










Serviços Personalizados
artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282versão On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.28 no.2 São Paulo maio/ago. 2018
http://dx.doi.org/10.7322/jhgd.141627
ORIGINAL ARTICLE
Nutritional status of children from lower Amazonas: agreement between three classification criteria
Marcelo Gonçalves DuarteI; Sueyla Ferreira da Silva dos SantosI; Giseli MinattoII; Glauber Carvalho NobreII, III; João Otacilio Libardoni dos SantosI; Thiago Ferreira de SousaIV; Ismael Freitas JuniorV
IDepartamento de Educação Física, Universidade Federal do Amazonas, Parintins (AM), Brasil
IIDepartamento de Educação Física, Universidade Federal de Santa Catarina, Florianópolis (SC), Brasil
IIIInstituto Federal de Educação, Ciências e Tecnologia do Ceará, Fortaleza (CE), Brasil
IVDepartamento de Educação Física, Universidade Federal do Triângulo Mineiro, Uberaba (MG), Brasil
VDepartamento de Educação Física, Universidade Estadual Julio Mesquita Filho, Presidente Prudente (SP), Brasil
ABSTRACT
INTRODUCTION: The knowledge of adequate methods to monitor growth and nutritional status during childhood and adolescence makes possible an early diagnosis of possible problems, such as malnutrition, overweight or obesity in adult life.
OBJECTIVE: To determine the agreement between three methods of nutritional assessment status of children 2 to 6 years old from Lower Amazonas region, Brazil.
METHODS: Exploratory, epidemiological, and cross-sectional school-based study conducted in 2014 with children of Child Education in the city of Parintins. We assessed the nutritional status, body mass index, according to three criteria: Conde and Monteiro, Cole et al, and World Health Organization (WHO). We used the Kappa coefficient to investigate the agreement between three criteria.
RESULTS: Participants were 1.387 children (714 boys) with a mean age of 5 years. The boys had a higher prevalence of overweight than girls by the WHO classification, but higher proportion of girls with low weight, according to the national criteria. The best levels of agreement were for females and national protocol showed good agreement with the international use of protocols, highlighting proposed by the WHO.
CONCLUSION: We concluded that there was agreement among the criteria for assessing the nutritional status of children in the Lower Amazonas.
Keywords: preschoolers, body mass index, anthropometry, nutrition assessment.
INTRODUCTION
The assessment of nutritional status is fundamental in childhood, since malnutrition, overweight and obesity are stages indicative of imbalances that may influence the adequate development of children and interfere in health/disease processes1,2. There is a significant increase in infectious diseases, retarded motor development, difficulties in school performance, decrease in height and productive capacity in adulthood3, resulting from this multifactorial aspect. Social and biological factors are related to the deficit or excess of food consumption4. Therefore, genetic factors and environmental and social context characteristics play an important role on nutritional status5.
Emerging countries have undergone intense changes in lifestyle and nutritional status4. Brazil is among the countries with the highest prevalence of malnutrition, but this aspect presents important regional disparities, as pointed out in the book "Geography of Hunger", by Josué de Castro, cited as one of the pioneers and principals on mapping the situation of the country. The regions of the Amazon and part of the Northeast were considered as expressive zones of endemic hunger6. In these regions, hunger or nutritional deficiencies affected half the population6.
The northern region of Brazil is one of the most vulnerable to children's nutritional deficits7,8, where the highest prevalence of stature deficit9 is also found, an aspect that is predominantly associated with precarious living conditions10. Among the forms of measurement of nutritional status, we have the body mass index (BMI) as a commonly used method because it is considered practical and low cost11. For the evaluation of BMI, different classification criteria are available that allow the estimation of health risks, through the categories of low weight and obesity12-15. The researches pointed out that the evaluation of nutritional status diverges considerably from the criteria used16-18.
The World Health Organization15 suggests as a criterion for the classification of nutritional status the z-score or percentiles of body weight for height15, such criterion was proposed from a study carried out in four continents15. Cole et al.13,14 reported new BMI curves for the age group of two to 18 years, using data from nationally representative surveys of six high and middle income countries (Brazil, Singapore, United States, Great Britain, Hong Kong and the Netherlands). Conde and Monteiro12 carried out a national study that evaluated the nutritional status of children and adolescents19.
