










Services on Demand
article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Share

 Permalink
PermalinkJournal of Human Growth and Development
Print version ISSN 0104-1282On-line version ISSN 2175-3598
J. Hum. Growth Dev. vol.27 no.2 São Paulo May/Aug. 2017
http://dx.doi.org/10.7322/jhgd.127747
ORIGINAL ARTICLE
Prevalence and factors associated with functional dependency in homebound elderly people in Brazil
Gracielle PampolimI; Christiane LourençoI; Vanezia Gonçalves da SilvaII; Maria Carlota de Rezende CoelhoIII; Luciana Carrupt Machado SogameIII
IDepartamento de Fisioterapia da Escola Superior de Ciências da Santa Casa de Misericórdia de Vitória (EMESCAM ) - Vitória (ES), Brasil
IIDepartamento de Medicina da Escola Superior de Ciências da Santa Casa de Misericórdia de Vitória (EMESCAM ) - Vitória (ES), Brasil
IIIPrograma de Pós-Graduação em Políticas Públicas e Desenvolvimento Local da Escola Superior de Ciências da Santa Casa de Misericórdia de Vitória (EMESCAM ) - Vitória (ES), Brasil
ABSTRACT
INTRODUCTION: Population ageing is a worldwide reality that requires attention, and a concern for healthy and functional ageing is increasingly the focus of government policies and programmes.
OBJECTIVE: To identify the prevalence of homebound elderly people, and the influence of sociodemographic and economic characteristics on their functional dependency.
METHODS: Cross-sectional study with 178 homebound elderly people assisted by a family healthcare unit in Vitória, ES, Brazil. Functional independence was measured by the Functional Independence Measure (FIM) and the sociodemographic and economic variables were collected by a questionnaire developed by the authors. Binary logistic regression was used to determine the influence of the sociodemographic and economic characteristics on the risk of being functionally dependent.
RESULTS: Forty-eight percent of the participants were functional dependents, 80% were female, 72% belonged to the fourth age, 74% were white, 63% were widowed, 78% had retired, 90% had children, 83% had a caregiver, 52% had low education and 40% had low income. Logistic regression indicated that having a caregiver increased by 40 times the chance of being functionally dependent (OR = 40.2; 95%CI 4.8-355.4) and having between one to eight years of education decreased the chance of functional dependency (OR = 0.2; 95%CI 0.04-0.9).
CONCLUSIONS: The prevalence of functional dependency was very high in this sample, and since the presence of a caregiver was the strongest and significant predictor of functional dependency, we suggest that guidance and support should be offered to caregivers, followed by a family healthcare strategy, to make consistent efforts with the objective of improving functional recovery and independence of homebound elderly.
Keywords: homebound elderly, functional dependence, family health strategy
INTRODUCTION
In the past few years, worldwide demographics have indicated intensive population ageing1. In Brazil, according to the Brazilian Institute of Geography and Statistics, this ageing process has accelerated over the past decade and, by 2060, they expect that more than 30% of the Brazilian population will be 60 years old or more2.
According to the Brazilian National Policy of Elderly Health, most of these elderly people will present some physical and/or mental disability that can impact upon their activities of daily living (ADLs). Therefore, the focus should be on the promotion of health and prevention of disabilities; this may be achieved through the Family Health Strategy (FHS) that works as a bridge between the health system and the elderly3, it has evolved into a robust approach to providing primary care for defined populations by deploying interdisciplinary health care teams. Family health teams are organized geographically, covering populations of up to 1000 households each, with no overlap or gap between catchment areas. Each FHS team member has defined roles and responsibilities, and national guidelines help structure FHS responses to most health problems (Brazil's Family Health Strategy - Delivering Community-Based Primary Care in a Universal Health System.
A few studies have investigated functional capacity in the Brazilian elderly population4-6 and have shown that 19% to 23% are functionally dependent7,8. However, there is not enough evidence regarding the functional capacity of homebound elderly people. Ursine et al.9 suggest that this lack of evidence makes the homebound elderly invisible to the health system and therefore is responsible for a lack of action regarding this population.
In order for new strategies to be developed towards functional dependence of the homebound population, there is a need to understand which factors can predict and influence this functional dependence. Therefore, the objective of this study is to identify the prevalence of functional dependence in homebound elderly people assisted by one Family Health Strategy center in Vitória (State of Espírito Santo); and to determine the influence of sociodemographic and economic factors on the functional dependence of this population.
