










Serviços Personalizados
artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282versão On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.29 no.3 São Paulo set./dez. 2019
http://dx.doi.org/10.7322/jhgd.v29.9527
ORIGINAL ARTICLE
Neonatal and temperament variables predict behavior problems of preterm children at toddlerhood
Variáveis neonatais e de temperamento que predizem problemas de comportamento em crianças nascidas pré-termo na idade pré-escolar
Sofia Muniz Alves Gracioli; Maria Beatriz Martins Linhares
Departament of Neurosciences and Behavior, University of São Paulo Ribeirão Preto Medical School
ABSTRACT
BACKGROUNG: Children born preterm are at high risk for behavior problems at different ages. To better understand these problems, we examine the predictive biopsychosocial variables
OBJECTIVE: To examine the predictive effects of neonatal clinical status and the temperament of the children and mothers on the behavior problems of children born preterm. : Longitudinal predictive study
METHODS: The sample was composed of 40 children born preterm at 18 to 36 months of age and their mothers. The temperament of the children was assessed using the Early Childhood Behavior Questionnaire, which comprises the negative affect, extroversion and effortful control factors and their domains. Behaviors were assessed using the Child Behavior Checklist 1 ½-5 (total, internalized, and externalized problems scores and classifications). The temperament of the mothers was assessed using the Adult Temperament Questionnaire. All instruments were applied through interviews with mothers. Descriptive and the hierarchical multiple linear regression statistical analyses were performed. The level of significance adopted in the study was p ≤ 0.05
RESULTS: The prediction analysis revealed that the internalized behavior problems were explained significantly by children's temperaments with more fear (negative affect) and less by mothers' temperament with inhibitory control (effortful control factor). The externalized behavior problems were explained significantly by greater time spent in the neonatal intensive care unit, less effortful control of children's temperament and less mothers` temperament inhibitory control
CONCLUSION: The behavior problems of children at toddlerhood who were born preterm were explained by high neonatal clinical risk as well as by the temperament dispositional traits of both the children and the mothers
Keywords: temperament; preterm birth; behavior problems; toddlerhood.
Authors summary
Why was this study done?
To examine the predictive effects of neonatal clinical status and the temperament of the children and mothers on the behavior problems of children born preterm
What did the researchers do and find?
The temperament of the children was assessed using the Early Childhood Behavior Questionnaire, which comprises the negative affect, extroversion and effortful control factors and their domains. Behaviors were assessed using the Child Behavior Checklist 1 ½-5 (total, internalized, and externalized problems scores and classifications). The temperament of the mothers was assessed using the Adult Temperament Questionnaire. All instruments were applied through interviews with mothers.
The prediction analysis revealed that the internalized behavior problems were explained significantly by children's temperaments with more fear (negative affect) and less by mothers' temperament with inhibitory control (effortful control factor). The externalized behavior problems were explained significantly by greater time spent in the neonatal intensive care unit, less effortful control of children's temperament and less mothers` temperament inhibitory control..
What do these findings mean?
The behavior problems of children at toddlerhood who were born preterm were explained by high neonatal clinical risk as well as by the temperament dispositional traits of both the children and the mothers. The findings is relevant to be considered in the follow-up preventive programs os premature infants
INTRODUCTION
Preterm birth represents a high-risk factor for child development in several areas and at different ages1,2. Preterm infants show great vulnerability for behavior problems with features dependent on the level of prematurity3. Children born preterm exhibited both externalized3-5 and internalized behavior problems6,7, as well as poor developmental self-regulation8 and executive functioning9. With respect to externalized behaviors, attention problems were detected in children born preterm at pre-school age3,10-12 and school age13-15. Furthermore, among the internalized behaviors, anxiety disorders are the dominant emotional problem16.
There remains a great challenge to understand the mechanisms of these behavior problems in this vulnerable population of children born preterm. Thus, individual and contextual variables should be examined regarding their influence on child behavior outcomes. On the one hand, temperament is an individual factor that could represent a relevant key to better understanding the emotional and behavioral problems in children. Temperament refers to individual differences regarding two broad aspects of behavior - as emotional motor and attentional reactivity and as a self-regulatory process that modulates such reactivity17. Temperament, which appears early in life, is influenced over time by heredity, maturation, and experience18.
The behavior problems are associated with temperament dimensions and traits related to child development. For example, a difficult temperament is associated with a high risk for behavior problems19, while a temperament with a low inhibitory control and a high level of anger and impulsivity at an early age is a predictor of externalized behavior problems for pre-school age children20. However, there are few studies regarding the relationship between behavior problems and temperament profiles among preterm children21,22.
On the other hand, parenting care represents a relevant contextual factor that moderates child behavior outcomes. Parenting educational practices can effectively regulate children's emotional23,24 and behavioral responses24. In the vulnerable preterm sample, the sensitive and non-hostile parenting behavior of mothers moderated the association between early pain stress during the neonatal phase and later internalized behaviors at 18 months of age7. The relationship between child temperament and high behavior inhibitory control was a predictor of child anxiety disorders, and, interestingly, this relationship was exacerbated by the mother's anxiety and overly protective parenting behaviors25. Moreover, the maternal emotion-related socialization behaviors were found to play a role in the toddlers´ self-regulation among low-income at-risk populations26.
In the literature, we detected well-established associations between child behavior problems, temperament traits, and educational parenting practices. However, to our knowledge, no studies have examined the associations between child behavior outcomes, child temperament, and mothers' temperament dispositional traits in preterm children. Thus, to better understand the mechanisms that explain the behavior problems in children born preterm it is relevant to consider together the temperament traits of both the children and their mothers/caregivers. The aim of the present study is to examine the predictive effects of children's neonatal clinical status and children's and mothers' temperament on behavior problems of preterm children between the ages of 18 to 36 months. Additionally, the secondary objective is to estimate the prevalence of behavior problems among this sample.
METHODS
This is a longitudinal predictive study.
