










Serviços Personalizados
artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282versão On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.27 no.1 São Paulo jan./abr. 2017
http://dx.doi.org/10.7322/jhgd.127652
ORIGINAL ARTICLE
Development of infants with a risk indicator for hearing loss associated to living enviroment
Desenvolvimento de lactentes com indicador de risco para deficiência auditiva e classificação ambiental
Danielle Mendonça Araujo; Natália Caroline Rovere; Maria Cecília Marconi Pinheiro Lima
Universidade Estadual de Campinas - UNICAMP - Rua Tarumã, 412 13098-341 Campinas, SP, Brasil. Departamento de Desenvolvimento Humano e Reabilitação da Universidade Estadual de Campinas
ABSTRACT
INTRODUCTION: Infants with a risk indicator of hearing loss (RIHL) are more likely to have delays in their development. Besides the biological risk, the infant's environment may determine the outcome of their development.
OBJECTIVE: To compare the motor, cognitive and language development of infants with and without RIHL and to know the affordances of the home environment of those infants.
METHODS: This was an observational research exploratory, cross-sectional and quantitative study, in which the development of 77 infants with RIHL (Study Group) were compared to 77 infants without RIHL (Compared Group). Cognition, language and motricity were evaluated according to the Bayley Scale of Infant Development, and the home environment according to the Affordability of the Home Environment for Motor Development - Baby Scale questionnaire.
RESULTS: The most frequent risk indicators were family history (25.6%) and hyperbilirubinaemia (24.4%). In the Study Group, 13 (16.8%) infants presented delays in at least one domain and in the Control Group 3 (3.9%) infants presented delays. There was a statistically significant difference in the motor (p = 0.0001), cognitive (p = 0.001) and language (p = 0.0304) domains, with a better score in the Control Group. Regarding the home environment, 70.2% of houses in the Study Group were classified as less than adequate or mildly adequate, while in the Control Group this was 50.7%.
CONCLUSION: The average development of the infants with risk indicators for hearing loss is below the average development of infants without them. Also, the number of environments below adequate is higher in the group with infants with risk indicators.
Keywords: infant development, risk factors, environment, hearing impairment, infants.
RESUMO
INTRODUÇÃO: Lactentes com indicadores de risco para deficiência auditiva (IRDA) têm maior probabilidade de apresentar atrasos do desenvolvimento. Além dos indicadores de risco biológicos, o ambiente em que o lactente está inserido pode determinar o desfecho do desenvolvimento infantil.
OBJETIVO: Comparar o desenvolvimento motor, cognitivo e de linguagem de lactentes com e sem indicadores de risco para deficiência auditiva e conhecer as affordances no ambiente domiciliar dos lactentes com e sem indicadores de risco.
MÉTODO: Pesquisa observacional exploratória, transversal e quantitativa, na qual o desenvolvimento de 77 lactentes com IRDA (GE- Grupo de Estudo) foi comparado ao de 77 lactentes sem os indicadores (GC- Grupo Comparado). Avaliou-se a cognição, linguagem e motricidade por meio das Escalas Bayley de Desenvolvimento Infantil e o ambiente domiciliar pelo questionário Affordances no Ambiente Domiciliar para o Desenvolvimento Motor - Escala Bebê.
RESULTADOS: Os indicadores de risco mais frequentes foram histórico familiar (25,6%) e hiperbilirrubinemia (24,4%). No GE, 13 (16,8%) dos lactentes apresentaram atrasos em pelo menos um domínio do desenvolvimento e no GC 3 lactentes (3,9%). Houve diferença estatisticamente significativa nos domínios motor (p = 0,0001), cognitivo (p = 0,001) e de linguagem (p = 0,0304), com melhor desempenho no GC. Quanto ao ambiente domiciliar, 70,2% dos domicílios do GE classificou-se em "Menos que o adequado" ou "Moderadamente adequado", enquanto no GC o valor foi de 50,7%.
CONCLUSÃO: O desenvolvimento médio dos lactentes com IRDA está abaixo comparado aos lactentes sem indicadores e o número de ambientes abaixo do esperado é maior no grupo de lactentes com IDRA
Palavras-chave: desenvolvimento infantil, fatores de risco, ambiente, deficiência auditiva, lactentes.