METHODS
This is a retrospective longitudinal study based on a secondary data analysis of a previous study "Perfil sócio demográfico e de saúde dos idosos restritos ao lar e acamados de uma unidade de saúde da família do Município de Vitória- ES" (number 567.990 EMESCAM Ethical Comitee).
Designed by the national programme for restructuring professional training in health and programme for training working in health (PRO-PET), in cooperation with the Superior School of Health Sciences of the Santa Casa de Misericordia de Vitória (EMESCAM), the State Secretariat of Health, and the Municipal Secretariat of Health of Vitória-ES.
Data were collected from April to November 2014, by structured interviews at the residences of the participants, by physiotherapy, nurse and medical students of EMESCAM. These students underwent specific training by the principal investigator and were always accompanied by a community health agent.
Participants
In February 2014, the Dr José Moyses Family Health Unit had five family health teams that assisted in total 23,080 people. Of these, 4,832 were elderly and 298 were homebound elderly, and it was from this latter population that the sample was recruited. Participants were included if they were 60 years old or more; homebound; with a cognitive level that allowed filling in the questionnaire or with a caregiver that could fill in the questionnaire; lived in the territory served by the Dr. José Moyses Family Health Unit; and signed the consent form.
The participants were classified as homebound if they were incapable of leaving the house by themselves9.
Outcomes
Data were obtained through face-to-face interviews conducted at the participants' residences by EMESCAM's physiotherapy, nursing and medical students, previously trained by the principal investigator. Sociodemographic and economic data were collected using a semistructured form, developed by the authors, that included: age, gender, race, level of education, marital status, number of children, presence of caregiver, place of residence, occupation, family and individual income, contribution to family income, number of people living with them, and place where most of their life was spent.
Functional dependency was assessed by the Functional Independence Measure (FIM) that quantifies the amount of help needed by others to perform ADLs. The FIM scale is considered one of the main scales to assess function in the elderly and has been adopted by the Brazilian Minister of Health as one of the instruments included in the battery of assessments of basic health, used mainly for the assessment of neurological and ageing disability6,10. It was translated and validated for the Brazilian population by Riberto et al.11
The scale contains 18 items measuring two domains, motor and cognitive, and six dimensions (self-care, bladder control, mobility, gait, communication, and social cognition). Data are collected by observations, and reports from the patients or caregivers. Each dimension is scored from 1 (total dependency) to 7 (total independency), with total scores ranging from 18 to 126. Participants with scores of 103 or less were considered as functional dependents12,13.
Since the assessments were conducted in the participant's residence, there was no need to adopt special resources to simulate real life situations; however, it is important to note that if the participant/caregiver was incapable of answering a specific item they would receive a score of 1, as recommended by the Brazilian Ministry of Health.
Statistical Analysis
The Kolgomorov-Smirnov test was used to verify normality of the data. Outcomes were compared between the functionally dependent and functionally independent groups, using the independent t-test for continuous variables and Pearson's chi-square or Fisher's exact test (if the frequency was less than 5 for one cell) for nominal variables.
To determine the extent to which the socioeconomic demographic variables predicted the level of functional dependency, a binary logistic regression was used in which the dependent variable was functional independency (0 independent; 1 dependent) and the independent variables were all the socioeconomic variables that reached the level of p < 0.15 in the "in between" group comparisons.
Regression analysis was conducted using the hierarchal model in which the variables with the lowest p-values in the "in between" groups comparisons were included first. Therefore, the first variable included in the model was presence of caregiver (model 1), followed by place of residence (model 2), place where most of their life was spent (model 3), sex (model 4), family income (model 5), level of education (model 6), age (model 7) and income (model 8). The fit of the model was verified by the omnibus chi-square (p < 0.05) and the Hosmer and Lemeshow tests (p > 0.05). Nagelkerke's R2 indicates the amount of variance in the dependent variable that could be explained by the independent variables. A higher R2 indicates the best model. All analyses were conducted using SPSS software (IBM 22) and the level of significance adopted was p < 0.05.
