










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores
Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282versão On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.29 no.3 São Paulo set./dez. 2019
https://doi.org/10.7322/jhgd.v29.9528
ORIGINAL ARTICLE
Preterm newborns undergoing selective correction surgery of the patent ductus arteriosus: is there still space for these procedures?
Renán PradoI, II; José Carlos Arteaga CamachoI; Raul Armando Micalay ParedesI; Fernando Magalhães CoutinhoI; Mariane Albuquerque Lima RibeiroII, III; Andrés Ricardo Pérez RieraII
ISanta Marcelina Hospital, Santa Marcelina College, São Paulo, SP, Brazil
IILaboratory of Studies Design and Scientific Writing. University Health Center ABC. Santo André, SP, Brazil
IIIHealth and Sports Science Center. Federal University of Acre, UFAC. Acre, Brazil
ABSTRACT
INTRODUCTION: The ductus arteriosus is a small fetal structure that connects two large arteries (aorta and pulmonary) but becomes pathological when it is maintained after birth. Morbidities associated with persistent patent ductus arteriosus (PDA) may lead to the conclusion that the best approach is early surgical treatment. However, there is evidence that expectant (more selective) surgical management may reduce the chances of unnecessary surgeries and their risks.
OBJECTIVE: To analyze the clinical and surgical profile of preterm newborns submitted to selective correction surgery of the patent ductus arteriosus.
METHODS: This paper contemplates a series of cases, in which all patients submitted to the surgical treatment of PDA in preterm infants were described retrospectively (2009-2016), through the analysis of medical records of the Santa Marcelina Hospital, SP-Brazil.
RESULTS: During this period, there were 13 cases of premature infants who underwent selective surgical correction of PDA. Gestational age was 26.92 weeks, maternal age ranged from 15 to 44, birth weight varied between 650 and 1500g, mostly women (61.54%). The diameter of the ductus arteriosus ranged from 1.7 to 4.1 mm, four patients had complex congenital heart disease (30.77%). The median courses of indomethacin were 1.77, congestive heart failure was shown in 11 patients (84.62%), the median age at surgery was 27.69 days and the median duration of orotracheal intubation was 22.62 days. The weight of the newborns at the time of the surgical act varied between 900 and 1820g. The postoperative complications were mostly infectious, with nine patients with bronchopneumonia (69.23%), one patient had pneumothorax. Sepsis occurred in two cases (15.35%) that died due to the same complication (15.35%).
CONCLUSION: All preterm newborns who underwent surgery had birth weight less than 1500g. The median arterial canal was 3.05 mm in diameter. The median gestational age was 26.92 weeks and 62% of the cases were female. The most frequent surgical technique was the triple clipping, there was no bleeding or reoperation in this series of cases.
Keywords: patent ductus arteriosus, cardiac surgery, preterm newborn, congenital heart disease, low birth weigth newborn.
Authors summary
Why was this study done?
This study was performed to report the surgical results and their complications of the patent ductus arteriosus correction in preterm infants at Santa Marcelina Hospital-SP between January 2009 and July 2016.
What did the researchers do and find?
It was performed the database at the Heart Surgery Department of Santa Marcelina Hospital to extract all cases of preterm newborn patients who had undergone surgery to repair the congenital defect. Soon after, the electronic medical records of the patients' hospitalization data were collected. During the study period, 13 patients who underwent surgery and had a birth weight of less than 1500g were found. The average of ductus arteriosus was 3.05 mm in diameter. Gestational age average was 26.92 weeks and 62% of the cases were female. The most frequent surgical technique was triple clipping, with no bleeding or reoperation in this series of cases.
What do these findings mean?
Selective PDA surgery is still needed nowadays to increase the chance of survival of these newborns diagnosed with PDA and with clinical signs of respiratory and/or heart failure.
The triple clipping technique proved to be highly effective.
Surgical indication was generally in patients with moderate to large ductus arteriosus with congestive heart failure.
INTRODUCTION
Ductus arteriosus is a small arteriosus structure which communicates two big arteries with different resistances (aorta and pulmonar), normally present in the infant in which becomes pathological when kept after birth1. The patent ductus arteriosus (PDA) has different clinic presentations, from newborn, newborns which present symptoms only in adult life to newborns with hemodynamical instability on the first days of birth.
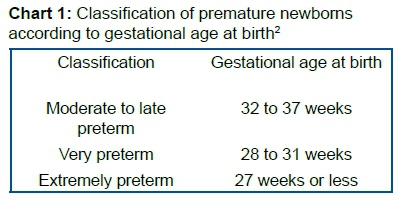
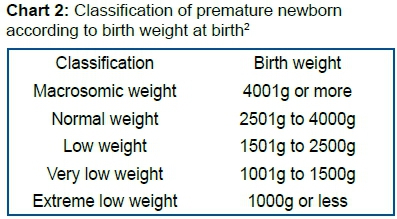
With technological advances and new knowledges and therapeutic strategies, the borders of fetal viability and neonatal have been expanded and more and more, extremely preterm infants and with really low weight (classified with the weight under 1.500g when born and born prior 28 weeks of gestation) have survived2 (Table 1 and 2). However, is still seen and elevated complications rate, long hospitalization and severe disabilities on these infants3,4.
Cardiovascular system changes are frequent on the preterm infant and among them, the patent ductus arteriosus being the one most mentioned5-12 (Chart 1 and 2).
The PDA occurs in 5 to 10% of the neonates to term with the congenital heart disease13,14, showing preference for the feminine gender (relation gender feminine-masculine 1:3)15.
On the premature, the incidences can variate to 20% to 60%, depending on the diagnostic standards used and the population studied16,17, but on average, around 50% of all preterm infants presents patent ductus arteriosus5,7,9,11,12. The gestational age and the weight when born are deeply connected to patent ductus arteriosus in preterm neonates18.
In premature infants with gestational age under 26 weeks, the prevalence of PDA can get to 65%10,19 and on those with weight minor than 1200g at birth, this prevalence is at 80%7 being the biggest cause of morbidity and mortality on this population of newborns20-23.
On the clinical-surgical conduction of the newborn with PDA, is necessary to identify the groups that will get benefits with the pharmacologic treatment, seen that in reason of the low weight, the prevalent low gestational age and the immune system of the premature infant, this will always be the best therapeutic strategy. However, done with this strategy, the clinic correction is a must for the hemodynamic stability and the raise of chances of survival on the infants with low-weight and low gestational age.
Therefore, the objective is to analyze the clinical-surgical profile of the premature infants diagnosed with patent ductus arteriosus and undergoing selective cardiac surgery.
METHODS
It is an report of a series of cases, cross-sectional24 and retrospective of newborns submitted to surgical treatment of patent ductus arteriosus (PDA) in preterm infant through the analyses of medical records and doppler echocardiographic lauds held in the Department of Cardiac Surgery of Santa Marcelina Hospital, located in the city São Paulo/SP, Brazil, in the period of January of 2009 to June of 2016.
The surgical procedure begins with a posterolateral thoracic incision with 1,5 to 2,0 cm, dissection of the subcutaneous and muscle, dissection of costal pleura or opening of the pleura till the medium mediastinum. Dissection of the ductus arteriosus, triple clipping with the surgical clips according to the size of the ductus, pleural drainage (when it opened) with water seal and closing.
