










Serviços Personalizados
artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282versão On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.27 no.1 São Paulo jan./abr. 2017
http://dx.doi.org/10.7322/jhgd.119236
ORIGINAL ARTICLE
Impact of bronchopulmonary dysplasia on pulmonary function during childhood: a systematic review
Repercussão da displasia broncopulmonar na função pulmonar durante infância: revisão sistemática
Janaina Cristina ScalcoI; Rafaela Coelho MinskyII; Francieli Camila MuchaIII; Camila Isabel Santos SchivinskiIV
IM.A., Professor of the Department of Physiotherapy at the State University of Santa Catarina, Florianopolis/SC/Brazil
IIPhysiotherapist, Master´s Degree in Physiotherapy from the State University of Santa Catarina, Florianopolis/SC/Brazil
IIIPhysiotherapist, Graduate Student in the Graduate Program for Physiotherapy at the State University of Santa Catarina, Florianopolis /SC/Brazil
IVPh.D., Full Professor of the Department of Physiotherapy at State University of Santa Catarina, Florianopolis/SC/Brazil
ABSTRACT
INTRODUCTION: Bronchopulmonary dysplasia (BPD) is a multifactorial chronic lung disease that contributes to disruption of pulmonary development. It may impair pulmonary function in early childhood and persist throughout school-age, adolescence, and into adulthood.
OBJECTIVE: To analyze, through a systematic review, the impact of BPD on pulmonary function in early childhood. : Systematic searches were performed in three electronic databases (Medline, SciELO and PEDro). Two independent examiners analyzed the titles, abstracts and full texts, considering the following study inclusion criteria: studies of pulmonary function in up to 5-year-old children diagnosed with BPD in the neonatal period.
RESULTS: Initially, 1789 articles were identified, and the final sample included 22 articles. It could be observed that children diagnosed with BPD in early childhood showed expiratory flow limitation and reduced functional residual capacity. However, pulmonary function in children with a history of BPD remains reduced when compared with healthy full-term children. Moreover, there are no positive responses in pulmonary function values with the use of bronchodilators.
CONCLUSION: Children with BPD show changes in pulmonary function, which may improve with growth, and most of them do not respond positively to bronchodilators.
Keywords: bronchopulmonary dysplasia, lung diseases, infant, respiratory function testing, child.
RESUMO
INTRODUÇÃO: A displasia broncopulmonar (DBP) é uma doença pulmonar crônica multifatorial que interrompe o desenvolvimento pulmonar, podendo repercutir em comprometimento da função pulmonar na primeira infância, que pode perdurar durante a idade escolar, adolescência, até a idade adulta.
OBJETIVO: Analisar, através de uma revisão sistemática, as repercussões da DBP na função pulmonar de crianças na primeira infância.
MÉTODO: Foram realizadas buscas sistematizadas em três bases de dados eletrônicas (Medline, SciELO e PEDro). Dois examinadores independentes analisaram sistematicamente os títulos, resumos e textos na íntegra, considerando os seguintes critérios de inclusão: estudos que avaliaram a função pulmonar de crianças com até 5 anos de idade que apresentaram diagnóstico de DBP no período neonatal
RESULTADOS: Inicialmente foram identificados 1789 artigos, sendo que a amostra final foi composta de 22 artigos. Evidenciou-se que crianças com DBP apresentam na primeira infância limitação dos fluxos expiratórios e redução da capacidade residual funcional. Estas alterações podem ser normalizadas ou minimizadas com o crescimento e adequação de peso, porém, a função pulmonar das crianças com história de DBP continua reduzida em comparação a crianças hígidas nascidas a termo. Ainda, a maioria delas não apresenta respostas positivas nos valores de função pulmonar com o uso de broncodilatadores.
CONCLUSÃO: Crianças com DBP apresentam alterações na função pulmonar, podendo melhorar com o crescimento, sendo que a maioria não responde positivamente ao broncodilatador.
Palavras-chave: displasia broncopulmonar, doenças pulmonares, lactente, testes de função respiratória, criança.
INTRODUCTION
Neonatal chronic lung disease, also known as bronchopulmonary dysplasia (BPD), is defined as the need for respiratory support with oxygen and/or mechanical ventilation in the first 28 days of life1-4. Children who developed the disease in the postnatal period may show abnormalities in pulmonary function5.
