










Services on Demand
article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Share

 Permalink
PermalinkJournal of Human Growth and Development
Print version ISSN 0104-1282On-line version ISSN 2175-3598
J. Hum. Growth Dev. vol.27 no.1 São Paulo Jan./Apr. 2017
http://dx.doi.org/10.7322/jhgd.119236
ORIGINAL ARTICLE
Abdominal obesity: prevalence,sociodemographic and lifestyle-associated factors in adolescents
Obesidade abdominal: prevalência, fatores sociodemográficos e de estilo de vida associados em adolescentes
William R. TebarI, II; Luiz Carlos M. VanderleiIII; Catarina C. ScarabotolloII; Edner F. ZanutoII; Bruna T. C. SaraivaII; Fernanda C.S.G. TebarII; Leandro D. DelfinoII; Diego G.D. ChristofaroII, IV
IMestre em Saúde Pública - Universidade de São Paulo - FSP/USP, São Paulo-SP
IIGrupo de Estudos em Atividade Física e Saúde (GEAFS), UNESP, Presidente Prudente, SP
IIIDocente do curso de Fisioterapia e do Programa de Pós-Graduação em Fisioterapia da UNESP de Presidente Prudente-SP
IVDocente do curso de Educação Física da UNESP de Presidente Prudente-SP e do Programa de Pós-Graduação em Ciências da Motricidade da UNESP de Rio Claro-SP
ABSTRACT
INTRODUCTION: Among human development stages, adolescence comprises the period in which intense somatic and behavioural changes occur1. In this period of life, the presence of detrimental health habits can be consolidated until and into adulthood, and can be a precursor for higher risk of mortality and chronic diseases.
OBJECTIVE: The aim of this study was to determine the prevalence of abdominal obesity and its associated factors among adolescents, independent of confounders.
METHODS: A sample of 14-17-year-old individuals (n = 1.231), who were students from Londrina/PR - Brazil public schools, was studied. A questionnaire about physical activity, sedentary behaviour and socioeconomic conditions was applied. Anthropometry was composed of body weight (kg), height (m), body mass index (BMI = kg/m2) and waist circumference (cm). The association of abdominal obesity and independent variables was assessed using the chi-square test and the magnitude of associations was verified using Binary Logistic Regression in an unadjusted model and adjusted for confounders (gender, age, socioeconomic status, physical activity and sedentary behaviour). The confidence interval and statistical significance were set at 95% and 5%, respectively, using SPSS v15.0.
RESULTS: The abdominal obesity prevalence was 17.5% (CI = 15.4%-19.6%), and was higher in boys than in girls. Adolescents with abdominal obesity had higher values of body weight, height, body mass index and sedentary behaviour compared to eutrophic individuals. Being male increased the risk of abdominal obesity by 36% in adolescents. This risk was two times higher in those with high levels of sedentary behaviour.
CONCLUSION: Abdominal obesity was significantly associated with gender and high levels of sedentary behaviour, regardless of confounding factors. Lifestyle habits are important modifiable risk factors that can effectively contribute to the reduction of obesity from an early age.
Keywords: abdominal obesity, waist circumference, sedentary behaviour, adolescents.
RESUMO
OBJETIVO: Verificar a prevalência de obesidade abdominal e fatores associados em adolescentes brasileiros, independentemente de fatores de confusão.
MÉTODO: Amostra composta por adolescentes de 14 a 17 anos (n = 1.231), alunos de escolas públicas de Londrina/PR-Brasil. Um questionário sobre o nível de atividade física, comportamento sedentário e condições socioeconômicas foi aplicado. A antropometria foi composta por peso corporal (kg), estatura (m), índice de massa corporal (IMC = kg/m2) e circunferência de cintura (cm). A associação entre obesidade abdominal e as variáveis independentes foi verificada pelo teste qui-quadrado e a magnitude das associações verificada por Regressão Logística Binária no modelo não-ajustado e ajustado por confundidores (sexo, idade, nível socioeconômico, atividade física e comportamento sedentário). O intervalo de confiança e a significância estatística foram fixados em 95% e 5%, respectivamente, por meio da utilização do programa estatístico SPSS v15.0.