Participants
The sample of the present study included 40 children born preterm and who, at the time of the study, were between the ages of 18 to 36 months and their respective mothers. The inclusion criteria for the children were as follows: gestational age < 37 weeks, birth weight <1,500 grams, age 18 to 36 months and son of the biological mothers who were also the main caregivers of the children. The exclusion criteria were as follows: mothers with cognitive impairments and/or mental health problems and/or mothers taking medications that affect their level of conscientiousness as these factors could interfere negatively on the mothers` perceptions when reporting data.
The children were born in a university hospital in southeastern Brazil (Hospital of Clinics, Ribeirão Preto Medical School, University of São Paulo). The sample was generated based on a search performed in the register of the Neonatology Division of the Department of Pediatrics and the outpatient-integrated system of the hospital. We identified 177 eligible participants in one year of data. Of these, 71 mothers could not be located. Of the 106 remaining participants, three mothers refused to participate in the study, five mothers could not participate because they presented with cognitive impairments, and 58 mothers did not attend the appointment for the assessment. Thus, the final sample was comprised 40 children and their mothers.
Ethical Issues
The study was approved by the Research Ethics Committee of the Hospital of Clinics of the Ribeirão Preto Medical School, University of São Paulo at Ribeirão Preto (SP, Brazil). The children's mothers signed informed consent forms.
Instrument and Measures
The Early Childhood Behavior Questionnaire - (ECBQ)27. (see "Mary Rothbart's Temperament Questionnaires". This questionnaire is composed of 201 items that assess 18 dimensions of temperament in children aged 18 to 36 months. Parents or caregivers were asked to assess the frequency of a given reaction exhibited by their children in specific contexts over the two previous weeks. These assessments were scored on a Likert scale that ranged from one (never) to seven (always). Factorial analysis disclosed the following three-factor structure: negative affectivity (discomfort, fear, frustration, sadness, motor activation, shyness, perceptual sensitivity, as well as an inverted score for soothability); surgency/extraversion (activity level, high-intensity pleasure, positive anticipation, impulsivity, and sociability); and effortful control (inhibitory control, low-intensity pleasure, cuddliness, attentional shifting, and attentional focusing). According to Putnam et al.27, the internal consistency of the scales varied from 0.57 to 0.90 (mean = 0.81), and the inter-respondent agreement varied from 0.09 to 0.57 (mean r= 0.39). According to Klein & Linhares28, the internal consistency of the scales in the Brazilian population, which included a sample from the present study, varied from 0.43 to 0.88 (mean = 0.72).
The Child Behavior Checklist for Ages 1.5 to 5 - CBCL 1½ to 529. The CBCL 1½ to 5, a children's behavior inventory for children aged 18 months to 5 years old, is assessed using parental reporting. Informants assess 99 items related to the behaviors their children have exhibited during the preceding two months using the following scale: 0= not true, 1= somewhat or sometimes true and 2= very true or often true for the child. The CBCL 1 ½ -5 allows for the quick acquisition of standardized assessments and descriptive details of the children's functioning based on the parents' assessments, and it includes two axes (externalizing and internalizing behavior problems) as well as seven scales (emotionally reactive, anxious/depressed, somatic complaints, withdrawn, attention problems, aggressive behavior, and sleep problems). The results are expressed as normalized T-scores as follows: normal (T-score < 65), borderline (T-score 65-69), and clinical (T-score ≥ 70), i.e., the higher the score, the more disruptive the behavior. According to the author, the score may be applied to establish a dichotomous demarcation between disruptive and non-disruptive behavior by clustering borderline and clinical classifications vs. normal classification.
The Adult Temperament Questionnaire (ATQ)30. The ATQ was translated and adapted to Portuguese language (Brazil), with authorization of the authors, by Scott et al,3. This is a self-report tool that assesses the temperament of adults. The domains assessed by the instrument are include anxiety, attention problems and hyperactivity, depression and mood swings, personality traits, risk taking, impulsive behavior, and social interaction. The Questionnaire Hierarchical Listing of Scales includes four factors and their respective dimensions: negative affect (fear: negative affect related to the anticipation of distress; sadness: negative affect and reduced mood and energy levels related to the exposure to suffering, disappointment, and object loss; discomfort: negative affect related to sensory qualities of stimulation including intensity, rate and complexity or visual, auditory, smell/taste, and tactile stimulation; frustration: negative affect related to interruption of ongoing tasks or goal blocking); extraversion/surgency (sociability: enjoyment derived from social interactions and being in the presence of others; positive affect: latency, threshold, intensity, duration, and frequency of experiencing pleasure; high intensity pleasure: pleasure related to situations involving high intensity, rate, complexity, novelty, and incongruity); effortful control (attention control: capacity to focus attention as well as to shift attention when desired; inhibitory control: capacity to suppress inappropriate approach behavior; activation control: capacity to perform an action when there is a strong tendency to avoid it); orienting sensitivity (neutral perceptual sensitivity: detection of slight, low intensity stimuli from within the body and from the external environment; affective perceptual sensitivity: spontaneous emotional valence, conscious cognition associated with low intensity stimuli; associative sensitivity: spontaneous cognitive content that is not related to standard associations with the environment). The ATQ uses the following Likert scale: (1) extremely untrue of you, (2) quite untrue of you, (3) slightly untrue of you, (4) neither true nor false of you, (5) slightly true of you, (6) quite true of you, (7) extremely true of you.
Structured Interview for DSM-III -R - Non-patient version (SCID/NP)31. Interview guide for mental health screening of mothers. Brazilian Association of Market Research Companies (Associação Brasileira das Empresas de Pesquisa) - Criteria for Economic Classification in Brazil (Critério de Classificação Econômica Brasil - CCEB)32. Data are based on the 2003 Socioeconomic Survey by IBOPE (Brazilian Institute of Public Opinion and Statistics/Instituto Brasileiro de Opinião Pública e Estatística). This questionnaire assesses the socioeconomic level of Brazilian families according to the following seven-level ordinal scale where higher scores indicate a higher socioeconomic level: A1 (30-34), A2 (25-29), B1 (21-24), B2 (17-20), C (11-16), D (6-10), and E (zero-5). This questionnaire includes questions, such as "What is the educational level of the head of the household?" and "How many televisions do you have in your home?"
