










Serviços Personalizados
artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282versão On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.29 no.2 São Paulo maio/ago. 2019
http://dx.doi.org/10.7322/jhgd.v29.9430
ORIGINAL ARTICLE
Access to minor surgical procedures in a community family health unit: an initiative for improving care and access as basic health units
Dimítra Lengruber SesquimI; José Lucas Souza RamosII; Gustavo Carreiro PinascoIII; Marianna Tamara Nunes LopesIV; Marcello Dala Bernadina DallaV; Marcelo Santana VetisVI; Italla Maria Pinheiro BezerraVII
IPrograma de Pós-graduação em Políticas Públicas e Desenvolvimento Local, Escola Superior de Ciências da Santa Casa de Vitória, EMESCAM. Vitória, ES, Brasil
IILaboratório de Escrita Científica, Escola Superior de Ciências da Santa Casa de Vitória, EMESCAM. Vitória, ES, Brasil
IIIEscola Superior de Ciências da Santa Casa de Vitória, EMESCAM. Vitória, ES, Brasil
IVPrograma de Pós-graduação em Políticas Públicas e Desenvolvimento Local, Escola Superior de Ciências da Santa Casa de Vitória, EMESCAM. Vitória, ES, Brasil
VSecretaria de Estado da Saúde do Espírito Santo (SESA), preceptor da Residencia em Medicina de Família e Comunidade. Escola Superior de Ciencias da Santa Casa de Misericórdia de Vitória, EMESCAM. Secretaria Municipal de Saúde de Vitória, ES, Brasil
VIResidência em Medicina de Família e Comunidade, Escola Superior de Ciencias da Santa Casa de Misericórdia de Vitória, EMESCAM
VIIBolsista CAPES Brasil. Setor de Pós-graduação, Pesquisa e Inovação, Centro Universitário Saúde ABC, CUSABC. Programa de Pós-graduação em Políticas Públicas e Desenvolvimento Local, Escola Superior de Ciências da Santa Casa de Misericórdia de Vitória, EMESCAM. Vitória, ES, Brasil
ABSTRACT
It was describe the implantation of small surgical procedures performed by physicians living in a Brazilian Family Health Unit. This is an experience report carried out in the city of Vitória, Espírito Santo, Brazil, describing the introduction of small surgical procedures by the Family and Community Medicine medical residency program in a Basic Health Unit (UBS) of the municipality. The selected US did not have a room for minor surgery procedures or the necessary materials. It was evidenced that the population demanded surgical complaints without resolution of the same ones, being these patients referenced to other specialties.
Keywords: Primary health care. Surgical procedures. Family Medicine. Community health.
Authors summary
Why was this study done?
This study was conducted to identify the impact of performing small procedures on PHC as a means of access to health and to minimize the waiting list for referral to surgical procedures at other levels of care, indirectly analyzing access and resolution of the SUS gateway.
What did the researchers do and find?
It was selected over a period of year and electronic medical records of users of health units in the city of Vitória, Espírito Santo, Brazil, to identify which and how many surgical procedures were performed by residents of the Family and Community Medicine Program and two preceptors of the program. The importance of performing small outpatient surgical procedures at the UBS as a means of access to health was highlighted.
What do these findings mean?
Investing in performing minor surgical procedures in Primary Health Care provides access to health and shortens the referral queue.
INTRODUCTION
On September 19, 1990, the Law 8.080 was implemented in Brazil, which regulates health actions and services throughout the country and creates the Unified Health System (SUS), which should provide assistance to people through Promotion, protection and recovery of health, with the integration of care interventions and preventive activities1. The SUS has as one of its guidelines the political-administrative decentralization, with a unique direction in each sphere of government, with emphasis on the decentralization of services to the municipalities and regionalization and hierarchization of the health services network. Therefore, the system user must follow a sequence of steps to have access to the health service needed1.