RESULTADOS: A prevalência de obesidade abdominal foi de 17,5% (IC = 15,4%-19,6%) em adolescentes brasileiros, sendo maior em meninos do que em meninas. Indivíduos com obesidade abdominal apresentaram maiores valores de peso corporal, estatura, índice de massa corporal e comportamento sedentário do que indivíduos eutróficos. Ser do sexo masculino elevou em 50% o risco de adolescentes apresentarem obesidade abdominal. Esse risco foi duas vezes maior nos que tiveram elevado comportamento sedentário.
CONCLUSÃO: Obesidade abdominal foi associada significativamente ao sexo e ao elevado comportamento sedentário, independentemente de fatores de confusão. Hábitos de vida são importantes fatores de risco modificáveis que podem contribuir efetivamente na redução da obesidade desde idades precoces.
Palavras-chave: obesidade abdominal, adolescentes, circunferência de cintura, comportamento sedentário.
INTRODUCTION
Among human development stages, adolescence comprises the period in which intense somatic and behavioural changes occur1. In this period of life, the presence of detrimental health habits can be consolidated until and into adulthood, and can be a precursor for higher risk of mortality and chronic diseases2,3. In Brazil, the prevalence of obesity among children and adolescents has demonstrated an abrupt and progressive increase in recent decades, especially among males4. When considered as a disease, obesity is a major risk factor for the development of, among others, hypertension, diabetes, some cancers and dyslipidaemia, as well as an increase in risk of early death5.
As well as general obesity, fat concentration in the abdominal region has been associated with an increased risk of metabolic diseases in the population in recent decades, and is the the most frequently occurring cardiometabolic factor among children and adolescents6,7. More than a quarter of Brazilian children and adolescents (27.3%) had a prevalence of fat gain around the waist, and abdominal fat was greater among younger individuals who lived in a household with higher income levels, as well as those who demonstrated lower levels of physical activity and high levels of sedentary behaviour8.
High waist circumference in adolescents was associated with increased arterial pressure9,10. Male adolescents had a higher prevalence of abdominal fat when compared to females, although being overweight presents similar behaviours in both sexes11. The findings that associated measurements of waist circumference to gender in children and adolescents are not agreed upon in the literature. When parsing this association, Moser et al.12 showed a higher incidence of abdominal obesity in girls than in boys.12 Another study of adolescents aged 12 to 17 years did not observe significant differences between the genders13.
High levels of sedentary behaviour has also been associated with higher levels of abdominal obesity8,14. Salvador et al.8 found that fat accumulation around the waist was associated with sedentary behaviour far more strongly than it was with being overweight. On the other hand, being physically active was not associated with lower levels of abdominal obesity, which had also been observed by other authors14.
The identification of factors associated with abdominal obesity in adolescents allows for a better understanding of their determinants and can guide prevention strategies for risk factors, as well as contribute to improvements in the overall health of this population. The negative contribution of high abdominal fat to health risks signals the need for prevention at earlier ages that is aimed at promoting the reinforcement of healthy habits in adulthood. This study aimed to determine the prevalence of abdominal obesity among adolescents in the city of Londrina/PR-Brazil, in addition to finding associated factors that contribute to obesity, independently of confounding factors.
METHODS
Sample
The sample consisted of adolescents at least 14 years of age, up to at a maximum of 17 years, from public schools in Londrina, located in southern Brazil. After surveying the Regional Education Centre of Londrina-PR, it was found that the schools that received more adolescents from all regions of the city (North, South, East, West and Central areas) were the downtown area schools. Thus, the six largest schools in the central area were selected for the research. To calculate the sample, we used an approximate prevalence of abdominal fat set at 28%, which was based on a previous study8, as well as a tolerable error of 3.5% and an effect correction of 1.5. This provided a minimum sample size of 914 subjects. Anticipating possible losses, 20% of this number was added, requiring a total of 1097 subjects. By the end of the study, 1231 adolescents had been assessed. All parents/guardians of the study participants signed an informed consent form, allowing the teens to participate in the study. The Research Ethics Committee of the State University of Londrina approved this study (process: 203/10).