Data Collection
The mothers were invited to participate in the study and freely signed the informed consent prior to their participation. First, to determine the mental health history of the mothers, we applied the SCID-NP. Second, if the mothers and children met the inclusion and criteria, they were included in the sample study. The mothers were interviewed individually to assess their children's behavior using the CBCL 1½ to 5 scale, their children's temperament using the ECBQ scale, and their own temperament using the ATQ scale. The instruments were applied in an alternate order to avoid carry-over effect, and two specialists of pediatric psychology who also possessed expertise and training in psychological assessment collected the data.
Data Analysis
The descriptive statistical analysis was performed, and the prediction models of child behavior problems exhibited at 18 to 36 months of age were analyzed using multiple linear regression analysis. The outcomes include the CBCL 1½ to 5 scores for total behaviors, externalized behaviors, and internalized behaviors. In the prediction analyses, the multicolinearity test was first performed to avoid predictor variables with a strong association between each other in the same model (VIF ≥ 5). Second, the Pearson correlation test was performed among the predictor variables (gestational age, length of stay in neonatal intensive care unit/NICU, and temperament factors and dimensions of children and mothers) and the child behavior problem outcome (predictive variable). Only the predictor variables that presented a statistically significant association (p ≤ 0.05) with the outcome variable were tested in the prediction analysis. Finally, the best model for each outcome tested was the model that exhibited the highest explanatory power (R2) that was composed of the prediction variables that presented statistical significance. The data were analyzed using the Statistical Package for Social Sciences (SPSS, version 19.0; Chicago, IL, USA), and a significance level of 5% was adopted for the study (p ≤0.05).
RESULTS
Sample characteristics
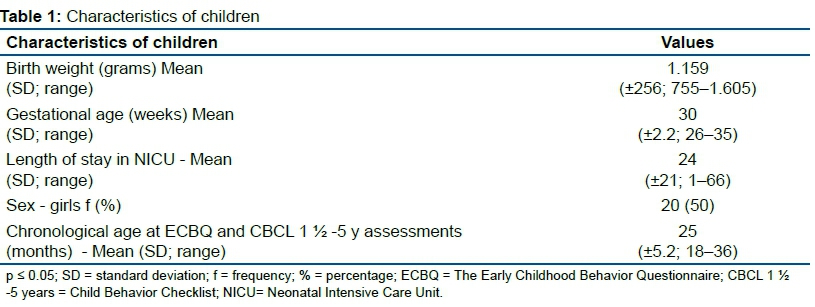
As presented in Table 1, the preterm children born in the present study had a mean birth weight of 1,159 grams and a mean gestational age of 30 weeks, thus indicating the presence of extreme pre-term in the sample. The mean length of stay in the NICU was 24 days. The mean age of the children on the day of assessment was 25 months, with a range from 18 to 36 months.
Complementing the information in Table 1 and focusing on the socio-demographical characteristics, the educational attainment levels of the mothers are as follows: 23 mothers (58%) had only an elementary school level of education, 11 mothers (27%) had a high school level of education, and six mothers (15%) had a college level of education. With respect to employment, 45% of the mothers were employed, while 55% were housewives. Of the mothers in the study, 82% indicated they were in a stable marital relationship. With 80% of the families grouped in the C and D socioeconomic levels, the families were predominantly of low-income status (monthly family income ranging from US$ 212.00 to US$ 522.00 (1 BRL value = US$ 2.31).
Child temperament
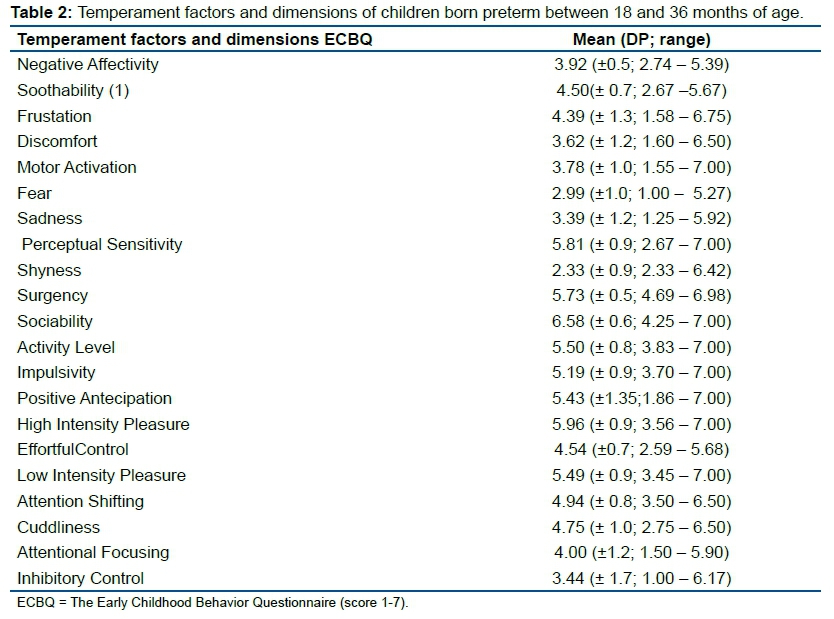
Table 2 indicates that the surgency temperament factor received the highest scores in comparison to the other two factors, at approximately 5 on a 1 to 7 scale, in preterm children aged 18 to 36 months. The negative affectivity temperament factor and its dimensions presented moderate scores of 3 and 4. However, the perceptual sensitivity dimension exhibited a higher score in comparison to the other dimensions with respect to this factor. The effortful control temperament factor also revealed moderate scores, showing high scores in dimensions that contribute to positive behavior regulation processes, albeit, in this temperament factor, the inhibitory control dimension showed lower scores compared to the others.