INTRODUCTION
Infants are considered to have risk indicators if there is the presence of biological and/or environmental conditions that increase the incidence of developmental delays or disorders. Even if conditions are unfavourable, it cannot be said that damage will occur, so child follow-up evaluations are necessary and can detect infants whose risk factors have caused delays in their development1.
Accompanying breastfeeding infants is part of the developmental surveillance approach, the concept of which reflects the complexity of the child's developmental process in the early years of life. The manual Child Development Monitoring in the Context of Integrated Management of Childhood Illness emphasizes the need to monitor the infant during the first two years of life, due to greater neuronal plasticity and better results in early interventions2.
With regard to sensory impairments, it is possible to identify neonates with risk indicators for hearing loss in the Universal Neonatal Hearing Screening (UNHS) process, since at the time of the test, the responsible is questioned about characteristic risk indicators during gestational and perinatal period. Babies having one or more risk indicators for hearing loss (RIHL) are referred to the auditory monitoring programmes in order to ensure that hearing loss and delays in language development are detected early3.
The Multiprofessional Committee on Auditory Health (MUCOAH) suggests that neonates with RIHL and with satisfactory results at the time of screening should undergo hearing monitoring by qualified professionals until the third year of age, usually speech-language pathologists conduct the monitoring, but since risk indicators are common to other domains of development (cognitive and motor) and auditory responses are expressed by motor behaviour, it is necessary to form interdisciplinary teams aimed at full monitoring of infants3.
Regarding the monitoring of child development and biological conditions, information about the environment in which the child is placed should be sought; this can influence and determine the outcome of the development of children4. Creating favourable environments is dependent on the quantity and quality of the available resources required to enable interactions between the child and other members of the family5.
Reviews of child development, involving cognitive domains, language and motor skills, are often performed with the use of the Bayley Scales of Infant Development, Third Edition (Bayley-III), considered a benchmark test for this purpose6. Regarding environmental factors influencing the infant's development, it is possible to assess these through the Affordances questionnaire in the Home Environment for Motor Development - Baby Scale (AHEMD-IS)7. According to Gibson8, the affordances (opportunities and events) are the possibilities offered by the environment to a particular agent and can be conducive to stimulating motor development.
Analysing the infant's development and its relation with biological indicators and the environment in which the subject is placed, is associated with the concept elaborated by Parker et al.9 entitled 'double risk'. According to the author and collaborators, children with risk factors, more susceptible to disease, are also those who suffer the consequences of living in adverse environmental conditions9. Therefore, it is necessary to monitor the development of infants with risk indicators and their surrounding environment.
The objective of this study was to compare the motor, cognitive and language development in infants with and without risk factors for hearing loss and to describe the affordances in their home environment.
METHODS
This was an observational research of an exploratory nature, with a cross-sectional design and a quantitative approach. In a total of 154 infants, aged between 8 and 10 months, 77 had at least one hearing impairment risk indicator (HIRI) (Study Group) and the other 77 had no risk indicators (Compared Group).
The risk indicators considered were: family history of deafness, hyperbilirubinaemia (no transfusion required), inbreeding, infectious diseases during pregnancy, use of ototoxic medications, neonatal asphyxia, use of drugs during pregnancy, infants followed by genetics and pregnant women with acquired immunodeficiency syndrome (HIV+) sectors. These indicators are pertinent to a population that is born in good health and does not require specific interventions or a stay in the intensive care unit.
The Study Group was composed of participants of a hearing-monitoring programme, who met the criteria of the survey and were invited to participate in the period from July 2014 to November 2015. The Compared Group was recruited by telephone contact with those responsible for infants who had undergone otoacoustic emissions testing at the same institution.
Infants who were born at the Neonatal Intensive Care Unit, who were born at a gestational age less than or equal to 35 weeks, and infants already enrolled in early stimulation programmes due to developmental delays, were excluded from the study.
The Research Ethics Committee of the State University of Campinas (UNICAMP), process number 637.421/2014, approved the project. All those responsible were informed about the study objectives as well as the methods adopted in the evaluations.
The instruments used were the diagnostic scales Bayley-III6 and the AHEMD-IS7 questionnaire. The diagnostic scale has five independent scales: cognition, language, motor, social-emotional and behavioural-adaptive, and can be used for children from zero to 42 months. This scale has frequently been used in the Brazilian population; despite not being translated from English to Portuguese it is adapted to the population, because it is a reference scale, making it possible to obtain detailed information about neurodevelopment10-12.