In the Strategy Health Family program (SHF) it is fundamental multiprofessional teams working in the PC composed of at least general practitioner or specialist in Family Health or Family and Community doctor, generalist nurse or specialist in Family Health, an auxiliary or nursing technician and community agents of Oral health professionals: general-surgeon-dentist or specialist in Family Health, auxiliary and / or dental health technician1, as part of the multiprofessional
The family and community doctor is the specialist responsible for health care in a continuous, and comprehensive way for people, their families and the community, therefore is considered the "medical professional with vocation and specific training to provide care in PC; he is a specialist in handling the problems under his responsibility2.
This capacity for problem solving by PC professionals is fundamental to user access, "welcoming and execution of those professionals are instruments for improving access, continuity of health care and integral care"3. Be outstanding in solving issues High means that referrals to other specialists should not exceed 10% of the total number of people served4.
If the patient attended in the Basic Health Unit is identified with an illness that exceeds the knowledge of his / her family doctor, he will enter the queue of referrals to another specialist specific to his / her illness. Then, he awaits for the call to be attended. When he receives the message "waiting to be referred", it can be associated with clinical worsening, stress due to non-attendance and administration costs of this queue that cause heavy administrative burdens, efficiency losses, organizational disorder and social pressure5.
The need to invest in PC is therefore questioned as one of the ways to minimize routing queues. The family and community physician (FCP) is qualified to perform small surgical procedures which are described in the FCP Competency Based Curriculum, the essential procedures in the training of this specialist are: drainage of abscess, suture, cantoplasty, insertion and removal of intrauterine device (IUD), chemical cauterization of viral wart, puncture and joint infiltration, local anesthesia and anesthetic blockade of quirodactyls and pododactyls, removal of cyst and lipomas, intramuscular, subcutaneous and intravenous injection, suturing, dressing, compression and immobilization, removal of cerumen , foreign body removal, frenectomy and anterior nasal packing6.
In this way, steps would be spared and the referencing system becomes less costly for cases that can not really be solved in PC. For example, the consequences of cerumen in the external auditory canal vary from mild pruritus, otalgia or even temporary hearing loss, or hearing loss7. To prevent such consequences is to offer the best assistance and quality of life to SUS users.
This study becomes relevant since the Brazilian population is increasing and more people will consequently be inserted in the queues of the PC centers. Thus, it aims to describe the implantation of minor surgical procedures performed by physicians residing in a Family Health Unit.
METHODS
This is an experience report carried out in the city of Vitória, Espírito Santo, Brazil, describing the introduction of minor surgical procedures by the medical residency program of Family and Community Care in a Basic Health Unit (BHU) of the mentioned municipality. The selected BHU works with three family health teams, one of them is coordinated by the resident phisician. This report of experience was carried out according to Revised Standards for Quality Improvement Reporting Excellence SQUIRE 2.0.
The data were collected on the procedures performed by team 1 of the selected BHU, used as a training camp for residents, from June 2015 to June 2016, through the Bem Estar Network, software used by the City of Vitória, which connects all municipal health network in a unique system (health units, ready-to-use clinics, pharmacies, laboratories, dental offices and referral and specialty centers). Where, the total number of procedures was generated and which were these made possible the current study. No medical records were evaluated.
The study respected the ethical precepts of research involving human beings, being submitted to the Technical School of Health of SUS (TSHSUS), and later to the Committee of Ethics in Research with Human Beings (CEP) obtaining approval opinion under number 5596565.
RESULTS
In June 2015, minor surgical procedures were started in team 1 of the selected BHU. The procedures were performed by residents of family medicine and community, supervised by preceptors. It is worth noting when patients knew that their doctors could do the procedure in their own unit, there was no opposition, but a feeling of surprise and optimism with their clinical situation.
