










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores
Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282versão On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.28 no.2 São Paulo maio/ago. 2018
https://doi.org/10.7322/jhgd.147215
ORIGINAL ARTICLE
Characteristics of medication use during lactation
Taís Albano Hernandes; Alessandra Nikaido Fuginami; Enrique Caetano Raimundo; Cristina Peres Cardoso; Elza de Fátima Ribeiro Higa; Carlos Alberto Lazarini
Marília School of Medicine Marília (SP), Brazil
ABSTRACT
INTRODUCTION: The importance of breastfeeding is undisputed. It provides benefits to infants, nursing mothers, families, and society as a whole. The World Health Organization encourages a diet of exclusive breastfeeding until six months of age; however, this routine may be unfeasible for many reasons, one of which is the mother's use of medication.
OBJECTIVE: To characterize medications used by nursing mothers in terms of risk categories, place of care and medical professionals responsible for the prescription, and the extent of medical advice received by the mothers.
METHODS: This is a retrospective, quantitative, and cross-sectional study. The data were collected from Brazil's Family Health Strategies (ESF) program and included information on 161 nursing mothers from 2012 and 2013 and their use of medications while breastfeeding. The data were considered in absolute and relative frequencies and compared to the secondary variables in the study in order to determine whether any associations existed. The chi-square test was applied as part of the analysis.
RESULTS: Of the nursing mothers interviewed, 55.9% reported taking medication. The most frequent groups of medications were those affecting the genito-urinary system and sex hormones, endocrine system, followed by systemic and cardiovascular medications. In the ESF program, general practitioners were the medical professionals who most frequently prescribed medication to these women, followed by gynecologists. Of the women who received prescriptions, 64.4% received some type of medical advice. The statistical analysis revealed a positive correlation between risk category and medical specialty (p=0.03), as well as between risk category and place of care (p=0.001).
CONCLUSION: The most frequently used drug class was that of contraceptives. All medication classified as contraindicated was found to have been prescribed as part of primary care by general practitioners. Thus, these results reflect the need for more qualified professionals throughout Brazil's public health care network.
Keywords: breastfeeding, prescription medications, lactation, maternal-infant health, primary health care.
INTRODUCTION
Breastfeeding is an age-old practice among humans and is influenced by multiple issues, including biological, psychological, spiritual, family-related, environmental, social, and economic factors1.
Breast milk is a complete food that contains vitamins, minerals, fats, sugars, and proteins, and it is recommended for the proper nutrition of newborns. In addition to its nutritional advantages, breast milk promotes the best development of the baby's oral cavity, prevents diarrhea and respiratory infections, and boosts immunological protection, thus decreasing infant mortality2. It also protects against overweight and diabetes throughout life3.
It addition to supplying the baby's nutritional needs, breastfeeding encourages close interaction between mother and child, with benefits for the baby's physiological, cognitive and emotional development4.
Brazilian legislation guarantees women the right to breastfeed their children. The World Health Organization (WHO) and the Brazilian Ministry of Health encourage a diet of exclusive breastfeeding until six months of age and consistent breastfeeding until two years of age, with the gradual introduction of new foods. Brazil's Constitution and public health care laws mandate maternity leave, as well as the right to day care and breastfeeding breaks5. Despite these options and recommendations, early termination of breastfeeding is common6. Premature weaning may lead to delayed neurological and psychomotor development in the first three years of life7.
Many factors may contribute to premature weaning. These include the mother's lack of knowledge on the advantages and importance of breastfeeding8,9, insufficiently trained health care professionals, public policies that only weakly promote breastfeeding, women's increasingly active role in the labor market10, a lack of interest on the part of the newborn, decreased breast milk production and expression, decreased nutritional capacity of the mother's breast milk, physical problems in the breasts11, and the use of medications during lactation12.
Because the use of pharmaceuticals during lactation can contribute to early weaning, the Brazilian Ministry of Health provides guidelines on medications that are safe for consumption during breastfeeding, identifying the drugs according to their category of risk. The categories established by the Brazilian Ministry of Health are compatible with breastfeeding, potential for risk if used during breastfeeding, and contraindicated during breastfeeding13.