Place of study
The Santa Marcelina Hospital (HSM) is a private philanthropic institution located in the city of São Paulo, Brazil. It has 700 beds and performs more than 1200 surgeries per month, which 80% are medium and high complexity, being a regional reference and also for other states.
It is performed around 350 births monthly. The adopted protocol of this institution is, mainly, an pharmacological approach, with use of indomethacin and, in unresponsive cases or that your use is contraindicated, is adopted the selective surgical treatment, which only can occur when its seen clinical complications due the patent ductus arteriosus, being basically, cardiac or respiratory failure which can be presented for the impossibility of orotracheal extubation.
Population and sample
The population studied included all the premature newborns, with gestational age at birth under than 37 weeks, underwent surgical treatment of Patent Ductus Arteriosus (PDA) at Santa Marcelina Hospital (HSM) in the city of São Paulo in the period of January 2009 to June 2016.
Data base analysis
It was used the ExcelTM 2013 programs to elaborate the data base and the version 21.0 of the SPSS (Statistical Package for Social Research) program for statistical analysis. The described statistics was done through average, standard deviation, median, minimum and maximum.
Ethical aspects
The research was approved by the Committee of Ethics in research of the Santa Marcelina Hospital, SP-Brazil (CAAE 15136019.6.0000.0066). For the beginning of this study it was drawn up a Term of Responsibility to make sure that the researcher would follow with his duty to elaborate and execute this job in agreement with Resolution no. 466/12 of the National Health Council (BR)25.
All participants were informed about the goal and procedures involved on the research and, after accepting to participate, it was asked the signature of the Term of Free and Informed Consent.
RESULTS
It was analyzed the data base of 13 premature newborns undergoing surgical treatment following the protocol of selective ligation of the hospital studied.
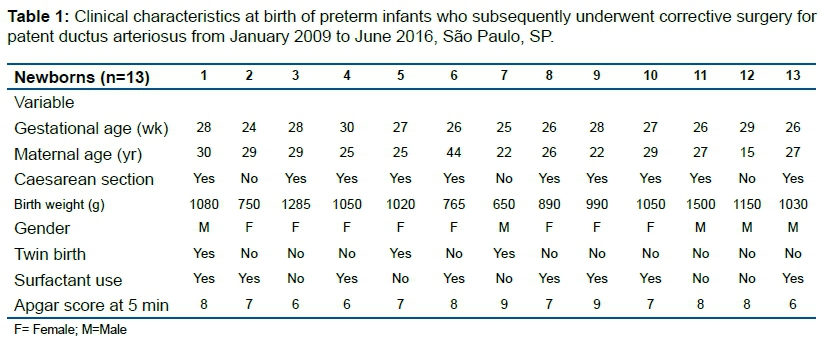
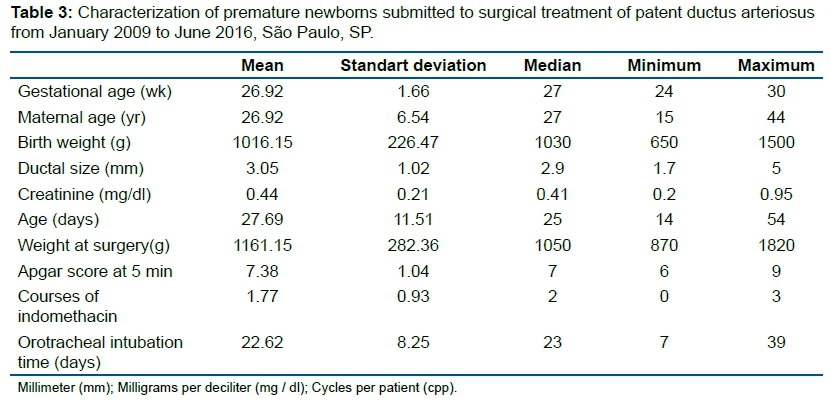
The gestational age variated between 24 and 30 weeks (Table 1) and average of 26,92 weeks (Table 3). Mother's age variated between 15 and 44 years old (Table 1), the median being 27 years old (Table 3), being eight newborns of the feminine gender (61,54%) and ten being delivered by cesarean section (76,92%). There were twins' births in three cases (23,08%) and the use of surfactant in nine cases (69,23%) according to Table 1. The Apgar test26 on the first 5 minutes of life variated between 9 and 6 points (Table 1), average 7,38 (Table 3) and the weight at birth variated between 650g to 1500g (Table 1), with average of 1016,15g (Table 3).
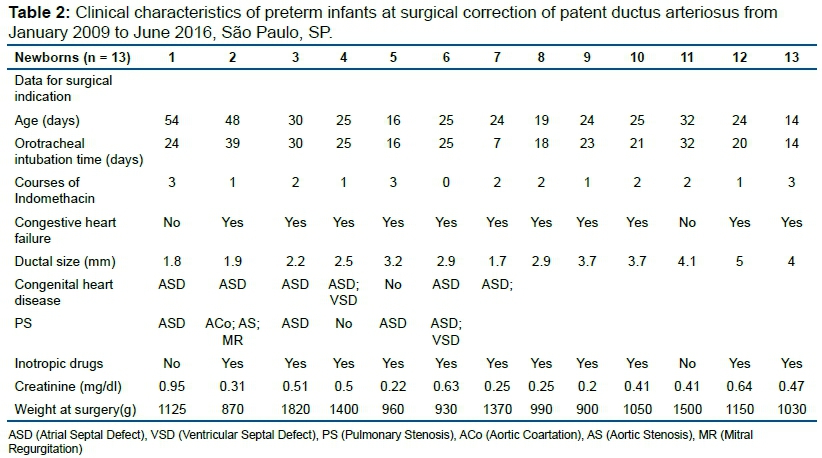
For surgical decision, clinical, laboratory and echocardiographic data were considered, as described in Table 2.
The number of indomethacin cycles ranged from zero to three (Table 2) with average of 1.77 cycles (Table 3). Congestive heart failure with vasoactive drugs was evident in 11 cases (84.62%). The age of the preterm infants during surgery ranged from 14 to 54 days (Table 2) and the average was 27.69 days (Table 3).
Orotracheal intubation time ranged from 7 to 39 days (Table 2), with average of 22.62 days (Table 3). Creatinine ranged from 0.2 to 0.95 mg/dl (Table 2), with an average of 0.44 mg/dl (Table 3) and the newborn's weight at the time of surgery ranged from 900 to 1820 grams (Table 2) with an average of 1161.15g (Table 3). The echocardiogram showed that the diameter of the ductus arteriosus varied between 1.7 and 5 mm (Table 2) and its average was 3.05 mm (Table 3). Two newborns had no other associated congenital heart disease (15.38%); four newborns had complex congenital heart disease described in Table 2 (30.77%) and seven newborns had PDA associated solely with atrial septal defect (ASD) (53.85%) (Table 2).