Anthropometry
Body weight was measured using a digital scale accurate to 0.1 kg. Height was measured accurately in centimetres (cm) using a stadiometer. Later, BMI was calculated by dividing weight by the square of the height. The waist circumference was determined in millimetres by the minimum circumference between the iliac crest and the last rib, using a non-elastic tape (mm). Taylor et al.15, considering the gender and age of the adolescents, established the cut-off points used to classify abdominal obesity.
Engagement in physical activity
Engagement in physical activity was assessed via Baecke et al.16 questionnaire, which has been validated for use in the Brazilian population17. It provides an adimensional score based on different degrees of physical activity among adolescents16. Teens classified as sufficiently active were located in the highest quartile for physical activity (Q4), those located in the lower quartiles were classified as insufficiently active.
Sedentary behaviour
Sedentary behaviour was determined by assessing the use of television, computer and videogames by adolescents throughout the week. The cut-off points used to classify adolescents as having high levels of sedentary behaviour were those Thibault et al.18 recommended. According to these authors, adolescents with sedentary behaviour of more than 22 hours per week (~ 3.1 hours/day) should be classified as demonstrating high levels of sedentary behaviour.
Socioeconomic status
Socioeconomic status was verified using the survey of the Brazilian Association of Companies and Research19. This instrument considers the classification of consumer goods (cars, home appliances, some specific rooms in the house such as the number of bathrooms in the home, and whether or not a maid is employed) and parental education. This instrument classifies the socioeconomic status of individuals as follows: A1, A2, B1, B2, C1, C2, D, E. The adolescents were classified according to economic class as follows: high (A1, A2, B1), medium (B2, C1, C2) and low (D, E).
Statistical analysis
The sample characterisation variables were presented as mean and standard deviation. Frequency analysis was used to show the prevalence of abdominal obesity. The association between the outcome variable (abdominal obesity) and the independent variables (gender, age, socioeconomic status, physical activity and sedentary behaviour) was verified using the chi-square test. Binary Logistic Regression verified the magnitude of the association. In an adjusted analysis, when one of the independent variables was not considered as the main independent variable at the time of the analysis, other independent variables in the setting were inserted. For example, in an analysis of the association between abdominal obesity and gender, other independent variables (age, socioeconomic status, physical activity and sedentary behaviour) were entered as adjustments. In the analysis between abdominal obesity and age, the other variables (gender, socioeconomic status, physical activity and sedentary behaviour) were considered as an adjustment, and so forth. The confidence interval adopted in this study was 95% and statistical significance was set at 5%. SPSS version 15.0 was used as the statistical programme in the analysis.
RESULTS
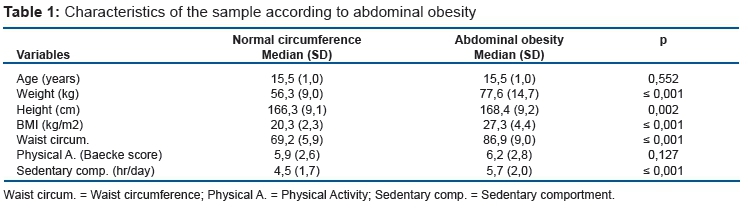
The abdominal obesity prevalence in the present study was 17.5% (CI = 15.4%-19.6%), which was proportionally higher in boys than in girls (p = 0.009). Table 1 shows the characteristics of adolescents by waist circumference classification (normal circumference or abdominal obesity). Adolescents with abdominal obesity had higher body weight, were taller, had higher BMI and waist circumference, and spent more time in sedentary behaviour (Table 1).
