










Serviços Personalizados
artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282versão On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.29 no.1 São Paulo abr. 2019
http://dx.doi.org/10.7322/jhgd.157755
ORIGINAL ARTICLE
http://dx.doi.org/10.7322/jhgd.157755
Mortality due to traffic accidents, before and after the reduction of the average speed of motor vehicles in the city of São Paulo, Brazil, from 2010 to 2016
Pablo de Almeida LeitãoI; Italla Maria Pinheiro BezerraI, III; Edige Felipe de Sousa SantosI, II; Silmara de Lira RibeiroI; Jéssica Miwa TakasuI; Juliana Spat CarlessoI; Marcelo Ferraz CamposI; Luiz Carlos de Abreu.I
ILaboratório de Delineamento de Estudos e Escrita Científica. Faculdade de Medicina do ABC, Santo André, São Paulo, Brasil
IIDepartamento de Epidemiologia. Faculdade de Saúde Pública da Universidade de São Paulo (USP). São Paulo (SP), Brasil
IIIPrograma de Pós-graduação em Serviço Social. Escola de Ciências da Santa Casa de Misericórdia de Vitoria (EMESCAM), Vitória, ES, Brasil
ABSTRACT
INTRODUCTION: Traffic accidents represent a relevant global public health problem and are associated with behavioral factors, vehicle maintenance, urban space precariousness and traffic surveillance. They are important causes of morbidity and mortality due to the increasing number of vehicles and changes in lifestyle and risk behaviors in the general population
OBJECTIVE: To analyze mortality numbers due to land transport accidents reported in the city of São Paulo, Brazil, before and after the decline of average speed of motor vehicles
METHODS: A study of temporal series was carried out using official database provided by the Sistema de Informação sobre Mortalidade. Data was collected according to the type of occurrence and place of residence in São Paulo, SP, Brazil. Other sources of data were Death Certificates. Population data was collected by the foundation SEADE for the other years used, and data from 2010 was collected by the Instituto Brasileiro de Geografia e Estatística do Brasil (IBGE), the Brazilian institute of geography and statistics. More death data has been collected using the tenth review of the WHO International Classification of Diseases (V00- V89) for overall population and were stratified in age groups (<10 years, 10-19 years, 20-49 years, 50 years and more), city (São Paulo) and the year timetable (2010, 2011, 2012, 2013, 2014, 2015 and 2016). The data was calculated based on plain death rate and standardized, for gender and age group. The measures of mortality were used for the construction of temporal series by the regression model of Prais-Winsten. All the analysis were made through the statistics program Stata 14.0
RESULTS: Reportedly, 7288 deaths occurred due to land accidents in São Paulo, the state's capital, between 2010 and 2016. The higher proportion of deaths happened between men with age between 20-49 years, brownish skin color, marital status single, between 4 e 7 years of study. 72.55% of deaths happened within of hospitals and/or other health establishments. The deaths ranged 1.200 in 2010 and went down to 779 in 2016. The standard mortality for transport accidents between 2010 and 2016 fluctuated from 10.04 to 6.29 for every 100 thousand inhabitants
CONCLUSION: There was a decrease in deaths related to traffic accidents in individuals over 20 years of age. After the reduction of the average speed of motor vehicles in the city of São Paulo, the decline in mortality due to traffic accidents was more pronounced among individuals aged 50 years or older, with significant differences for men and women
Keywords: accidents traffic, mortality, underlying cause of death, motor vehicles, epidemiology.
Why was this study done?
The objective of this study was to evaluate traffic accident mortality in the city of São Paulo, before and after the reduction of the average speed of motor vehicles. Thus, the study was done to evaluate the longitudinal effect of intervention of a health policy on mortality due to traffic accidents between men and women and age groups during 2010-2016.
What did the researchers do and find?
The researchers developed an ecological time-series study using the Prais-Winsten regression model for interrupted time series and segmented regression analysis. This statistical analysis is considered the most effective non-experimental resource to evaluate the longitudinal effect of health interventions. Thus, a reduction in deaths related to traffic accidents was observed in individuals over 20 years of age. After reducing the average speed of motor vehicles in the city of São Paulo, the decline in mortality due to traffic accidents was more pronounced among individuals aged 50 years or more, with differences for men and women.
What do these findings mean?
The results indicate a favorable evaluation of the "mean velocity reduction" intervention, suggesting that the decline in mortality between 2010-2016 was intensified after the implementation period of the "average speed reduction" intervention (2015 onward), benefiting mainly the highest risk groups: men and people aged 50 years and over.
INTRODUCTION
Traffic accidents are the third-highest cause of death in the world. For the 20 years, there have been major changes in Brazil, especially in terms of advances in the automobile industries, that have generated multiplier effects of urban and social transformations. All these advances and technological changes allowed the growth of the city to happen in a disorderly way, without adequate infrastructure, and the urban centres did not accommodate for the increase in the number of vehicles. The unsatisfactory quality of public transport has led people to opt for individual means of transport, which has led to traffic problems in large cities1.
The acquisition of these means of transport for work or leisure by a large part of the population has brought, to a large extent, negative consequences, given the large number of accidents with these vehicles with generally severe traumas, which do not lead to death, leave sequels, most of the time, disabling, leading to the problematic to be considered as a serious public health problem2.
Traffic accidents represent a relevant global public health problem and are associated with behavioural factors, vehicle safety and the precariousness of urban space. They are important causes of morbidity and mortality due to the increasing number of vehicles, changes in lifestyle and risky behaviours in the general population3.