Currently, pulmonary function testing in early childhood, i.e., the time period ranging from 0 to 6 years including infants and preschoolers, can be performed by examinations, such as rapid chest compression, single breath occlusion, plethysmography and helium dilution6. Studies indicate that infants with BPD show compromised pulmonary function in the first years of life, with significant expiratory flow limitation, namely, forced expiratory volume in one second (FEV1), mean forced expiratory flow (FEF25-75%), as well as reduced pulmonary compliance, increased pulmonary resistance, higher respiratory rate, reduced functional residual capacity (FRC) and residual volume7-24.
These results are characteristics of ventilatory and functional changes, the knowledge of which may provide a better understanding of the disease and, consequently, improve treatment and preventive strategies to manage the disease. Therefore, this study aimed to analyze the impact of bronchopulmonary dysplasia on the pulmonary function of infants and preschool children between 0 and 4 years of age.
METHODS
Search Strategy
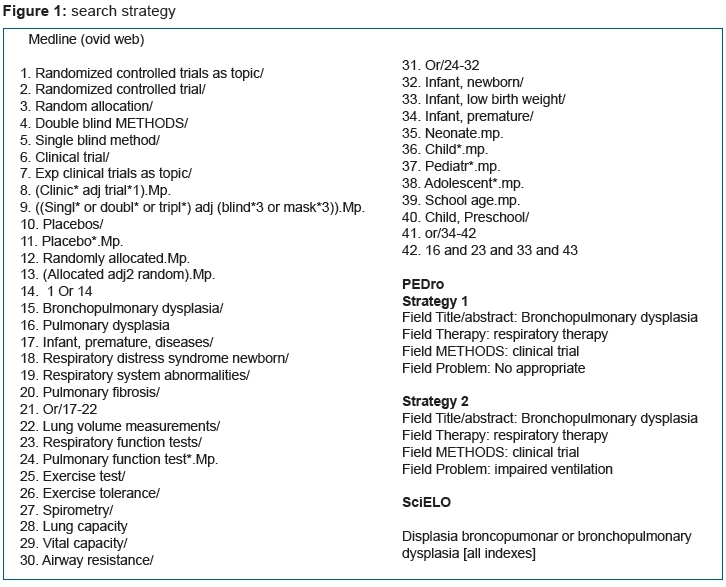
The literature review strategy included electronic searching using three bibliographic online databases: SciELO (Scientific Electronic Library Online), PEDro (Physiotherapy Evidence Data base) and Medline (Medical Literature Analysis and Retrieval System Online via Ovid. The publications were selected until the date of online searching, i.e., September 2016, regardless of the language.
The authors developed a search strategy for Medline (via OVID web) and PEDro, which are shown in (Figure 1), due to the absence of this type of publication on the topic. The following keywords were used for the SciELO database: displasia broncopulmonar, bronchopulmonary dysplasia.
