecological conditions created by their environment and living conditions and their education in more general terms. These factors can negatively influence biopsychosocial development, thereby raising the chances of presenting some kind of shortfall or delay in their neuropsychomotor development.
One study evaluated two cohorts of children with 12 months of age using the DDST II. In the first cohort, the poorest children showed twice as many flaws in the screening test Denver II as compared to those whose families had higher incomes. According to the author, the comparison between the results obtained in 2004 and those obtained in 1993 shows a tendency toward a reduction in the percentage of children with a suspected developmental delay. For example, it should be noted that there has been a reduction of around 29% in situations where children of wealthier families were deemed to be at risk for developmental delay, while among poor households the prevalence fell to 36% (p < 0.05). However, the study also showed that when the relative risk among poorer and richer children was calculated, this perspective has decreased only slightly (from 1.6 to 1.4), indicating a relatively stable effect of family income on the condition in the 11 years separating the two cohorts.19
Among the correlations between the variables analysed and the outcome, an association between schooling and a suspected delay in development was identified. The literature shows strong evidence that the higher the educational level of the parents, the lower the chance that the child presented suspected delay in developing.19.25 Parents with higher education generally have a more accurate perception of the needs of their children and are more likely to be able to promote the development expected in given age group, performing stimuli and proper care for the acquisition of domain coarse and fine motor skills, as well as language and social-personal development.
The type of occupation of the father was also statistically correlated with a suspected developmental delay. This result may be in accordance with the hypothesis that the higher the level of schooling the better the father's job may be, thereby promoting greater opportunities and stimuli for the development of the child. Therefore, while the education of the mother acts as a protective factor for the development of the child, the father's education may also have a similar effect.24
In the present study, maternal schooling showed no association with the condition of the NPMD, a finding observed in other work.26 Studies have shown that the level of maternal education involves a situation of vulnerability for children in early childhood, revealing an important association between this variable and development delays.17,19,25
In fact, the educational level of the parents is a predictive factor of development, since the length of time studying is closely related to cognitive skills that parents use to stimulate their children. It is understood that the educational level of the parents increases the chances of their children's schooling, conditions the practices of care and the ecological environment in which the child lives, thereby expanding physical and sociocultural experiences for these children, encouraging their best overall development.
In this study, the variable "primary caregiver" showed a significant association with respect to the development of the child. Neuropsychomotor development in children invariably takes place in a context that is subject to interference from different factors that are considered by the experts as positive or negative, as far as they play a decisive role on the processes of maturation and learning of the child. Among these, the mother/child or caregiver/child relationship may be mentioned.1,23
Therefore, consensus is the importance of mother-child interaction for the cognitive and motor development of the child and the mother, in general, who can play with relative ease the subtle signs of children and respond appropriately to them, being that children who has less time with her mother showed a higher frequency of static balance deficit when compared to those who remained longer with this caregiver, suggesting that maternal presence can act as a protective factor for acquisition of such motor skill1,23.
In this study, in relation to the sex of the children, it was possible to perceive that there was no significant difference regarding the overall result of the DDST II. Approximate results were also recorded in previous studies that used the same instrument.19-21 However, similar studies have found sex interference in the performance of children submitted to DDST II, demonstrating that there tends to be a correlation between the sex of the child and the variable that designates the outcome stated by evaluation of developmental areas.21 This fact can be linked to the expectations that society has today in relation to different skills/ways of being of boys and girls, as well as the fact they develop faster than they do with regard to physical maturity27.
CONCLUSION
In the sample, it was observed that the children showed a high prevalence of suspect performance late in development, when evaluated by the DDST II. The results build a frame that must be analysed with concern. It points to the need for the establishment of a surveillance system capable of detecting the development risk groups among children who attend the ECEU located in different administrative districts of the city of Belém, Pará, Brazil, and contribute to the formulation of effective measures for the prevention and correction of deficits and outstanding issues in the various areas of development.
This type of study and, therefore, the discussion of its main results, is a necessary and essential measure that aims to contribute to the systematic evaluation of public policies directed at the education and health of children in the town of Belém, Pará, Brazil and in other urban contexts. In addition, it supports and guides strategies for monitoring and surveillance programs in the development of a multidisciplinary team. It is recommended that new longitudinal studies be done using a larger sample, and that may involve children in other age groups, in order to obtain more consistent results and inconclusive in this respect to the understanding of the complex ecology of its development.