As a result of the significant increase in vehicles and the high frequency of inappropriate behaviour among drivers, these accidents have become a major cause of trauma, multi-traumas and death, especially among the young population4.
According to World Health Organization (WHO) estimates in the year, there were 1.24 million road deaths, when the world population was approximately 6.79 billion. There were 18 deaths per 100,000 inhabitants5.
In Brazil, the numbers are even more alarming: in 2013, according to sources from the Department of Information Technology of the Unified Health System6, the number is 21 deaths per 100,000 inhabitants. The Brazilian population was 201.3 million, and there was an average of 42,300 road transport deaths that year.
In São Paulo, although the numbers are smaller than the world and national averages, with reference to the year 2013 and a population of 43.6 million inhabitants, there were 6,564 road deaths that year or 15 deaths per 100,000 inhabitants, three times smaller than the world average and six than the national6.
Traffic accidents are considered one of the expressions of violence that violate social relations in traffic situations and may or may not have the intentionality of their perpetrators. In other words, they may be caused by the recklessness of the drivers who know the limits of speed and the condition of sobriety necessary for driving vehicles but intentionally ignore them; or they may result from unintentional problems such as mechanical failures in the vehicles or the public roadway signalling system7.
The health damages from these accidents can reach varied dimensions, resulting in physical and emotional repercussions which reduce the quality of life at individual and collective levels and generate overloads in the health services. External causes require more complex hospital procedures, with a greater number of surgeries, the need for intensive care, drug consumption and multi-professional support, resulting in higher costs of health services8.
Studying mortality rates due to traffic accidents becomes paramount for identifying related factors in order to prevent injuries and reduce the number of such accidents. In addition, it can awaken the critical-scientific sense of professionals working in health and education so that they can carry out activities that enable the reduction of the impacts to the general population due to traffic violence.
Thus, the objective of this study is to analyse mortality from traffic accidents reported in the city of São Paulo, Brazil, before and after reducing the average speed of motor vehicles.
METHODS
The method employed is a time-series study9 using official microdata of mortality by place of occurrence and residence from the Accidents of Transit (AT) recorded in the city of São Paulo, Brazil, in the Mortality Information System. This system makes the data available through the website (www.datasus.gov.br) of the Department of Information Technology of the Unified Health System (DATASUS)6. The data of the deaths correspond to the period between 1 January 2010 and 31 December 2016.
Database and Study Population
All deaths occurred in the city of São Paulo and included residents of the same city whose basic cause of death was classified as a traffic accident. The information was extracted from the death certificate, the basic document of the Mortality Information System (SIM) that records, analyses, processes and makes available data on deaths due to natural causes and external causes and is therefore a system that records all deaths occurring in São Paulo, Brazil. This data was extracted through the file transfer system and was later converted to a database through the TabWin program. Population data were obtained by means of estimates made by the Foundation State System of Data Analysis (SEADE) Foundation for the intercensities years and for the 2010 census by the Brazilian Institute of Geography and Statistics of Brazil (IBGE)10.
The data were extracted from DATASUS by two trained researchers designated by the authors, and a third investigator was responsible for correcting possible discrepancies.
Study Variables
Data from car accident deaths were collected using the tenth revision of the International Classification of Diseases (V00-V89) and were stratified by sex (male and female), age groups (<10 years, 10-19 years, 20-49 years, 50 years and more), municipality (São Paulo) and calendar years (2010, 2011, 2012, 2013, 2014, 2015 and 2016). Excluded were deaths of children under one year of age.
Statistical Analysis
The study population consisted of people who died due to accidents of transit. Gross and standardized mortality rates by age group were calculated using the World Health Organization's standard world population between 2000-202510 for the total population, as well as crude mortality rates by sex and age group.
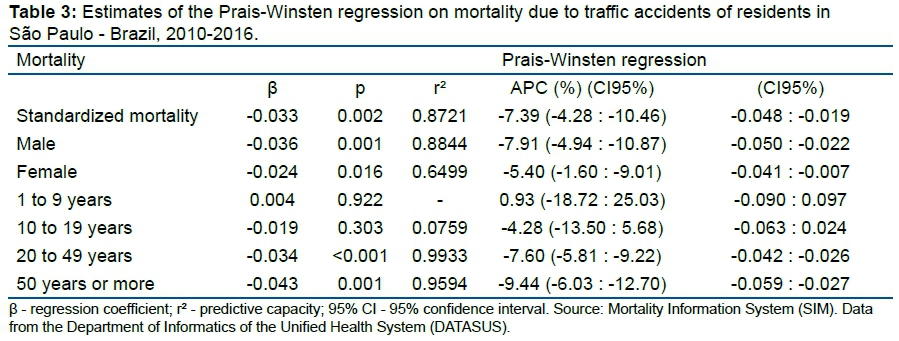
For the analysis of the temporal tendency of the grievance, we followed the methodological indications presented9. Thus, we used the mortality measures to construct time series using the Prais-Winsten regression model, which allows for first-order autocorrelation to be corrected in the analysis of time series of values. Thus, the following values were estimated: angular coefficient (β) and respective probability (p); coefficient of determination (r2); and a confidence interval of 95%.
This procedure made it possible to classify the mortality by traffic accidents , discriminated by sex and age, as increasing, decreasing or stationary, in addition to quantifying the Annual Percent Change (APC). All analyses were performed in the statistical program Stata 14.0.