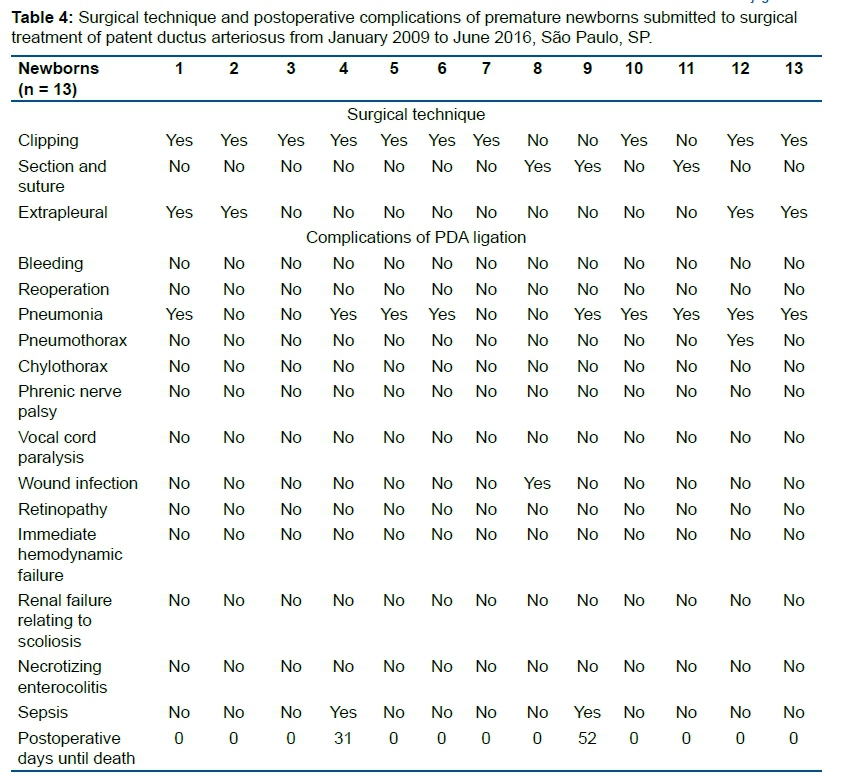
Table 4 shows the surgical techniques used, having the triple clipping performed on ten newborns (76.92%); a section and suture technique of the ductus arteriosus with absorbable thread PDS with diameter of 6-0 was used in three cases (23,08%) and the extrapleural technique without posterior thoracic drainage in four cases (30,77%).
Most of the postoperative complications were infectious. Nine newborns presented bronchopneumonia (69.23%) and in one pacient was showed superficial wound infection (7.69%). One patient presented pneumothorax and sepsis occurred in two cases (15.35%), which died due to the same complication (15.35%). Deaths were observed on the 31st and 52nd postoperative days (Table 4).
DISCUSSION
The PDA is a heart condition most common between premature infants. In the beginning of the 90s, it was reported rates of 40 to 55% of premature newborns with less than 29 weeks of gestation and/or weight under 1500g in birth27-29.
However in this decade, it is reported rates from 60 to 70% of prematures under 29 weeks of gestation and, in proximally two thirds of the cases, it doesn't occur the spontaneous closure of the ductus arteriosus30-33. Besides, around 50% of the neonates weighting <1000g progressed with PDA symptomatic having the need of intervention32.
The literature does not correlate maternal age with the incidence of PDA, and in the present study, it was found that the mother's age ranged from 15 to 44 years.
Persistent ductus arteriosus remains hemodynamically significant in premature infants for a variety of reasons, including decreased ductal sensitivity to partial oxygen pressure, increased circulating PGE2, and increased ductal tissue sensitivity to PGE2 and nitric oxide7,34-36.
Hemodynamically significant PDA is associated with left to right shunt of the systemic blood with subsequent pulmonary volume overload and a diastolic deficit that results in vital organ hypoperfusion. In infants with very low weight, symptomatic PDA increases the risk of prolonged ventilation, oxygen requirement, pulmonary hemorrhage37 and bronchopulmonary dysplasia38-40.
Diastolic deficit is associated with renal hypoperfusion41, intestinal ischemia, necrotizing enterocolitis, reduced speed of the blood flux in the medium brain artery42-45 retinopathy of prematurity and decreased of flow in the superior vena cava with increased risk of intraventricular hemorrhage46,47. If not properly treated, complications of symptomatic PDA can lead to death48.
The relationship between patent ductus arteriosus and necrotizing enterocolitis is controversial. Although population studies have reported an association between PDA and necrotizing enterocolitis49-51, there are no randomized controlled trials in the medical literature examining the desirability of continuing or stopping enteral feeding in the presence of PDA.
The treatment is initially clinical. This way, the preterm hemodynamic variables are first stabilized. We try to improve the gas exchange of oxygen and carbon dioxide by surfactant injection (this occurred in nine newborns of the present study), it´s done oxygen supplementation, stabilization of the neonate temperature, balance blood volume and vasoactive drugs are administered when heart failure is present, parameters that are related to the initial state of the preterm infant (in this study, for example, the Apgar test at birth was observed between 9 and 6 points, with average of 7.38).
When echocardiographic confirmation of PDA exists, pharmacological treatment can be included with the administration of non-steroidal anti-inflammatory drugs (usually indomethacin or ibuprofen). The first to report the use of non-steroidal anti-inflammatory drugs in the treatment of PDA were Friedman and colleagues and Heymann and colleagues. Both works being from 197652,53.
Because indomethacin inhibits the synthesis of all prostaglandins, several adverse effects may occur, including necrotizing enterocolitis, spontaneous intestinal perforation54, alteration of renal function55, altered cerebral vascular self-regulation56, retinopathy, pulmonary edema or hemorrhage, and thrombocytopenia. Similar effects have been observed with ibuprofen57 although they may be less frequent.
Although it wasn't analyzed the cases of PDA solved with pharmacological treatment in the hospital of the study, it is possible to state that the drug approach was performed protocollary with intravenous indomethacin in 100% of the cases.
However, there are criteria to contraindicate the use of cyclooxygenase inhibitors such as active bleeding (especially intracranial or gastrointestinal bleeding), thrombocytopenia, renal failure (increased creatinine (> 120 µmol/L) or oliguria (<0.5 mL/kg/h)), confirmation or suspicion of necrotizing enterocolitis58.
Due to these contraindications and also the fact that not all pharmacologically treated neonates for persistent ductus arteriosus respond satisfactorily59, surgical PDA ligation can be a reasonable alternative in a high-risk population as it results in the definitive closure of the ductus and, therefore, can prevent associated neonatal morbidities and accelerate extubating and weaning of vasoactive drugs60. However, the procedure (thoracotomy) is associated with its own set of morbidities: hypothermia, intraoperative bleeding, wound infection, pneumothorax, chylothorax, postoperative hypotension, vocal fold paralysis (recurrent nerve), phrenic nerve paralysis, infection and scoliosis61-63.
The correct timing that must be done the surgical approach for closure of the ductus arteriosus is still controversial. Some authors suggest an early surgical approach, also known as "early ligation"64-66, others suggest a more expectant surgical approach ("selective ligation"), which would occur only after unresponsive pharmacological treatment and with significant hemodynamic changes31,32,60,67,68 and there are those who prefer non-surgical treatment, arguing that the risks of surgical intervention outweigh the benefits and that conservative pharmacological treatment is ideal for these newborns, as they focus on spontaneous duct closure69-71.