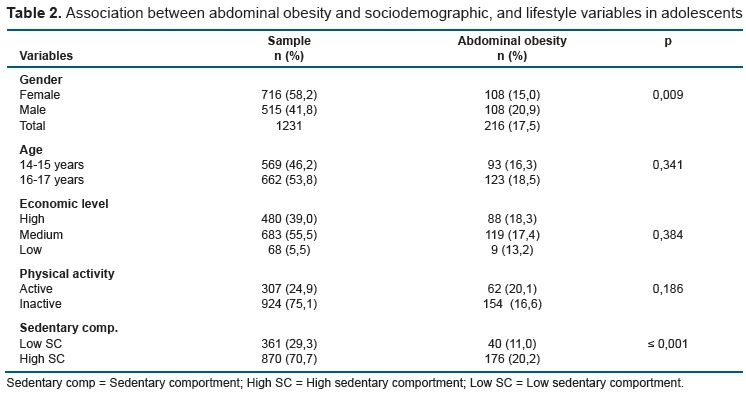
Table 2 presents information about the association of abdominal obesity and the independent variables considered in the study: the socio-demographic variable (gender, age and socioeconomic status) and the lifestyle variable (physical activity and time spent in sedentary behaviour). It was observed that being a male and having high levels of sedentary behaviour were factors associated with abdominal obesity in adolescents (Table 2).
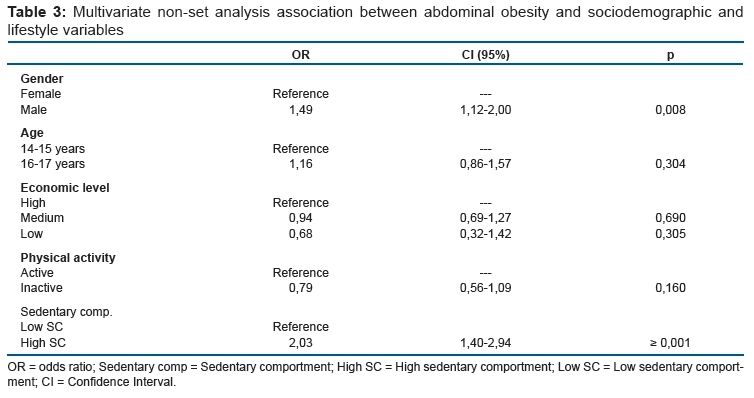
Binary Logistic Regression verified the magnitude of the association. The male adolescents were about 50% more likely to develop abdominal obesity when compared to females. There were no statistically significant differences when considering age, socioeconomic status and physical activity. However, the great amounts of time spent in sedentary behaviours was the biggest factor associated with abdominal obesity, with adolescents classified as having high levels of sedentary behaviour being about twice as likely to present abdominal obesity (Table 3).
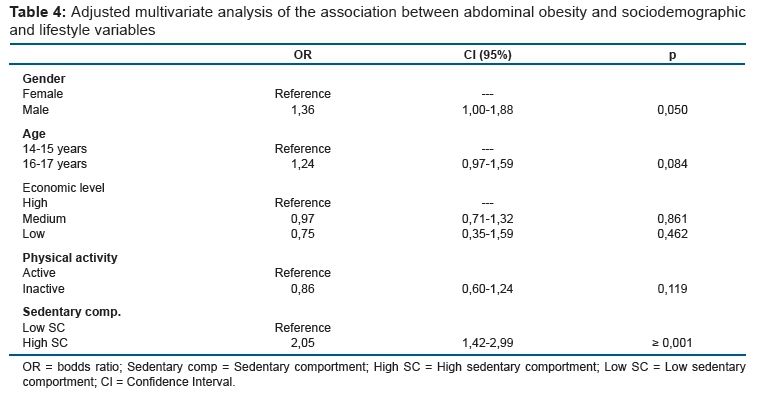
Associations after adjustments are presented in Table 4. In this setting, each dependent variable, when not considered a primary dependent variable, was inserted together as an adjustment. After this analysis, it was observed that being male and having high levels of sedentary behaviour were factors associated with abdominal obesity (Table 4).
DISCUSSION
The prevalence of abdominal obesity observed in adolescents was 17.5%. This prevalence was higher in males when compared to females. Adolescents who had abdominal obesity showed higher body weight, height, BMI and sedentary behaviour than did lean individuals. Being male increased the risk of presenting abdominal obesity by 36% (adjusted analysis). This risk was twice as high in those who demonstrated high levels of sedentary behaviours.