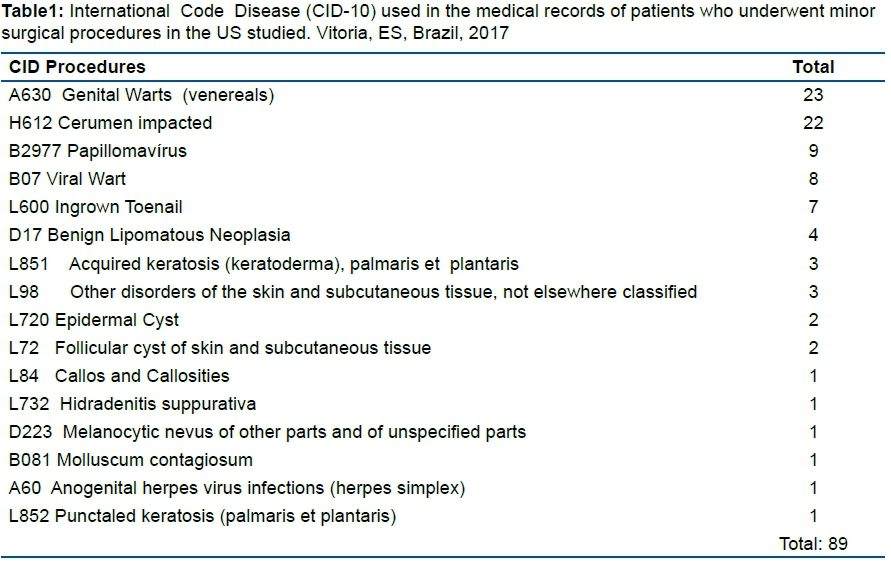
Then, from June 1, 2015 to June 1, 2016, ninety procedures were performed, according to table 1. Forty-three chemical cauterizations of small lesions, twenty-five skin tumor excisions and sebaceous cyst / lipoma and twenty-two cerumen removals from uni / bilateral external auditory canals. The International Code of Diseases (ICD) was used to justify the procedures (Table 1).
Previously, the BHU referred patients to the emergency room (ER) and hospitals, currently residents and preceptors are responsible for receiving the referrals. The ER that is associated with BHU studied, has already referenced cases of patients attending this, who needed some minor procedure for residents to do so. BHU has also been referenced by physicians, within the Unit itself, who do not perform procedures. Currently the only units that perform procedures in the city of Vitória are those which have a phisician resident of Family Medicine and community as an internship field.
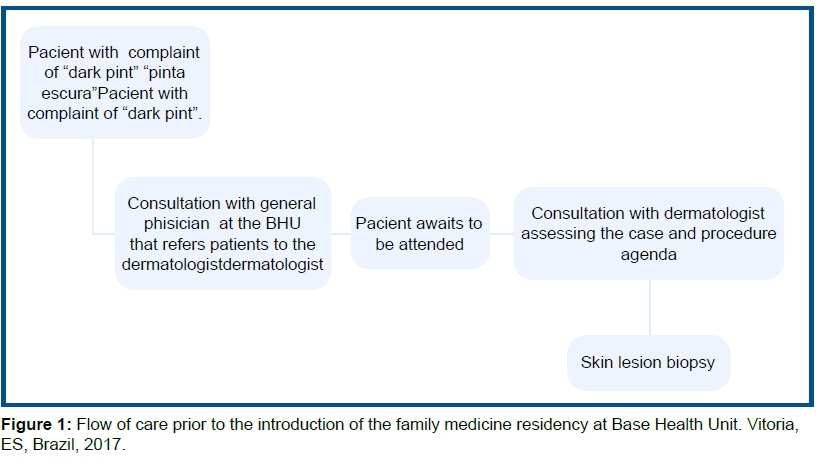
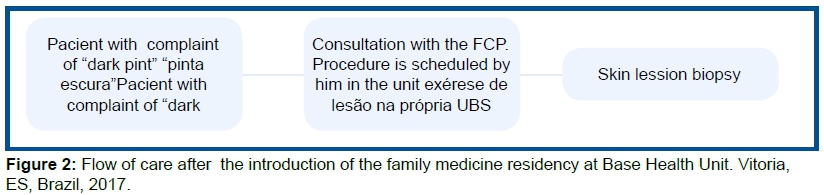
As shown in the figure below, the organization of the work process of the Health Unit regarding the accomplishment of the procedures led to the reduction of waiting times and contributed to the improvement of patients' flow (Figure 1 and Figure 2).