In the present study, we have not investigated the use of different classification criteria in research on the nutritional status of children in the northern region of Brazil. Thus, the present study aims to estimate the concordance between three methods of nutritional status classification, through BMI, in children aged two to six years of age in the region of Baixo Amazonas, Brazil.
METHODS
Participants
An exploratory, epidemiological study with a cross-sectional design, developed in 2014 with public elementary school children in the city of Parintins, Amazonas. The research was submitted and approved by the Research Ethics Committee (CEP) in humans of the Universidade Federal do Amazonas- UFAM under the number of opinion 860.883.
The study population was determined by total enrolment in pre-schools in the previous year of data collections. According to data from the Brazilian Institute of Geography and Statistics (IBGE), 3,955 enrolments were made20. A consent form was obtained from the directors of each teaching institution included in the sample, in the same way, parents and / or guardians of the students involved in the research signed a free and informed consent form authorizing the participation of their children.
The total number of schools eligible for participation in the survey was 13. It was decided to carry out a school census, including all children, in the analysis, who met the following criteria: a) aged from two to six years; b) enrolled in kindergarten schools in the urban area of the municipality of Parintins/Amazonas in the academic year 2014; c) have the consent of the parents or guardians to perform the data collection. For schoolchildren who attended kindergarten, but did not meet the age group criterion, the measurements were taken.
Procedures
The data collection team was composed of a teacher and two students of Physical Education properly trained and standardized to carry out the measurements. A pilot study was carried out involving 60 students from two classes of a school not included in the sample, with the intention of testing the instruments and the logistics of the study. During the present study, parents and/or guardians of the students were informed at least one day in advance about the research and the appropriate clothing to participate in the collection of data. The measurements were taken during recreation classes, which occurred twice a week and in the same class shift. Data collection took place from August to November 2014.
The body mass was measured by means of a calibrated scale with an accuracy of 0.1 kg. The stature was collected with a tape measure with precision of 0.1 cm, fixed to the wall, on a flat support surface and with the aid of a square overlapped to the children's head and supported to the wall. The measurement was made with light clothing (shorts or pants, school shirt) and barefoot21. Most of the measurements were performed by a single evaluator, with the help of another team member. The BMI calculation was applied by dividing body mass in kilograms (kg) by the square of height in meters (m).
The outcome variable of the study was the nutritional status, classified according to three BMI criteria for children: Conde and Monteiro12, Cole et al.13,14 e World Health Organization (WHO)15,22. The BMI classification for the present study was standardized as presented in Figure 1, in order to allow comparability between the criteria.
The independent variables of the study were the age group, calculated from the date of birth and the evaluation, later categorized in tertiles, and sex (male and female). The statistical program SPSS, version 15.0 was used to build the database and conduct analyses. The descriptive statistics, by means of mean, standard deviation (±), absolute and relative frequencies, were applied to characterize the group and describe the nutritional status of the children in each of the adopted classification criteria. The association between BMI classification and gender for the three classification criteria was obtained using the chi-square test.
Statistical analysis
The independent variables of the study were the age group, calculated from the date of birth and the evaluation, later categorized in tertiles, and sex (male and female). The results were described by mean, standard deviation, absolute and relative frequencies. The chi-square test was used to verify possible associations between BMI classification and gender for the three classification criteria. The concordance between the selected nutritional status criteria was verified by the weighted Kappa test for the general sample and by sex. The FleissKappa test was used to verify the agreement between the classification categories (low weight, eutrophic, overweight and obesity). The values between 0.21 and 0.4 were considered as discrete agreement; moderate 0.41 to 0.6; substantial 0.61 to 0.8 and almost perfect 0.81 to 1.0023. The significance level of 5%.
RESULTS
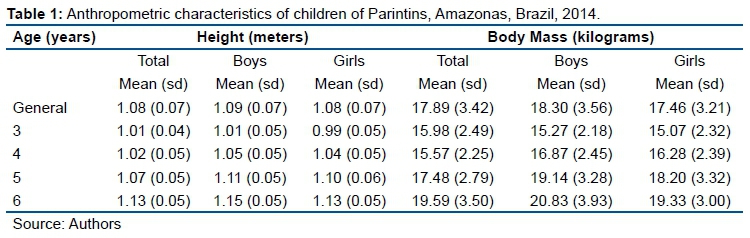
Of the 13 preschools located in Parintins, eight (61.5%) participated in the study. A total of 1,387 children (35.1% response rate) were evaluated from three to six years (mean: 5.11; ± 0.86). The mean height was 1.08 m (± 0.07) and the body mass was 17.89 kg (± 3.42) (Table 1).