Child behavior problems
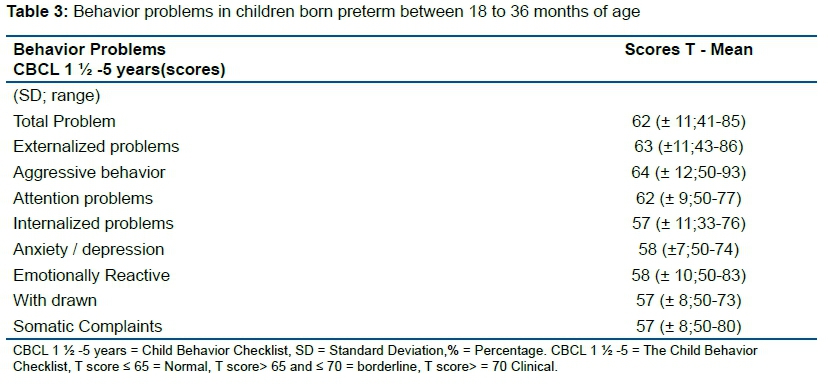
In Table 3, the CBCL 1½ to 5 presented total scores below 65 for the, internalizing and externalizing of behavior problems in preterm children aged 18 to 36 months. The externalizing problems received the highest scores in aggressive behavior.
In addition to the data in Table 3, the clinical levels of the preterm children`s behavior problems are as follows: 19 children (47%) - total behaviors, 19 children (47%) - externalizing axis, and 13 children (32%) - internalizing axis. It is noted that the prevalence of externalized behaviors was higher than that of the internalized behaviors.
Predictive models of child behavior problems
The total behavior problems of children born preterm was predicted in 18% of the sample using the temperament variable frustration (negative affectivity factor) (β = 0.45; p ≤ 0.003). The higher the frustration levels evident in children's temperaments, the higher behavior problems for those children when they were between 18 and 36 months of age (Table 4).
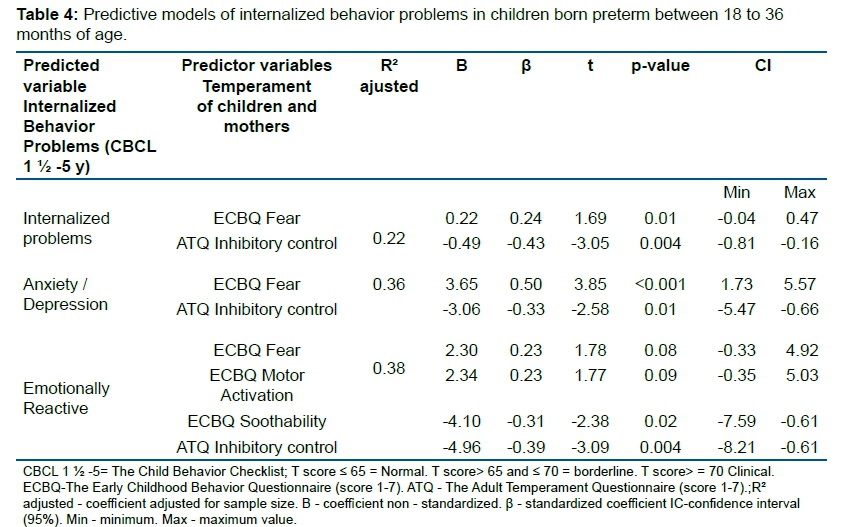
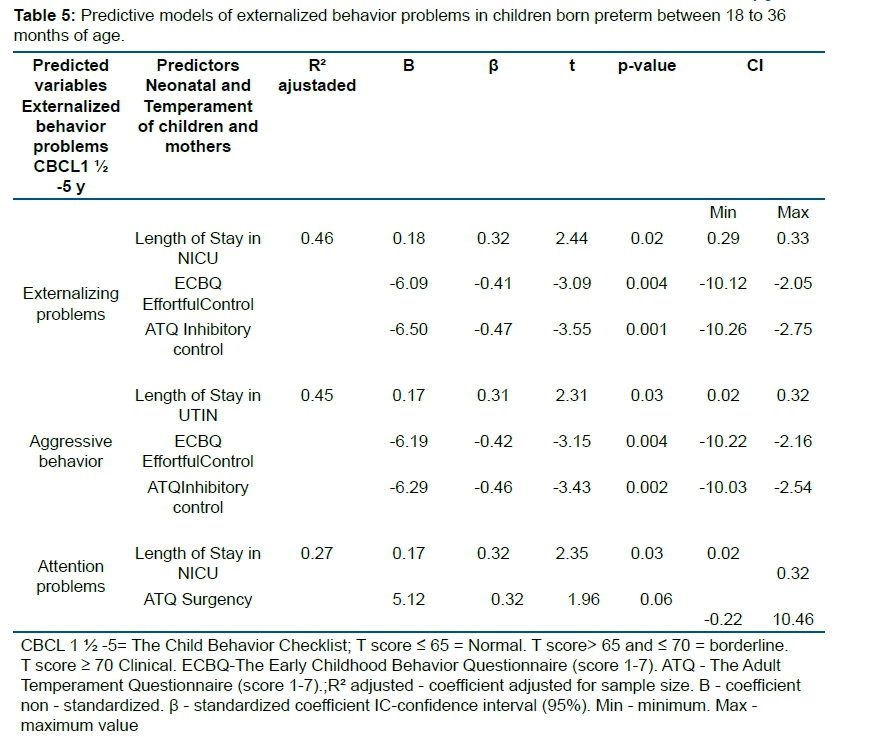
As presented in Table 4, the internalizing behavior problems as well as the anxiety and depression problems in children born preterm were predicted in 22% of the sample based on children`s temperament with respect to fear (negative affectivity factor) and the mothers` temperament with respect to their inhibitory control (effortful control factor). Thus, the higher the level of fear in the children's temperament and the lower the level of inhibitory control of the mothers, the greater the children's internalizing behavior problems when they were between 18 and 36 months of age. Moreover, the children`s emotional reaction problems were explained by four variables of temperament - children`s fear, motor activity, soothability and mothers` inhibitory control. The higher levels of fear and motor activity combined with lower levels of soothability are associated with the mothers' lower levels of inhibitory control, and thus, with increased emotional reaction problems in preterm children aged 18 to 36 months. In all three models of prediction, the mothers` temperament dimension demonstrated the highest weight in explaining children's behavior problems on the internalization axis (Table 5).