RESULTS
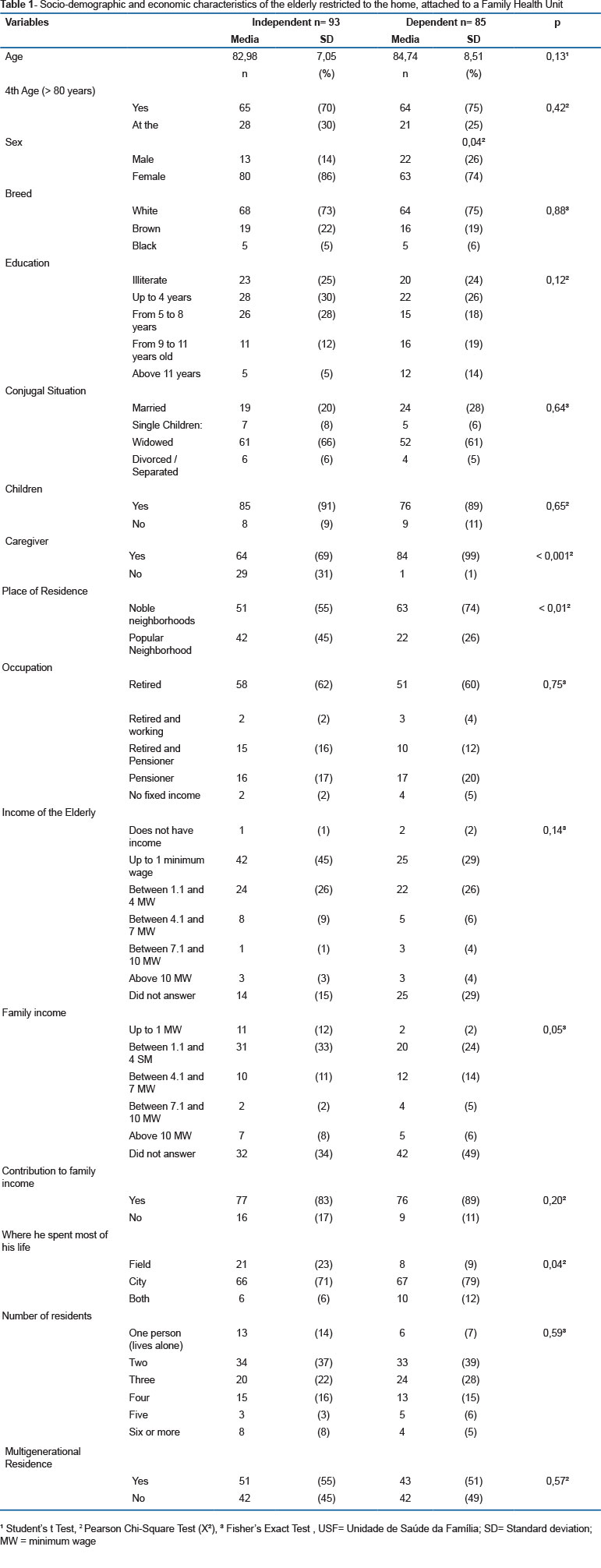
From the 298 homebound elderly available for the study, 178 (60%) fit the inclusion criteria and agreed to participate. The socioeconomic demographics of these participants are displayed in Table 1.
As can be observed, 48% of the participants (85/178) were classified as functionally dependent and 52% as functionally independent. When comparing the socioeconomic demographics between these two groups, there were some important significant differences. The dependent group had fewer women (p = 0.04), spent most of their lives in the city, and lived in high-income neighbourhoods (p < 0.01) when compared to the independent groups. However, the most significant difference was observed for the variable 'presence of caregiver'. Ninety nine percent of the dependent group had caregivers, compared to only 69% of the independent group (p < 0.001).
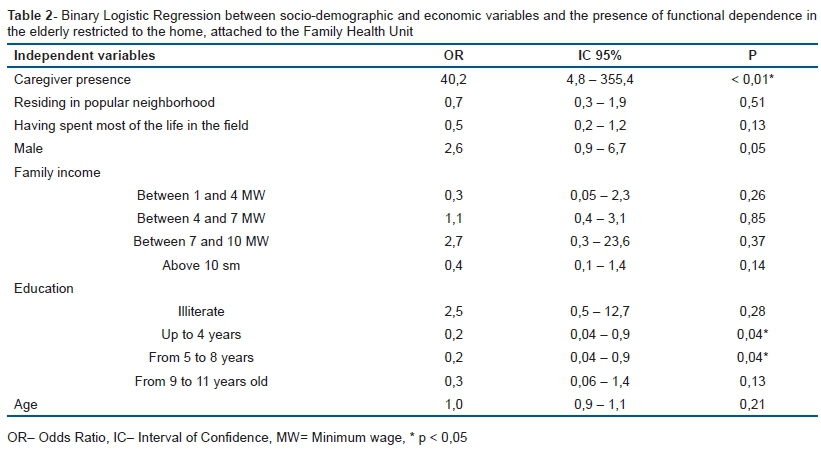
The regression analysis resulted in eight different models but, according to the model fit criteria described in the Methods section, the 7th model showed the best fit (omnibus test: x2 [13] = 56.4, p = 0.00; Hosmer and Lemeshow: x2 [8] = 8.6, p = 0.39) (Table 2).