Brazil's public primary care system consists of two types of practices: family health care centers, known locally as USFs, and basic health care centers, known locally as UBSs. Most nursing mothers visit USFs for their initial treatment and may visit or be transferred to UBSs or secondary or tertiary care centers for more urgent or specialized care. Care at USFs is provided solely by general practitioners. A previous study found that the most commonly used medications in one UBS, were iron and vitamin supplements (59%), nonsteroidal anti-inflammatory drugs, or NSAIDs (15%), hormones (2%), antibiotics (7%), and antifever medications (2%), with only 1% of patients discontinuing breastfeeding because they needed to use lithium carbonate14. Other drugs responsible for discontinuation included diazepam, which caused sleepiness in the newborn; doxepin, which induced vomiting and jaundice in the baby, and ethinylestradiol, a hormonal contraceptive that has been found to decrease the production of breast milk15.
In another study, also performed at a UBS in Brazil, 80% of the participants used medication during breastfeeding; NSAIDs were the most commonly used (58%), followed by contraceptives (11%) and antianemic drugs (11%). In the study, 58.3% of the nursing mothers received no medical advice regarding the use of medication while breastfeeding16.
According to the Brazilian Ministry of Health, some of these medications are not safe for use while breastfeeding. This risk is compounded by the lack of research on this topic in the country. Thus, medical professionals responsible for prescribing medication to nursing mothers must receive more information in an attempt to improve care for both mothers and babies during this important time. If prescription medication is necessary in this period, the medical professionals must know the factors involved, particularly in terms of the metabolic and physiological aspects of human breast milk, since it is these issues which determine the safety of the drug use during breastfeeding13. Therefore, the motivation for this research was the need for knowledge and training on the use of medications during lactation by all professionals in the health care network who care for breastfeeding women and their children.
In light of these factors, this study sought to characterize the medications taken by nursing mothers in terms of risk categories, places and medical professionals responsible for the prescription, and the medical advice received by the mothers.
METHODS
This was a cross-sectional, retrospective, and quantitative study performed in a city located in the central-western region of São Paulo State, the population of which is approximately 230,000 inhabitants.
The subjects were mothers who met the inclusion criteria: they were patients enrolled in Brazil's Family Health Strategies (ESF) program who had breastfed in 2012 and 2013. The sample size was calculated using the following statistical parameters: total live births in the southern region of the city (the region which had the highest number of births; n=467), a sampling error of 5%, a 95% confidence level and a maximum percentage of 78%; thus, 161 nursing mothers were required.
Data was collected through at-home interviews using a standardized and semi-structured questionnaire adapted from Fragoso et al.17 Data was collected on sociodemographic characteristics (mother's age, level of schooling, and age of the baby) and medications (use, drug class, prescribing physician's medical specialty, place of prescription, and advice received on use during breastfeeding).
Patients were excluded from the study if they missed more than three medical visits and if they changed the USF in which they were enrolled.
In order to identify the medications, the researcher asked each nursing mother to present all of the medications she was taking. The categories into which the drugs were classified were those provided by the Anatomical Therapeutic Chemical Classification System (ATC)18. After their identification, the drugs were classified by risk of use during breastfeeding19.
The data were processed and analyzed using the SPSS Software, version 17.0. Sociodemographic variables and variables involving the medications are presented as absolute and relative frequencies. Category of risk was treated as an independent variable and was compared to the following dependent variables: the stage of lactation during which the medication was prescribed, the prescribing physician's medical specialty, the place where the prescription was made, and whether the nursing mother received medical advice. The chi-square test was used to determine any associations between the variables. Associations between variables were considered statistically significant when p≤0.05.
The study was approved by the Research Ethics Committee of the Marília School of Medicine under case number 133.616 and by the Municipal Research Assessment Board run by the Municipal Health Secretariat (COMAP) under case number 373/12-SS.
RESULTS
The sociodemographic data of the 161 participants revealed a predominance of patients between 20 and 29 years of age and a majority of patients who had completed high school as their highest level of schooling.