Initially, an inventory of the available materials was carried out. The unit did not have a specific room for procedures, but it had a dressing room. There were no trays for procedures, no suture wire or scalpel blade, however there was a sterilization machine for IUD insertion materials used by the gynecologist who attends the unit. Nurses and nursing technicians were available to assist during the procedures. Inspection of the central level, through epidemiological surveillance, analyzed the structure of the BHU and authorized the accomplishment of the procedures in the dressing room. It was agreed with the cleaning staff so that before and after each procedure the site was cleaned. Those who were in the room at the time of the procedure should use personal protective equipment (PPE) such as a cap, mask, goggles, stereo gloves (depending on the procedure), and a closed waistcoat.
The necessary materials available were needles and syringes. Residents and preceptors made a list to obtain the other missing materials by requesting them to the city hall through the direction of the Unit, these would be: protective goggles, surgical mask, surgical cap, disposable fenestrated field, sterile gloves, anesthetics, scalpel blade, sutures and formalin
After requesting the materials, it was thought to organize the attendance agenda. Four hours of consultation, each lasting thirty minutes, were reserved on Tuesday morning from seven hours and ten minutes to nine hours and ten minutes, on Thursday afternoom from four hours to six hours. Thus, during the week, there would be procedures in two different days and in different shifts to favor the access of those patients who worked or had other activities
The scheduling was done by preceptors, who were authorized by the BHU board to schedule patients on the residents' agenda. Patients with indication of procedures were identified in outpatient consultations by the residents who informed their preceptors who were in charge of registering the patients in the system.
While the requested materials did not arrive, the residents prepared themselves by reviewing the procedures' techniques. The number 30 issue of Primary Care launched in 2011 by the Ministry of Health is entitled "Procedures" and describes all the minor surgical procedures that the Family and Community doctor has the competence to perform within a Basic Family Health Unit. This interval between the release of the materials and the beginning of the surgical practice was also important to capture the patients who had the indication and desire to undergo the minor procedures.
DISCUSSION
The BHU chosen did not have a room for minor surgery procedures, as well as procedures trays, suture thread or scalpel blade, however there was a sterilization machine for IUD insertion materials used by the gynecologist who attends the unit.
After the implementation of the room, the minor surgeries that had the highest request were those of genital warts and cerumen impacted.
When discussing the failure to perform small surgical procedures in a health unit composed of general practitioners, it was evidenced that the population demanded surgical complaints without solution, being these patients referenced to other specialties, which caused a delay for consultations with another Specialist for elective surgery
It is important to emphasize that primary care should serve as a prevention port for more serious cases, avoiding the overload of secondary or tertiary care health services, thus, it is important to have an adequate place to perform minor surgical procedures, since they comply with the rules of hygiene and precaution for health professionals, providing patient safety.
Thus, unlike the reality found in the study by Moura et al. 8, when comparing the reality of two different municipalities, it was observed that there is the presence of this room in both, however that the investment in materials that come to equip this place is more present in one of these.
Confronting this result with an old reality, in the years 2001 and 2002, according to research for Normative Evaluation of the Family Health Program, carried out at national level, it was identified that in nine Brazilian states, there was a room for minor surgical procedures, however, there were few materials available from government spheres9,10.
As described, among the most sought-after procedures, we highlighted genital / anus warts and impacted cerumen. This result refers to the high social vulnerability in which the Health Unit is located , mainly reflecting on sexually transmitted infections (STIs), as well as simple self-care activities such as hygiene.
Related to STIs, this is still a problematic which requires a greater performance of primary care, in order to prevent its complications. In addition to the occasional assistance, such as the removal of warts and treatment, preventive methods include health education. However, in the studies, there is still a focus directed only at the adolescent public11,12.
As for the high incidence of patients requiring ear washing due to impacted cerumen, it can be understood that it is directly related to the physiological processes, however, that can be avoided through self-care by hygiene, improving the habits of the clients by applying activities of Health education12,13.
It was identified a difficulty related to referral of patients, and thus, it is understood that some strategies to minimize the referral queue are based on the understanding of the need for enhancement of PC professionals, reinforcement of prevention and health protection schemes14.