This r model explained 36% of the variance of functional dependency and included seven independent variables (presence of caregiver; place of residence; place where most of their life was spent; sex; family income; level of education; and age) of which presence of caregiver was a strong and significant predictor. Having a caregiver increased by 40.2 times the chance of being functionally dependent (p < 0.01). It is important to note that being male might also increase the chance of being functionally dependent (OR 2.6, 95%CI 0.9-6.7); however, this was not statistically significant (p = 0.05). Level of education appeared to be a protecting factor; having up to eight years of study decreased the chance of functional dependency (OR = 0,2, 95%CI 0.04-0.9, p = 0.04).
DISCUSSION
According to the World Health Organization14, functional dependency is a consequence of structural and functional deficits caused by chronic degenerative diseases, or external factors, such as falls and fear of falling. The results of this study showed that 48% of the homebound elderly included in the study were functionally dependent. Conversely, evidence provided by the literature shows a higher prevalence of functional dependency among the homebound elderly15 and suggests that the higher the functional dependency, the higher the chance of the person being homebound15,16.
However, the variability among functional independence measurement instruments and procedures makes it difficult to compare prevalence between studies. For example, one study17 classified participants as functional dependents if they had limitations in only one ADL, while others used limitations in two or more ADLs, or used specific validated instruments, such as the FIM6,10.
Macêdo et al.12 applied the FIM using the same cut-off score as in the present study and showed a prevalence of 14.9% of functional dependency among elderly people with cognitive deficits. Ricci et al.13 showed higher prevalences of functional dependency in elderly people assisted by homecare, and also reaffirmed the reliability of the FIM instrument as a measure of functional independency in the elderly, either applied via the caregiver or directly to the patient.
However, even using a specific and validated instrument can lead to misconstruction. For example, some elderly participants might be homebound due to limitations in mobility, yet if the item in the FIM to measure mobility, such as climbing stairs, cannot be tested in the home environment, the participant will receive a score of 1, as suggested by the Brazilian Ministry of Health criteria. However, this score does not indicate that he or she actually has a mobility limitation, just that it was not tested.
Nevertheless, independent of the measurement instrument adopted, the results of the present study raise the question of why these participants are classified as homebound. According to the literature, one of the main reasons to classify an elderly person as homebound is that he or she is functionally dependent10; however, in our sample, less than 50% were actually functionally dependent. Maybe our elderly people are being prematurely and mistakenly classified as homebound and are actually capable of social participation, which suggests that more attention should be given to this population in order to obtain a decent, active and health ageing, as stated by the Brazilian National Policy of Elderly Health3.
The results of the sociodemographic variables showed a high percentage of white, widows and retired female participants in the fourth age (starting at about age 80 or 85) with low levels of education and income who have had children and live in a multigenerational household, with two or more members, and still contribute to the family income. In addition, these participants had spent most of their life in the city and currently live in a high-income neighbourhood and have a caregiver. These characteristics are in agreement with worldwide studies9,16,18,19 and emphasise the feminisation of ageing.
Among all the independent variables influencing functional dependency, having a caregiver was the most significant factor, which suggests that having someone to provide assistance can increase, on average, 40.2 times (CI95% 4.8; 355.4) the chance of being functionally dependent. In accord, Lage et al.20 demonstrated that a higher proportion of functionally dependent elderly have a caregiver in an emergency service in the state of São Paulo; and Gratão et al.6 showed that elderly with caregivers presented lower FIM scores. However, all these studies have cross-sectional designs that do not allow for causation inference between dependent and independent factors and, therefore, we cannot conclude whether elderly people are becoming functionally dependent because they have caregivers, or if the elderly have caregivers due to functional dependency. In addition, the present study did not examine the influence of comorbidities on functional dependency, which could also explain the need for caregivers.