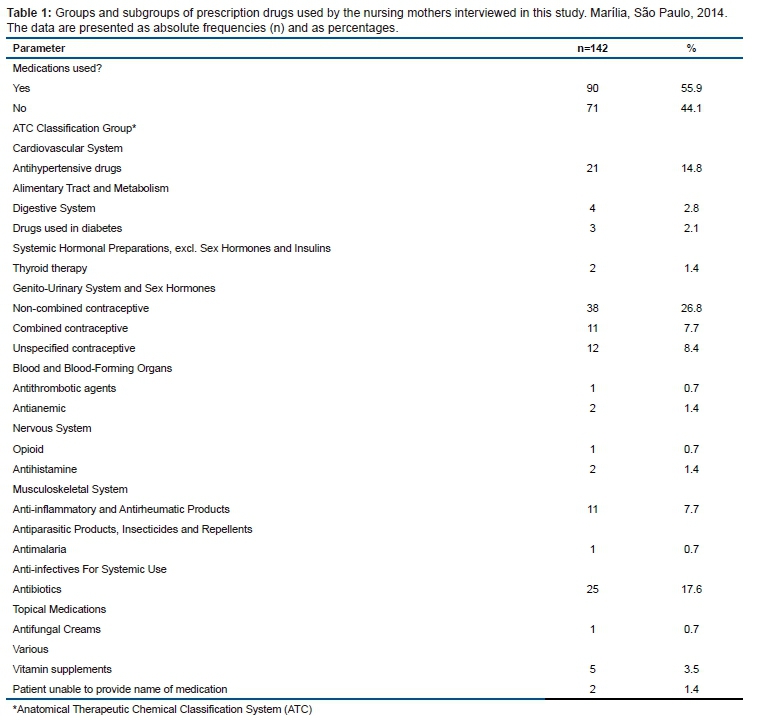
Most subjects reported having used some type of medication while breastfeeding. Table 1 describes the 142 prescription drugs that were used by the mothers interviewed. The most commonly used drugs were those in the hormonal system ATC group, followed by the anti-infectives for systemic use group and the cardiovascular system group.
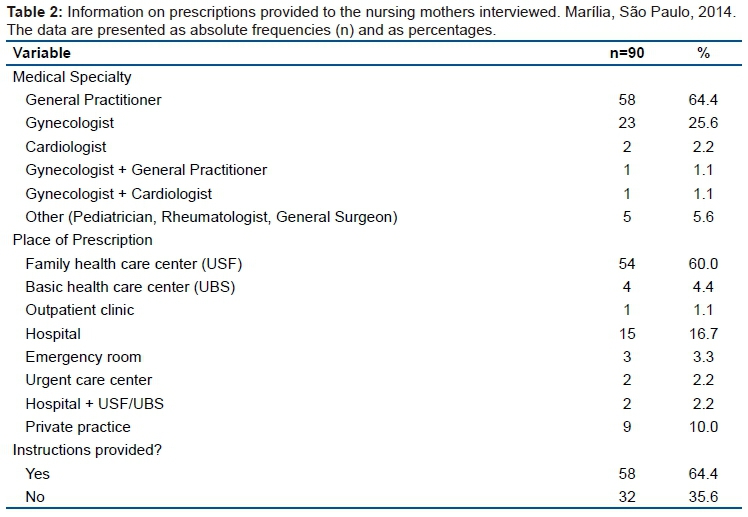
General practitioners were the most common medical specialists to prescribe drugs to these mothers, followed by gynecologists. Most of the prescriptions were provided at USFs, followed by UBSs. Most of the interviewees received some type of medical advice regarding which medications were safe to use while breastfeeding (Table 2).
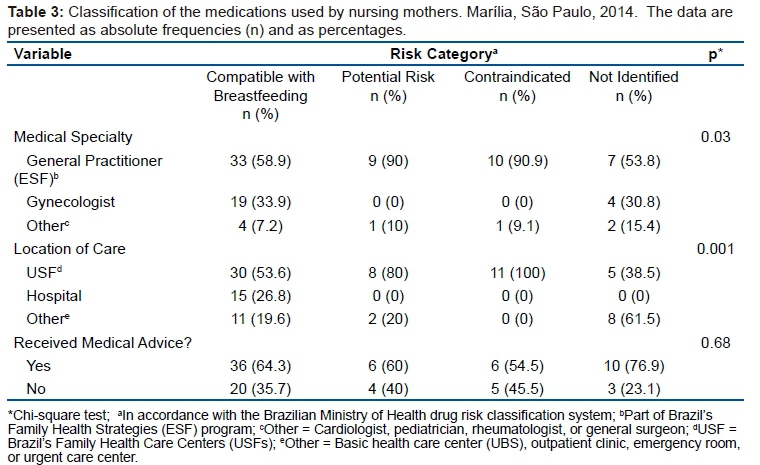
The statistical analysis showed a positive correlation between risk classification and the variables representing the prescribing physician's specialty and the place of care. The highest percentages of prescriptions of drugs with potential for risk if used during breastfeeding and of drugs contraindicated during breastfeeding were made by general practitioners in the ESF program (Table 3).