RESULTS
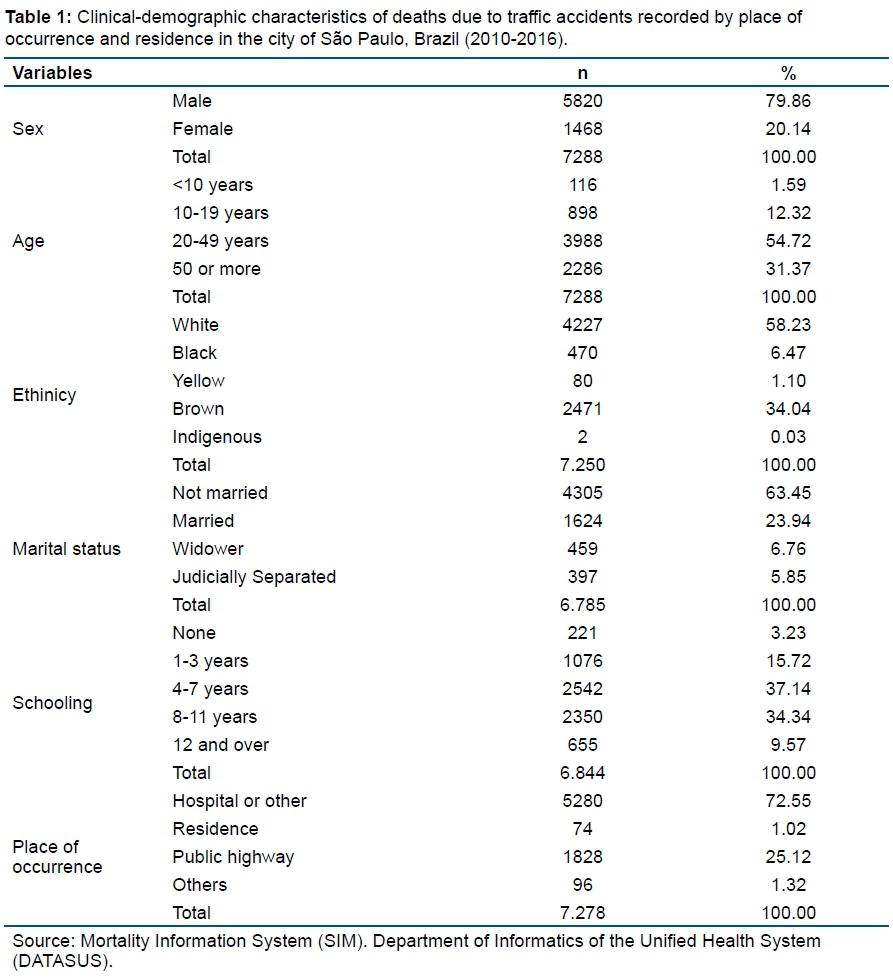
A total of 7,288 residents of the city of São Paulo died in traffic accidents during the period 2010 to 2016. The highest proportion of deaths occurred among males aged 20-49 years whose colour of skin was brown and who had between four and seven years of schooling. A total of 72.55% of deaths occurred in hospitals and/or other health facilities (Table 1).
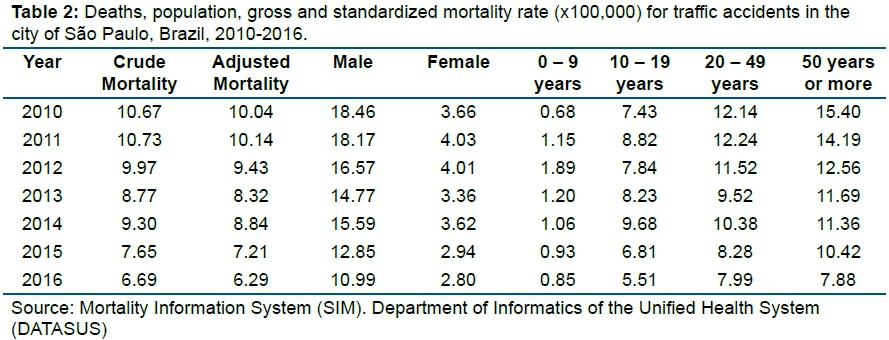
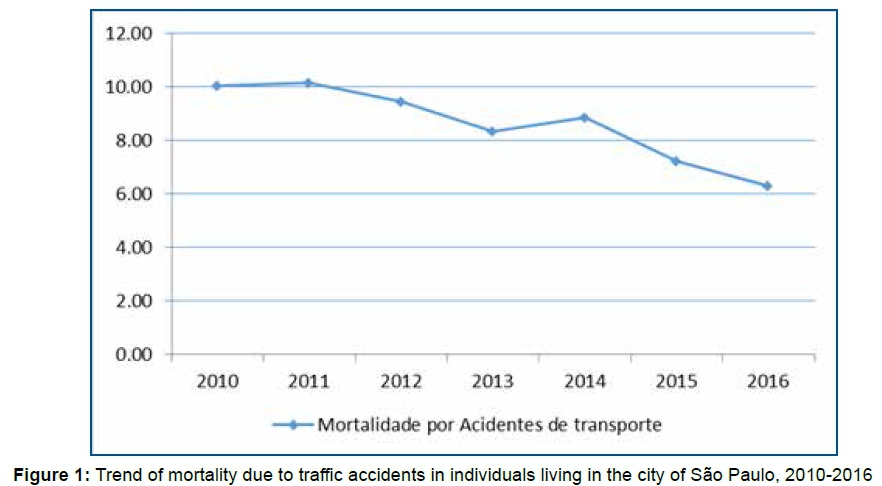
Deaths ranged from 1,200 in 2010 to 779 in 2016. The standardized mortality by traffic accidents between 2010 and 2016 ranged from 10.04 to 6.29 per 100,000 inhabitants. Mortality was always higher among men and ranged from 18.46 to 10.99 per 100,000 inhabitants, while mortality among women ranged from 3.66 to 2.80 per 100,000 inhabitants (Table 2).