Nevertheless, the literature shows that most caregivers are not prepared to deal with the specific demands of geriatrics6; specifically, caring for chronic diseases and maintaining function21. Therefore, independent of what is causing functional dependency, this should not be seen as stable and irreversible but, instead, as a dynamic and multidimensional condition14 that can be prevented, modified or improved20. In addition, caregivers have an important role and therefore should receive more attention and orientation from health care professionals20.
In the ideal geriatric care process, the person providing assistance should only supervise and encourage the elderly person during an activity, only assisting with or executing the task when strictly necessary. The focus should be on maintaining functional capacity by preserving autonomy and independency and providing a life worth living, as endorsed by the Brazilian National Policy of Elderly Health3.
In order for this to become reality, caregivers should receive training of the process of care by health care professionals who should provide orientations and assistance whilst working alongside the elderly people and their caregivers. Hence, taking into consideration the complexity of geriatric care, and aiming to delay disabilities in this population, the Brazilian National Policy of Elderly Health3 advocates that the Family Health Strategy should be the main facilitator of this process, focusing on the prevention of diseases and promotion of health, and also promoting a bridge between the health system (along with healthcare professionals), the elderly and family members or caregivers.
There has been a continuing increase in the care and attention delivered by the Family Health Strategy to the elderly population in all Brazilian cities22-24. Evidence shows higher benefits among patients cared by Family Health Strategy health centers than to those linked to health centers without the Family Health Strategy25. However, this population still poses many challenges to health care22-24. According to Mota, Aguiar and Caldas22, the major challenge is to address specific elderly care issues with the members of the health team, which suggests a lack of training regarding elderly people's needs. Similarly, Oliveira, Tavares23, and Muniz et al.24 showed the need to train health care professionals regarding the ageing process.
Therefore, it might not be enough to point to the Family Health Strategy as the main facilitator of elderly orientation and care. There is also a need for training and further education of health care professionals to promote their ability to deal with the specific demands imposed by this population. It is also important to discuss this subject in the meetings of municipal health managers in order to encourage implementation and reinforce the international and national strategies working towards active and healthy ageing.
Another important finding of the present study was the association between the level of education, an important socioeconomic factor. The results suggest that having only up to eight years of studies in Brazil decreases the chance of being functionally dependent (OR = 0.2; CI95% 0.04-0.9). However, contrary to our findings, the literature has shown an association between lower level of education and presence of functional dependency6,19.
Low social income has also been associated with less access to health care and poorer health status. However, in respect to function, the present study showed that individuals who lived in low income neighborhoods, and spent most of their lives in rural areas, were less dependent than individuals living in high-income neighbourhoods and who had spent most of their lives in the city (p < 0.01; p = 0.04, respectively). There was also a tendency for low income to be associated with low dependency (p = 0.05).
One explanation might be the role of family members as the main source of care for the elderly population. In low income families, the relative will need to keep working to support the elderly person and may not have the time or the luxury to be absent, partially or completely, from work to provide care; neither will the elderly person have the resources to hire a professional caregiver. Therefore, low income elderly people who do not have someone to count on for helping in daily activities and self-care, might be required to keep functioning as a necessity; and this may delay functional disability.
Another reason for less dependency among poorer, lower educated and rural elderly people might be related to the physical demands of lower income and rural labour, which usually involves intensive physical activity. Since it is well known that maintaining regular physical activity during the whole life is the best way to achieve healthy ageing, the highly intensive labour may have acted as a protective factor against ageing functional disability in this population.
One more interesting finding was the tendency for men to be more functionally dependent then women (OR 2.6; CI95% 0.9-6.7). The lack of significance may be explained by the major difference in proportion between men and women in this sample of 20% and 80%, respectively; there were insufficient numbers of men to allow inferences to be made for sex difference in function. According to Macêdo et al.12, there is a higher tendency for male participants to be functionally dependent and suggests that the lack of statistical significance in this present study was due to a major difference in the number of males (35) compared to females (134). Nerevtheless, other studies8,20 have shown higher dependency among elderly women and have attributed this sex difference to the greater longevity of women compared to men. Since women live longer, they have higher chances of developing disabilities than men. Indeed, in the present study, we noted that the males were on average 3.5 years younger than the females. If we had included older male participants, we might have found a higher proportion of functional dependency among males, maybe even higher than females.