The abdominal obesity observed in these samples was very similar to the prevalence that Kelishadi and colleagues verified in the Iranian population20. The authors evaluated 23,043 individuals between 6 and 18 years of age and found a prevalence of 17.6%. Out of these individuals, 90.9% were from public schools. They also observed that the prevalence of abdominal obesity was higher among boys, which corroborates Klein-Platat et al.14 findings, along with the present study's findings
When assessing Brazilian children and adolescents between 8 and 17 years of age, Salvador et al.8 found a central obesity prevalence of 27.3%, but among adolescents 14-17 years of age, this rate decreased to 16.7%. However, significant differences between genders were not observed. The smaller sample size (n = 72), especially of individuals between 14 and 17 years of age, may, however, affect their comparison with other population studies.
The association of abdominal obesity with high levels of sedentary behaviour, as found in this study, corroborates other findings in the literature8,14,20. Salvador et al.8 found that physical inactivity was more significantly associated with abdominal obesity than was being overweight. Kelishadi et al.20 observed that the prevalence of obesity was higher among individuals with higher levels of sedentary behaviour. Klein-Platat et al.14 found that, regardless of gender, waist circumference was negatively associated with structured physical activity and was positively associated with physical inactivity.
Lengthy engagement in activities such as watching television or using the computer has demonstrated an association with poor dietary habits such as consuming foods and beverages rich in energy, further aggravated by the consumer stimulus presented by advertisements21. One in four teens with bad eating habits presented abdominal obesity, with 40-50% higher risk when compared to adolescents who had high food safety22. Thus, the increase in caloric intake volume, coupled with the sharp decline in daily physical activity levels among teens23-25, and even further among overweight subjects26, corresponded to important determinants for increasing adiposity and body weight. However, the association between abdominal obesity and inadequate dietary habits has not yet been fully verified in the literature27.
The association between abdominal obesity and lower levels of physical activity was not observed in this study, which was also not observed by Salvador et al.8 One possible explanation is due to the fact that subjects suffering from abdominal obesity can engage in physical activity in an attempt to reduce adiposity, which thus results in a reverse causality phenomenon and inhibits possible inferences. However, other studies found a significant association between being physically active and a lower prevalence of obesity among adolescents14,28.
There were no differences in abdominal obesity when considering the socioeconomic status of adolescents. Unlike our findings, Salvador et al.8 found a higher prevalence of abdominal obesity among individuals with higher income levels. However, that study assessed individuals in public and private schools, while respecting their proportional distribution in the studied area. Research suggests that private schools concentrate children and adolescents of higher socioeconomic status, presenting a higher prevalence of being overweight/obese when compared to students from lower socioeconomic conditions29,30. The homogeneity of adolescents evaluated in this study, whom all came from public schools, can probably be considered when analysing the correlations between socioeconomic status and abdominal obesity.
A longitudinal study of Chinese adolescents found that family income was negatively associated with abdominal adiposity over the years31. Another follow-up study among British adolescents also found that waist circumference values were higher in lower socioeconomic groups, although the researchers did not verify statistical differences between boys and girls32. Regardless, high levels of abdominal obesity in children and adolescents represent a significant public health problem, especially because of its deleterious health effects over time33,34. An important form of intervention in combating abdominal obesity in school-age children and adolescents can be started right at school. Increased activity levels in physical education classes were found to be associated with lower adiposity gains in adolescents. Boys between 11 and 12 years of age who participated in physical education classes three times a week decreased their waist circumference by about 3 cm when compared to boys who participated only once or twice. The comparisons between girls showed the same behaviour, but without a statistically significant difference35.
These findings strengthen our conclusion that engagement in physical education is a good strategy for the control of obesity in children and adolescents. The effective intervention in the paediatric population can result in healthier adults, as it has been established that obesity before 11 years of age persists significantly during adolescence, and has no decreasing maturation32.
The frequent and regular inclusion of breaks from sedentary behaviour has been associated with lower levels of BMI, waist circumference, triglycerides and blood glucose, when compared with individuals who did not take breaks36. Interrupting sedentary behaviour therefore seems to be a mitigating factor for the health problems stemming from sedentary behaviour. Studies suggest that the recommendation of breaks from sedentary behaviour should be complementary to the recommendations of physical activity in order to improve health conditions and decrease harm caused by this kind of behaviour in the adult population. It may also possibly offer benefits in the paediatric population.