The majority of the children were male (51.5%) and BMI in the range recommended for health. Regarding each criterion, it was observed that Cole et al.13,14 presented a prevalence of low weight (26%) distinct from the other criteria, and overweight (12.9%), by means of WHO classification15, 22presented a higher prevalence (Table 2).
The association between nutritional status and sex, according to the three BMI classification criteria, showed a difference between boys and girls, with a higher proportion of overweight and obesity for boys (p = 0.006), in WHO classification15,22 and of low weight for girls (p = 0.004), that of Conde and Monteiro12 (Table 2).
Table 3 shows the concordance between the three criteria of classification of BMI, general and by sex, with values from k= 0.473 p <0.001 (discrete) to k= 0.707 p <0.001 (substantial). The lowest values of agreement were observed in males, in all the criteria. The Brazilian protocol of Conde and Monteiro12 presented satisfactory agreement with the WHO classifications15,22 and Cole et al.13,14, both male (WHO15 0.67; Cole et al.13 0.43) and female (WHO22 0.72, Cole et al.14 0.65) (Table 3).
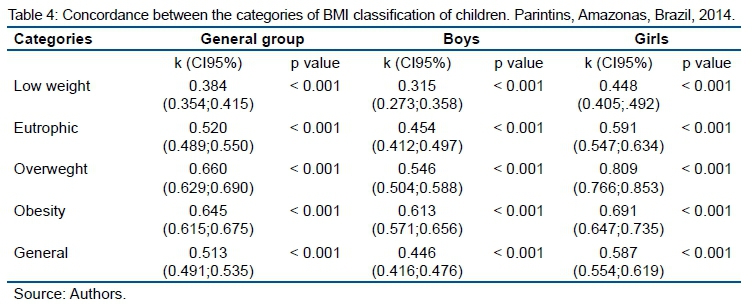
Fleisskappa analyzes showed moderate and significant agreement for most of the classification categories (k= 0.520 to 0.691, p <0.001). The "low weight" category showed low agreement for the group in general (k= 0.384 p <0.001). The "overweight" classification presented substantial agreement between the protocols in the female group (k= 0.809, p <0.001) (Table 4).
DISCUSSION
Although an evident nutritional transition occurs in Brazil, which causes an increase in overweight and obesity in pre-school children24-27. In this study, high prevalence's of nutritional deficits were observed. It was noted in the context of the Lower Amazon region, the double demand for health directed to the control of body weight and infant malnutrition.
When comparing the weight and height measures of the sample of children aged three to six years, from this research, with the estimation of the Brazilian population for the same age by the Family Budget Survey (POF), in the years 2008 and 200928, the anthropometric characteristics of the children of Amazonas are lower than the national average, for both sexes. The highest percentage discrepancies between the sample of this study and the Brazilian infant population were observed at the age of six years, with a difference of 3.0 cm for boys and 5.0 cm for girls in mean height, and less than 1.37 kg for boys and 2.87 kg for girls in mean body weight28.
Despite the recognition of the indigenous Sateré-Mawé indigenous ethnic group of the Brazilian Amazon that belongs to the Tupi linguistic trunk and inhabit the Andirá-Marau Indigenous Territory, on the border of the states of Amazonas and Pará, with a population estimated at approximately 7.5 thousand people29 of the children of the Lower Amazon, the potential of child growth involves, besides the genetic component, the influence of external and modifiable factors, such as breastfeeding, housing and feeding conditions in the first years of life30. Currently, through the accumulation of follow-up studies conducted by the United Nations Children's Fund (UNICEF) with Eastern peoples, African ethnicities and Latin American, it is difficult to affirm the preponderant power of genetic potential for child growth5.
National surveys with indigenous people10,31,32 evidenced characteristics similar to those observed in this study. Guarani children, living in the states of São Paulo and Rio de Janeiro, Brazil,presented a prevalence of low weight for the age of 7.9%32, similar to that observed in children from quilombola regions and from different rural communities in the Pará region (6.25%)32 and higher than the survey conducted in Mato Grosso with Xavante children under 5 (4.5%)31.
In an epidemiological study conducted in Manaus with children (zero to 10 years old), prevalences of underweight were higher than expected in all age groups, with height-for-age deficits (17.5%) being the most compromised8. In Socoraba, São Paulo, a quasi-experimental study with children (three to 72 months of age) of families with low purchasing power33, the relevance of the attendance to the day care center was observed as a determinant condition for the children's growth, and the adequacy of the weight for height was higher among children over two years old.