DISCUSSION
The socioeconomic data on the patients' age and level of schooling in the present study resemble those from a study performed in the state of Rio de Janeiro, in which the majority of patients were between 21 and 30 years of age and in which the highest level of schooling of 46% of the patients was a completed high school education17. Variables such as age and schooling have been described as factors associated with early weaning; studies have suggested that the lower the mother's level of schooling, the earlier the weaning tends to take place20. In agreement with these findings, another cross-sectional study demonstrated that mothers with less schooling are more likely to introduce foods in their children's diet prematurely21. It is also worth mentioning that marital status can also be a determinant of early weaning. Married women seem to be more likely to breastfeed22. As detailed in Table 1, the interviews revealed that 90 of the nursing mothers (55.9%) used prescription medications. These data are slightly lower than those observed in a study on nursing mothers treated at a public hospital, in which 78% of the mothers reported using prescribed medication17. The current findings were also lower than those in a study on nursing mothers treated at a UBS (80%)16. In these previous studies, the most commonly prescribed medications were NSAIDs, prescriptions for which ranged from 58%16 to 61.5%17.
In a cross-sectional study on mothers of infants less than 6 months of age treated in UBSs in the inland cities of São Paulo State, 93% of the medications the mothers used had been prescribed to them. The most common prescriptions were for vitamins and iron supplements (59%); antibiotics and antihypertensive drugs totaled only 2% and 1%, respectively14. According to a study carried out in a clinic in the Netherlands, 65.9% of 451 breastfeeding women used some type of medication, while 40.8% used vitamin supplements, and 7.1% oral contraceptives23.
In the current study, the most commonly used medications were oral contraceptives, followed by antibiotics and antihypertensive drugs. The high percentage of contraceptive use may be a factor of the predominantly young age of the nursing mothers involved in the study, most of whom were still of childbearing potential. We consider it important to classify contraceptives as combined or non-combined, since the former are contraindicated during lactation: the presence of the estrogen component compromises the breast milk production13.
In our study, 7.7% of the contraceptives prescribed were combined. However, 8.4% of the women interviewed were unable to specify which contraceptive they used. According to the Brazilian Ministry of Health's risk categories, the antihypertensive drugs and antibiotics prescribed to the women in this study have a potential for risk if used during breastfeeding. Furthermore, 12.2% of the nursing mothers used contraindicated drugs in this period. This finding differed from a study on mothers treated at the hospital level, where all of the drugs prescribed were in the Ministry of Health's "compatible with breastfeeding" category17. In general, studies show that most women use prescription drugs during lactation, but different drug classes are used at different rates, and study results may be influenced by country, the number of nursing mothers considered, and the type of health care service or center where the data is obtained.
As Table 2 details, most of the medications were prescribed to the women in this study by general practitioners. The nursing mothers interviewed in the present study were treated as part of the ESF program, but the results go against the purpose and proposals of Brazil's primary health care system: given the longitudinal nature of the program, the point of this care is not to limit prevention measures only to the prescription of medication24; both primary and secondary prevention measures must be prioritized. Though Brazil's USFs do not have gynecologists on staff, the presence of the gynecologists in the data can be explained by the fact that some of the nursing mothers interviewed were treated in a hospital setting.
In the interviews, 64.4% of the mothers reported having received some kind of medical advice. This rate was similar to those in the literature, in which 76.9% of the mothers were advised on the use of the drugs by doctors or nurses17,20.
Table 3 demonstrates that drug risk classification was positively correlated with the prescribing physician's medical specialty and with the place of care. As mentioned previously, all medication classified as contraindicated was found to have been prescribed as part of primary care (in a local UBS or USF) by general practitioners. This behavior may be a factor of the prescribing physician's medical education, since general practitioners do not routinely have experience with breastfeeding mothers and the types of medications considered safe for them. The presence of gynecologists may have contributed to the lack of contraindicated prescriptions in the other places of care, since OBGYNs are theoretically more qualified to manage these medications during this phase of patients' lives. According to recommendations from the Brazilian Ministry of Health, when pharmacological treatment is required during breastfeeding, the risks to the health of the mother and the child be carefully evaluated so that mothers can be appropriately treated without interrupting breastfeeding19.
The statistical analysis showed no positive correlation between medical advice being given and the risk category of the medications prescribed (Table 3). However, nine nursing mothers received prescriptions for drugs classified as contraindicated or having the potential for risk if used during breastfeeding. These erroneous prescriptions reflect the need for better training for professionals involved in treating nursing mothers, who require specialized care25.