Table 5 indicates that the externalized behavior problems, and in particular aggressive behavior, in children born preterm was predicted in 46% and 45%, respectively, by the preterm infants' length of stay in the NICU, the children`s effortful control temperament factor, and the mothers` inhibitory control temperament. That is, the longer the stay in the NICU during the neonatal phase, which is associated with children's lower levels of effortful control during toddlerhood and the mothers` inhibitory control, the greater the externalized behavior problems in preterm children aged 18 to 36 months. In these two models of prediction, the mothers` temperament dimension presented the highest weight with respect to explaining the children's externalized behavior outcomes. Finally, the attention problems in children born preterm were predicted in 27% of the sample based on the length of time in the NICU and the mothers` surgency temperament factor such that the longer the stay in the NICU and the higher the mothers` surgency score, the more severe the attention problems in preterm children aged 18 to 36 months.
DISCUSSION
The prevalence rates of behavior problems in preterm children aged 18 to 36 months were 47% for total behaviors, 47% for externalized behavior problems and 32% for internalized behavior problems at the clinical level. Moreover, the prevalence of behavior problems in the present preterm sample was higher in comparison to children born full term1,33,34. Of note is that the sample of the present study had high-risk neonatal clinical status with a mean of 1,159 grams and 30 weeks gestational age, which represents an extreme preterm status. Those infants in the sample who presented as extremely preterm and of very low birth weight usually exhibited more behavior problems throughout the development trajectory than did children born full-term34 and children born late/moderate preterm35.
The present findings add to the literature that examines the prediction models of behavior problems in preterm children at toddlerhood. The models combined various relevant variables of children's neonatal clinical status and their temperament dispositional traits at toddlerhood as well as the temperaments of the mothers. The models of prediction regarding total behavior problems showed that 18% of the problems were explained by the frustration dimension in children born preterm. Frustration, a dimension of the negative affect factor, was related to interruption of an ongoing task or objectives27.
Focusing on the internalized axis, 22% of the behavior problems were explained by children's fear, which is a dimension of the affect negativity temperament factor and the mother's inhibitory control, which is a dimension of the effortful control temperament factor. The higher the child's fear dimension combined with the mother's low level of inhibitory control, the higher the internalizing behavior problems. Mothers who had difficulty with inhibitory control failed to regulate and moderate their own behaviors as well as the behaviors of their children. In addition, these same factors explained 36% of preterm children's anxiety and depression symptoms according to the DSM-IV scales of the CBCL 1 ½ -5. Children who fail to control negative affective behaviors experience limitations in exhibiting adaptive behaviors in social interactions36. Furthermore, the inhibition of emotional expressions, such as anger and sadness, provoke high levels of internalized behavior problems along with anxiety and symptoms of depression37. The extremely low gestational age infants showed greater emotional reactivity and more self-comforting behaviors than did the very low gestational age infants38.
The mothers` temperament tended to influence their children's behaviors. Very low gestational age children whose mothers were less responsive and sensitive in their interactions with their infants at three months of age, showed internalized behavior problems at 8 years of age39. Mothers who demonstrated overly protective behaviors associated with anxiety symptoms negatively affected on children's development25. Conversely, mothers who exhibited an effortful control temperament factor and who spent more time with their children positively impacted the effortful control temperament trait in their children at 18 months of age40. The mothers` behaviors could either exacerbate or buffer the risk factor with respect to the development of preterm infants, depending on the parenting educational practices they have adopted41.
The higher the maternal sensitivity, the fewer the internalized behaviors problems in preterm children. However, mothers with less sensitivity had children with more difficult temperaments and more behaviors problems42. The mothers of children who are more withdrawn must encourage spontaneity and behavior choices in their children43. These findings support the relevance of the parents` stimulation, and they especially emphasize that the mothers` behaviors may impact their children's behaviors.
Regarding the externalized behaviors, 46% of these problems, and more specifically 45% of aggressive behaviors, were explained by the following variables: length of stay in the NICU, children`s effortful control at toddlerhood and maternal inhibitory control. Furthermore, the externalized behavior problems in children born preterm were explained by the length of stay in the NICU together with the temperament traits of children's effortful control and mothers' inhibitory control. The longer the stay in the NICU combined with lower levels of children's effortful control and lower levels of maternal inhibitory control, the higher the externalized problems of the preterm children. It is relevant to note that the maternal temperament trait was the main variable in explaining the externalized behavior problems of preterm children in the present study. The length of stay in the NICU is a strong parameter regarding the criticality of the illness of the preterm infants in the present study during early development stages, which is consistent with the high-risk profile of the present sample.
As evidenced in the literature, children born preterm presented more externalized problems than did their full-term counterparts44. On the other hand, taking the effortful control temperament dispositional traits of children and mothers together could contribute to a better understanding of the externalized behavior problems. The low effortful control factor included low intensity pleasure, inhibitory control, and focalization of attention, all of which predicted externalized behavior problems45.
Additionally, in the present study, the attention problems in children born preterm were explained by their length of stay in the NICU combined with the mothers` surgency temperament dimension variables. Children born preterm with low birth weight, in comparison to full-term children, presented more attentional problems, more internalized behaviors, and poorer executive functioning46.
The mothers who experienced difficulty in stopping or moderating their undesirable behaviors also exhibited problems regulating the emotions and behaviors of their children47. The mothers of children born preterm, in comparison to their full-term counterparts, offered less support to their children and were more intrusive, frequently interfering with their children's autonomous behavior48,49. The higher the level of extraversion and the lower the effortful control in children, the higher the aggressive behaviors exhibited in school50.
Maternal intrusiveness and harsh control were related to increased levels of expressed anger among toddlers, while maternal sensitivity was related to lower levels of child anger, increased play behaviors and higher levels of attention manipulation51. Moreover, children born preterm demonstrated less maternal scaffolding, less emotional regulation, more negative affect, and less mutual enjoyment in play situations than did their full-term counterparts52.
As previously demonstrated, the maternal emotional related socialization promotes the development of an early self-regulatory system, thus contributing effectively to children's emotional social development26. Children's temperaments were influenced by the quality of their interactions with their mothers, and the maternal sensitivity and responsiveness were predictors of the sensitivity perceptual dimension of temperament of infants at 12 months of age53. The mothers with high sensitivity and responsiveness were better able to interpret precisely the responses of their children and consequently to direct their attention to the stimulus. These mothers` behaviors promote the attention competence in children associated with their perceptual sensitivity.