The trend of deaths due to traffic accidents was decreasing during the study period, and until 2014, the Annual Percent Change (APC) was -4.92% per year, whereas from 2015, the APC was -7.38% year. From 2015 onwards, there was an intensification in the reduction of mortality due to traffic accidents in the city of São Paulo (Table 3).
The reduction during the period of overall mortality among men, women and individuals aged 20 to 49 years was interrupted in 2014, decreasing again from 2015 onwards (Table 2, Figures 2 and 3).
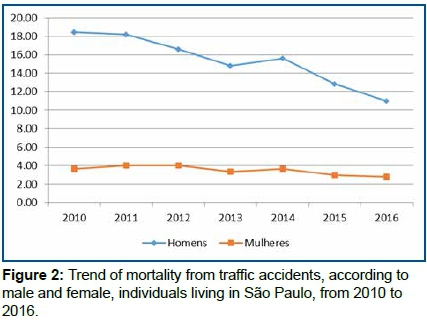
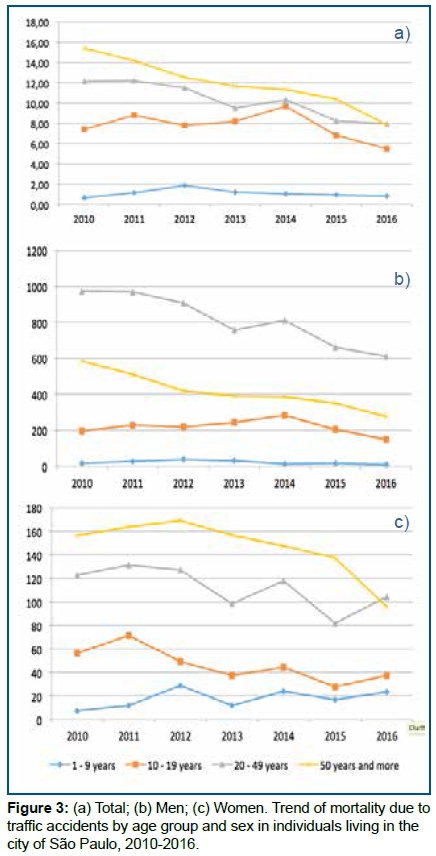
The stratified analysis by sex showed a reduction in mortality due to traffic accidents among men (APC: -7.91%) and women (APC: -5.40%), while an analysis stratified by age showed a reduction after 20 years of age. Mortality remained constant among individuals younger than 20 years (p > 0.05) (Table 3).
When both sexes were analyzed, the mortality trend due to traffic accidents was decreasing for individuals 20 years of age or older. A reduction was observed among people aged 50 years or over (APC: -9.44%). Among men, mortality was declining after 20 years of age. However, it was observed that among adolescents from 10 to 19 years of age there was a gradual increase in deaths during 2010-2014, declining from 2015 (p = 0.027). Mortality was decreasing for women aged 10-49 years during 2010-2016. In addition, women over 50 years old had a significant reduction in mortality due to traffic accidents from 2015 (p = 0.009) (Table 3, figure 3).
DISCUSSION
The results showed that 6,577 individuals living in the city of São Paulo, Brazil, died due to traffic accidents during the period 2010 to 2014. The mortality rate due to traffic accidents ranged from 13.8 to 12.3 deaths/100,000 inhabitants, with a proportional mortality rate of 2% on average. Proportional mortality ranged from 2.22% to 1.91%. The majority of the individuals who died were male, aged between 20-49 years, single, white and having less than 12 years of education. The chance of mortality due to traffic accidents for whites corresponds to 2.09 times the chance of mortality due to traffic accidents for non-whites (black, brown, yellow and indigenous).
External causes of traffic accidents are considered a major public health problem in the world, often the second- or third-highest cause of death, and they are related to socioeconomic, political and cultural disparities11.
Approximately 1.2 million people are killed and 50 million injured annually due to traffic accidents12. In a study carried out in Bogota over a one-year period, 430 people died due to traffic accidents13. The number of deaths in Mexico rose from 14,423 in 1998 to 18,205 in 2009, an increase of 29%14. In Brazil, the number of fatal traffic accident victims in 2014 was 43,075. Since 2009, the number of traffic accidents in the country has jumped from 19 per 100,000 inhabitants to 23.4 per 100,000 inhabitants, the highest in South America5.
Regarding sex, in this study, the male deaths corresponded to 79.41% when compared to the female sex. Convergent data were found in the study by Quitian-Reyes et al.13, in which 79% of the affected population were men. Xie et al.15 identified a prevalence of 71.3% of men in this population.
The UK Department of Transportation conducted a study in partnership with the School of Psychology of the University of Nottingham in 2004 and found that men are 12 times more likely to be involved in an accident than women, and 70% were in the urban areas with a predominance of males and young people under 30 years of age16.
More than three-quarters of the deaths from traffic accidents in the world are young males. Male Brazilians also die more from this type of accident than women17, and the trend of mortality among men in Brazil increased from 1998 to 200718. In the Federal District, those who died from motorcyclists' accidents from 1996 to 2007 were found to be largely male (94.3%), brown (71.0%) and aged between 20 and 39 years (73.8%)19.
It is frequent and routine in traffic accidents to find a prevalence of males, as shown in several national and international studies. These reveal that this fact may be related to men being the drivers of the vehicles involved because they are the largest group with the ability to drive and learned to handle the vehicles at young ages, leading to feelings of superiority and omnipotence in traffic20.