Other assessment tools can also be used to evaluate the ecological characteristics of environments such as the family and the ECEU, as well as to investigate conceptions of caregivers and care practices that are expected to influence the development of the child. It is understood that this is the condition required to propose interventions with more effective results in the field of health promotion and education in early childhood.
ACKNOWLEDGEMENTS
Thanks to Mariane Lopes for collaboration in data collection, as well as in the entire research.
REFERENCES
1. Bronfenbrenner U. Bioecologia do desenvolvimento humano - tornando os seres humanos mais humanos. Porto Alegre: Artmed; 2011. p. 127-193 [ Links ]
2. Sigolo ARL, Aiello ALR. Análise de instrumentos para triagem do desenvolvimento infantil. Paidéia 2011; 21(48): 51-60. DOI: http://dx.doi.org/10.1590/S0103-863X2011000100007. [ Links ]
3. Custódio ZAO, Crepaldi MA, Cruz RM. Desenvolvimento de Crianças Nascidas Pré-Termo Avaliado pelo Teste de Denver-II: Revisão da Produção Científica Brasileira. Psicol Reflex Crit. 2012; 25(2): 400-06. DOI: http://dx.doi.org/10.1590/S0102-79722012000200022 [ Links ]
4. Quansah E, Ohene LA, Norman L, Mireku MO, Karikari TK. Social Factors Influencing Child Health in Ghana. PLoS ONE 2016; 11(1). DOI: 10.1371/journal.pone.0145401. [ Links ]
5. Tampubolon G. Growing Up in Poverty, Growing Old in Infirmity: The Long Arm of Childhood Conditions in Great Britain. PLoS ONE 2015; 10 (12). DOI:10.1371/journal.pone.0144722 [ Links ]
6. Zeppone SC, Volpon LC, Del Ciampo LA. Monitoramento do desenvolvimento infantil realizado no Brasil. Rev Paul Pediatr. 2012; 30(4): 594-9. DOI: http://dx.doi.org/10.1590/S0103-05822012000400019 [ Links ]
7. Brito CML, VIEIRA GO, Costa COM, Oliveira NF. Desenvolvimento neuropsicomotor: o teste de Denver na triagem dos atrasos cognitivos e neuromotores de pré-escolares. Cad Saúde Pública (Rio J). 2011; 27(7):1403-14. DOI: http://dx.doi.org/10.1590/0102-311X00104814 [ Links ]
8. Dornelas LF, Duarte NMC, Magalhães LC. Atraso do desenvolvimento neuropsicomotor: mapa conceitual, definições, usos e limitações do termo. Rev Paul Pediatr. 2015; 33: 88-103. DOI: http://dx.doi.org/10.1016/j.rpped.2014.04.009 [ Links ]
9. Silva GK, Lamônica DAC. Desempenho de crianças com fenilcetonúria no Teste de Screening de Desenvolvimento Denver - II. Pro Fono. 2010; 22(1): 345-50. DOI: 10.1590/S0104-56872010000300031 [ Links ]
10. Braga AKP, Rodovalho JC, Formiga CK, Martins R. Evolução do crescimento e desenvolvimento neuropsicomotor de crianças pré-escolares de zero a dois anos do município de Goiânia(GO). Journal of Human Growth and Development 2011; 21(2): 230-239. DOI: http://dx.doi.org/10.1590/S0104-12822011000200006 [ Links ]
11. Souza SC, Leone C, Takano AO, Moratelli HB. Desenvolvimento de pré-escolares na educação infantil em Cuiabá, Mato Grosso, Brasil. Cad. Saúde Pública 2008; 24(8):1917-1926. DOI: http://dx.doi.org/10.1590/S0102-311X2008000800020 [ Links ]
12. Issler RMS, Giugliani ERJ. Identificação de grupos mais vulneráveis à desnutrição infantil pela medição do nível de pobreza. Jornal de Pediatria 1997; 73 (2): 101-105. [ Links ]
13. Frankenburg WK, Dodds J, Archer P, Shapiro H, Bresnick B. The Denver II: a major revision and restandardization of the Denver Developmental Screening Test. Pediatrics 1992; 89: 7-91. PubMed 1370185 [ Links ]
14. Caon G, Ries LGK. Suspeita de atraso no desenvolvimento neuropsicomotor em idade precoce: uma abordagem em creches públicas. Temas Sobre Desenvolvimento 2003; 12(70): 11-17. [ Links ]