Selection Strategy
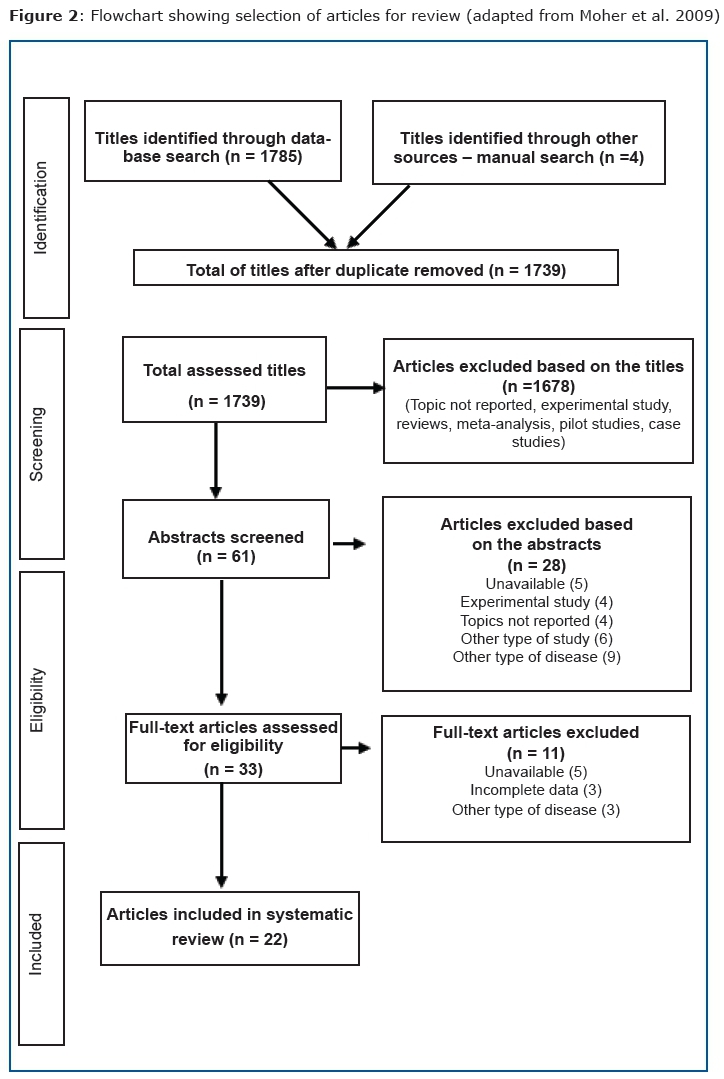
The articles were screened by 2 examiners, who independently analyzed the results of the online search for potentially eligible articles. The publications which met all previously established inclusion criteria were selected, and doubtful cases were discussed. First, the reviewers read the titles, followed by an analysis of the abstracts. The studies that proved to be eligible were reviewed in full, in agreement with the recommendations of the Main Items for Reporting Systematic Reviews and Meta-analysis (PRISMA)25,26 (Figure 2).
Analysis of data
Inclusion criteria were: clinical trials that assessed pulmonary function of infants and preschool children aged 0-4 years with a diagnosis of BPD in the neonatal period. The diagnosis of BPD was defined as the need for supplemental oxygen above 21% during 28 days or more.24 Studies that were not available through the Program Manager Bibliographic Commuting (Comut), the newspaper's website or Ovid database, were not used for analysis.newspaper's website or Ovid database, were not used for analysis.
RESULTS
A total of 1789 articles were identified, 61 titles of which were selected for analysis of their respective abstracts. Next, 33 articles were shortlisted for full review, and 11 were excluded because they did not meet the inclusion criteria. The final sample consisted of 22 articles as shown in the flowchart (figure 2).
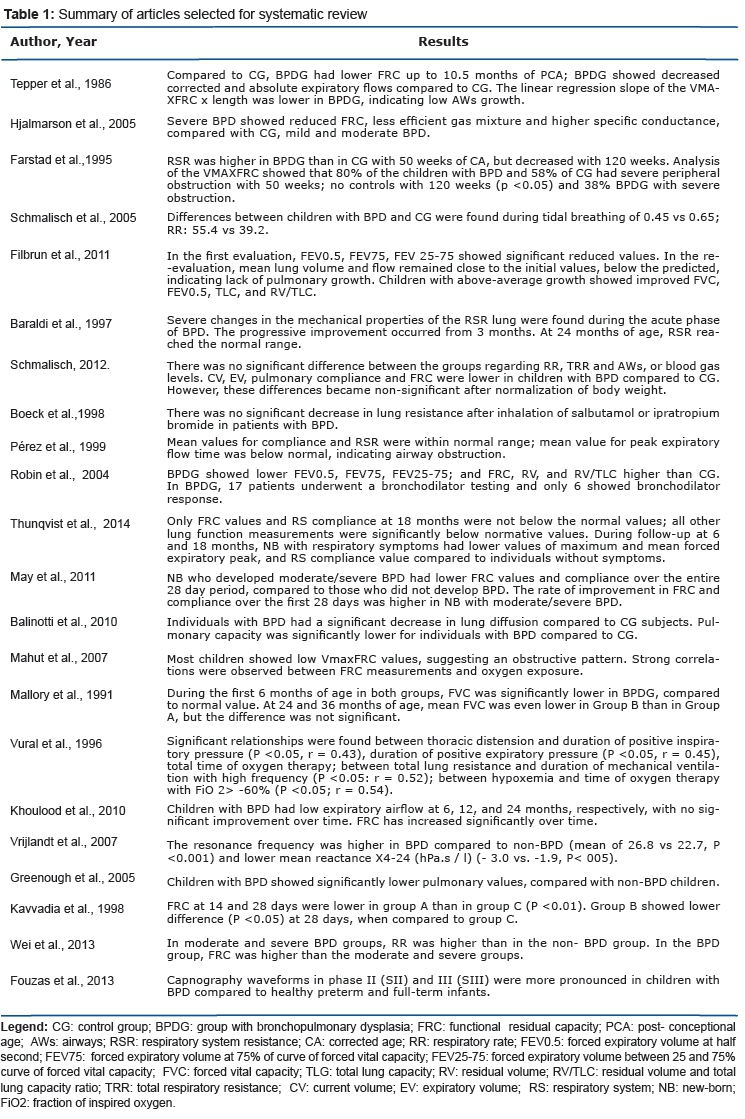
Of the 22 articles included (table 1), 12 assessed children with a history of BPD at different moments (longitudinal)7-16,27,28 and the maximum follow-up was the interval between the neonatal hospital stay and five years of life. The remaining ten reviewed studies performed pulmonary function testing in one single moment (transversal).17-22,29-32
DISCUSSION
Notably, maintaining the integrity of the respiratory system in the first two years of life is essential and will determine the improvement of gas exchange and respiratory reserve after infancy33 as this is the period of greatest alveolar growth34. In this review, the studies suggest that respiratory symptoms and pulmonary function seem to improve in early childhood7,8,10,12,27 with the growth and development of the child with a history of BPD. Farstad et al.12 found that, at 50 weeks of corrected age (CA), 80% of the children with BPD in their study sample had severe peripheral obstruction, compared to 58% of preterm infants without BPD. In the reevaluation period (120 weeks of CA), only 38% of the children with BPD presented with severe obstruction versus no preterm children. According to Sanchez et al.35 the progressive improvement of capacity and flow-volume curves in