The findings of the present study show the relationship of mothers` dispositional traits related to temperament and children`s behavior during toddlerhood. The mothers of the present study do not support the behavior of children born preterm, which could be a risk factor that exacerbates negative excitement among children, and consequently, this could negatively influence the self-regulation developmental process. The quality of mother-child interactions at early ages promotes effective child development54,55. Caregivers sensitive to behavior hints were efficacious in reducing distress and negative emotions of children56. Accordingly, mothers act as external co-regulators of children's behaviors, thus promoting development, particularly as it relates to the self-regulation process56,57.
The present study has some limitations. First, the present study analyzed a convenience sample. Second, temperament and behavior problems were assessed by a single informant`s report based on the perception of the mothers. Third, the children`s temperaments were assessed through hetero-report questionnaires and did not use complementary data from structured observations.
Future studies should be addressed the following aspects: a) longitudinally temperament and behavior problems assessment to examine the stability of the present findings throughout childhood development, b) combine the assessment of temperament using both interviews and observational procedures, c) employ multiple informants to assess consistencies among the data provided by the caretaker, and d) assess the characteristics of children's and mothers' temperaments relative to parenting educational practices.
Acknowledgments
The authors are thankful for the financial support from the Coordination for the Improvement of Higher Level of Education Personnel (CAPES, Brazil) to SMAG and from The National Council for Scientific and Technological Development (CNPq, Brazil) to MBML. The authors also thank the Neonatology Service at the Hospital of Clinics of Ribeirão Preto Medical School, University of São Paulo and the families for participating in this study.
REFERENCES
1.Vieira MEB, Linhares MBM. Developmental outcomes and quality of life in children born preterm at preschool and school age. J Pediatr. 2011;87(4):281-91. DOI: http://dx.doi.org/10.1590/S0021-75572011000400003 [ Links ]
2.Arpi E, Ferrari F. Preterm birth and behaviour problems in infants and preschool-age children: a review of the recent literature. Dev Med Child Neurol. 2013;55(9):788-96. DOI: http://dx.doi.org/10.1111/dmcn.12142 [ Links ]
3.Scott MN, Taylor HG, Fristad MA, Klein N, Espy KA, Minich N, et al. Behavior disorders in extremely preterm/extremely low birthweight children in kindergarten. J Dev Behav Pediatr. 2012;33(3):202-13. DOI: http://dx.doi.org/10.1097/DBP.0b013e3182475287 [ Links ]
4.Groote I, Vanhaesebrouck P, Bruneel E, Dom L, Durein I, Hasaerts D, et al. Outcome at 3 years of age in a population-based cohort of extremely preterm infants. Obstet Gynecol. 2007;110(4):855-64. DOI: http://dx.doi.org/10.1097/01.AOG.0000284447.43442.55 [ Links ]
5.Woodward LJ, Moor S, Hood KM, Champion PR, Foster-Cohen S, Inder TE, et al. Very preterm children show impairments across multiple neurodevelopmental domains by age 4 years. Arch Dis Child Fetal Neonatal Ed. 2009;94(5): F339-44. DOI: http://dx.doi.org/10.1136/adc.2008.146282 [ Links ]
6.Espírito Santo JL, Portuguez MW, Nunes ML. Cognitive and behavioral status of low birth weight preterm children raised in a developing country at preschool age. J Pediatr. 2009;85(1):35-41. DOI: http://dx.doi.org/10.1590/S0021-75572009000100007 [ Links ]
7.Vinall J, Miller SP, Synnes AR, Grunau RE. Parent behaviors moderate the relationship between neonatal pain and internalizing behaviors at 18 months corrected age in children born very prematurely. Pain. 2013;154(9):1831-9. DOI: http://dx.doi.org/10.1016/j.pain.2013.05.050 [ Links ]
8.Feldman R. The development of regulatory functions from birth to 5 years: Insights from premature infants. Child Dev. 2009; 80(2):544-61. DOI: http://dx.doi.org/10.1111/j.1467-8624.2009.01278.x [ Links ]
9.Sun J, Mohay HA, O'Callaghan M. A comparison of executive function in very preterm and term infants at 8 months corrected age. Early Hum Dev. 2009;85(4):225-30. DOI: http://dx.doi.org/10.1016/j.earlhumdev.2008.10.005 [ Links ]
10.Caravale B, Tozzi C, Albino G, Vicari S. Cognitive development in low risk preterm infants at 3-4 years of life. Arch Dis Child Fetal Neonatal Ed. 2005;90(6):F474-9. DOI: http://dx.doi.org/10.1136/adc.2004.070284 [ Links ]
11.Mikkola K, Ritari N, Tommiska V, Salokorpi T, Lehtonen L, Tammela O, et al. Neurodevelopmental outcome at 5 years of age of a national cohort of extremely low birth weight infants who were born in 1996-1997. Pediatrics. 2005;116(6):1391-400. DOI: http://dx.doi.org/10.1542/peds.2005-0171 [ Links ]
12.Mikkola K, Kushnerenko E, Partanen E, Serenius-Sirve S, Leipälä J, Huotilainen M, et al. Auditory event-related potentials and cognitive function of preterm children at five years of age. Clin Neurophysiol. 2007;118(7):1494-502. DOI: http://dx.doi.org/10.1016/j.clinph.2007.04.012 [ Links ]
13.Fallang B, Oien I, Hellem E, Saugstad Od, Hadders-Algra M. Quality of reaching and postural control in young preterm infants is related to neuromotor outcome at 6 years. Pediatr Res. 2005;5892):347-53. DOI: http://dx.doi.org/10.1203/01.PDR.0000170898.60160.09 [ Links ]