The beginning of the evaluation is associated with the child's age, according to the registration records. In the case of children born prematurely, the chronological age should be corrected. The average time for evaluation varies from between 25 and 40 minutes. When the child's response does not reflect his or her ability because they are crying or sleeping, the evaluation must be discontinued, returning as soon as the issue/discomfort has been resolved. The evaluation should be suspended when, even after the permitted pause, the crying, sleeping, or other discomforts are not resolved.
The score for each item of each category can be either one (1) or zero (0). A score of 1 (one) means that the child has fulfilled the requirements of the item according to established criteria. A score of 0 (zero) means the child did not comply with what was recommended by the item or did not perform it. Each independent scale is scored based on the sum of the tasks performed by the child, generating raw scores, which are then converted into different types of scores. According to the manual, in scientific research it is recommended that the scores are based on the norms for the age, such as the composite score, since it is from these scores that the psychometric measures are guaranteed. For the composite score, 100 is the mean score with a standard deviation of ± 15 points. It is also possible to classify the composite scores in bands: very high (above 130 points); high (between 129 and 120 points); above average (119-110 points); average (109-90); below average (89-80); borderline (79-70) and extremely low (69 or fewer points)6.
The AHEMD-IS questionnaire, created and validated in the United States and Brazil, is considered simple, effective and self-administered directed to those responsible for the evaluation of the affordances at home that favour motor development in children aged between 3 and 18 months7.
The questionnaire consists of an initial part concerning the child's information (name, gender, birth weight and the time in which the child attends day care) and family characteristics, such as the mother's and father's degree of education, and residence information: type of residence (apartment or house), the number of adults and children who live there, how long the family has lived in the place of residence and the number of existing rooms.7
There are 35 other questions divided into three dimensions: Physical Space of the residence; Variety of Stimulation; Toys for Fine Motricity and Toys for Gross Motricity. The session called 'Physical Space', aims to evaluate the presence of adequate space for the child to play and move freely, the type of surface or soil, the presence of furniture, inclined surfaces and steps. In the 'Variety of Stimulation' session, information is obtained about the child's routine, the presence of peers of his/her age, and whether parents encourage them in play. The third session is called 'Toys for Fine and Gross Motricity', and establishes the types and amount of toys that the child has, according to their description and function7.
The sum of the points obtained in the questions belonging to each of the subscales is known as the 'total score'. The scores of the subscales and the total score can be classified into: 'less than adequate', 'moderately appropriate', 'adequate' and 'excellent', thus quantifying the affordances present in the home environment for child development7.
Two researchers, the evaluator and an observer carried out the evaluations of the BAYLEY-III scales. Information was recorded when both agreed with the infant's response. During the evaluation, the infants should be in good general condition, with no signs of agitation or excessive discouragement beyond the usual, according to the report of the person in charge. Subsequent to the evaluation of the development of infants, the responders answered the AHEMD-IS questionnaire.
The population characterization was obtained by using the BAYLEY-III and AHEMD-IS questionnaire, the descriptive statistical method was used for the presentation, results were presented with mean, standard deviation, median and minimum and maximum values. The Mann-Whitney test was used to compare the development of the groups. Statistically significant differences were observed in all tests with values of 'p' less than 0.05.
RESULTS
A total of 154 infants were included in the study, subdivided into the study group (SG) and compared group (CG). The SG was composed of 77 infants, 38 (49.4%) female and 39 (50.6%) male. The CG was composed of 77 infants, 43 (55.8%) female and 34 (44.2%) male. The mean age corrected at the time of evaluation for the SG was 282.3 days (± 20) and for the CG it was 273.9 days (± 20). The mean maternal age was 25.9 (± 7.1) years for the SG and 27.5 (± 6.9) years for the CG.