this population is proportional to the increase in weight and length of infants. On the other hand, Hjalmarson et al.13 observed that the pulmonary function in infants using bronchodilators remains reduced even after normalization of weight, compared to healthy infants. However, these alterations may not be significant considering the normal values of pulmonary function parameters12,17. In this context, some authors7,8,10 point out that improved pulmonary function during infancy is more evident in children with moderate/severe BPD, compared to those with mild BPD, or in preterm infants without BPD28.
It is well-established that some complications caused by BPD in early childhood may favor high rates of respiratory infections, recurrent wheezing and hospital readmissions12,28,33,34,36. According to a study conducted by Tepper et al.14 55% of infants with BPD required prehospitalization during the first year of life due to diseases of the lower respiratory tract. The incidence of respiratory morbidity and prehospitalization has been lower in healthy full-term infants28, as well as in preterm infants who developed respiratory distress syndrome12 when compared to infants with bronchopulmonary dysplasia . However, Mahut et al.29 observed that there is no difference in pulmonary function among BPD infants with frequent symptoms and those with fewer or no symptoms, and all of them showed reduced FRC. These results suggest that pulmonary function as well as other factors may be involved in the high susceptibility to respiratory infections in this population.
Another topic identified in the current review is the response of BPD children to bronchodilators. The selected studies demonstrate no reduction in inspiratory and expiratory resistance after the use of bronchodilators in most children with a history of BPD.
Children who respond to these medications show greater abnormalities in pulmonary function parameters than non-responders22,32. According to Fakhoury et al.23 up to 3 years of age, only 20 to 30% of children with moderate to severe BPD show bronchodilator response. Therefore, this drug should not be indicated for all patients with BPD, but only for responders or patients show worsening in wheezing during acute respiratory exacerbation22,32
Current articles and reviews have shown limited pulmonary function, functional capacity and quality of life of schoolchildren37 and adults38 with BPD. However, the impact of BPD on infants and preschool children has not been often discussed. This review was able to collect results of current studies about the disease in this age group. A limitation of this review is the lack of classification of the methodological quality, by means of valid instruments.