Palder et al.72 and Trus et al.29 argue that surgical ligation should be the first option of treatment when compared to the use of indomethacin in preterm infants weighing less than 800g for the fact that extremely low birth weight infants have a poor response to pharmacological treatment73. Some studies indicate that 40% of cases, there is no response to the drug approach74,75 and preterm infants weighing less than 1000g respond even less to indomethacin76. Also, about 87% of newborns weighing less than 1000g can initially have their ductus arteriosus closed with the use of indomethacin, but in 47% of cases the canals open again77.
Still in relation to the line supporting the early surgical approach, approximately four decades ago, several randomized controlled studies examined the impact of symptomatic PDA surgical ligation on neonatal pulmonary morbidity48,49,78,79. These studies not only demonstrated that surgical PDA ligation decreased the need for prolonged ventilatory support, but also avoided morbidity and mortality associated with cardiopulmonary insufficiency observed in infants who were not submitted to artery duct ligation78,79. Lee et al.66 further concluded that "early ligation" may decrease the incidence of necrotizing enteritis and improve intolerance to oral feeding in preterm infants. However, these findings are still a matter of controversy among neonatologists80.
On the other hand, the line of conduct that defends selective ligation advocates that this approach only indicates surgical treatment for those newborns who remain with heart failure or respiratory failure, despite clinical treatment with mechanical ventilation and vasoactive drugs31,60,67,68,81.
The defenders of selective ligation understand that the surgical procedure has its own complications and, since preterm infants have a high rate of spontaneous closure of the PDA during the first two years after birth69,71 early ligation may expose the preterm infants to surgery which they don't need67.
With improvements in the medical management of neonates, the surgical approach could be seen as the last step in the treatment of PDA, since sick children may have pharmacological support which allows their growth and, eventually, later perform transcatheter intervention (hemodynamic interventionist procedure with no need of surgery) in case the ductus arteriosus does not close spontaneously60.
Proponents of the pharmacological approach often conduct observational studies suggesting that surgical attachment of the PDA is associated with an increased incidence of chronic lung disease, bronchopulmonary dysplasia, necrotizing enterocolitis, and retinopathy of prematurity33. The results described in the present study were related to surgical ligation. It is believed that the selective indication (ie, later) for the closure of the ductus arteriosus in preterm infants may decrease the number of cases to be operated and, consequently, the complications of the procedure, being them short or long term31,60,67,68,81.
Analyzing the work of Jhaveri et al.31, the indication for surgical treatment is inversely proportional to gestational age; between 24 and 25 weeks of gestation, surgery was indicated in 81% of cases, while for neonates between 26 and 27 weeks, there was surgical indication in 56% of cases. As the data presented in this study is from a series of surgical cases, it was not possible to compare this information, however, the average gestational age ranged from 24 to 30 weeks, with an average of 26.92 weeks with a standard deviation of 1.66.
Still regarding the work of Jhaveri et al.31, the researchers found that in only 33% of the cases belonging to the group of neonates who were submmited to selective canal ligation surgery had persistent arterial channels classified echocardiographically as moderate to large in size Kluckow and Evans classification82. However, in the work presented here, 100% of the studied PDAs were of moderate to large size, ranging from 1.7 to 5 mm (average 3.05 mm in diameter).
These divergences could suggest that only the size of the PDA is not a determinant for surgical indication and the hemodynamic repercussion as a criterion for surgery should also be considered. In addition, the one-millimeter diameter difference in ductus arteriosus represents big area difference when considering preterm infants weighing less than 1000g.
The present study only retrospectively evaluated infants who were submitted to selective ductus arteriosus persistent corrective surgery (thirteen cases) and did not consider clinically treated infants. Nine newborns (69.23%) required the use of exogenous pulmonary surfactant; however, it was not enough to generate hemodynamic stability. The average prescribed cycles of indomethacin was 1.77 and ibuprofen was not used. Even so, 11 preterm infants (84.62%) had congestive heart failure, requiring the use of vasoactive drugs and two of them had respiratory failure (15.38%). In the study by Jhaveri et al.31, the main reasons for ligation were increased ventilatory requirements (87%) and/or persistent hypotension requiring inotropic support (39%), which could not be explained by other causes.
It was also observed that the average age of preterm infants at the time of surgery in this study was higher (27.69 days) when compared to the studies by Jhaveri et al.31 which was 23 days and Lee et al.83 which was 15 days. This shows that the indication of newborns for surgical approach by the hospital's Heart Team was even more expectant and conservative in this study.
Another important factor was the difference between birth weight, which ranged from 650g to 1500g with an average of 1016.15g and weight at the time of surgery that ranged from 900 to 1820g, with an average of 1161.15g. It was possible to observe an average gain of approximately 150g. However, the most underweight child who went to surgery gained 720g operating with 1370g and not 650g (important for intraoperative anesthetic control and to avoid sequelae due to the size of the surgical incision).
After the surgical procedures of closure of the ductus arteriosus described in this study, some postoperative complications were observed, most of which were infectious, nine neonates developed bronchopneumonia (69.23%); one patient presented superficial wound infection (7.69%) and one case of pneumothorax (7.69%). The high rate of pneumonia is believed to be related to prolonged preoperative orotracheal intubation time, which ranged from 7 to 39 days, with an average of 22.62 days.
Lehenbauer et al.60 showed the cases of preterm infants who were underwent surgical ligation between 2003 and 2015 and reported that morbidity in preterm infants weighing less than 1000g was 2.4%. In this study, two newborns (1.2%) had pneumothorax requiring chest drainage, one patient (0.6%) had recurrent laryngeal nerve injury, and one patient (0.6%) had significant intraoperative bleeding.
Jhaveri et al.31, Lee et al.83 and Madan et al.84 had postoperative mortality rates of 9%, 19% and 20%, respectively. In the study here presented, there were two cases of sepsis that resulted in death (15.35%). It was observed that the deaths occured 31 and 52 days after the procedure, which leads to clinical rather than surgical complications.
However, it is important to note that both neonates who died also had complex congenital heart disease (PDA + ASD + VSD in one case and PDA + Aortic Coartation + Aortic Stenosis + Mitral Insufficiency in the second case). This association between PDA and other congenital heart disease is not uncommon. There were two newborns with no other heart disease (15.38%), but four newborns had complex heart diseases described in Table 2 (30.77%) and seven newborns had PDA solely associated with atrial septal defect (ASD) (53.85%).
The association of PCA and ASD is frequent in preterm infants, considering that both are physiologically necessary conditions for intrauterine life, and both have the possibility of spontaneous closure. Rivera et al.85 revealed a prevalence of congenital heart disease in low birth weight preterm infants of 13.2: 1000 newborns alive and Guitti86 observed a congenital heart disease rate of 5.5: 1000 newborns alive, regardless of newborn weight.
Jhaveri et al.31 analyzed that the selective approach was associated with decreased canal ligation rates (72% versus 100%, p <0.05). Although preterm infants were exposed to longer PDA shunts for longer periods in the conservative treatment period, the rates of bronchopulmonary dysplasia, sepsis, retinopathy of prematurity, neurological injury and death did not change, and the overall rate of necrotizing enterocolitis was significantly lower.