Also, it should be noted that poor service can mask the indicators and reduce the waiting time in the queues. Thus, it is necessary to clearly define the responsibilities regarding evaluation, administration and overall coordination of queues, to observe that different clinical cases require different types of efforts to reduce deadlines and queues5.
In this context, Marinho, Cardos and Almeida5 considers that this delay in care has significant negative impacts on well-being, cure probabilities, the nature and extent of patient sequelae, as well as on the family members involved.
The promotion of resolutivity generates satisfaction in the clientele and in the quality of health care15. Therefore, it is important to train family physicians with quality to provide the population with resolution, quality care and those patients who really need referrals, can obtain this access quickly avoiding health complications.
Thus, it is recognized that family and community medicine is the strategic medical specialization in the shaping of health systems. The first contact, longitudinal care, integral care and coordination of a person's health is assigned to the FCP, considering their family and community context. Therefore, family and community medicine is a primary component of primary health care16.
It is still fundamental to prioritize the demand that a specific location will require; Being aware of what is most urgent within a population and making this a priority will transform the place. In this report in question, the demand for minor surgical procedures was perceived. It is corroborated with Braga et al.17 when they affirm that population demand, FCP's ability and local infrastructure influence the quantity and procedures to be performed.
Although this study refers to an experience report with a group of residents in its practice scenario, it was possible to highlight the importance of the family physician in working with the health team, thus facilitating (re) organization of the Services, and in particular, meeting the health needs of the population.
This point brings to light the discussion of the health care model that has long been implemented with a view to reducing queues, meeting the population's health needs, preserving the quality of life through prevention and promotion actions Health18-20.
Such actions, when implemented by the professionals of the area, end up promoting better service, as well as a better redirection of the users that will be assisted from their needs: the need to perform invasive procedures, disease prevention and / or health promotion.
It was noticed that the reality of the Health Unit was transformed with the insertion of the of the resident family physician, contributed to the resolution of users' complaints in primary care, there being no need to be referenced for secondary care. In this way, it was possible to observe that with the accomplishment of the minor procedures during the insertion of the residents in the scenario of the study, the access to the health of the population attended by the health team in which the medical residency was ahead was facilitated. Trained residents were able to resolve the health complaints, provide quality of life, and avoid possible complications caused by waiting in the queue for referrals.
REFERENCES
1.Brasil. Ministério da Saúde. Lei n. 8.080, de 19 de setembro de 1990. Dispõe sobre as condições para a promoção, proteção e recuperação da saúde, a organização e o funcionamento dos serviços correspondentes, e dá outras providências. [cited 2018 Oct 28] Available from: http://www.planalto.gov.br/ccivil_03/leis/l8080.htm [ Links ]
2.Gusso GDF, Lopes JMC. Tratado de Medicina de Família e Comunidade: Princípios, Formação e Prática. Porto Alegre: Artmed, 2012. [ Links ]
3.Lanza FM, Lana FCF, Carvalho APM, Davi RFL. Ações de controle da hanseníase: tecnologias desenvolvidas nos municípios do Vale do Jequitinhonha, Minas Gerais. Rev Enferm Centro-Oeste Mineiro. 2011;1(2):164-75. DOI: http://dx.doi.org/10.19175/recom.v0i0.82 [ Links ]