In summary, children with a history of BPD usually show alterations in pulmonary function in the first three years of life, which seems to improve with growth and become non-significant after body weight adequacy. However, when comparing BPD children with full-term children, this limitation can still be observed. Also, most BPD children do not show positive response in pulmonary function after the use of inhaled bronchodilator. But, responders have compromised pulmonary function.
Admittedly, there is a gradual improvement of pulmonary function in the first years of life. Therefore, public health professionals involved in the care of this population should consider the importance of nutritional aspects and prevention of respiratory infections in this period, in order to allow conditions for adequate pulmonary growth and development. This may attenuate alterations in pulmonary function due to neonatal injury. Furthermore, early identification of possible impairment of pulmonary function may help pediatricians and/or pulmonologists to prevent disease complications by means of strategies, e.g., to encourage children to keep regular physical activities as soon as possible, and to refer patients for physical therapy as a preventive measure or during acute respiratory events.
CONCLUSION
It could be observed that children diagnosed with BPD during the neonatal period showed expiratory flow limitation and reduced FRC when assessed in early childhood, compared to healthy full-term and preterm children. Most children show improved values of pulmonary function with growth and normalization of weight.
This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
REFERENCES
1. Gupta S, Sinhá SK, Donn SM. Ventilatory management and bronchopulmonary dysplasia in preterm infants. Semin Fetal Neonatal Med. 2009;14(6):367-73. DOI: http://dx.doi.org/10.1016/j.siny.2009.08.011 [ Links ]
2. Gonzaga AD, Figueira BBD, Sousa JMA, Carvalho WB. Tempo de ventilação mecânica e desenvolvimento de displasia broncopulmonar. Rev Ass Med Bras. 2007;53(1):64-7. DOI: http://dx.doi.org/10.1590/S0104-42302007000100022 [ Links ]
3. Isayama T, Iwami H, McDonald S, Beyene J. Association of noninvasive ventilation strategies with mortality and bronchopulmonary dysplasia among preterm infants: a systematic review and meta-analysis. JAMA. 2016;316(6):611-24. DOI: http://dx.doi.org/10.1001/jama.2016.10708 [ Links ]
4. Lima MRO, Andrade MA, Araújo APG, Figueroa JN, Andrade LB. Influência de fatores maternos e neonatais no desenvolvimento da displasia broncopulmonar. Rev Assoc Med Bras. 2011;57(4):398-403. DOI: http://dx.doi.org/10.1590/S0104-42302011000400012 [ Links ]
5. Coalson JJ. Pathology of new bronchopulmonary dysplasia. SeminNeonatol. 2003; 8(1):73-81. [ Links ]
6. Pérez Tarazona S, Rueda Esteban S, Alfonso Diego J, Barrio Gómez de Agüero MI, Callejón Callejón A, Cortell Aznar I, et al. Guidelines for the follow up of patients with bronchopulmonary dysplasia. An Pediatr (Barc). 2016;84(1):61-e1-9. DOI: http://dx.doi.org/10.1016/j.anpedi.2015.04.020 [ Links ]
7. Mallory GB Jr, Chaney H, Mutich RL, Motoyama EK. Longitudinal changes in lung function during the first three years of premature infants with moderate to severe bronchopulmonary dysplasia. Pediatr Pulm.1991;11(1):8-14. [ Links ]
8. Baraldi E, Filippone M, Trevisanuto D, Zanardo V, Zacchello F. Pulmonary function until two years of life in infants with bronchopulmonary dysplasia. Am Respir Crit Care Med. 1997;155(1):149-55. DOI: http://dx.doi.org/10.1164/ajrccm.155.1.9001304 [ Links ]