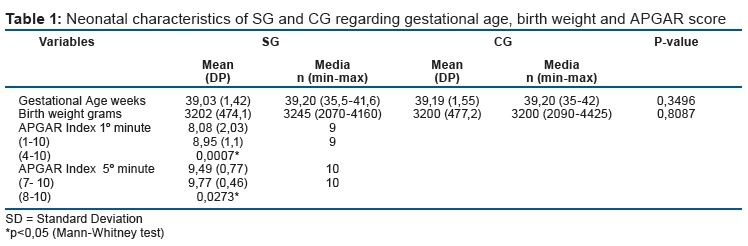
Table 1 shows the neonatal characterization of the sample, including information on gestational age, birth weight and APGAR score in the fifth minute of life. Regarding gestational age, 14 (9%) infants were classified as preterm, 9 (5.8%) of them were in the comparative group and 5 (3.24%) were in the study group. None of the preterm infants presented less than 35 weeks of gestational age. The APGAR score presented a statistically significant difference between the groups, the values were lower for the SG.
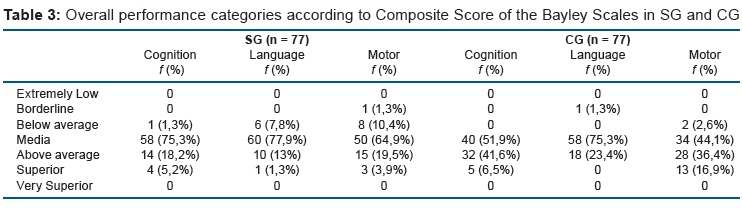
Table 3 shows the frequency in the classification of the BAYLEY-III Scales of the SG and CG groups. One infant from each group was classified as borderline: the child from the SG this classification applied to the motor scale and for the child from the CG it applied to the language scale. Other infants were below average in the SG compared to the CG. In the SG, 13 (16.8%) infants were under the expected rating, three of them were below average in more than one of the observed domains. Eight cases were below the mean: these comprised one on the borderline scale in the motor domain, six in the language domain and one in the cognition domain. In the CG, three (3.9%) infants were below the expected rating: two of these were below the mean in the motor domain and the other /the third was borderline in the language domain. There was a higher frequency of infants who were above average in the compared group.
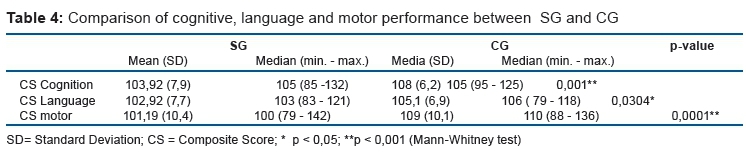
Table 4 presents a comparison of cognitive, language and motor performances using the composite score of the Bayley Scales. The results are expressed by the mean, standard deviation, median and maximum and minimum values of the scores. A statistically significant difference was observed in all evaluated domains, and the SG showed lower values than the CG.
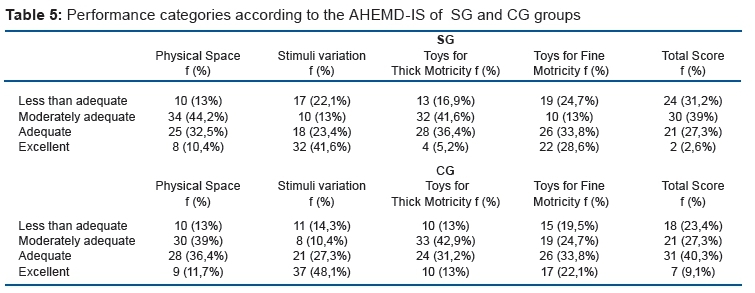
Table 5 shows the frequency of the classification of the environment according to the AHEMD-IS questionnaire. When comparing the groups for the AHEMD-IS scores there were no statistically significant differences in any of the categories proposed by the questionnaire. The total mean score of both groups was classified as moderately adequate, as well as physical space and toys for gross stimulation.
The variety of stimulation and the fine-motor toys were classified as suitable for both groups. In the SG, 23 (29.9%) of the households were adequate or excellent, while in the CG the total score was 38 (49.4%). Regarding the total number and percentage ratings in the AHEMD-ID the total score in 'less than adequate' and 'moderately appropriate' amounted to 54 (70.2%) affordances for SG and 39 (50.7%) affordances for the CG.
DISCUSSION
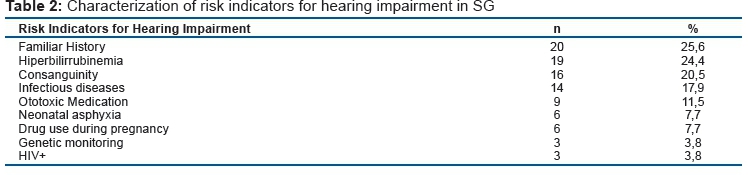
In the present study, 154 infants were evaluated. Regarding the risk indicators for progressive or late-onset hearing loss present in the SG, it was verified that the most prevalent indicator was a family history of hearing loss. In addition, it was observed that 16 (20.8%) infants had more than one risk indicator.
