










Serviços Personalizados
artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282versão On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.29 no.3 São Paulo set./dez. 2019
http://dx.doi.org/10.7322/jhgd.v29.9530
ORIGINAL ARTICLE
Is there an association between the forced expiratory volume value in the first second and the Asthma Control Test and the degree of control proposed by the Global initiative for Asthma in asthmatic children and adolescents treated with inhaled corticosteroids?
Karla Delevedove Taglia-FerreI; Sandra LisboaII; Luanda Dias da S. SalvianoII; Ana Carolina Carioca da CostaII; Shandra Lisboa MonteiroIII; Hisbello da Silva CamposII; Maria de Fátima Pombo MarchIV
IHospital Infantil Francisco de Assis. Cachoeiro de Itapemirim (ES), Brasil
IIInstituto Nacional de Saúde da Mulher, da Criança e do Adolescente Fernandes Figueira da Fundação Oswaldo Cruz (IFF/Fiocruz) - Rio de Janeiro (RJ), Brasil
IIIAcadêmica da Escola de Medicina Souza Marques. Rio de Janeiro, (RJ), Brasil
IVUniversidade Federal do Rio de Janeiro (UFRJ), Av. Pedro Calmon, 550, Cidade Universitária, Rio de Janeiro, RJ, Brasil
ABSTRACT
OBJECTIVE: To assess the presence of an association between the classification of the degree of asthma control, using the proposal by the Global Initiative for Asthma (GINA), the AsthmaControl Test (ACT)/Childhood-ACT, and forced expiratory volume at 1 second (FEV1), in asthmatic children and adolescents undergoing treatment with inhaled corticosteroids, treated at the National Institute of Women's, Child and Adolescent Health Fernandes Figueira of the Oswaldo Cruz Foundation (IFF/FIOCRUZ)
METHODS: Cross-sectional study, with review of medical records of all children aged 7 to 17 years, followed at the Asthma Outpatient Clinic and referred to the Respiratory Function Test (PFR) sector between March 2013 and September 2014. At the same day the C-ACT/ACT questionnaires, the classification of the degree of asthma control proposed by the GINA were applied and the FEV1 value obtained by spirometric examination.
RESULTS: From the total of medical records evaluated (72), 16 children were excluded because they did not meet the criteria required for spirometry. The sample studied (56 children) showed a predominance of males (58.9%) and a median age of 12 (7-17) years. Association between FEV1 values and GINA was observed (p <0.01_.
CONCLUSION: The results found in this study indicate that FEV1 measurement is a useful component among the instruments for assessing clinical control of asthma by GINA.
Keywords: asthma, questionnaires, children, adolescents, spirometry.
Authors summary
Why was this study done?
Asthma is a heterogeneous disease with a broad genetic basis modulating the behavior of all constitutive and functional cells of the respiratory tract. Altered cellular responses to the different pathogenic factors involved (physical, chemical and biological) produce a wide range of clinical presentations known as phenotypes. This diversity of mechanisms involved generates a variety of clinical presentations and therapeutic responses that make assessing clinical asthma control a challenge. For this, different instruments can be used during asthma follow-up appointments. This study was conducted to investigate whether the results of the asthma control assessment questionnaires (GINA and C-ACT / ACT) are related to FEV1, a spirometric parameter that indicates the degree of bronchial obstruction in order to assist in the therapy decision
What did the researchers do and find?
The medical records of 72 children and adolescents diagnosed with asthma, aged 7 to 17 years old, followed up at the Asthma Outpatient Clinic of the Fernandes Figueira (IFF) / FIOCRUZ and who underwent spirometry with bronchodilator testing in the Respiratory Function Test sector from March 2013 to September 2014. The degrees of asthma control according to the GINA proposal and the C-ACT / ACT questionnaire of these patients were obtained on the same day of the respiratory function test, during consultation with the attending physician. After applying the questionnaires to assess the degree of asthma control, the patients underwent complete spirometry. The medical records collected anthropometric characteristics (age, gender and body mass index) and the ongoing treatment. The daily dose of inhaled corticosteroid (IC) (budesonide or equivalent) was categorized as recommended by GINA 2017. The study remained on 56 patients who met the criteria: use of IC regularly, either alone or in combination with long-acting beta 2 agonist, at least 3 months and had none of the conditions (associated pulmonary comorbidity, inadequately performed spirometric tests, or incorrect completion of the C-ACT/ACT questionnaire).
In the study sample (56 children) , it was found a predominance of males (58.9%) and a median age of 12 (7-17) years. There was a statistical association between FEV1 and GINA values (p <0.01), as well as between FEV1 values and those of C-ACT/ACT scores (p <0.01) in relation to controlled and untreated patients. controlled.
What do these findings mean?
The results found in this study indicate that the measurement of FEV1 is a useful component among the instruments for evaluating clinical asthma control. Apparently, its result is related to the usual tests to evaluate asthma control: GINA and ACT/C-ACT. The study also suggested the possibility that these instruments are not being used as due to guide the most appropriate prescription.
INTRODUCTION
Asthma is a heterogeneous disease, usually characterized by chronic airway inflammation and defined by the history of respiratory symptoms such as wheezing, shortness of breath, chest oppression, and cough that vary over time and intensity, along with varying expiratory airflow1.