In this study, it was observed that the surgical clipping technique used in ten cases (76.92%) was highly effective, without the need of reoperation, with 100% resolution and with low complications rate. The sectioning and suturing technique performed in three cases (23.08%) was performed in newborns with very large ductus arteriosus, where the clip sizes did not allow their complete occlusion. The extra pleural technique without posterior thoracic drainage that was performed in four cases (30.77%) was always tried first, but the delicate pleura of the preterm infants and the size of the surgical incision needed to perform the procedure do not always make this technique possible.
Another important parameter to consider is the place where the surgical procedure is performed. Because of the instability of premature infants and the risk of ICU transfer to the operating room, in some centers surgery is routinely performed in neonatal ICUs75,83. In the study presented here all surgeries were performed at the Surgical Center, since the neonatal ICU where the study was performed does not have the necessary infrastructure to perform the surgical ligation on there.
The retrospective nature and modest size of the sample limits the type of analysis that can be performed and the conclusions that can be done. It was not possible to conclude whether expectant conduct was an approach with superior results in case early surgical treatment had been performed.
In addition, this study focused on short-term morbidity and mortality and did not assess the possible complications of these newborns in long-term, such as sensorineural dysfunction.
In conclusion, all preterm infants who were submitted to surgery had a birth weight of less than 1500g. The average ductus arteriosus was 3.05mm in diameter. The average gestational age was 26.92 weeks and 62% of the cases were female. The most frequent surgical technique was triple clipping, there was no bleeding or reoperation in this series of cases. Selective PDA surgery is still needed today to increase the chance of survival of these newborns diagnosed with PDA and with clinical signs of respiratory and or heart failure.
Acknowledgments
We thank Prof. Dr. Luiz Carlos de Abreu for the discussions about the research object and for subsidizing the space for discussions about the subject Scientific Methodology and its applicability in Health Sciences. We also thank the postgraduate student Juliana Zangirolamo-Raimundo for the statistical analysis performed in the elaboration of the analysis of this case series.
Conflict of interest
The authors declare that there is no ethical or interest conflict in presenting the results of this research.
Contributions for the manuscript
Renán Prado: Project design and search of the research scenario, definition of the research object and data collection, discussion and management of the database; José Carlos Arteaga Camacho: Discussion of results and analysis of outcomes; Raul Armando Micalay Paredes: Results Discussion and Outcomes Analysis, Fernando Magalhães Coutinho: Results Discussion and Outcomes Analysis, Mariane Albuquerque Lima Ribeiro: Empirical Literature and Results Discussion, Andrés Ricardo Pérez Riera: Object Design, Design of the study and closing of the final wording of the text.
REFERENCES
1.VettukattiL JJ. Pathophysiology of patent ductus arteriosus in the preterm infant. Curr Pediatr Rev. 2016;12(2):120-2. DOI: http://doi.org/10.2174/157339631202160506002215 [ Links ]
2.World Health Organization (WHO). Born too soon: the global action report on preterm birth. [cited 2019 Mar 10]. Available from: https://www.who.int/pmnch/media/news/2012/201204_borntoosoon-report.pdf. [ Links ]
3.Lemons JA, Bauer CR, Oh W, Korones SB, Papile LA, Stoll BJ, et al. Very low birth weight outcomes of the National Institute of Child health and human development neonatal research network. Pediatrics. 2001;107(1):E1. DOI: http://doi.org/10.1542/peds.107.1.e1 [ Links ]
4.Hintz SR, Poole WK, Wright LL, Fanaroff AA, Kendrick DE, Laptook AR, et al. Changes in mortality and morbidities among infants born at less than 25 weeks during the post-surfactant era. Arch Dis Child Fetal Neonatal Ed. 2005;90(2):F128-33. DOI: http://doi.org/10.1136/adc.2003.046268 [ Links ]
5.Heymann MA, Rudolph AM. Control of the ductus arteriosus. Physiol Rev. 1975;55(1):62-78. DOI: http://doi.org/10.1152/physrev.1975.55.1.62 [ Links ]
6.Lloyd TR, Beekman RH. Clinically silent patent ductus arteriosus. Am Heart J. 1994;127(6):1664-5. DOI: http://doi.org/10.1016/0002-8703(94)90415-4 [ Links ]
7.Clyman RI. Ibuprofen and patent ductus arteriosus. N Engl J Med. 2000; 343(10):728-30. DOI: http://doi.org/10.1056/NEJM200009073431009 [ Links ]
8.Koehne PS, Bein G, Alexi-Meskhishvili V, Weng Y, Bührer C, Obladen M. Patent ductus arteriosus in very low birthweight infants: complication of pharmacological and surgical treatment. J Perinat Med. 2001;29(4):327-34. DOI: http://doi.org/10.1515/JPM.2001.047 [ Links ]
9.Gould DS, Montenegro LM, Gaynor JW, Lacy SP, Ittenbach R, Stephens P, et al. A comparison of on-site and off-site patent ductus arteriosus ligation in premature infants. Pediatrics. 2003;112(6 Pt 1):1298-301. DOI: http://doi.org/10.1542/peds.112.6.1298 [ Links ]
10.Hammoud MS, Elsori HA, Hanafi EA, Shalabi AA, Fouda IA, Devarajan LV. Incidence and risk factors associated with the patency of ductus arteriosus in preterm infants with respiratory distress syndrome in Kuwait. Saudi Med J. 2003;24(9):982-5. [ Links ]
11.Thébaud B, Michelakis ED, Wu XC, Moudgil R, Kuzyk M, Dyck JR, et al. Oxygen-sensitive Kv channel gene transfer confers oxygen responsiveness to preterm rabbit and remodeled human ductus arteriosus: implications for infants with patent ductus arteriosus. Circulation. 2004;110(11):1372-9. DOI: http://doi.org/10.1161/01.CIR.0000141292.28616.65 [ Links ]