National studies10 and others with urban populations8,34, rural and indigenous32 in the northern region warned of the influence of living conditions on nutritional and anthropometric aspects, such as low infant height. The adhesion of needy families to income distribution programs and the improvement of quality of school meals can be identified as contributory strategies for the eradication of child malnutrition and other nutritional deficiencies35.
The classification by Cole et al.13,14 indicated a prevalence of underweight, statistically higher than that reported in the WHO classifications15,22 and Conde e Monteiro12. This result corroborates the Barbosa et al.16 study, comparing the classifications of Cole et al.13,14, Conde Monteiro12 and the Centers for Disease Control (CDC). Excess weight in the present study was higher in the WHO classification16,23 among the children of Parintins. Other studies with preschool children, comparing different criteria for classification of nutritional status, also observed higher prevalences of overweight by WHO classification18,36. These growth curves were identified as the most sensitive to identify obesity in a cardiovascular risk population when compared to the National Center of Health Statistics (NCHS) and CDC curves37.
In the survey on the health and nutritional conditions of the infantile population of the state of Amazonas, the prevalence of acute malnutrition in the capital and in the interior was 4.6% and 3.5% respectively34. As for overweight for height, prevalences were 7.7% in the capital and 4.3% in the interior34. These prevalences for the infant population of Amazonas were lower than those found in children in the Lower Amazon region, both for malnutrition and for overweight, which indicates an important public health issue.
In day care centers in the city of Manaus, Amazonas, children (two to seven years old) from private day care centers were more frequently overweight than those in public day care centers. On the other hand, children at public day-care centers were more prone to low weight for age and height38. In rural communities in the state of Pará, Brazil, the prevalence of overweight and obesity was 22.9%, which32 characterizes the alteration of the nutritional status of children in the northern region.
In a study carried out in the southeast region, in the state of São Paulo, it was verified that in children from private schools the prevalence of overweight was 35.4%, higher than the national average of the Brazilian population39. In public and private school surveys, overweight was 11.3% among preschool children, but there were differences between the type of institution, with higher prevalences of overweight and obesity being found in private preschools39.
In this study, female children presented a higher proportion of overweight according to WHO criteria15,22, and of low weight according to the classification of Conde and Monteiro12 for boys. In research conducted in the northern region, no differences were found for these classifications of nutritional status for sex38. Among the indigenous population, a divergent result was found, indigenous boys (two to 10 years old) Pakanóva (Wari'), from Rondônia, presented a higher frequency of low weight, using the curves of NCHS40.
The national classification criterion of Conde and Monteiro12 presented satisfactory agreement with the international criteria of Cole et al.13,14 and WHO15,22. In the sex-stratified evaluation, data from this study indicated that the lowest coefficients for all the evaluated criteria were for the male sex. Barbosa et al.16, in research with children (five to 10 years old) also found that the choice of the Brazilian criterion of classification of BMI does not interfere in the comparison with other international criteria.
In an international study with indigenous children of school age, using the criteria of the CDC, WHO, International Obesity Task Force (IOTF), to find out the adequacy of these three criteria, in children aged eight to 14 years, found a higher level of agreement between the CDC and IOTF protocols, however, substantial WHO compliance was maintained for IOTF and CDC17. In a national survey with pre-school children in the city of Viçosa, Minas Gerais, the WHO curves presented higher sensitivity values when compared to CDC and NCHS, in addition to good agreement for both sexes for NCHS18.
Thus, it was concluded that the best concordance indexes were found for the national population criterion of Conde and Monteiro12, on the other hand, the level of agreement was higher for females in all criteria. Thus, the results suggest the use of the national criterion of Conde and Monteiro12 to evaluate the nutritional status of children from the Lower Amazon or similar populations that live with nutritional problems associated with malnutrition and obesity in a concurrent way.
The nutritional status of the children of the Lower Amazon, characterized in this study, characterizes a double risk scenario of nutritional problems: on the one hand, the deficit of stature and malnutrition and, on the other hand, the prevalence of excess weight. The female children presented significantly higher proportions for both factors mentioned above, according to WHO15,22 criteria and Conde e Monteiro12.