Tiensoli et al.13 identified the prevalence of hearing impairment in a public children's hospital in Belo Horizonte, Minas Gerais, Brazil. A total of 798 infants and newborns were evaluated, of whom 468 (25.6%) presented at least one indicator of risk for hearing loss. The most prevalent risk indicators of newborns were family history, represented by 25%, equal to that found in our study (25.6%)13. Another study conducted in a public hospital in São Paulo, Brazil, in 2009, found the percentage of neonates with risk indicators to be similar to those of Minas Gerais14. Unlike results found in the south-east, in which a survey conducted in a public hospital in Pernambuco, Brazil found the most prevalent indicator was hyperbilirubinaemia in 47% of infants who had undergone the UNHS programme15.
Ribeiro, Beltrame16, while evaluating the neuromotor and biopsychosocial characteristics of infants with biological risk historical, observed that these may have committed in relation to aspects of neuromotor development and underscore the importance of the monitoring of child development.
Table 3 shows that the majority of the participants demonstrated cognitive, motor and language development within the limits of normality. However, those below-average or borderline in the SG performance were higher than the 5% expected in normative samples in the three areas of the Bayley-III Scales,6 reaching 16.8%, represented by 13 subjects, three of whom had delays in more than one area of development. In the CG, three subjects were below average or borderline, which corresponds to 3.9%, which is within the range expected by the BAYLEY-III Development standardization.
Recent studies on the cognitive, language and motor development, especially in the population of premature infants born with low weight, agree that these factors pose risks for child development, especially in the first years of life17-21. Yet in addition to these factors, Saccani, Valentini22 emphasized the length of stay in the intensive care unit is inversely related to child development.
No studies have been found that assess the development in a comprehensive way for infants with RIHL; the presence of these indicators is still mainly related to language delays. Fernandes et al.17, in assessing infant language, found the most altered function at 12 months was the expressive one. It was also observed how the hearing and vision senses are primordial in the first year of life and the importance of the relation of these with oral language, since an association was revealed between the babies that presented transient alterations between 4 and 8 months of age and the delays in oral language at 12 months. It is noteworthy that in this study, out of the 20 cases that had alterations at 4 and 8 months, five continued to present delay at 12 months.
Similar results were observed in a group of infants at 12 and 24 months, considered as transient deviations, leading the team to realize the importance of orienting the family to the appropriate intervention, otherwise the alterations could become persistent. In meetings with the families, especially the mother, exchanges of information and experiences among parents and researchers always happened, which could have a positive effect on the relationship between the child and the family, promoting the development of the infants23.
In the present research, the total mean score of both groups was classified as moderately adequate, as was the physical space and toys for gross stimulation. The variety of stimulation and the fine-motor toys were classified as suitable for both groups.
It is shown that in the SG, 29.9% of households were considered adequate or excellent, while in the CG this value was 49.4%. When the AHEMD-IS total score was analysed, 70.12% (n = 108) of the participants scored up to 24 points, thus not reaching half of the possible total (49 points), and 27.3% (N = 42) scored up to 18 points, indicating very low values. Similar results were found in the studies of Defilipo et al.24 and Noble et al.25 who found the affordances of the assessed households to be insufficient.
This data acquires greater relevance in the SG, since they are infants with biological risk factors. According to Mancini et al.26, children exposed to biological and environmental risk factors are more likely to have developmental delays. Moreover, they state that children with biological risks tend to be more susceptible to the influence of unfavourable environments when compared to those without these factors27.
According to Halpern et al.28, delays in child development have multifactorial causes, as observed in this study, and it is still possible to check in developing countries that infants are often exposed to numerous causes and the mix up of those causes increases the likelihood of delays.
In conclusion, the comprehensive development of infants with risk indicators for hearing impairment is below the expected age range, when compared to infants without indicators. Environmental stimuli were insufficient in most residences, indicating restricted opportunities for children's motor development.