12.Locali RF, Matsuoka PK, Gabriel EA, Bertini Júnior A, Rotta CA, Catan R, et al. Tratamento da persistência do canal arterial em recém-nascidos prematuros: análise clínica e cirúrgica. Arq Bras Cardiol. 2008;90(5):345-9. DOI: http://dx.doi.org/10.1590/S0066-782X2008000500007 [ Links ]
13.Carlgren LE. The incidence of congenital heart disease in children born in Gothenburg 1941-1950. Br Heart J. 1959;21(1):40-50. DOI: http://doi.org/10.1136/hrt.21.1.40 [ Links ]
14.Mitchell SC, Korones SB, Berendes HW. Congenital heart disease in 56,109 births. Incidence and natural history. Circulation. 1971;43(3):323-32. DOI: http://doi.org/10.1161/01.cir.43.3.323 [ Links ]
15.Catani LH. Defeitos cardíacos congênitos específicos In: Park MK. Cardiologia pediátrica. 6th ed. Rio de Janeiro: Elsevier, 2015; p. 168. [ Links ]
16.Iyer P, Evans N. Re-evaluation of the left atrial to aortic root ratio as a marker of patent ductus arteriosus. Arch Dis Child Fetal Neonatal Ed 1994;70(2):F112-7. DOI: http://doi.org/10.1136/fn.70.2.f112 [ Links ]
17.Ellison RC, Peckham GJ, Lang P, Talner NS, Lerer TJ, Lin L, et al. Evaluation of the preterm infant for patent ductus arteriosus. Pediatrics. 1983;71(3):364-72. [ Links ]
18.Dice JE, Bhatia J. Patent ductus arteriosus: an overview. J Pediatr Pharmacol Ther. 2007;12(3):138-46. DOI: http://doi.org/10.5863/1551-6776-12.3.138 [ Links ]
19.Costeloe K, Hennessy E, Gibson AT, Marlow N, Wilkinson AR. The EPICure study: outcomes to discharge from hospital for infants born at the threshold of viability. Pediatrics. 2000;106(4):659-71. DOI: http://doi.org/10.1542/peds.106.4.659 [ Links ]
20.Cooke L, Steer P, Woodgate P. Indomethacin for asymptomatic patent ductus arteriosus in preterm infants. Cochrane Database Syst Rev. 2003;(2):CD003745. DOI: http://doi.org/10.1002/14651858.CD003745 [ Links ]
21.Moore P, Brook MM, Heyman MA. Patent ductus arteriosus. In: Allen HD, Driscoll DJ, Shaddy RE, Feltes TF. Heart Disease in Infants, Children and Adolescents: including the fetus and young adults. 7th ed. Baltimore: Williams & Wilkins, 2008; p. 683-702. [ Links ]
22.Noori S, McCoy M, Friedlich P, Bright B, Gottipati V, Seri I, et al. Failure of ductus arteriosus closure is associated with increased mortality in preterm infants. Pediatrics. 2009;123(1):e138-44. DOI: http://doi.org/10.1542/peds.2008-2418 [ Links ]
23.Mezu-Ndubuisi OJ, Agarwal G, Raghavan A, Pham JT, Ohler KH, Maheshwari A. Patent ductus arteriosus in premature neonates. Drugs. 2012;72(7):907-16. DOI: http://doi.org/10.2165/11632870-000000000-00000 [ Links ]
24.Zangirolami-Raimundo J, Echeimberg JO, Leone C. Research methodology topics: Cross-sectional studies. J Hum Growth Dev. 2018;28(3):356-60. DOI: http://dx.doi.org/10.7322/jhgd.152198 [ Links ]
25.Brasil. Conselho Nacional de Saúde (CNS). Resolução 466, de 12 de dezembro de 2012. Diretrizes e normas regulamentadoras de pesquisas envolvendo seres humanos. [cited 2019 Mar 10]. Available from: http://conselho.saude.gov.br/resolucoes/2012/Reso466.pdf [ Links ]
26.Apgar V. A proposal for a new method of evaluation of the newborn infant. Curr Res Anesth Analg. 1953;32(4):260-7. [ Links ]
27.Mouzinho AI, Rosenfeld CR, Risser R. Symptomatic patent ductus arteriosus in very-low-birth-weight infants: 1987-1989. Early Hum Dev. 1991;27(1-2):65-77. DOI: http://dx.doi.org/10.1016/0378-3782(91)90028-2 [ Links ]
28.Reller MD, Rice MJ, McDonald RW. Review of studies evaluating ductal patency in the premature infant. J Pediatr. 1993;122(6):S59-62. DOI: http://dx.doi.org/10.1016/s0022-3476(09)90044-0 [ Links ]
29.Trus T, Winthrop AL, Pipe S, Shah J, Langer JC, Lau GY. Optimal management of patent ductus arteriosus in the neonate weighing less than 800 g. J Pediatr Surg. 1993;28(9):1137-9. DOI: http://dx.doi.org/10.1016/0022-3468(93)90148-e [ Links ]
30.Benitz WE. Treatment of persistent patent ductus arteriosus in preterm infants: time to accept the null hypothesis? J Perinatol. 2010;30(4):241-52. DOI: http://dx.doi.org/10.1038/jp.2010.3 [ Links ]
31.Jhaveri N, Moon-Grady A, Clyman RI. Early surgical ligation versus a conservative approach for management of patent ductus arteriosus that fail to close after indomethacin treatment. J Pediatr. 2010;157(3):381-7. DOI: http://dx.doi.org/10.1016/j.jpeds.2010.02.062 [ Links ]
32.Hamrick SE, Hansmann G. Patent ductus arteriosus of the preterm infant. Pediatrics. 2010;125(5):1020-30. DOI: http://dx.doi.org/10.1542/peds.2009-3506 [ Links ]
33.Bancalari E, Claure N, Gonzalez A. Patent ductus arteriosus and respiratory outcome in premature infants. Biol Neonate. 2005;88(3):192-201. DOI: http://dx.doi.org/10.1159/000087582 [ Links ]
34.Clyman RI. Developmental physiology of the ductus arteriosus. In: Long WA. Fetal and neonatal cardiology. Philadelphia: WB Saunders, 1990; p.64-75. [ Links ]
35.Clyman RI. Patent ductus arteriosus in the premature infant. In: Avery ME. Diseases of the newborn. Philadelphia: WB Saunders, 1998. [ Links ]
36.Brook M, Heymann M. Patent ductus arteriosus. In: Emmanouilides GC, Riemenschneider TA, Allen HD, Gutgesell HP. Moss and adams heart disease in infants, children and adolescents including the fetus and young adult. 5th ed. Baltimore: Williams & Wilkins, 1995; p. 746-64. [ Links ]
37.Kluckow M, Evans N. Ductal shunting, high pulmonary blood flow, and pulmonary hemorrhage. J Pediatr. 2000;137(1):68-72. DOI: http://dx.doi.org/10.1067/mpd.2000.106569 [ Links ]
38.Brown ER. Increased risk of bronchopulmonary dysplasia in infants with patent ductus arteriosus. J Pediatr. 1979;95(5 Pt 2):865-6. DOI: http://dx.doi.org/10.1016/s0022-3476(79)80454-0 [ Links ]
39.Rojas MA, Gonzalez A, Bancalari E, Claure N, Poole C, Silva-Neto G. Changing trends in the epidemiology and pathogenesis of neonatal chronic lung disease. J Pediatr. 1995;126(4):605-10. DOI: http://dx.doi.org/10.1016/s0022-3476(95)70362-4 [ Links ]
40.Bancalari E, Claure N, Sosenko IR. Bronchopulmonary dysplasia: changes in pathogenesis, epidemiology and definition. Semin Neonatol. 2003;8(1):63-71. DOI: http://dx.doi.org/10.1016/s1084-2756(02)00192-6 [ Links ]