As a limitation of this study, the sampling procedure, which, even though it was at random, was not proportional by educational sectors and excluded schools located in rural or riverside regions, on the other hand a representative sample of the pre-school population was reached of the city of Parintins, Amazonas, Brazil. The study demonstrates the importance of selecting criteria for assessing the nutritional status of the research population and contributes to the interpretation of these indicators for populations with multiple nutritional risks due to dietary habits and socioeconomic factors.
The results point to the need to implement health interventions aimed at improving eating habits that cause overweight and obesity; and the reduction of social inequities that lead to the state of malnutrition and growth deficit. Maintaining and improving the reach of distribution and income generation policies, as well as the quality of food offered in schools and the provision of nutritional counseling for schoolchildren are recommended to improve the nutritional state of children.
REFERENCES
1. Bismarck-NasrEM, Frutuoso MFP, Gamabardella AMD. Efeitos tardios do baixo peso ao nascer. Rev Bras Crescimento Desenvolv Hum. 2008;18(1):98-103. DOI: http://dx.doi.org/10.7322/jhgd.19871 [ Links ]
2.Singh AS, Mulder C, Twisk JWR, Mechelen W, Chinapaw MJ. Tracking of childhood overweight into adulthood: a systematic review of the literature. Obes Ver. 2008; 9(5):474-488. DOI: http://dx.doi.org/10.1111/j.1467-789X.2008.00475.x [ Links ]
3. Monteiro CA, Conde WL. Tendência secular da desnutrição e da obesidade na infância na cidade de São Paulo (1974-1996). Rev Saúde Pública. 2000;34(6):52-61. DOI: http://dx.doi.org/10.1590/S0034-89102000000700008 [ Links ]
4. Escoda MSQ. Para a crítica da transição nutricional. Ciênc Saúde Coletiva. 2002;7(2):219-26. DOI: http://dx.doi.org/10.1590/S1413-81232002000200002 [ Links ]
5. Fundo das Nações Unidas para a Infância (UNICEF). Situação mundial da infância. Brasília: UNICEF; 2000. [ Links ]
6. Castro J. Geografia da fome. 11ª ed. Rio de Janeiro: Griphus, 1992. [ Links ]
7. Araujo TS, Oliveira CSM, Muniz PT, Silva-Nunes M, Cardoso MA. Desnutrição infantil em um dos municípios de maior risco nutricional do Brasil: estudo de base populacional na Amazônia Ocidental Brasileira. Rev Bras Epidemiol. 2016;19(3):554-66. DOI: https://doi.org/10.1590/1980-5497201600030007 [ Links ]
8. Tavares BM, Veiga GV, Yuyama LKO, Bueno MB, Fisberg RM, Fisberg M. Estado nutricional e consumo de energia e nutrientes de pré escolares que frequentam creches no município de Manaus, Amazonas: existem diferenças entre creches públicas e privadas? Rev Paul Pediatr. 2012;30(1):42-50. DOI: http://dx.doi.org/10.1590/S0103-05822012000100007 [ Links ]
9. Instituto Brasileiro de Geografia e Estatística (IBGE). Pesquisa de Orçamento Familiar 2008 - 2009. Antropometria e estado nutricional de crianças, adolescentes e adultos no Brasil. [cited 2016 Sep 14] Available from: http://www.ibge.gov.br/home/estatistica/populacao/condicaodevida/pof/2008_ 2009_encaa/pof_20082009_encaa.pdf. [ Links ]
10. Barreto CTG, Cardoso AM, Coimbra Jr CEA. Estado nutricional de crianças indígenas Guarani nos estados do Rio de Janeiro e São Paulo, Brasil. Cad Saúde Pública. 2014;30(3):657-62. DOI: http://dx.doi.org/10.1590/0102-311X00117813 [ Links ]
11. Organização Mundial de Saúde (OMS). Physical status: the use and interpretation of anthropometry. Geneva: WHO, 1995. [ Links ]
12. Conde WL, Monteiro CA. Body mass index cutoff points for evaluation of nutritional status in Brazilian children and adolescents. J Pediatr. 2006;82(4):266-72. DOI: http://dx.doi.org/10.2223/JPED.1502 [ Links ]