REFERENCES
1. Almeida CGM, Salgado MH, Rodrigues OMPR. Diferenças no desenvolvimento de meninos e meninas em condições de risco. Bol Psicol. 2012;62(136):1-14. [ Links ]
2. Almeida AC, Mendes LC, Sad IR, Ramos EG, Fonseca VM, Peixoto MVM. Use of a monitoring tool for growth and development in Brazilian children-systematic review. Rev Paul Pediatr. 2016;34(1):122-31. DOI: http://dx.doi.org/10.1016/j.rppede.2015.12.002 [ Links ]
3. Lewis DR, Marone SAM, Mendes BCA, Cruz OLM, Nóbrega M. Comitê multiprofissional em saúde auditiva: COMUSA. Braz J Otorhinolaryngol. 2010; 76(1):121-8. DOI: http://dx.doi.org/10.1590/S1808-86942010000100020 [ Links ]
4. Gabbard C, Caçola P, Rodrigues LP. A New Inventory for Assessing Affordances in the Home Environment for Motor Development (AHEMD-SR). Early Child Educ J. 2008;36(1):5-9. [ Links ]
5. Freitas TCB, Gabbard C, Caçola P, Montebelo MIL, Santos DCC. Family socioeconomic status and the provision of motor affordances in the home. Braz J Phys Ther. 2013;17(4):319-27. DOI: http://dx.doi.org/10.1590/S1413-35552013005000096 [ Links ]
6. Bayley N. Screening Test of Bayley Scales of Infant and Toddler Development-III San Antonio: Pearson; 2006. [ Links ]
7. Caçola PM, Gabbard C, Montebelo MIL, Santos DCC. The new affordances in the home environment for motor development - infant scale (AHEMD-IS): Versions in English and Portuguese languages. Braz J Phys Ther 2015;19(6):507-25. DOI: http://dx.doi.org/10.1590/bjpt-rbf.2014.0112 [ Links ]
8. Gibson JJ. The ecological approach to visual perception. New York: Pshychology Press; 1986. [ Links ]
9. Parker S, Greer S, Zuckermann B. Double jeopardy: the impact of poverty on early child development. Pediatr Clin North Am. 1988;35(6):1227-40. DOI: http://dx.doi.org/10.1016/S0031-3955(16)36580-4 [ Links ]
10. Baltieri L, Santos DCC, Gibim NC, Souza CT, Batistela ACT, Tolocka RE. Desempenho motor de lactentes frequentadores de berçários em creches públicas. Rev Paul Pediatr. 2010;28(3):283-9. DOI: http://dx.doi.org/10.1590/S0103-05822010000300005 [ Links ]
11. Fernandes LV, Goulart AL, Santos AMND, Barros MCDM, Guerra CC, Kopelman BI. Avaliação do neurodesenvolvimento de prematuros de muito baixo peso ao nascer entre 18 e 24 meses de idade corrigida pelas escalas Bayley III. J Pediatr. 2012;88(6): 471-8. DOI: http://dx.doi.org/10.1590/S0021-75572012000600005 [ Links ]
12. Souza CT, Santos DCC, Tolocka RE, Baltieri L, Gibim NC, Habechian FAP. Avaliação do desempenho motor global e em habilidades motoras axiais e apendiculares de lactentes frequentadores de creche. Rev Bras Fisioter. 2010;14(4):309-15. DOI: http://dx.doi.org/10.1590/S1413-35552010000400007 [ Links ]
13. Tiensoli LO, Goulart LMHF, Resende LM, Colosimo EA. Triagem auditiva em hospital público de Belo Horizonte, Minas Gerais, Brasil: deficiência auditiva e seus fatores de risco em neonatos e lactentes. Cad Saúde Pública. 2007;23(6):1431-41. DOI: http://dx.doi.org/10.1590/S0102-311X2007000600018 [ Links ]
14. Amado BCT, Almeida EOC, Berni PS. Prevalência de indicadores de risco para surdez em neonatos em uma maternidade paulista. Rev CEFAC. 2009;11(Supl.1):18-23. DOI: http://dx.doi.org/10.1590/S1516-18462009005000020 [ Links ]
15. Barbosa CP, Menezes DC, Curado NRPV, Silveira AK, Teixeira DA. Indicadores de risco para perda auditiva em neonatos e lactentes atendidos em um programa de triagem auditiva neonatal. Rev CEFAC. 2011;13(2). DOI: http://dx.doi.org/10.1590/S1516-18462010005000071 [ Links ]