41.Hammerman C. Patent ductus arteriosus. Clinical relevance of prostaglandins and prostaglandin inhibitors in PDA pathophysiology and treatment. Clin Perinatol. 1995;22(2):457-79. [ Links ]
42.Martin CG, Snider AR, Katz SM, Peabody JL, Brady JP. Abnormal cerebral blood flow patterns in preterm infants with a large patent ductus arteriosus. J Pediatr. 1982;101(4):587-93. DOI: http://dx.doi.org/10.1016/s0022-3476(82)80715-4 [ Links ]
43.Nestrud RM, Hill DE, Arrington RW, Beard AG, Dungan WT, Lau PY, et al. Indomethacin treatment in patent ductus arteriosus. A double-blind study utilizing indomethacin plasma levels. Dev Pharmacol Ther. 1980;1(2-3):125-36. [ Links ]
44.Shimada S, Kasai T, Konishi M, Fujiwara T. Effects of patent ductus arteriosus on left ventricular output and organ blood flows in preterm infants with respiratory distress syndrome treated with surfactant. J Pediatr. 1994;125(2):270-7. DOI: http://dx.doi.org/10.1016/s0022-3476(94)70210-1 [ Links ]
45.Weir FJ, Ohlsson A, Myhr TL, Fong K, Ryan ML. A patent ductus arteriosus is associated with reduced middle cerebral artery blood flow velocity. Eur J Pediatr. 1999;158(6):484-7. DOI: http://dx.doi.org/10.1007/s004310051125 [ Links ]
46.Dudell GG, Gersony WM. Patent ductus arteriosus in neonates with severe respiratory disease. J Pediatr. 1984;104(6):915-20. DOI: http://dx.doi.org/10.1016/s0022-3476(84)80499-0 [ Links ]
47.Osborn DA, Evans N, Kluckow M. Effect of early targeted indomethacin on the ductus arteriosus and blood flow to the upper body and brain in the preterm infant. Arch Dis Child Fetal Neonatal Ed. 2003;88(6):F477-82. DOI: http://dx.doi.org/10.1136/fn.88.6.f477 [ Links ]
48.Cotton RB, Stahlman MT, Bender HW, Graham TP, Catterton WZ, Kovar I. Randomized trial of early closure of symptomatic patent ductus arteriosus in small preterm infants. J Pediatr. 1978;93(4):647-51. DOI: http://dx.doi.org/10.1016/s0022-3476(78)80910-x [ Links ]
49.Cassady G, Crouse DT, Kirklin JW, Strange MJ, Joiner CH, Godoy G, Odrezin GT, et al. A randomized, controlled trial of very early prophylactic ligation of the ductus arteriosus in babies who weighed 1000 g or less at birth. N Engl J Med. 1989;320(23):1511-6. DOI: http://dx.doi.org/10.1056/NEJM198906083202302 [ Links ]
50.Dollberg S, Lusky A, Reichman B. Patent ductus arteriosus, indomethacin and necrotizing enterocolitis in very low birth weight infants: a population-based study. J Pediatr Gastroenterol Nutr. 2005;40(2):184-8. DOI: http://dx.doi.org/10.1097/00005176-200502000-00019 [ Links ]
51.Sankaran K, Puckett B, Lee DS, Seshia M, Boulton J, Qiu Z, et al. Variations in incidence of necrotizing enterocolitis in Canadian neonatal intensive care units. J Pediatr Gastroenterol Nutr. 2004;39(4):366-72. DOI: http://dx.doi.org/10.1097/00005176-200410000-00012 [ Links ]
52.Friedman WF, Hirschklau MJ, Printz MP, Pitlick PT, Kirkpatrick SE. Pharmacologic closure of patent ductus arteriosus in the premature infant. N Engl J Med. 1976;295(10):526-9. DOI: http://dx.doi.org/10.1056/NEJM197609022951003 [ Links ]
53.Heymann MA, Rudolph AM, Silverman NH. Closure of the ductus arteriosus in premature infants by inhibition of prostaglandin synthesis. N Engl J Med. 1976;295(10):530-3. DOI: http://dx.doi.org/10.1056/NEJM197609022951004 [ Links ]
54.Attridge JT, Clark R, Walker MW, Gordon PV. New insights into spontaneous intestinal perforation using a national data set: (1) SIP is associated with early indomethacin exposure. J Perinatol. 2006;26(2):93-9. DOI: http://dx.doi.org/10.1038/sj.jp.7211429 [ Links ]
55.Vanpée M, Ergander U, Herin P, Aperia A. Renal function in sick, very low-birth-weight infants. Acta Paediatr. 1993;82(9):714-8. DOI: http://dx.doi.org/10.1111/j.1651-2227.1993.tb12544.x [ Links ]
56.Keating P, Verhagen E, van Hoften J, ter Horst H, Bos AF. Effect of indomethacin infused over 30 minutes on cerebral fractional tissue oxygen extraction in preterm newborns with a patent ductus arteriosus. Neonatology. 2010;98(3):232-7. DOI: http://dx.doi.org/10.1159/000283946 [ Links ]
57.Vieux R, Desandes R, Boubred F, Semama D, Guillemin F, Buchweiller MC, et al. Ibuprofen in very preterm infants impairs renal function for the first month of life. Pediatr Nephrol. 2010;25(2):267-74. DOI: http://dx.doi.org/10.1007/s00467-009-1349-9 [ Links ]
58.Hundscheid T, Onland W, van Overmeire B, Dijk P, van Kaam AHLC, Dijkman KP, et al. Early treatment versus expectative management of patent ductus arteriosus in preterm infants: a multicentre, randomised, non-inferiority trial in Europe (BeNeDuctus trial). BMC Pediatr. 2018;18(1):262. DOI: http://dx.doi.org/10.1186/s12887-018-1215-7 [ Links ]
59.Ivey HH, Kattwinkel J, Park TS, Krovetz LJ. Failure of indomethacin to close persistent ductus arteriosus in infants weighing under 1000 grams. Br Heart J. 1979;41(3):304-7. DOI: http://dx.doi.org/10.1136/hrt.41.3.304 [ Links ]
60.Lehenbauer DG, Fraser CD, Crawford TC, Hibino N, Aucott S, Grimm JC, et al. Surgical closure of patent ductus arteriosus in premature neonates weighing less than 1,000 grams: contemporary outcomes. World J Pediatr Congenit Heart Surg. 2018;9(4):419-23. DOI: http://dx.doi.org/10.1177/2150135118766454 [ Links ]
61.Roclawski M, Sabiniewicz R, Potaz P, Smoczynski A, Pankowski R, Mazurek T, et al. Scoliosis in patients with aortic coarctation and patent ductus arteriosus: does standard posterolateral thoracotomy play a role in the development of the lateral curve of the spine? Pediatr Cardiol. 2009;30(7):941-5. DOI: http://dx.doi.org/10.1007/s00246-009-9469-3 [ Links ]
62.Smith ME, King JD, Elsherif A, Muntz HR, Park AH, Kouretas PC. Should all newborns who undergo patent ductus arteriosus ligation be examined for vocal fold mobility? Laryngoscope. 2009;119(8):1606-9. DOI: http://dx.doi.org/10.1002/lary.20148 [ Links ]
63.Moin F, Kennedy KA, Moya FR. Risk factors predicting vasopressor use after patent ductus arteriosus ligation. Am J Perinatol. 2003;20(6):313-20. DOI: http://dx.doi.org/10.1055/s-2003-42693 [ Links ]