14.Jeyaseelan D, O'Callaghan M, Neulinger K, Shum D, Burns Y. The association between early minor motor difficulties in extreme low birth weight infants and school age attentional difficulties. Early Hum Dev. 2006;82(4):249-55. DOI: https://doi.org/10.1016/j.earlhumdev.2005.10.012 [ Links ]
15.Bayless S, Stevenson J. Executive functions in school-age children born very prematurely. Early Hum Dev. 2007;83(4):247-54. DOI: https://doi.org/10.1016/j.earlhumdev.2006.05.021 [ Links ]
16.Gagne JR, Van Hulle CA, Aksan N, Essex MJ, Goldsmith HH. Deriving childhood temperament measures from emotion-eliciting behavioral episodes: Scale construction and initial validation. Psychol Assess. 2011;23(2):337-53. DOI: https://doi.org/10.1037/a0021746 [ Links ]
17.Rueda MR, Rothbart MK. The influence of temperament on the development of coping: the role of maturation and experience. In: Skinner EA, MJ Zimmer-Gembeck MJ. Coping and the development of regulation: new directions for child and adolescent development. San Francisco: Jossey-Bass, 2009; p.19-31. [ Links ]
18.Rothbart MK, Putnam S. Temperament and socialization. In: Pulkinnen L, Caspi A. Paths to successful development: Personality in the life course. Cambridge: Cambridge University Press, 2002; p.19-45. [ Links ]
19.Derauf C, LaGasse L, Smith L, Newman E, Shah R, Arria A, et al. Infant temperament and high risk environment relate to behavior problems and language in toddlers. J Dev Behav Pediatr. 2011;32(2):125-35. DOI: https://doi.org/10.1097/DBP.0b013e31820839d7 [ Links ]
20.Eisenberg N, Vaughan J, Hofer C. Temperament, self-regulation, and peer social competence. In: Bukowski WM, Laursen B, Rubin KH. Handbook of peer interactions, relationships, and groups. New York: Guilford Press, 2009; p.473-89. [ Links ]
21.Gracioli SMA, Linhares MB. Temperament related to emotional and behavioral problems in preschool. Psicol Estud. 2014;19(1):71-80. DOI: http://dx.doi.org/10.1590/1413-7372189590007 [ Links ]
22.Cosentino-Rocha L, Linhares MBM. Child temperament and gender differences. Paidéia. 2013;23(54):63-72. DOI: http://dx.doi.org/10.1590/1982-43272354201308 [ Links ]
23.Stifter CA, Bono MA. The effect of infant colic on maternal self-perceptions and mother-infant attachment. Child Care Health Dev. 1998;2495):339-51. DOI: http://dx.doi.org/10.1046/j.1365-2214.2002.00088.x [ Links ]
24.Piotrowski JT, Lapierre MA, Linebarger DL. Investigating correlates of self-regulation in early childhood with a representative sample of English-Speaking American Families. J Child Fam Stud. 2013;22(3):423-36. DOI: http://dx.doi.org/10.1007/s10826-012-9595-z [ Links ]
25.Hudson JL, Dodd HF, Lyneham HJ, Bovopoulous N. Temperament and family environment in the development of anxiety disorder: Two-year follow-up. J Am Acad Child Adolesc Psychiatry. 2009;50(12):1255-64. DOI: http://dx.doi.org/10.1016/j.jaac.2011.09.009 [ Links ]
26.Brophy-Herb HE, Stansbury K, Bocknek E, Horodynski MA. Modeling maternal emotion-related socialization behaviors in a low-income sample: relations with toddlers' self-regulation. Early Child Res Q. 2012;27(3):352-64. DOI: https://doi.org/10.1016/j.ecresq.2011.11.005 [ Links ]
27.Putnam SP, Gartstein MA, Rothbart MK. Measurement of fine-grained aspects of toddler temperament: the early childhood behavior questionnaire. Infant Behav Dev. 2006;29(3):386-401. DOI: https://doi.org/10.1016/j.infbeh.2006.01.004 [ Links ]
28.Klein VC, Linhares MBM. Temperament, behavior and painful experience in the child development course. Paidéia. 2007;17(36):33-44. DOI: http://dx.doi.org/10.1590/S0103-863X2007000100004 [ Links ]
29.Achenbach TM, Rescorla LA. Child Behavior Checklist for Ages 1 ½-5. Burlington: ASEBA, 2000. [ Links ]
30.Evans DE, Rothbart MK. Development of a model for adult temperament. J Res Personality. 2007;41(4):868-88. DOI: https://doi.org/10.1016/j.jrp.2006.11.002 [ Links ]
31.Del Ben CM, Zuardi AW. Estudo da confiabilidade do diagnóstico psiquiátrico obtido através da Entrevista Clínica Estruturada para o DSM-III-R (SCID) em um serviço ambulatorial de um Hospital Escola. Dissertação (Mestrado) - Faculdade de Medicina de Ribeirão Preto, Universidade de São Paulo. Ribeirão Preto: 1995. [ Links ]
32.Associação Brasileira das Empresas de Pesquisa (ABEP). Critério de Classificação Brasil. ABEP, 2003. [ Links ]
33.Delobel-Ayoub M, Arnaud C, White-Koning M, Casper C, Pierrat V, Garel M, et al. Behavioral problems and cognitive performance at 5 years of age after very preterm birth: the EPIPAGE study. Pediatrics. 2009;123(6):1485-92. DOI: https://doi.org/10.1542/peds.2008-1216 [ Links ]
34.Schiariti V, Hoube JS, Lisonkova S, Klassen AF, Lee SK. Caregiver-reported health outcomes of preschool children born at 28 to 32 weeks' gestation. J Dev Beh Pediatr. 2007; 28(1):9-15. DOI: https://doi.org/10.1097/01.DBP.0000257516.52459.33 [ Links ]
35.Rose SA, Feldman JF, Jankowski JJ. A cognitive approach to the development of early language. Child Dev. 2009;80(1):134-50. DOI: https://doi.org/10.1111/j.1467-8624.2008.01250.x [ Links ]
36.Calkins SD. Regulatory competence and early disruptive behavior problems: the role of physiological regulation. In: Olson SL, Sameroff AJ. Biopsychosocial regulatory processes in the development of childhood behavioral problems. New York: Cambridge University Press, 2009; p.86-115. [ Links ]