The male sex has fewer pathologies than women when considering the physiological and hormonal processes of each sex. However, men have a higher mortality rate due to external causes, such as traffic accidents, violence and homicides21.
When performing a retrospective analysis of the socio-demographic variables between the years 2001 and 2010, Soriano et al.22 observed that men are more involved in accidents but within the expected percentage for each year. On the other hand, women were increasingly involved in a sprawling manner, with 254 cases in 2001 and 1,120 in 2010, which is a notable increase in the number of women in traffic accidents.
Regarding the age groups, 56% of the studied population were between 20-49 years old. In Zanjan, Iran, the average age of the victims was 37.22 years23. In Africa, the age range of the victims ranged from 15 to 34 years24. In Vietnam, the majority of deaths due to traffic accidents are male (79%), aged between 15 and 49 years, and 58% of them are motorcycle users25.
When they start driving, young people represent a high-risk population for transit and public health because they are generally characterized by inexperience in driving, impulsiveness, or even frequent use of alcohol and drugs, wich contribute to the increase in accident cases26.
Regarding race/colour of the skin, more than half of the individuals who died due to auto accidents in the city of São Paulo were white. A survey of the trend of mortality in Brazil between 2000 and 2010 observed that the black population presented the highest percentages of mortality from external causes (17.7% in 2000 and 17.6% in 2010). For the white population, the percentages were 10.7% and less than 1.0% in the years 2000 and 2010, respectively. These results diverge from this study, since white individuals were the highest victims of traffic deaths in the city of São Paulo19.
Although estimates of death rates from road traffic accidents are projected to increase, as illustrated by the World Health Organization (WHO) which shows that the number of road deaths worldwide can reach 1 million per year by 203027, in the city of São Paulo between 2010 and 2014, there was a drop in the mortality rate, as shown in other studies in the country from 1980 to 200328 and 1996 to 200729.
However, despite the fact that traffic fatalities have shown significant reductions in recent years in several developed countries, they cannot be explained solely by political efforts, but they must also be attributed to the global economic recession that affected the economy and mobility in most countries. In order to test the effect of annual per capita GDP variations on accident mortality rates, Yannis et al.30, used data for the 1975-2011 period from 27 European countries and showed that annual GDP growth per capita mortality leads to an increase in mortality rates, while an annual retraction of per capita GDP induces a decrease in mortality rates.
Other research has sought to determine the impact of traffic accidents on economic growth and also to analyse the effect of macroeconomic variables on traffic accidents. In conducting research in Ghana, Enu31 found that traffic accidents negatively affect the economic growth of this country and the degree of this negative effect is approximately 0.21% of GDP. The study also showed that the main macroeconomic variables that affect traffic accidents in Ghana are the size of the economy (GDP), citizens' living standards (GDP per capita) and government spending.
In Brazil, the economic literature on traffic accidents is scarce, but when assessing the relationship between deaths due to traffic accidents and the level of economic activity in the period 1980-1999, Silva and Kilsztajn32 observed a cyclical behaviour in the number of traffic accident deaths due to motor vehicle accidents. These deaths were associated with the level of economic activity in the country, as well as a declining trend in the number of deaths per vehicle, which accompanies an increase in the number of vehicles per inhabitant.
The study by Kume33 illustrated that changes in laws can reduce traffic deaths, since tougher laws with substantive financial penalties can have significant effects on individuals' incentives. The implementation of the new Brazilian Traffic Code, effective since 1998, significantly reduced traffic deaths in Brazil by up to 5.8%, representing more than 26,300 saved lives, in addition to a savings of R$71 billion for public coffers, and reduced transfer service of removal cars and victims between 1998 and 2004.
In 2012, the law that prohibits the use of alcohol in traffic underwent an intense reformulation. It reduced the rate of alcohol in the Breathalyzer test, as well as increased the application of penalties34. Between 2007 and 2013, a process of greater application occurred, especially during holidays and weekends, which may explain the decrease in the indices35.
Hospital costs are related to traffic accidents and economic impacts because external causes require more complex hospital procedures, along with more surgeries, need for intensive care, drug consumption and multi-professional support, resulting in higher costs to health services36.
When analysing hospital costs generated by external causes in a large hospital emergency service in Teresina, Piauí, Brazil, identified expenses of R$1,019,755.90 between 2005 and 2007 for admissions due to external causes, which is higher compared to other causes in the same period (R$888,912.44)36.
In the year 2010, The World Health Organization37 recommended that the time between 2011 and 2020 be the decade of actions for traffic safety. In the last survey in 2010, about 1.3 million deaths from traffic accidents occurred worldwide, with approximately 50 million surviving with complications37.
Thus, working to reduce traffic violence is certainly a complex goal that should include intersectoral and interdisciplinary actions. The health system, besides acting inter-sectorally with road safety agents, managers and professionals, has the role of defining the general conditions in which drivers must drive. It is important to introduce and make known risk factors, such as high-speed driving hazards under the effects of alcohol and other drugs. It is still important to promote health in order to empower the population in relation to situations of traffic violence through actions that can be developed in the school context, in addition to family health strategies38.
In the field of public health, prehospital care services, which is a mobile service that provides an early rescue, can have an effect on reducing the dangers to accident victims, but it cannot reverse an extremely serious situation, which is dependent on the process of continuous education of drivers and pedestrians on a daily basis and in the public thoroughfares of a metropolis, such as the city of São Paulo.