CONCLUSION
In terms of sociodemographic data, most of the nursing mothers interviewed in this study were under thirty years of age and had a high-school-level education. The most frequently used drug class was that of contraceptives. Because approximately one fifth of the mothers interviewed reported using combined contraceptives, which are contraindicated by the Brazilian Ministry of Health, and because close to one third of the mothers were prescribed drugs that had a potential for risk if used during breastfeeding, these results reflect the importance of improving the quality of care when it comes to prescribing medications to this population. One limitation of this study is the lack of information on the likely medical issues experienced by these patients, which may have been able to explain the prescription of contraindicated pharmaceuticals.
This study provides evidence that most of the patients interviewed received medical advice regarding the use of medication while breastfeeding, and also that every case in which contraindicated medication was prescribed occurred in a visit with a general practitioner as part of primary care.
These results therefore reflect the need for qualified professionals throughout Brazil's public health care network, since more properly trained professionals will provide more accurate prescriptions and advice regarding the use of medication that is compatible with breastfeeding and will therefore provide better care to both mothers and children.
REFERENCES
1. Corintio MN. Manual de aleitamento materno. 3ª ed. São Paulo: FEBRASGO, 2015. [ Links ]
2. Moura ERBB, Florentino ECL, Bezerra MEB, Machado ALG. Investigação dos fatores sociais que interferem na duração do aleitamento materno exclusivo. Rev Intert. 2015;8(2):94-116. DOI: http://dx.doi.org/10.22280/revintervol8ed2.203 [ Links ]
3. Victora CG, Barros AJD, França GVA, Bahl R, Horton S, Krasevec J, et al. Amamentação no século 21: epidemiologia, mecanismos, e efeitos ao longo da vida. Epidemiol Serv Saúde. 2016;1-24. [ Links ]
4. Dias EG, Alves JCS, Santos MRA, Pereira PG. Prevalência do aleitamento materno exclusivo até o sexto mês no município de Mamonas-MG em 2013. Rev Contexto Saúde. 2015;15(29):81-90. DOI: http://dx.doi.org/10.21527/2176-7114.2015.29.81-90 [ Links ]
5. Brasil. Ministério da Saúde. Centro Brasileiro de Análise e Planejamento. Pesquisa nacional demográfica e saúde da criança e da mulher PNDS 2006: dimensões do processo reprodutivo e da saúde da criança. [cited 2017 Nov 20] Available from: http://bvsms.saude.gov.br/bvs/publicacoes/pnds_crianca_mulher.pdf. [ Links ]
6. Prado CVC, Fabbro MRC, Ferreira GI. Desmame precoce na perspectiva de puérperas: uma abordagem dialógica. Texto Contexto Enferm. 2016;25(2):e1580015. DOI: http://dx.doi.org/10.1590/0104-07072016001580015 [ Links ]
7. Severiano AAO, Dantas DS, Oliveira VLC, Lopes JM, Souza DE, Magalhães AG. Associação entre amamentação, fatores obstétricos e o desenvolvimento infantil de crianças do interior do nordeste brasileiro. J Hum Growth Dev. 2017;27(2):158-65. DOI: http://dx.doi.org/10.7322/jhgd.114483 [ Links ]
8. Fonseca-Machado MO, Haas VJ, Stefanello J, Nakano AMS, Gomes-Sponholz F. Aleitamento materno: conhecimento e prática. Rev Esc Enferm USP. 2012;46(4):809-15. DOI: http://dx.doi.org/10.1590/S0080-62342012000400004 [ Links ]
9. Silva NM, Waterkemper R, Silva EF, Cordova FP, Bonilha ALL. Conhecimento de puérperas sobre amamentação exclusiva. Rev Bras Enferm. 2014;67(2):290-5. DOI: http://dx.doi.org/10.5935/0034-7167.20140039 [ Links ]
10. Silva CA, Davim RMB. Mulher trabalhadora e fatores que interferem na amamentação: revisão integrativa. Rev Rene. 2012;13(5):1208-1217. DOI: http://dx.doi.org/10.15253/rev%20rene.v13i5.4143 [ Links ]