15. Santos R, Araújo A, Porto MA. Early diagnosis of abnormal development of preterm new borns: assessment instruments. Jornal de pediatria 2008; 84 (Supl4): 289-299.DOI: http://dx.doi.org/10.1590/S0021-75572008000400003 [ Links ]
16. Rydz D, Srour M, Oskoui M, Marget N, Shiller M, Birnbaum R, Majnemer A, Shevell M. Screening for Developmental Delay in the Setting of a Community Pediatric Clinic: A Prospective Assessment of Parent-Report Questionnaires. Pediatrics 2006; 118(4), 1178-1186. DOI: http://dx.doi.org/10.1542/peds.2006-0466 [ Links ]
17. Hyo-yun Ga, MD, Kwon JY. A Comparison of the Korean-Ages and Stages Questionnaires and Denver Developmental Delay Screening Test. M.D.Ann Rehabil Med 2011; 35:369-374. DOI: 10.5535/arm.2011.35.3.369 [ Links ]
18. Ozmen A, Terlemez S, Tunaoglu FS, Soysal S, Pektas A, Cilsal E, Koca U, Kula S, Oguz AD. Evaluation of Neurodevelopment and Factors Affecting it in Children With Acyanotic Congenital Cardiac Disease. Iran J Pediatr. 2016; 26(1): 32-78. DOI: 10.5812/ijp.3278. [ Links ]
19. Halpern R, Barros AJD, Matijasevich A, Santos IS, Victora CG, Barros FC. Developmental status at age 12 months according to birth weight and family income: a comparison of two Brazilian birth cohorts. Cad. Saúde Pública 2008; 24(3): 444-450. DOI: http://dx.doi.org/10.1590/S0102-311X2008001500010 [ Links ]
20. Amaro LLM, Pinto SA, Morais RLS, Tolentino JÁ, Felício LR, Camargos ACR, et al. Child development: comparison between children who attend or do not attend public daycare centers. Journal of Human Growth and Development 2015; 25(2): 170-176. DOI: http://dx.doi.org/10.7322/jhgd.103002 [ Links ]
21. Biscegli TS, Polis LB, Santos LM, Vicentin M. Avaliação do estado nutricional e do desenvolvimento neuropsicomotor em crianças frequentadoras de creche. Rev. Paul. Pediatr. 2007; 25 (4): 337-342. DOI: http://dx.doi.org/10.1590/S0103-05822007000400007 [ Links ]
22. Sabatés AL, Mendes LCO. Perfil do crescimento e desenvolvimento de crianças entre 12 e 36 meses de idade que frequentam uma creche municipal da cidade de Guarulhos. Cienc Cuid Saude 2007; 6(2):164-170. DOI: http://dx.doi.org/10.4025/cienccuidsaude.v6i2.4143 [ Links ]
23. Amorim RCA, Laurentino GEC, Barros KMFT, Ferreira ALPR, Moura Filho AG, Raposo MCF. Programa de saúde da família: proposta para identificação de fatores de risco para o desenvolvimento neuropsicomotor. RevBrasFisioter. 2009; 13(6): 506-513. DOI: http://dx.doi.org/10.1590/S1413-35552009005000065 [ Links ]
24. Mengel MRSM, Linhares MBM (2007). Risk factors for infant developmental problems. Rev Latino-am Enfermagem 2007; 15 (número especial): 837-842. DOI: http://dx.doi.org/10.1590/S0104-11692007000700019 [ Links ]
25. Pasian MS, Bazon MR, Pasian SR, Lacharite C. Negligência infantil a partir do Child Neglect Index aplicado no Brasil. Psicol. Reflex. Crit. 2015; 28(1):106-115. DOI: http://dx.doi.org/10.1590/1678-7153.201528112. [ Links ]
26. Andraca I, Pino P, Parra AL, Rivera F, Castillo M. Factores de riesgo para el de-sarrollo psicomotor em lactantes nascidos em óptimas condiciones biológicas. Revista de Saúde Pública 1998; 32(2): 138-147. DOI: http://dx.doi.org/10.1590/S0034-89101998000200006 [ Links ]
27. Lejarraga H, Pascuccib MC, Krupitzkya S, Kelmanskyc D, Biancoc A, Martínezc E, Tibaldic F, Camerond N. Psychomotor development in Argentinean children aged 0-5 years. Pediatric and Perinatal Epidemiology 2002; 16: 47-60. DOI: 10.1046/j.1365-3016.2002.00388.x [ Links ]
Manuscript submitted: Mai 12 2016
Accepted for publication Jun 16 2016
Corresponding author: Lília Iêda Chaves Cavalcante. E-mail: liliaccavalcante@gmail.com


{kind=link}
{kind=link}
{kind=link}
{kind=link}