Accidents and violence due to external causes have had an important impact on the health of populations in various countries of the world. Health services need to allocate professionals and equipment to care for these victims, who often require the care of a number of specialists: neurosurgeons, orthopaedists, abdomen and thorax surgeons, physiotherapists and other professionals. The consequences of accidents and violence for the health system and for society indicate the need to improve the information system on mortality and morbidity due to external causes, with a view to subsidizing public policies39.
Mortality was always higher among individuals aged 50 years or older, except in 2016 (Table 2 and Graph 3), indicating that the reduction in speed limit benefited, mostly, individuals aged 50 years or older. These results are convergent with those listed by Duim et al.40, who demonstrated that the majority of the elderly living in the city of São Paulo cannot cross the streets at their own walking speed, because they walk at a slower pace than is currently demanded by the lights at the pedestrian crossings, providing an increased risk of collision between the vehicle and the pedestrian 60 years old or more. Although the analyses of Figure 3 and Table 2 are characterized by stratified populations aged 50 years or older, it is inferred that the affected individuals are those similarly aged to those reported in the study40.
Public policies and specific health interventions to cardiovascular diseases, especially those focused on Cerebrovascular Accident (CVA), contributed to reduce the mortality due to CVA in Brazilian young adults41. We also consider that the prevention of external causes of accidents should be a relevant and current subject in the field of Public Health, as well as for the other Public Safety, Education, Social Promotion and Citizenship Institutions, which will result in decrease of the incidence and mortality due to these group of external causes. Health professionals, through health education, should and can be important messengers for publicizing the benefits of improving the daily living conditions of the pedestrian and the driver. They can contribute to the exercise of citizenship and less violence in the transit of large and small cities in Brazil, since they are in a prominent position to promote these actions in modern society. Discussing and proposing solutions to reduce traffic violence is a relevant and current fact in the field of public health. In addition, it has already been identified that effective Public Health programs contribute to the reduction of mortality from specific causes, favoring the reduction of noncommunicable diseases at all ages, including among children and adolescents42-44.
CONCLUSION
There was a decrease of deaths related to traffic accidents in individuals over 20 years. After the reduction of the average speed of motor vehicles in the city of São Paulo, the decline in mortality due to traffic accidents was more pronounced among individuals aged 50 years or older, with significant differences for men and women. In addition, death rates remain very high. In addition, the traffic violence remains a global public health problem, requiring effective health policies for the prevention of traffic accidents.
Acknowledgments: The authors wish to acknowledge the Dr. José Leopoldo Ferreira Antunes, Full Professor, Department of Epidemiology, Faculty of Public Health, University of São Paulo.
REFERENCES
1.Anjos KC, Evangelista MRB, Silva, JS, Zumiott AV. Paciente vítima de violência no trânsito: análise do perfil socioeconômico, características do acidente e intervenção do Serviço Social na emergência. Acta Ortop Bras. 2007;15(5):262-6. DOI: http://dx.doi.org/10.1590/S1413-78522007000500006 [ Links ]
2. Alves ACBB, Oliveira AS, Pedro JB, Mamlak L, Oliveira LS, Mendonça LO, et al. A nova lei seca: mudanças ocasionadas pela antiga e nova lei no código de trânsito brasileiro. Cad Grad Ciênc Hum Sociais. 2014;2(2):137-46. [ Links ]
3. Kanchan T, Kulkarni V, Bakkannavar SM, Kumar N, Unnikrishnan B. Analysis of fatal road traffic accidents in a coastal township of South India. J Forensic Leg Med. 2012;19(8):448-51. DOI: http://dx.doi.org/10.1016/j.jflm.2012.02.031 [ Links ]
4.Malta DC, Andrade SSCA, Gomes N, Silva MMA, Morais Neto OL, Reis AAC, et al. Injuries from traffic accidents and use of protection equipment in the Brazilian population, according to a population-based study. Ciênc Saúde Coletiva. 2016; 21(2):399-410. DOI: http://dx.doi.org/10.1590/1413-81232015212.23742015 [ Links ]
5.Organização mundial de saúde (OMS). Mais de 270 mil pedestres morrem a cada ano em acidentes, diz OMS. [cited 2018 Aug 22] Available from: http://g1.globo.com/mundo/noticia/2013/05/mais-de-270000-pedetres-morrem-a-cada-ano-em-acidentes-oms.html [ Links ]