Since functional capacity is an essential component of elderly health, it should be incorporated into health care assessment routines, especially in the Family Health Strategy routine that plays an important role in homebound elderly assistance. The Brazilian Ministry of Health has suggested and provided a variety of specific instruments to assess functional capacity in elderly people. In addition to assessment, promotion of health measures should be taken in order to improve or strengthen functional capacity and, consequently, quality of life26.
Overall, we believe the findings from the present study can be used as a baseline diagnostic assessment to help elaborate actions and plan interventions towards the care of homebound elderly people and of their caregivers. The goal should be to recover, maintain or promote autonomy and functional independency of long-living people, within their family and social context, always respecting the principle and guidelines of the Brazilian Health System as proposed by the Brazilian National Policy of Elderly Health.
Some of the main limitations of the present study are related to the study design and statistical analysis. A cross-sectional design does not provide information about the evolution of elderly functions which could help point to the real causes of functional dependency. Also, the results from regression analysis indicated that the independent variables explained only 36% of the variance of functional dependence. New studies should be designed to try to identify independent factors responsible for the other 64% of variance. We believe that associated comorbidities and geographic limitations might play an important role in functional dependence. Finally, the lack of Brazilian studies investigating homebound elderly people, specifically using the FIM, restricted the discussion of the results. Future studies should also investigate function and its associated factors over time, in order to verify the progression of the outcome in elderly people over the years.
The prevalence of functional dependency in the present study was 48% and having a caregiver was the strongest and most significant factor increasing the chance of being functionally dependent, while high level of education was a protective factor.
REFERENCES
1. World Health Organization (WHO). World health statistics 2014: a wealth of information on global public health. Geneva: WHO; 2014. [ Links ]
2. Instituto Brasileiro de Geografia e Estatística (IBGE). Pesquisa nacional por amostra de domicílios - PNAD 2012. Rio de Janeiro: IBGE; 2013. [ Links ]
3. Brasil. Ministério da Saúde. Portaria nº 2.528, de 19 de outubro de 2006. Institui a Política Nacional de Saúde da Pessoa Idosa. Diário Oficial da União 20 nov. 2006. [ Links ]
4. Mattos IE, do Carmo CN, Santiago LM, Luz LL. Factors associated with functional incapacity in elders living in long stay institutions in Brazil: a cross-sectional study. BMC Geriatr. 2014;14:47. DOI: http://dx.doi.org/10.1186/1471-2318-14-47 [ Links ]
5. Alves LC, Leite IC, Machado CJ. Factors associated with functional disability of elderly in Brazil: a multilevel analysis. Rev Saúde Pública. 2010;44(3):468-78. DOI: http://dx.doi.org/10.1590/S0034-89102010005000009 [ Links ]
6. Gratão ACM, Talmelli LFS, Figueiredo LC, Rosset I, Freitas CP, Rodrigues RAP. Functional dependency of older individuals and caregiver burden. Rev Esc Enferm USP. 2013;47(1):134-41. DOI: http://dx.doi.org/10.1590/S0080-62342013000100017 [ Links ]
7. Guerra RO, Alvarado BE, Zunzunegui MV. Life course, gender and ethnic inequalities in functional disability in a Brazilian urban elderly population. Aging Clin Exp Res. 2008;20(1):53-61. DOI: http://dx.doi.org/10.1007/BF03324748 [ Links ]
8. Parahyba MI, Simões CCS. Disability prevalence among the elderly in Brazil. Cienc Saúde Coletiva. 2006;11(4):967-74. DOI: http://dx.doi.org/10.1590/S1413-81232006000400018 [ Links ]
9. Ursine PGS, Cordeiro HA, Moraes CL. Prevalence of housebound elderly people in the urban region of Belo Horizonte (Minas Gerais, Brazil). Cienc Saúde Coletiva. 2011;16(6):2953-62. DOI: http://dx.doi.org/10.1590/S1413-81232011000600033 [ Links ]