13. Cole TJ, Bellizzi MC, Flegal KM, Dietz WH. Establishing a standard definition for child overweight and obesity worldwide: international survey. BMJ. 2000; 320:1240. DOI: https://dx.doi.org/10.1136/bmj.320.7244.1240 [ Links ]
14. Cole TJ, Flegal KM, Nicholls D, Jackson A. Body mass index cut offs to define thinness in children and adolescents: international survey. BMJ. 2007;335:194. DOI: https://dx.doi.org/10.1136/bmj.39238.399444.55 [ Links ]
15. WHO Multicentre Growth Reference Study Group. Child Growth Standards based on length/height, weight and age. Acta Paediatr Suppl. 2006;450:76-85. DOI: https://dx.doi.org/10.1080/08035320500495548 [ Links ]
16. Barbosa RMS, Soares EA, Lanzillotti HS. Avaliação do estado nutricional de escolares segundo três referências. Rev Paul Pediatr. 2009;27(3):243-50. DOI: http://dx.doi.org/10.1590/S0103-05822009000300003 [ Links ]
17. Medehouenou TCM, Ayotte P, St-Jean A, Meziou S, Roy C, Muckle G, et al. Overweight and obesity prevalence among school-aged nunavik inuit children according to three body mass index classification systems. J Adolescent Health. 2015;57(1): 31-6. DOI: http://dx.doi.org/10.1016/j.jadohealth.2015.03.022 [ Links ]
18. Sperandio N, Sant'ana LFR, Franceschini SCC, Priore SE. Comparação do estado nutricional infantil com utilização de diferentes curvas de crescimento. Rev Nutr. 2011; 24(4):565-74. DOI: http://dx.doi.org/10.1590/S1415-527320110004000 [ Links ]
19. Instituto Brasileiro de Geografia e Estatística, Fundo das Nações Unidas para a Infância. Perfil estatístico de crianças e mães no Brasil: aspectos de saúde e nutrição de crianças no Brasil. Rio de Janeiro: IBGE; 1992. [cited 2016 Sep 26] Available from: biblioteca.ibge.gov.br/biblioteca-catalogo.html?view=detalhes&id22297 [ Links ]
20. Instituto Brasileiro de Geografia e Estatística (IBGE). Ensino - matrículas, docentes e rede escolar. [cited 2015 Sep 14] Available from: http://www.cidades.ibge.gov.br/xtras/grafico_cidades.php?lang=&codmun=130340&idt ema=117&search=amazonas|parintins|ensino-matriculas-docentes-e-rede-escolar-2012. [ Links ]
21. Alvarez BR, Pavan AL. Alturas e comprimentos. In: Petroski EL. Antropometria: técnicas e padronizações. 5ed. Várzea Paulista: Fontoura; 2011, p.31-44. [ Links ]
22. World Health Organization (WHO). Growth reference data for 5 -19 years. [cited 2015 Sep 29] Available from: http://www.who.int/growthref/who2007_bmi_for_age/en/index.html [ Links ]
23. Batista Filho M, Rissin A. A transição nutricional no Brasil: tendências regionais e temporais. Cad Saúde Pública. 2003;19(Suppl.1):181-91.DOI: http://dx.doi.org/10.1590/S0102-311X2003000700019 [ Links ]
24. Landis JR, Kock GG. The measurements of observer agreement for categorical data. Biometrics. 1977;33(3):159-74. DOI: http://dx.doi.org/10.2307/2529310 [ Links ]
25. Schuch I, Castro TG, Vasconcelos FAG, Dutra CLC, Goldani MZ. Excesso de peso em crianças de pré-escolas: prevalência e fatores associados. J Pediatr. 2013; 89(2):179-88. DOI: http://dx.doi.org/10.1016/j.jped.2013.03.003 [ Links ]
26.Alencar MSS, Barros SEL, Borges IS, Cavalcante KN, Melo MTSM, Nunes IFOC, et al. Adequações e inadequações nos perfis antropométrico e dietético de crianças pré-escolares. J Hum Growth Dev. 2016;26(2):234-42. DOI: http://dx.doi.org/10.7322/jhgd.119290 [ Links ]
27. Freitas AG, Lima DG, Bortolini MJS, Meneguetti DUO, Santos EFS, Macedo Junior H, et al. Comparação do estado nutricional em crianças de cinco a dez anos de idade beneficiárias do Programa de transferência de dinheiro condicional nos Estados do Acre e do Rio Grande do Sul, Brasil. J Hum Growth Dev. 2017;27(1):35-41. DOI: http://dx.doi.org/10.7322/jhgd.121206 [ Links ]