6.Brasil. Ministério da Saúde. DATASUS: Departamento de Informática do SUS. [cited 2018 Aug 22] Available from: http://datasus.saude.gov.br/ [ Links ]
7.Lima TL, Souza MES, Barbosa XC, Souza Junior M.S. Violência no trânsito uma abordagem da problemática na cidade de Porto Velho. Zona Impacto. 2015;17(1):97-112. [ Links ]
8.Mesquita GV, Oliveira FAFV, Santos AMR, Tapety FI, Martins MCC, Carvalho CMRS. Análise dos custos hospitalares em um serviço de emergência. Rev Texto Contexto Enferm. 2009;18(2):273-9. DOI: http://dx.doi.org/10.1590/S0104-07072009000200010 [ Links ]
9.Antunes JLF, Cardoso MRA. Uso da análise de séries temporais em estudos epidemiológicos. Epidemiol Serv Saúde. 2015;24(3):565-76. DOI: http://dx.doi.org/10.5123/S1679-49742015000300024 [ Links ]
10.Instituto Brasileiro de Geografia e Estatística do Brasil (IBGE). Censo 2010. [cited 2018 Aug 22] Available from: https://censo2010.ibge.gov.br/ [ Links ]
11.White A, McKee M, Sousa B, Visser R, Hogston R, Madsen SA, et al. An examination of the association between premature mortality and life expectancy among men in Europe. Eur J Public Health. 2013;24(4):673-9. https://dx.doi.org/10.1093/eurpub/ckt076 [ Links ]
12.Peden M. Global collaboration on road traffic injury prevention. Int J Inj Contr Saf Promot. 2005;12(2):85-91. DOI: https://dx.doi.org/10.1080/15660970500086130 [ Links ]
13.Quitian-Reyes H, Gómez-Restrepo C, Gómez MJ, Naranjo S, Heredia P, Villegas J. Latin American Clinical Epidemiology Network series-paper 5: years of life lost due to premature death in traffic accidents in Bogota, Colombia. J Clin Epidemiol. 2017;86:101-5. DOI: https://dx.doi.org/10.1016/j.jclinepi.2016.04.017 [ Links ]
14.Cervantes-Trejo A, Leenen I, Fabila-Carrasco JS, Rojas-Vargas R. Trends in traffic fatalities in Mexico: examining progress on the decade of action for road safety. Int J Public Health. 2016;61(8):903-13. DOI: https://dx.doi.org/10.1007/s00038-016-0867-z [ Links ]
15.Xie SH, Wu YS, Liu XJ, Fu YB, Li SS, Ma HW, et al. Mortality from road traffic accidents in a rapidly urbanizing Chinese city: a 20-year analysis in Shenzhen, 1994-2013. Traffic Inj Prev. 2016;17(1):39-43. DOI: https://dx.doi.org/10.1080/15389588.2015.1035370 [ Links ]
16.Pinto CS, Cunha MM. Educação para o trânsito: a violência no trânsito trabalhada no contexto escolar. Rev Even Pedagóg. 2013;4(1):63-71. DOI: https://dx.doi.org/10.30681/2236-3165 [ Links ]
17.Almeida APB, Lima MLC, Oliveira Júnior FJM, Abath MB, Lima MLLT. Anos potenciais de vida perdidos por acidentes de transitono Estado de Pernambuco, Brasil, em 2007. Epidemiol Serv Saude. 2013;22(2):235-42. DOI: https://dx.doi.org/10.5123/S1679-49742013000200005 [ Links ]
18.Duarte EC, Duarte E, Sousa MC, Tauil PL, Monteiro RA. Mortalidade por acidentes de transito e homicídios em homens jovens das capitais das Regiões Norte e Centro-Oeste do Brasil, 1980-2005. Epidemiol Serv Saude. 2008;17(1):7-20. DOI: https://dx.doi.org/10.5123/S1679-49742008000100002 [ Links ]
19.Morais Neto OL, Montenegro MMS, Monteiro RA, Siqueira Júnior JB, Silva MMA, Lima CM, et al. Mortalidade por acidentes de transito no Brasil na última década: tendência e aglomerados de risco. Ciênc Saúde Coletiva. 2012;17(9): 2223-36. DOI: http://dx.doi.org/10.1590/S1413-81232012000900002 [ Links ]
20.Batista FS, Silveira LO, Castillo JJAQ, Pontes JE, Villalobos LDC. Epidemiological profile of extremity fractures in victims of motorcycle accidents. Acta Ortop Bras. 2015;23(1):43-6. DOI: http://dx.doi.org/10.1590/1413-78522015230100998 [ Links ]
21.Moura EC, Gomes R, Falcão MTC, Schwarz E, Neves ACM, Santos W. Desigualdades de gênero na mortalidade por causas externas no Brasil, 2010. Rev Ciênc Saúde Coletiva. 2015;20(3):779-788. DOI: http://dx.doi.org/10.1590/1413-81232015203.11172014 [ Links ]
22.Soriano EP, Carvalho MVD, Montenegro JB, Campello RIC, Almeida AC, Lins Filho JDL, et al. Violência no trânsito: uma década de vidas perdidas em acidentes motociclísticos no Brasil. [cited 2018 Aug 22] Available from: www.derechoycambiosocial.com [ Links ]
23.Yousefzadeh-Chabok S, Ranjbar-Taklimie F, Malekpouri R, Razzaghi A. A Time Series Model for Assessing the Trend and Forecasting the Road Traffic Accident Mortality. Arch Trauma Res. 2016;5(3):e36570. DOI: http://dx.doi.org/10.5812/atr.36570 [ Links ]
24.Sango HA, Testa J, Meda N, Contrand B, Traoré MS, Staccini P, et al. Mortality and morbidity of urban road traffic crashes in Africa: capture-recapture estimates in Bamako, Mali, 2012. PLoS One. 2016;11(2):e0149070. DOI: https://dx.doi.org/10.1371/journal.pone.0149070 [ Links ]
25.Ngo Ad, Rao C, Hoa NP, Hoy DG, Trang KTQ, Hill PS. Road traffic related mortality in Vietnam: Evidence for policy from a national sample mortality surveillance system. BMC Public Health. 2012;12:561. DOI: https://dx.doi.org/10.1186/1471-2458-12-561 [ Links ]