64.Ciongoll W, Fiorelli AI, Gaioto FA, Busnardo FF, Cruz LNF, Meira EBS, et al. Tratamento do canal arterial persistente em neonatos prematuros: análise de 18 casos. Rev Bras Cir Cardiovasc. 1993;8(4):282-92. DOI: http://dx.doi.org/10.1590/S0102-76381993000400006 [ Links ]
65.Mosalli R, Alfaleh K. Prophylactic surgical ligation of patent ductus arteriosus for prevention of mortality and morbidity in extremely low birth weight infants. Cochrane Database Syst Rev. 2008;(1):CD006181. DOI: http://dx.doi.org/10.1002/14651858.CD006181.pub2 [ Links ]
66.Lee JH, Ro SK, Lee HJ, Park HK, Chung WS, Kim YH, et al. Surgical ligation on significant patent ductus arteriosus in very low birth weight infants: Comparison between early and late ligations. Korean J Thorac Cardiovasc Surg. 2014;47(5):444-50. DOI: http://dx.doi.org/10.5090/kjtcs.2014.47.5.444 [ Links ]
67.Benitz WE. Patent ductus arteriosus: to treat or not to treat? Arch Dis Child Fetal Neonatal Ed. 2012;97(2):F80-2. DOI: http://dx.doi.org/10.1136/archdischild-2011-300381 [ Links ]
68.Abdel-Hady H, Nasef N, Shabaan AE, Nour I. Patent ductus arteriosus in preterm infants: do we have the right answers. Biomed Res Int. 2013;2013:676192. DOI: http://dx.doi.org/10.1155/2013/676192 [ Links ]
69.Nemerofsky SL, Parravicini E, Bateman D, Kleinman C, Polin RA, Lorenz JM. ductus arteriosus rarely requires treatment in infants > 1000 grams. Am J Perinatol. 2008;25(10):661-6. DOI: http://dx.doi.org/10.1055/s-0028-1090594 [ Links ]
70.Mohamed MA, El-Dib M, Alqahtani S, Alyami K, Ibrahim AN, Aly H. Patent ductus arteriosus in premature infants: to treat or not to treat? J Perinatol. 2017;37(6):652-7. DOI: http://dx.doi.org/10.1038/jp.2017.4 [ Links ]
71.Romagnoli V, Pedini A, Santoni M, Scutti G, Colaneri M, Pozzi M, et al. Patent ductus arteriosus in preterm infants born before 30 weeks' gestation: high rate of spontaneous closure after hospital discharge. Cardiol Young. 2018;28(8):995-1000. DOI: http://dx.doi.org/10.1017/S1047951118000641 [ Links ]
72.Palder SB, Schwartz MZ, Tyson KR, Marr CC. Management of patent ductus arteriosus: a comparison of operative v pharmacologic treatment. J Pediatr Surg. 1987;22(12):1171-4. DOI: http://dx.doi.org/10.1016/s0022-3468(87)80730-3 [ Links ]
73.Cooke RW, Pickering D. Poor response to oral indomethacin therapy for persistent ductus arteriosus in very low birthweight infants. Br Heart J. 1979;41(3):301-3. DOI: http://dx.doi.org/10.1136/hrt.41.3.301 [ Links ]
74.Lee LLC, Tillett A, Tulloh R, Yates R, Kelsall W. Outcome following patent ductus arteriosus ligation in premature infants: a retrospective cohort analysis. BMC Pediatr. 2006;6:15. DOI: http://dx.doi.org/10.1186/1471-2431-6-15 [ Links ]
75.Avsar MK, Demir T, Celiksular C, Zeybek C. Bedside PDA ligation in premature infants less than 28 weeks and 1000 grams. J Cardiothorac Surg. 2016;11(1):146. DOI: http://dx.doi.org/10.1186/s13019-016-0539-3 [ Links ]
76.Little DC, Pratt TC, Blalock SE, Krauss DR, Cooney DR, Custer MD. Patent ductus arteriosus in micropreemies and full-term infants: the relative merits of surgical ligation versus indomethacin treatment. J Pediatr Surg. 2003;38(3):492-6. DOI: http://dx.doi.org/10.1053/jpsu.2003.50086 [ Links ]
77.Rudd P, Montanez P, Hallidie-Smith K, Silverman M. Indomethacin treatment for patent ductus arteriosus in very low birthweight infants: double blind trial. Arch Dis Child. 1983;58(4):267-70. DOI: http://dx.doi.org/10.1136/adc.58.4.267 [ Links ]
78.Malviya MN, Ohlsson A, Shah SS. Surgical versus medical treatment with cyclooxygenase inhibitors for symptomatic patent ductus arteriosus in preterm infants. Cochrane Database Syst Rev. 2013;(3):CD003951. DOI: http://dx.doi.org/10.1002/14651858.CD003951.pub3 [ Links ]
79.Kääpä P, Lanning P, Koivisto M. Early closure of patent ductus arteriosus with indomethacin in preterm infants with idiopathic respiratory distress syndrome. Acta Paediatr Scand. 1983;72(2):179-84. DOI: http://dx.doi.org/10.1111/j.1651-2227.1983.tb09693.x [ Links ]
80.Bose CL, Laughon MM. Patent ductus arteriosus: lack of evidence for common treatments. Arch Dis Child Fetal Neonatal Ed. 2007;92(6):F498-502. DOI: http://dx.doi.org/10.1136/adc.2005.092734 [ Links ]
81.Wickremasinghe AC, Rogers EE, Piecuch RE, Johnson BC, Golden S, Moon-Grady AJ, et al. Neurodevelopmental outcomes following two different treatment approaches (early ligation and selective ligation) for patent ductus arteriosus. J Pediatr. 2012;161(6):1065-72. DOI: http://dx.doi.org/10.1016/j.jpeds.2012.05.062 [ Links ]
82.Kluckow M, Evans N. Early echocardiographic prediction of symptomatic patent ductus arteriosus in preterm infants undergoing mechanical ventilation. J Pediatr. 1995;127(5):774-9. DOI: http://dx.doi.org/10.1016/s0022-3476(95)70172-9 [ Links ]
83.Lee GY, Sohn YB, Kim MJ, Jeon GW, Shim JW, Chang YS, et al. Outcome following surgical closure of patent ductus arteriosus in very low birth weight infants in neonatal intensive care unit. Yonsei Med J. 2008;49(2):265-71. DOI: http://dx.doi.org/10.3349/ymj.2008.49.2.265 [ Links ]
84.Madan JC, Kendrick D, Hagadorn JI, Frantz ID; National Institute of Child Health and Human Development Neonatal Research Network. Patent ductus arteriosus therapy: impact on neonatal and 18-month outcome. Pediatrics. 2009;123(2):674-81. DOI: http://dx.doi.org/10.1542/peds.2007-2781 [ Links ]
85.Rivera IR, Silva MA, Fernandes JM, Thomaz AC, Soriano CF, Souza MG. Congenital heart diseases in the newborn: from the pediatrician's request to the cardiologist's evaluation. Arq Bras Cardiol. 2007;89(1):6-10. DOI: http://dx.doi.org/10.1590/s0066-782x2007001300002 [ Links ]
86.Guitti JC. Epidemiological characteristics of congenital heart diseases in Londrina, Paraná South Brazil. Arq Bras Cardiol. 2000;74(5):395-404. DOI: http://dx.doi.org/10.1590/S0066-782X2000000500001 [ Links ]
 Correspondence:
Correspondence:
renan_prado@hotmail.com
Manuscript received: September 2018
Manuscript accepted: August 2019
Version of record online: October 2019


{kind=link}
{kind=link}
{kind=link}
{kind=link}