4. Starfield B. Atenção primária: equilíbrio entre necessidades de saúde, serviços e tecnologia. Brasília: Unesco, 2002. [ Links ]
5.Marinho A, Cardos SS, Almeida VV. A economia das filas no sistema único de saúde (SUS) brasileiro. Brasília: IPEA, 2009. [ Links ]
6.Sociedade Brasileira de Medicina de Família e Comunidade (SBMFC). Currículo Baseado em Competências para medicina de Família e Comunidade, 2014. [ Links ]
7.Tiago RSL, Salgado DC, Corrêa JP, Pio MRB, Lambert EE. Corpo estranho de orelha, nariz e orofaringe: experiência de um hospital terciário. Rev Bras Otorrinolaringol. 2006;72(2):177-81. DOI: http://dx.doi.org/10.1590/S0034-72992006000200005 [ Links ]
8.Moura BLA, Cunha RC, Fonseca ACF, Aquino R, Medina MG, Vilasbôas ALQ, et al. Atenção primária à saúde: estrutura das unidades como componente da atenção à saúde. Rev Bras Saúde Matern Infant. 2010;10(Supl. 1):S69-81. DOI: http://dx.doi.org/10.1590/S1519-38292010000500007 [ Links ]
9.Brasil. Ministério da Saúde. Portaria nº 2.488, de 21 de outubro de 2011. Aprova a Política Nacional de Atenção Básica, estabelecendo a revisão de diretrizes e normas para a organização da Atenção Básica, para a Estratégia Saúde da Família (ESF) e o Programa de Agentes Comunitários de Saúde (PACS). [cited 2018 Oct 28] Available from: http://bvsms.saude.gov.br/bvs/saudelegis/gm/2011/prt2488_21_10_2011.html [ Links ]
10.Brasil. Ministério da Saúde. Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Procedimentos. Brasília: Ministério da Saúde, 2011. [ Links ]
11.Lima DLP, Coelho VCS, Siqueira JP, Cavalcanti PP. Implantação do aconselhamento sobre DST, HIV e hepatites virais no planejamento familiar: relato de experiência. Rev Enferm UFPE. 2015;9(1):7175-9. DOI: http://dx.doi.org/10.5205/reuol.7505-65182-1-RV.0903201521 [ Links ]
12.Carneiro RF, Silva NC, Alves TA, Brito DC, Oliveira LL. Educação sexual na adolescência: uma abordagem no contexto escolar. Sanare. 2015;14(1):104-8. [ Links ]
13.Duarte MTC, Ayres JA, Simonetti JP. Consulta de enfermagem: estratégia de cuidado ao portador de hanseníase em atenção primária. Texto Contexto Enferm. 2009;18(1):100-7. DOI: http://dx.doi.org/10.1590/S0104-07072009000100012 [ Links ]
14.Kanno NP, Bellodi PL, Tess BH. Profissionais da Estratégia Saúde da Família diante de demandas médico-sociais: dificuldades e estratégias de enfrentamento. Saúde Soc. 2012;21(4):884-94. DOI: http://dx.doi.org/10.1590/S0104-12902012000400008 [ Links ]
15.Costa JP, Jorge MSB, Vasconcelos MGF, Paula ML, Bezerra IC. Resolubilidade do cuidado na atenção primária: articulação multiprofissional e rede de serviços. Saúde Debate. 2014;38(103):733-43. DOI: http://dx.doi.org/10.5935/0103-1104.20140067 [ Links ]
16.Vasconcelos FGA, Zaniboni MRG. Dificuldades do trabalho médico no PSF. Ciênc Saúde Coletiva. 2011;16(Suppl 1):1497-1504. DOI: http://dx.doi.org/10.1590/S1413-81232011000700085 [ Links ]
17.Braga DC, Bortolini SM, Barazetti G, Viel J, Vebber SS. Procedimentos cirúrgicos ambulatoriais realizados na Atenção Primária. An Congr Sul-Bras Med Fam Comunidade. 2014:169. [ Links ]
18.Bezerra IMP, Sorpreso ICE. Concepts and movements in health promotion to guide educational practices. J Hum Growth Dev. 2016;26(1):11-20. DOI: https://doi.org/10.7322/jhgd.113709 [ Links ]
19.Bezerra IMP. Translational medicine and its contribution to public health. J Hum Growth Dev. 2017;27(1):6-9. DOI: http://dx.doi.org/10.7322/jhgd.127642 [ Links ]
20.Abreu LC, Pereira VX, Silva RPM, Macedo Junior H, Bezerra IMP. The right to scientific information: one of the main elements of the unified health system. J Hum Growth Dev. 2017; 27(3):258-61. DOI: http://dx.doi.org/10.7322/jhgd.141485 [ Links ]
 Correspondence:
Correspondence:
Italla.bezerra@emescam.br
Manuscript received: August 2018
Manuscript accepted: May 2019
Version of record online: October 2019


{kind=link}
{kind=link}
{kind=link}