9. Fakhoury KF, Sellers C, Smith E O'Brian, Rama JA, Fan LL. Serial Measurements of Lung Function in a Cohort of Young Children WithBronchopulmonary Dysplasia. Pediatrics. 2010;125(6). [ Links ]
10. Filbrun AG, Popova AP, Linn MJ, McIntosh NA, Hershenson MB. Longitudinal measures of lung function in infants with bronchopulmonary dysplasia. Pediatr Pulmonol. 2011;46(4):369-75. DOI: http://dx.doi.org/10.1002/ppul.21378 [ Links ]
11. Thunqvist P, Gustafsson P, Norman M, Wickman M, Hallberg J. Lung function at 6 and 18 months after preterm birth in relation to severity of bronchopulmonary dysplasia. Pediatr Pulmonol. 2015;50(10):978-86. DOI: http://dx.doi.org/10.1002/ppul.23090 [ Links ]
12. Farstad T, Brockmeier F, Bratlid D. Cardiopulmonary function in premature infants with bronchopulmonary dysplasia 2-year follow up. Eur J Pediatr. 1995;154(10):853-8. DOI: http://dx.doi.org/10.1007/BF01959797 [ Links ]
13. Hjalmarson O, Sandberg KL. Lung function at term reflects severity of bronchopulmonary dysplasia. J Pediatr. 2005 Jan;146(1):86-90. DOI: http://dx.doi.org/10.1016/j.jpeds.2004.08.044 [ Links ]
14. Tepper RS, Morgan WJ, Cota K, Taussig LM. Expiratory flow limitation in infants with bronchopulmonary dysplasia. J Pediatr. 1986;109(6):1040-6. DOI: http://dx.doi.org/10.1016/S0022-3476(86)80296-7 [ Links ]
15. Kavvadia V, Greenough A, Dimitriou G, Itakura Y. Lung volume measurements in infants with and without chronic lung disease. Eur J Pediatr. 1998;157(4):336-9. DOI: http://dx.doi.org/10.1007/s004310050823 [ Links ]
16. Vural M, Kremp O, Cambier F, Krim G, Kilani L, Leke L, et al. Evolution of the result of respiratory function studies in children with bronchopulmonary dysplasia. Arch Pediatr. 1996;3(12):1229-38. [ Links ]
17. Schmalisch G, Wilitzki S, Wauer RR. Differences in tidal breathing between infants with chronic lung diseases and healthy controls. BMC Pediatr. 2005;5:36. DOI: http://dx.doi.org/10.1186/1471-2431-5-36 [ Links ]
18. Greenough A, Broughton S. Chronic manifestations of respiratory syncytial virus infection in premature infants. Pediat Infect Dis J. 2005;24(11 Suppl): S184-7. [ Links ]
19. Balinotti JE, Chakr VC, Tiller C, Kimmel R, Coates C, Kisling J, et al. Growth of lung parenchyma in infants and toddlers with chronic lung disease of infancy. Am J Respir Crit Care Med. 2010;181(10):1093-7. DOI: http://dx.doi.org/10.1164/rccm.200908-1190OC [ Links ]
20. Vrijlandt EJ, Gerritsen J, Boezen HM, Grevink RG, Duiverman EJ. Lung function and exercise capacity in young adults born prematurely. Am J Resp Crit Care Med. 2006;173(8):890-6. DOI: http://dx.doi.org/10.1164/rccm.200507-1140OC [ Links ]
21. Wei MC, Yu JL, Liu XH, Qi LF. Characteristics of lung function in preterm infants with varying degrees of bronchopulmonary dysplasia. Zhonghua Yi Xue Za Zhi. 2013;93(22):1716-20. [ Links ]
22. Robin B, Kim YJ, Huth J, Klocksieben J, Torres M, Tepper RS, et al. Pulmonary function in bronchopulmonary dysplasia. Pediatr Pulmonol. 2004;37(3):236-42. DOI: http://dx.doi.org/10.1002/ppul.10424 [ Links ]
23. Fakhoury KF, Sellers C, Smith EO, Rama JA, Fan LL. Serial measurements of lung function in a cohort of young children with bronchopulmonary dysplasia. Pediatrics. 2010;125(6):e1441-7. DOI: http://dx.doi.org/10.1542/peds.2009-0668 [ Links ]
24. Jobe AH, Bancalari E. Bronchopulmonary dysplasia. Am J Respir Crit Care Med. 2001;163(7):1723-9. DOI: http://dx.doi.org/10.1164/ajrccm.163.7.2011060 [ Links ]