37.Betts J, Gullone E, Allen JS. An examination of emotion regulation, temperament and parenting as potential predictors of adolescent depression risk status. Br J Dev Psychol. 2009; 27(Pt 2):473-85. DOI: https://doi.org/10.1348/026151008x314900 [ Links ]
38.Maclean PC, Erickson SJ, Lowe JR. Comparing emotional reactivity and regulation in infants born ELGA and VLGA. Infant Beh Dev. 2009;32(3):336-9. DOI: https://doi.org/10.1016/j.infbeh.2009.02.005 [ Links ]
39.Laucht M, Esser G, Schmidt MH. Differential development of infants at risk for psychopathology: the moderating role of early maternal responsivity. Dev Med Child Neurol. 2001;45(5):292-300. DOI: https://doi.org/10.1017/s0012162201000561 [ Links ]
40.Bridgett DJ, Gartstein MA, Putnam SP, Lance KO, Iddins E, Waits R, et al. Emerging effortful control in toddlerhood: The role of infant orienting/regulation, maternal effortful control, and maternal time spent in caregiving activities. Infant Beh Dev. 2011;34(1):189-99. DOI: https://doi.org/10.1016/j.infbeh.2010.12.008 [ Links ]
41.Bates JE, Goodnight JA, Fite JE, Staples AD. Behavior regulation as the product of temperament and environment. In: Olson SL, Sameroff AJ. Biopsychosocial regulatory processes in the development of childhood behavioral problems. New York: Cambridge University Press, 2009; p.116-43. [ Links ]
42.Bradley RH, Corwyn RF. Infant temperament, parenting, and externalizing behavior in first grade: A test of the differential susceptibility hypothesis. J Child Psychol Psychiatry. 2008;49(2): 124-31. DOI: https://doi.org/10.1111/j.1469-7610.2007.01829.x [ Links ]
43.Sclafani JD. The educated parent: recent trends in raising children. Westport: Praeger Publishers, 2004. [ Links ]
44.Schirmer CR, Portuguez MW, Nunes ML. Clinical assessment of language development in children at age 3 years that were born preterm. Arq Neuropsiquiatr. 2006;64(4):926-31. DOI: http://dx.doi.org/10.1590/S0004-282X2006000600007 [ Links ]
45.Prior M, Bavinb EL, Cinic E, Reillyc S, Brethertond L, Wake M, et al. Influences on communicative development at 24 months of age: Child temperament, behaviour problems, and maternal factors. Infant Beh Dev. 2008;31(2):270-9. DOI: http://dx.doi.org/10.1016/j.infbeh.2007.11.001 [ Links ]
46.Aarnoudse-Moens CS, Weisglas-Kuperus N, van Goudoever JB, Oosterlaan J. Meta-analysis of neurobehavioral outcomes in very preterm and/or very low birth weigth children. Pediatrics. 2009;124(2):717-28. DOI: http://dx.doi.org/10.1542/peds.2008-2816 [ Links ]
47.Henderson HA, Fox NA. Considerations in studying emotion in infants and children. In: Coan JA, Allen JJB. The handbook of emotion elicitation and assessment. New York: Oxford University Press, 2007; p.827-64. [ Links ]
48.Cassiano RGM, Linhares MBM. Temperament, prematurity and mother-child interaction behavior. Psicol Reflex Crit. 2015;28(2):416-24. DOI: http://dx.doi.org/10.1590/1678-7153.201528222 [ Links ]
49.Barratt MS, Roach MA, Leavitt LA. The impact of low-risk prematurity on maternal behavior and toddler outcomes. Int J Beh Dev. 1996;19(3):581-602. DOI: https://doi.org/10.1177/016502549601900308 [ Links ]
50.Gunnar MR. Integrating neuroscience and psychological approaches in the study of early experiences. Ann N Y Acad Sci. 2003;1008:238-47. DOI: https://doi.org/10.1196/annals.1301.024 [ Links ]
51.Feldman R, Dollberg D, Nadam R. The expression and regulation of anger in toddlers: Relations to maternal behavior and mental representations. Infant Beh Dev. 2011;34(2):310-20. DOI: https://doi.org/10.1016/j.infbeh.2011.02.001 [ Links ]
52.Erickson SJ, Duvall SW, Fuller J, Schrader R, MacLean P, Lowe J.R Differential associations between maternal scaffolding and toddler emotion regulation in toddlers born preterm and full term. Early Hum Dev. 2013;89(9):699-704. DOI: https://doi.org/10.1016/j.earlhumdev.2013.05.003 [ Links ]
53.Gartstein MA, Marmion J. Fear and Positive affectivity in infancy: convergence/discrepancy between parent-report and laboratory-based indicators. Infant Behav Dev. 2008;31(2):227-38. DOI: https://doi.org/10.1016/j.infbeh.2007.10.012 [ Links ]
54.Morris AS, Morris MDS, Silk JS, Steinberg L, Aucoin KJ, Keyes AW. The influence of mother-child emotion regulation strategies on children's expression of anger and sadness. Dev Psychol. 2011;47(1):213-25. DOI: https://doi.org/10.1037/a0021021 [ Links ]
55.Potharst EV, Schuengel C, Last BF, van Wassenaer AG, Kok JH, Houtzager BA. Difference in mother-child interaction between preterm- and term-born preschoolers with and without disabilities. Acta Pediatr. 2012;101(6):597-603. DOI: https://doi.org/10.1111/j.1651-2227.2012.02599.x| [ Links ]
56.Bernier A, Carlson SM, Whipple N. From external regulation to self-regulation: early parenting precursors of young children's executive functioning. Child Dev. 2010;81(1): 326-39. DOI: https://doi.org/10.1111/j.1467-8624.2009.01397.x [ Links ]
57.Sameroff AJ. Conceptual issues in studying the development of self-regulation. In: Olson SL, Sameroff AJ. Biopsychosocial regulatory processes in the development of childhood behavioral problems. New York: Cambridge University Press, 2009; p.1-18. [ Links ]
 Correspondence:
Correspondence:
sofiagracioli@yahoo.com.br linhares@fmrp.usp.br
Manuscript received: September 2018
Manuscript accepted: August 2019
Version of record online: October 2019


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}