The limitations of this study correspond to the cross-sectional design, which precludes the causality inference and risk estimation. The self-reported information about physical activity and sedentary behaviour levels were susceptible to memory bias of the interviewees, as well as to the reliability of the provided information. Maturational and genetic factors were not evaluated in this study and could foster better investigations.
On the other hand, this study consists of the analysis of epidemiological data from a relevant sample size, obtained through a high response rate (84.9%). One new feature of this study is consideration of the adjusted multivariate analysis, as well commonly considered variables such as confounding factors (gender, age and socioeconomic status), and other independent variables (physical activity and sedentary behaviour). It is noteworthy that this study considered several types of sedentary behaviour in adolescents (use of television, computers and video games), and not just the single use of time spent watching television, to characterise this kind of behaviour.
CONCLUSION
Abdominal obesity was significantly associated with gender and high levels of sedentary behaviour among adolescents, regardless of other factors. Sedentary behaviour represents an important modifiable risk factor that can significantly contribute to the reduction of abdominal obesity by promoting healthy lifestyles. Obesity needs to be controlled at an early age in order to reduce its levels in adulthood.
REFERENCES
1. World Health Organization (WHO). Physical status: the use and interpretation of anthropometry. Geneva: World Health Organization; 1995. [ Links ]
2. Sichieri R, Souza RA. Strategies for obesity prevention in children and adolescents. Cad ude Publica. 2008; 24(Suppl 2):209-23. DOI: http://dx.doi.org/10.1590/S0102-311X2008001400002 [ Links ]
3. Klein JD, Matos Auerbach M. Improving adolescent health outcomes. Minerva Pediatr. 2002;54(1):25-39. [ Links ]
4. Friedrich RR, Schuch I, Wagner MB. Effect of interventions on the body mass index of school-age students. Rev Saude Publica. 2012; 46(3):551-60. DOI: http://dx.doi.org/10.1590/S0034-89102012005000036 [ Links ]
5. Halley Castillo E, Borges G, Talavera JO, Orozco R, Vargas-Alemán C, Huitrón-Bravo G, et al. Body mass index and the prevalence of metabolic syndrome among children and adolescents in two Mexican populations. J Adolesc Health. 2007;40(6):521-6. DOI: http://dx.doi.org/10.1016/j.jadohealth.2006.12.015 [ Links ]
6. Martins IS, Marinho SP. The potential of central obesity anthropometric indicators as diagnostic tools. Rev Saude Publica. 2003; 37(6):760-67. DOI: http://dx.doi.org/10.1590/S0034-89102003000600011 [ Links ]
7. Sena ASS, Cardoso AS, Carvalho DF, Medeiros JL, Coutinho GF, Albuquerque FCL, et al. Excessive daytime sleepness and cardiometabolic risk factors in children and teenagers with overweight. J Hum Growth Dev. 2013;23(1):24-30. DOI: http://dx.doi.org/10.7322/jhgd.50387 [ Links ]
8. Salvador CCZ, Kitoko PM, Gambardella AMD. Nutritional status of children and adolescents: factors associated to overweight and fat accumulation. J Hum Growth Dev. 2014; 24(3): 313-319. DOI: http://dx.doi.org/10.7322/jhdg.88969. [ Links ]
9. Noronha JAF, Ramos ALC, Ramos AT, Cardoso MAA, Carvalho DF, Medeiros CCM. High blood pressure in overweight children and adolescents. J Hum Growth Dev. 2012; 22(2):196-201. DOI: http://dx.doi.org/10.7322/jhgd.44940 [ Links ]