25. Moher D, Cook DJ, Eastwood S, Olkin I, Rennie D, Stroup DF. Improving the quality of reporting of meta-analsis of randomised controlled trials: the QUOROM statement. Quality of Reporting of Meta-analyses. Lancet. 1999;354(9193):1896-900. [ Links ]
26. The Cochrane Collaboration. Glossary of terms in The Cochrane Collaboration [Internet]. Version 4.2.5. London: Cochrane Collaboration; 2005. [ Links ]
27. Schmalisch G, Wilitzki S, Roehr CC, Proquitté H, Bührer C. Development of lung function in very low birth weight infants with or without bronchopulmonary dysplasia: longitudinal assessment during the first 15 months of corrected age. BMC Pediatr. 2012;12:37. DOI: http://dx.doi.org/10.1186/1471-2431-12-37 [ Links ]
28. May C, Kennedy C, Milner AD, Rafferty GF, Peacock JL, Greenough A. Lung function abnormalities in infants developing bronchopulmonary dysplasia. Arch Dis Child. 2011;96(11): 1014-9. DOI: http://dx.doi.org/10.1136/adc.2011.212332 [ Links ]
29. Mahut B, De Blic J, Emond S, Benoist MR, Jarreau PH, Lacaze-Masmonteil T, et al. Chest computed tomography findings in bronchopulmonary dysplasia and correlation with lung function. Arch Dis Child Fetal Neonatal Ed. 2007;92(6):F459-64. DOI: http://dx.doi.org/10.1136/adc.2006.111765 [ Links ]
30. Perez CA, Bui KC, Bustorff-Silva J, Atkinson JB. Comparison of intratracheal pulmonary ventilation and hybrid intratracheal pulmonar ventilation with conventional mechanical ventilation in a rabbit model of acute respiratory distress syndrome by saline lavage. Crit Care Med. 2000;28(3):774-81. [ Links ]
31. Fouzas S, Häcki C, Latzin P, Proietti E, Schulzke S, Frey U, et al. Volumetric capnography in infants with bronchopulmonary dysplasia. J Pediatr. 2014;164(2):283-8.e1-3. DOI: http://dx.doi.org/10.1016/j.jpeds.2013.09.034 [ Links ]
32. Boeck K, Smith J, Van Lierde S, Devlieger H. Response to bronchodilators in clinically stable 1-year-old patients with bronchopulmonary dysplasia. Eur J Pediatr. 1998;157(1):75-9. DOI: http://dx.doi.org/10.1007/s004310050771 [ Links ]
33. Chien YH, Tsao PN, Chou HC, Tang JR, Tsou KI. Rehospitalization of extremely-lowbirth-weight infants in first 2 years of life. Ear Hum Dev. 2002;66(1):33-40. http://dx.doi.org/10.1016/S0378-3782(01)00233-X [ Links ]
34. Doyle LW, Ford G, Davis N. Health and hospitalistions after discharge in extremely low birth weight infants. Semin Neonat. 2003;8(2):137-45. DOI: http://dx.doi.org/10.1016/S1084-2756(02)00221-X [ Links ]
35. Sanchez-Solis M, Perez-Fernandez V, Bosch-Gimenez V, Quesada JJ, Garcia-Marcos L. Lung function gain in preterm infants with and without bronchopulmonary dysplasia. Pediatr Pulmonol. 2016;51(9):936-42. DOI: http://dx.doi.org/10.1002/ppul.23393 [ Links ]
36. Ronkainen E, Kaukola T, Marttila R, Hallman M, Dunder T. School-age children enjoyed good respiratory health and fewer allergies despite having lung disease after preterm birth. Acta Paediatr. 2016;105(11):1298-1304. DOI: http://dx.doi.org/10.1111/apa.13526 [ Links ]
37. Scalco JC, Medeiros DL, Schivinski CIS. Capacidade de exercício e função pulmonar de escolares com história de displasia broncopulmonar: revisão sistemática. Medicina (Ribeirão Preto). 2015;48(5):501-11. [ Links ]
38. Gough A, Linden M, Spence D, Patterson CC, Halliday HL, McGarvey LP. Impaired lung function and health status in adult survivors of bronchopulmonary dysplasia. Eur Resp J. 2014;43(3):808-16. DOI: http://dx.doi.org/10.1183/09031936.00039513 [ Links ]
 Correspondence:
Correspondence:
Camila I. S. Schivinski
E-mail: cacaiss@yahoo.com.br
Manuscript submitted Nov 2015
Accepted for publication Jan 2016


{kind=link}
{kind=link}
{kind=link}