11. Hernandes TA, Fuginami AN, Raimundo EC, Cardoso CP, Higa EFR, Lazarini CA. Significado e dificuldades da amamentação: representação social das mães. Rev Psicol Diversid Saúde. 2017;6(4):247-57. DOI: http://dx.doi.org/10.17267/2317-3394rpds.v6i4.1692 [ Links ]
12. Barbosa JAG, Santos FPC, Silva PMC. Fatores associados à baixa adesão ao aleitamento materno exclusivo e ao desmame precoce. Rev Tecer. 2013;6(11):154-65. DOI: http://dx.doi.org/10.15601/1983-7631/rt.v6n11p154-16 [ Links ]
13. Brasil. Ministério da Saúde. Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Saúde da criança: aleitamento materno e alimentação complementar. 2ed. Brasília: Ministério da Saúde, 2015. [ Links ]
14. Del Ciampo LA, Ferraz IS, Daneluzzi JC, Ricco RG, Martinelli Junior CE. Aleitamento materno e uso de medicamentos durante a lactação. Rev Paul Pediatr. 2007;25(4):355-7. DOI: http://dx.doi.org/10.1590/S0103-05822007000400010 [ Links ]
15. Queiroz RFC, Santos SLF, Pessoa CV, Borges RN, Barros KBT. Aleitamento materno e uso de medicamentos por puérperas em um município do estado do Ceará. Bol Inform Geum. 2015;6(3):7-14. [ Links ]
16. Mota LS, Chaves EMC, Barbosa RCM, Amaral JF, Farias LM, Almeida, PC. Uso de medicamentos durante a lactação por usuárias de uma unidade básica de saúde. Rev Rene. 2013;14(1):139-47. DOI: http://dx.doi.org/10.15253/rev%20rene.v14i1.3344 [ Links ]
17. Fragoso VMS, Silva ED, Mota JM. Lactantes em tratamento medicamentoso da rede pública de saúde. Rev Bras Promoç Saúde. 2014;27(2):283-90. DOI: http://dx.doi.org/10.5020/18061230.2014.p283 [ Links ]
18. World Health Organization (WHO). Collaborating Centre for Drug Statistics Methodology. Guidelines for ATC classification and DDD assignment 2013. Oslo: 2012 [cited 2017 Oct 4]. Available from: https://www.whocc.no/filearchive/publications/1_2013guidelines.pdf. [ Links ]
19. Brasil. Ministério da Saúde. Secretaria de Atenção à Saúde. Departamento de ações pragmáticas e estratégicas. Amamentação e uso de medicamentos e outras substâncias. 2ed. Brasília: Ministério da Saúde, 2014. [cited 2018 Fev 12]. Available from: bvsms.saude.gov.br/bvs/publicacoes/amamentacao_uso_medicamentos_outras_substancias.pdf. [ Links ]
20. Teter MSH, Oselame GB, Neves EB. Amamentação e desmame precoce em lactantes de Curitiba. Espaço Saúde. 2015;16(4):55-63. DOI: http://dx.doi.org/10.22421/1517-7130.2015v16n4p54 [ Links ]
21. Pereira RSV, Oliveira MIC, Andrade CLT, Brito AS. Fatores associados ao aleitamento materno exclusivo: o papel do cuidado na atenção básica. Cad Saúde Pública. 2010;26(12):2343-54. DOI: http://dx.doi.org/10.1590/S0102-311X2010001200013 [ Links ]
22. Dodt RCM, Ferreira AMV, Nascimento LA, Macêdo AC, Joventino ES, Ximenes LB. Influência de estratégia de educação em saúde mediada por álbum seriado sobre a autoeficácia materna para amamentar. Texto Contexto Enferm. 2013;22(3):610-8. DOI: http://dx.doi.org/10.1590/S0104-07072013000300006 [ Links ]
23.E Schirm E, Schwagermann MP, Tobi H, Jong-van den Berg LT. Drug use during breastfeeding. Eur J Clin Nutr. 2004;58(2):386-90. DOI: http://dx.doi.org/10.1038/sj.ejcn.1601799 [ Links ]
24. Vitoi NC, Fogal AS, Nascimento CM, Franceschini SCC, Ribeiro AQ. Prevalência e fatores associados ao diabetes em idosos no município de Viçosa, Minas Gerais. Rev Bras Epidemiol. 2015;18(4):953-65. DOI: http://dx.doi.org/10.1590/1980-5497201500040022 [ Links ]
25. Maciel JMMP, Ramos AGB. Uso de medicamentos durante a lactação: um fator para a suspenção do aleitamemento materno. Rev Pesq Interdiscipl. 2017;(2):504-13. DOI: http://dx.doi.org/10.24219/rpi.v2i2.274 [ Links ]
 Correspondence:
Correspondence:
Carlos Alberto Lazarini
lazarini@famema.br
Manuscript received: January 2018
Manuscript accepted: April 2018
Version of record online: June 2018


{kind=link}
{kind=link}
{kind=link}