10. Guimarães ICB, Almeida AM, Santos AS, Barbosa DBV, Guimarães AC. Blood Pressure: Effect of Body Mass Index and of Waist Circumference on Adolescents. Arq Bras Cardiol. 2008;90(6):426-32. DOI: http://dx.doi.org/10.1590/S0066-782X2008000600007 [ Links ]
11. Leite ACB, Ferrazzi NB, Mezadri T, Höfelmann DA. Body dissatisfaction among students in Brazilian Southern city. J Hum Growth Dev. 2014;24(1):54-61. DOI: http://dx.doi.org/10.7322/jhgd.72154 [ Links ]
12. Moser DC, Milano GE, Brito LMS, Titski ACK, Leite N. High blood pressure, overweigth and abdominal obesity in children and adolescents. Rev Educ Física/UEM. 2011;22(4): 591-600. DOI: http://dx.doi.org/10.4025/reveducfisv22n4p591-600 [ Links ]
13. Cabrera TFC, Correia IFL, Santos DO, Pacagnelli FL, Prado MTA, Silva TD, et al. Analisys of the prevalence of overweight and obesity and the level of physical activity in children and adolescents of a southwestern city of Sao Paulo. J Hum Growth Dev. 2014; 24(1):67-72. DOI: http://dx.doi.org/10.7322/jhgd.73455 [ Links ]
14. Klein-Platat C, Oujaa M, Wagner A, Haan MC, Arveiler D, Schlienger JL, et al. Physical activity is inversely related to waist circumference in 12-y-old French adolescents. Int J Obes. 2005; 29(1):9-14. DOI: http://dx.doi.org/10.1038/sj.ijo.0802740 [ Links ]
15. Taylor RW, Jones IE, Williams SM, Goulding A. Evaluation of waist circumference, waist-to-hip ratio, and the conicity index as screening tools for high trunk fat mass, as measured by dual-energy X-ray absorptiometry, in children aged 3-19 y. Am J Clin Nutr. 2000;72(2):490-5. [ Links ]
16. Baecke JA, Burema J, Frijters JE. A short questionnaire for the measurement of habitual physical activity in epidemiological studies. Am J Clin Nutr. 1982; 36(5):936-42. [ Links ]
17. Guedes DP, Lopes CC, Guedes J, Stanganelli LC. Reproducibility and validity of the Baecke questionnaire for assessing of the habitual physical activity in adolescents. Rev Port Cien Desp. 2006; 6(3):265-74. [ Links ]
18. Thibault H, Contrand B, Saubusse E, Baine M, Maurice-Tison S. Risk factors for overweight and obesity in French adolescents: physical activity, sedentary behavior and parental characteristics. Nutrition. 2010;26(2):192-200. DOI: http://dx.doi.org/10.1016/j.nut.2009.03.015 [ Links ]
19. Instituto Brasileiro de Opinião Pública e Estatística (IBOPE). Levantamento sócio-econômico, 2009. Rio de Janeiro. [cited 2015 Oct 08] Available from: www.abep.org/Servicos/Download.aspx? [ Links ]
20. Kelishadi R, Motlagh ME, Bahreynian M, Gharavi MJ, Kabir K, Ardalan G, et al. Methodology and Early Findings of the Assessment of Determinants of Weight Disorders among Iranian Children and Adolescents: The Childhood and Adolescence Surveillance and PreventIon of Adult Noncommunicable Disease-IV Study. Int J Prev Med. 2015;6:77. DOI: http://dx.doi.org/10.4103/2008-7802.162953 [ Links ]
21. Novaes JF, Franceschini SC, Priore SE. Comparison of the anthropometric and biochemical variables between children and their parents. Arch Latinoam Nutr. 2007;57 (2):137-45. [ Links ]
22. Holben DH, Taylor CA. Food Insecurity and Its Association With Central Obesity and Other Markers of Metabolic Syndrome Among Persons Aged 12 to 18 Years in the United States. J Am Osteopath Assoc. 2015;115(9):536-43. DOI: http://dx.doi.org/10.7556/jaoa.2015.111 [ Links ]
23. Shokrvash B, Majlessi F, Montazeri A, Nedjat S, Rahimi A, Djazayeri A, et al. Correlates of physical activity in adolescence: a study from a developing country. Glob Health Action. 2013; 6: 203-27. DOI: http://dx.doi.org/10.3402/gha.v6i0.20327 [ Links ]