28. Instituto Brasileiro de Geografia e Estatística (IBGE). Pesquisa de Orçamento Familiar 2008 - 2009. Antropometria e Estado Nutricional de Crianças, Adolescentes e Adultos no Brasil. [cited 2015 Oct 10] Available from: http://www.ibge.gov.br/home/estatistica/populacao/condicaodevida/pof/2008_ 2009_encaa/pof_20082009_encaa.pdf. [ Links ]
29. Teixeira P, Brasil M. Estudo Demográfico dos Sateré-Mawé: um exemplo de censo participativo. In: Pagliaro H, Azevedo MM, Santos RV. Demografia dos Povos Indígenas no Brasil. Rio de Janeiro: FIOCRUZ; 2005, p.135-54. [ Links ]
30. Moro D. Birthweight and breast feeding of babies during the war in one municipal area of Sarajevo. Eur J Clin Nutr. 1995;49(Suppl.2):S37-9. [ Links ]
31. Ferreira AA, Coimbra Junior CEA, Gugelmin SA. Estado nutricional e fatores associados ao crescimento de crianças indígenas Xavante, Mato Grosso. Dissertação (Mestradro) - Fundação Oswaldo Cruz. Rio de Janeiro: 2009. [ Links ]
32. Guimarães RCR, Silva HP. Estado nutricional e crescimento de crianças quilombolas de diferentes comunidades do Estado do Pará. Amazôn Rev Antropol. 2015;7(1):186-209. DOI: http://dx.doi.org/10.18542/amazonica.v7i1.2156 [ Links ]
33. Segall-Corrêa AM, Gonçalves NNS, Chalita LVAS, Russo-Leite GP, Padovani CR, Gonçalves A. Determinantes da evolução do peso e altura em crianças de 3 meses a 6 anos assistidas em creche: análise por modelo linear não hierarquizado em ensaio quase-experimental. Rev Panam Salud Publica. 2002;12(1):19-25. [ Links ]
34. Secretaria de Estado da Saúde do Amazonas (SUSAM), Instituto Nacional de Pesquisas da Amazônia (INPA), ENSP/Fiocruz e Universidades do Estado do Amazonas. Chamada nutricional para crianças menores de cinco anos de idade do Estado do Amazonas, 2006. [cited 2015 Sep 14] Available from: http://aplicacoes.mds.gov.br/sagi/PainelPEI/Publicacoes/Sum%C3%A1rio%20Exec utivo%20Chamada%20Nutricional%20Amazonas.pdf. [ Links ]
35. Brasil. Ministério da Saúde. Política nacional de alimentação e nutrição. Brasília: Ministério da Saúde, 2012. [ Links ]
36. Bueno MB, Fisberg RM. Comparação de três critérios de classificação de sobrepeso e obesidade entre pré-escolares. Rev Bras Saúde Matern Infant. 2006;6(4):411-8. DOI: http://dx.doi.org/10.1590/S1519-38292006000400008 [ Links ]
37. Oliveira GJ, Barbiero SM, Cesa CC, Pellanda LC. Comparação das curvas NCHS, CDC e OMS em crianças com risco cardiovascular. Rev Assoc Med Bras. 2013;59(4):375-80. DOI: http://dx.doi.org/10.1016/j.ramb.2013.02.001 [ Links ]
38. Tavares BM, Veiga GV, Yuyama LKO, Bueno MB, Fisberg RM, Fisberg M. Estado nutricional e consumo de energia e nutrientes de pré escolares que frequentam creches no município de Manaus, Amazonas: existem diferenças entre creches públicas e privadas? Rev Paul Pediatr. 2012;30(1):42-50. DOI: http://dx.doi.org/10.1590/S0103-05822012000100007 [ Links ]
39. Nascimento VG, Schoeps DO, Souza SB, Souza JMP, Leone C. Risco de sobrepeso e excesso de peso em crianças de pré-escolas privadas e filantrópicas. Rev Assoc Med Bras, 2011;57(6):657-61. DOI: http://dx.doi.org/10.1590/S0104-42302011000600012 [ Links ]
40. Escobar AL, Santos RV, Coimbra Jr CEA. Avaliação Nutricional de Crianças Indígenas Pakaanóva (Wari´), Rondônia, Brasil. Rev Bras Saúde Matern Infant. 2003;3(4):457-61. DOI: http://dx.doi.org/10.1590/S1519-38292003000400010 [ Links ]
 Correspondence:
Correspondence:
Marcelo Gonçalves Duarte
duartemg@gmail.com
Manuscript received: December 2017
Manuscript accepted: March 2018
Version of record online: June 2018


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}