26.Andrade SM, Soares DA, Matsuo T, Liberatti CLB, Iwakura MLH. Road injury-related mortality in a medium-sized Brazilian city after some preventive interventions. Traffic Inj Prev. 2008;9(5):450-5. DOI: https://dx.doi.org/10.1080/15389580802272831 [ Links ]
27.World Health Organization (WHO). Global status report on road safety 2013: supporting a decade of action. Geneva: WHO, 2013. [ Links ]
28.Souza MFM, Malta DC, Conceição GMS, Silva MMA, Gazal-Carvalho C, Morais Neto OL. Análise descritiva e de tendência de acidentes de transito para políticas sociais no Brasil. Epidemiol Serv Saúde. 2007;16(1):33-44. https://dx.doi.org/10.5123/S1679-49742007000100004 [ Links ]
29.Reichenheim ME, Souza ER, Moraes CL, Jorge MHPM, Silva CMFP, Minayo MCS. Violence and injuries in Brazil: the effect, progress made, and challenges ahead. Lancet. 2011;377(9781):1962-75. DOI: https://dx.doi.org/10.1016/S0140-6736(11)60053-6 [ Links ]
30.Yannis G, Papadimitriou E, Folla K. Effect of GDP changes on road traffic fatalities. Saf Sci. 2014;63:42-9. DOI: http://dx.doi.org/10.1016/j.ssci.2013.10.017 [ Links ]
31.Enu P. Road traffic accidents and macroeconomic conditions in Ghana. Soc Basic Sci Res Rev. 2014;2(9):374-93. [ Links ]
32.Silva CRL, Kilsztajn S. Acidentes de trânsito, frota de veículos e nível de atividade econômica. Rev Econ Contemp. 2003;7(1):147-59. [ Links ]
33.Kume L. É possível reduzir as mortes no trânsito? O efeito do novo Código Brasileiro de Trânsito. [cited 2018 Aug 22] Available from: https://cps.fgv.br/e-possivel-reduzir-mortes-no-transito-o-efeito-do-novo-codigo-brasileiro-de-transito. [ Links ]
34.Oliveira NLB, Sousa RMC. Ocorrências de trânsito com motocicleta e sua relação com a mortalidade. Rev Latino-Am Enfermagem. 2011;19(2):403-10. DOI: http://dx.doi.org/10.1590/S0104-11692011000200024 [ Links ]
35.Malta DC, Berna RTI, Silva MMA, Claro RM, Silva Júnior JB, Reis AAC. Consumo de bebidas alcoólicas e direção de veículos, balanço da lei seca, Brasil 2007 a 2013. Rev Saúde Pública. 2014;48(4):692-6. DOI: http://dx.doi.org/10.1590/S0034-8910.2014048005633 [ Links ]
36.World Health Organization (WHO). Declaração política do Rio sobre Determinantes Sociais da Saúde. [cited 2018 Aug 22] Available from: http://www.who.int/sdhconference/declaration/Rio_political_declaration_portuguese.pdf [ Links ]
37.Bezerra IMP, Sorpreso ICE. Concepts and movements in health promotion to guide educational practices. J Hum Growth Dev. 2016;26(1):11-16. DOI: http://dx.doi.org/10.7322/jhgd.113709 [ Links ]
38.Grupo Técnico de Prevenção de Acidentes e violências. Centro de Vigilância Epidemiológica "Prof. Alexandre Vranjac". Coordenadoria de Controle de Doenças. Secretaria de Estado da Saúde de São Paulo. O impacto dos acidentes e violências nos gastos da saúde. Rev Saúde Pública. 2006;40(3):553-6. DOI: http://dx.doi.org/10.1590/S0034-89102006000300028 [ Links ]
39.Silva MMA, Mascarenhas MDM, Lima CM, Malta DC, Monteiro RA, Freitas MG, et al. Perfil do inquérito de violências e acidentes em serviços sentinela de urgência e emergência. Epidemiol Serv Saude. 2017;26(1):183-94. DOI: https://dx.doi.org/10.5123/S1679-49742017000100019 [ Links ]
40.Duim E, Lebrão ML, Antunes JLF. Walking speed of older people and pedestrian crossing time. J Transport Health. 2017;5:70-6. DOI: https://dx.doi.org/10.1016/j.jth.2017.02.001 [ Links ]
41.Adami, fernando ; figueiredo, francisco winter dos santos ; paiva, laércio da silva ; sá, thiago hérick de ; santos, edige felipe de sousa ; martins, bruno luis ; valenti, vitor engrácia ; abreu, luiz carlos de . Mortality and Incidence of Hospital Admissions for Stroke among Brazilians Aged 15 to 49 Years between 2008 and 2012. Plos One , v. 11, p. e0152739-10, 2016. doi: 10.1371/journal.pone.0152739 [ Links ]
42.Feitosa, AC, Santos, EFS, Ramos, JLS, Bezerra, IMP, Nascimento, VG, Macedo, CC, Macedo Jr, H, & Abreu, LC.. Factors associated with infant mortality in the metropolitan region of Cariri, Ceará, Brazil. J. Hum. Growth Dev., São Paulo , v. 25, n. 2, p. 224-229, 2015. https://dx.doi.org/10.7322/JHGD.103019 [ Links ]
43.Freitas, AG, Lima, DG, Bortolini, MJS, Meneguetti, DUO, Santos, EFSS, & Silva, RPM. Comparison of the nutritional status in children aged 5 to 10 years old on the Conditional Cash Transfer Programme in the States of Acre and Rio Grande do Sul, Brazil. J. Hum. Growth Dev., São Paulo , v. 27, n. 1, p. 35-41, 2017. https://dx.doi.org/10.7322/jhgd.127647 [ Links ]
44.Zangirolami-Raimundo J, Echeimberg JO, Leone C. Research methodology topics: Cross-sectional studies. Journal of Human Growth and Development. 2018; 28(3):356-360. DOI: http://dx.doi.org/10.7322/jhgd.152198 [ Links ]
 Correspondence:
Correspondence:
Italla.Bezerra@emescam.br; edige@usp.br
Manuscript received: May 2018
Manuscript accepted: July 2018
Version of record online: April 2019


{kind=link}
{kind=link}
{kind=link}
{kind=link}