24. Nader P; National Institute of Child Health and Human Development Study of Early Child Care and Youth Development Network. Frequency and intensity of activity of third-grade children in physical education. Arch Pediatr Adolesc Med. 2003;157(2):185-90. DOI: http://dx.doi.org/10.1001/archpedi.157.2.185 [ Links ]
25. Ridgers ND, Stratton G, Fairclough SJ. Physical activity levels of children during school playtime. Sports Med 2006;36(4):359-71. DOI: http://dx.doi.org/10.2165/00007256-200636040-00005 [ Links ]
26. Baruki SB, Rosado LE, Rosado GP, Ribeiro RC. Association between nutritional status and physical activity in Municipal Schools in Corumbá - MS. Rev Bras Med Esporte. 2006;12(2):90-4. DOI: http://dx.doi.org/10.1590/S1517-86922006000200007 [ Links ]
27. Pinasco GC, Silva JP, Almeida PCD, Silva VR, Arruda BF, Lopes BP, et al. Association between food consumption as predictor of cardiovascular risk and waist circumference increase in teenagers. J Hum Growth Dev. 2015; 25(3):319-24. DOI: http://dx.doi.org/10.7322/jhgd.106010 [ Links ]
28. Cavalcanti CBS, Barros MVG, Menêses AL, Santos CM, Azevedo AMP, Guimarães FJSP. Obesidade abdominal em adolescentes: prevalência e associação com atividade física e hábitos alimentares. Arq Bras Cardiol. 2010; 94(3):371-7. DOI: http://dx.doi.org/10.1590/S0066-782X2010000300015 [ Links ]
29. Leão LSCS, Araújo LMB, Moraes LTLP, Assis AM. Prevalência de obesidade em escolares de Salvador, Bahia. Arq Bras Endocrinol Metab. 2003;47(2):151-7. DOI: http://dx.doi.org/10.1590/S0004-27302003000200007 [ Links ]
30. Ronque ERV, Cyrino ES, Dorea VR, Serassuelo Junior H, Galdi EHG, Arruda M. Prevalence of overweight and obesity in schoolchildren of high socioeconomic level in Londrina, Paraná, Brazil. Rev Nutr. 2005;18(6):709-17. DOI: http://dx.doi.org/10.1590/S1415-52732005000600001 [ Links ]
31. Felicitas JQ, Tanenbaum HC, Li Y, Chou CP, Palmer PH, Spruijt-Metz D, et al. A longitudinal analysis of the effects of socioeconomic factors, foreign media, and attitude toward appearance on general and central adiposity in chinese adolescents. Prev Med Rep. 2015;2:608-214. DOI: http://dx.doi.org/10.1016/j.pmedr.2015.07.003 [ Links ]
32. Wardle J, Brodersen NH, Cole TJ, Jarvis MJ, Boniface DR. Development of adiposity in adolescence: five year longitudinal study of an ethnically and socioeconomically diverse sample of young people in Britain. BMJ. 2006; 13;332(7550):1130-5. DOI: http://dx.doi.org/10.1136/bmj.38807.594792.AE [ Links ]
33. Schutte AE, van Rooyen JM, Huisman HW, Kruger HS, Malan NT, De Ridder JH, et al. Dietary risk markers that contribute to the aetiology of hypertension in black South African children: The THUSA BANA study. J Hum Hypertens. 2003;17(1):29-35. DOI: http://dx.doi.org/10.1038/sj.jhh.1001508 [ Links ]
34. Van Rooyen JM, Kruger HS, Huisman HW, Schutte AE, Malan NT, Schutte R. Early cardiovascular changes in 10- to 15-year-old stunted children: The transition and health during urbanization in South Africa in Children study. Nutrition. 2005;21(7-8):808-14. DOI: http://dx.doi.org/10.1016/j.nut.2004.12.007 [ Links ]
35. Wardle J, Brodersen NH, Boniface D. School-based physical activity and changes in adiposity. Int J Obes (Lond). 2007; 31(9):1464-8. DOI: http://dx.doi.org/10.1038/sj.ijo.0803651 [ Links ]
36. Healy GN, Dunstan DW, Salmon J, Cerin E, Shaw JE, Zimmet PZ, et al. Breaks in sedentary time: beneficial associations with metabolic risk. Diabetes Care. 2008;31(4): 661-6. DOI: http://dx.doi.org/10.2337/dc07-2046 [ Links ]
 Correspondence:
Correspondence:
Diego Giuliano Destro Christofaro
E-mail: diegochristofaro@yahoo.com.br
Manuscript submitted Nov 2015
Accepted for publication Jan 2016


{kind=link}
{kind=link}
{kind=link}
{kind=link}