10. Petitpierre NJ, Trombetti A, Carroll I, Michel JP, Herrmann FR. The FIM instrument to identify patients at risk of falling in geriatric wards: a 10-year retrospective study. Age Ageing. 2010;39(3):326-31. DOI: https://doi.org/10.1093/ageing/afq010 [ Links ]
11. Riberto M, Miyazaki MH, Jucá SSH, Sakamoto H, Pinto PPN, Battistella LR. Validation of the Brazilian version of Functional Independence Measure. Acta Fisiatr. 2004;11(2):3-7. DOI: http://dx.doi.org/10.1590/0004-282X20140066 [ Links ]
12. Macêdo AML, Cerquiari EAN, Alvarenga MRM, Faccenda O, Oliveira MAC. Functional assessment of elderly with cognitive deficit. Acta Paul Enferm. 2012;25(3):358-63. DOI: http://dx.doi.org/10.1590/S0103-21002012000300007 [ Links ]
13. Ricci NA, Kubota MT, Cordeiro RC. Agreement between observations on the functional capacity of home care elderly patients. Rev Saúde Públ. 2005;39(4):655-62. DOI: http://dx.doi.org/10.1590/S0034-89102005000400021 [ Links ]
14. World Health Organization (WHO). The International Classification of Functioning, Disability and Health - ICF. Geneva: WHO; 2002. [ Links ]
15. Lopes AB, Gazzola JM, Lemos ND, Riccid NA. Functional independence and factors that influence it in the scope of home care to elderly people. Rev Bras Geriatr e Gerontol. 2007;10(3):285-300. [ Links ]
16. Ornstein KA, Leff B, Covinsky KE, Ritchie CS, Federman AD, Roberts L, et al. Epidemiology of the Homebound Population in the United States. JAMA Intern Med. 2015;175(7):1180-6. DOI: http://dx.doi.org/10.1001/jamainternmed.2015.1849. [ Links ]
17. Doubova Dubova SV, Pérez-Cuevas R, Espinosa-Alarcón P, Flores-Hernández S. Social network types and functional dependency in older adults in Mexico. BMC Public Health. 2010;10:104. DOI: http://dx.doi.org/10.1186/1471-2458-10-104 [ Links ]
18. Musich S, Wang SS, Hawkins K, Yeh CS. Homebound older adults: Prevalence, characteristics, health care utilization and quality of care. Geriatr Nurs. 2015;36(6):445-50. DOI: http://dx.doi.org/10.1016/j.gerinurse.2015.06.013 [ Links ]
19. Sudré MRS, Reiners AAO, Azevedo RCS, Floriano LA. Socioeconomic and health conditions of the elderly assisted by Family Health Teams. Cienc Cuid Saúde. 2015;14(1):933-40. DOI: http://dx.doi.org/10.4025/cienccuidsaude.v14i1.19794 [ Links ]
20. Lage JSS, Okuno MFP, Campanharo CRV, Lopes MCBT, Batista REA. Functional capacity and profile of elderly people at emergency units. REME Rev Min Enferm. 2014;18(4):861-5. [ Links ]
21. Nardi EFR, Sawada NO, Santos JLF. The association between the functional incapacity of the older adult and the family caregiver's burden. Rev Latino-Am Enfermagem. 2013;21(5):1096-103. DOI: http://dx.doi.org/10.1590/S0104-11692013000500012 [ Links ]
22. Mota LB, Aguiar AC, Caldas CP. The Family Health Strategy and healthcare for the elderly: experiences in three Brazilian cities. Cad Saúde Pública. 2011:27(4);779-86. DOI: http://dx.doi.org/10.1590/S0102-311X2011000400017 [ Links ]
23. Oliveira JCA, Tavares DMS. Elderly attention to health strategy in the family: action of nurses. Rev Esc Enferm USP. 2010;44(3):163-70. DOI: http://dx.doi.org/10.1590/S0080-62342010000300032 [ Links ]
24. Muniz EA, Freitas CASL, Alburquerque IMN, Linhares MSC. Home nursing of the elderly in the context of the Family Health Strategy: analysis of scientific production. SONARE. 2014;13(2):86-91. [ Links ]
25. Carvalho VCHS, Rossato SL, Fuchs FD, Harzheim E, Fuchs SC. Assessment of primary health care received by the elderly and health related quality of life: a cross-sectional study. BMC Public Health. 2013;13:605. DOI: http://dx.doi.org/10.1186/1471-2458-13-605 [ Links ]
26. Bezerra IMP, Sorpreso ICE. Concepts and movements in health promotion to guide educational practices. J Hum Growth Dev. 2016;26(1):11-20. DOI: http://dx.doi.org/10.7322/jhgd.113709 [ Links ]
 Correspondence:
Correspondence:
graciellepampolim@hotmail.com
Manuscript received: 25 January 2017
Manuscript accepted: 12 May 2017
Version of record online: 06 September 2017


{kind=link}
{kind=link}