16. Ribeiro J, Beltrame TS. Características neuromotoras e biopsicossocias de lactentes com histórico de risco biológico. Fisioter Mov. 2010;23(1):25-34. DOI: http://dx.doi.org/10.1590/S0103-51502010000100003 [ Links ]
17. Fernandes LV, Goulart AL, Santos AM, Barros MC, Guerra CC, Kopelman BI. Neurodevelopmental assessment of very low birth weight preterm infants at corrected age of 18-24 months by Bayley III scales. J Pediatr (Rio J). 2012;88(6):471-8. DOI: http://dx.doi.org/10.2223/JPED.2230 [ Links ]
18. Anderson PJ, De Luca CR, Hutchinson E, Roberts G, Doyle LW; Victorian Infant Collaborative Group. Underestimation of developmental delay by the new Bayley-III Scale. Arch Pediatr Adolesc Med. 2010;164(4):352-6. DOI: http://dx.doi.org/10.1001/archpediatrics.2010.20 [ Links ]
19. Formiga CKMR, Vieira MEB, Linhares MBM. Developmental assessment of infants born preterm: comparison between the chronological and corrected ages. J Hum Growth Dev. 2015;25(2):230-6. DOI: http://dx.doi.org/10.7322/jhgd.103020 [ Links ]
20. Zerbeto AB, Cortelo FM, Élio Filho BC. Association between gestational age and birth weight on the language development of Brazilian children: a systematic review. J Pediatr. 2015;91(4):326-32. DOI: http://dx.doi.org/10.1016/j.jped.2014.11.003 [ Links ]
21. Spittle AJ, Spencer-Smith MM, Eeles AL, Lee KJ, Lorefice LE, Anderson PJ, et al. Does the Bayley-III Motor Scale at 2 years predict motor outcome at 4 years in very preterm children? Dev Med Child Neurol. 2013;55(5):448-52. DOI: http://dx.doi.org/10.1111/dmcn.12049 [ Links ]
22. Saccani R, Valentini NC. Desenvolvimento motor de crianças de 0 a 18 meses de idade: um estudo transversal. Pediatr Mod. 2012;48(2):57-64. [ Links ]
23. Buschmann A, Jooss B, Rupp A, Dockter S, Blaschtikowitz H, Heggen I, et al. Children with developmental language delay at 24 months of age: results of a diagnostic work‐up. Dev Med Child Neurol. 2008;50(3):223-9. DOI: http://dx.doi.org/10.1111/j.1469-8749.2008.02034.x [ Links ]
24. Defilipo EC, Frônio JS, Teixeira MT, Leite IC, Bastos RR, Vieira MT, et al. Opportunities in the home environment for motor development. Rev Saude Publica. 2012;46(4):633-41. DOI: http://dx.doi.org/10.1590/S0034-89102012005000040 [ Links ]
25. Nobre FSS, Costa CLA, Oliveira DL, Cabral DA, Nobre GC, Caçola P. Análise das oportunidades para o desenvolvimento motor (affordances) em ambientes domésticos no Ceará- Brasil. Rev Bras Crescimento Desenvol Hum. 2009;19(1):9-18. DOI: http://dx.doi.org/10.7322/jhgd.19898 [ Links ]
26. Mancini MC, Paixão ML, Silva TT, Magalhães LC, Barbosa VM. Comparação das habilidades motoras de crianças prematuras e crianças nascidas a termo. Rev Fisioter Univ. 2000;7(1/2):25-31. DOI: http://dx.doi.org/10.1590/fpusp.v7i1-2.79362 [ Links ]
27. Abbott AL, Bartlett DJ, Fanning JEK, Kramer J. Infant motor development and aspects of the home environment. Pediatr Phys Ther. 2000;12(2):62-7. DOI: http://dx.doi.org/10.1097/00001577-200012020-00003 [ Links ]
28. Halpern R, Giugliani ER, Victora CG, Barros FC, Horta BL. Risk factors for suspicion of developmental delays at 12 months of age. J Pediatr (Rio J). 2000;76(6):421-8. [ Links ]
 Correspondence:
Correspondence:
maraujo.danielle@gmail.com
Manuscript submitted in 2016
Accepted for publication in Sep 2016
Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - CAPES. Processo nº 01P - 4347/2015


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}