Asthmatic treatment is not only aimed at controlling symptoms, but also to prevent exacerbations and decline in pulmonary function1. Clinical evaluation of asthma control is still a challenge. Different instruments can be used during follow-up appointments to aid in therapeutic decision making2,3. One is the control classification proposed by the Global Initiative for Asthma (GINA), which is based on clinical and functional parameters that define three categories: controlled, partially controlled and out of control1. Another instrument is the AsthmaControl Test (ACT). Self-applicable, it has two versions: one for children over 11 and one specific for children from 4 to 11 years old (Childhood-ACT (C-ACT). In both, values equal to or greater than 20, the asthmatic is classified as controlled; if less than 20, poorly controlled4,5. In addition to these instruments, spirometric parameters, such as forced expiratory volume in one second (FEV1) and forced vital capacity (FVC), are useful in assessing the degree of bronchial obstruction and in assessing asthma control and therapeutic response2.
The main medications used in asthma treatment can be divided into two categories: bronchodilators and anti-inflammatory drugs. Among the bronchodilators, inhaled beta2-agonists (SABA) and long-acting beta-agonists (LABA) are the most commonly used. In the anti-inflammatory class, inhaled corticosteroids (IC) are the most effective. Regular use of CI-LABA inhalation combination achieves better results in the treatment of symptomatic asthmatics6.
The aim of this study was to investigate whether the results of the asthma control assessment questionnaires (GINA and C-ACT/ACT) are related to FEV1, a spirometric parameter that indicates the degree of bronchial obstruction.
METHODS
Study design
This is a cross-sectional study7.
Place and period of study
The study was conducted at the Asthma Outpatient Clinic (AOC) of the Fernandes Figueira (IFF)/FIOCRUZ National Institute of Women's, Child and Adolescent Health who underwent spirometry with bronchodilator testing (PBD) in the Respiratory Function Test (PFR) laboratory. From March 2013 to September 2014.
Population of study
Patients diagnosed with asthma, aged 7 to 17 years, treated at the Asthma Outpatient Clinic during the study period. Children under 7 years were not included as spirometric analysis in this age group is performed by z-score and not by predicted percentages.
Calculation and sample size
For sample composition, children and adolescents would have to be able to perform spirometry with the acceptability and reproducibility criteria required for the test result and complete the self-administered C-ACT/ACT questionnaire. However, of the 72 children and adolescents evaluated, 16 were excluded from the study due to the following conditions: associated pulmonary comorbidity, inadequately performed spirometric tests, or incorrect completion of the C-ACT/ACT questionnaire.
Data Collection Procedures
The asthma control degrees according to the GINA proposal and the C-ACT/ACT questionnaire were obtained on the same day of the respiratory function test during the consultation with the attending physician.
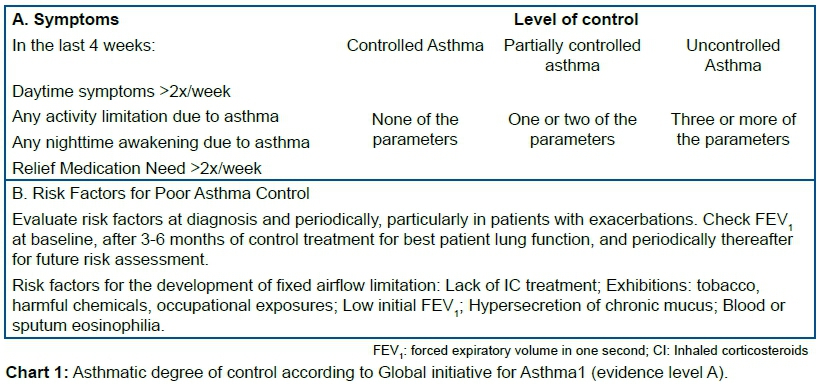
The evaluation of the degree of asthma control according to the proposal of GINA1 (Chart 1) evaluates two domains: the symptomatic response to the therapy instituted in the last 4 weeks and the future risk of exacerbations (through FEV1). By classification, patients are categorized as: controlled, partially controlled and uncontrolled, as observed in chart 1.
The C-ACT/ACT8 is a self-administered questionnaire for clinical assessment of asthma control over the past four weeks, consisting of simple questions about the frequency and intensity of symptoms. It is a validated instrument for children aged 4-11 years (C-ACT) and for children aged 12 and over (ACT). When children are under 12, they and their guardians answer the questions. Those older than or equal to 12 years respond alone. In the end, they are stratified according to the following scores:
C-ACT:
>20 points - controlled asthma;
≤19 points - uncontrolled asthma.
ACT:
20 to 25 points - controlled asthma;
16 to 20 points - partially controlled asthma;
5 to 15 points - uncontrolled asthma.
After applying the questionnaires to assess the degree of asthma control, the patients underwent complete spirometry. All spirometric tests analyzed in this study were performed according to the standards established by the American Thoracic Society and European Respiratory Society (ATS/ERS) 20059. Spirometry was always performed by the same professional on the Master Screen® spirometer, Jaeger, Wurzburg, Germany. All expiratory maneuvers were performed without and with bronchodilator and archived in their original sequence. The patients met all the requirements for the exam. For bronchodilator response, 400μg inhaled salbutamol was used through an expansion chamber. Fifteen minutes after drug administration, each child underwent a new spirometry to analyze the bronchodilator response. Spirometric results were interpreted as VOD when observed, a FEV1/FVC ratio below the lower limit of normality (LIN) of the 50th percentile. Spirometry was considered normal when the FEV1/FVC ratio was above the upper limit of normality (ULN). In addition, spirometric results are used to classify the obstructive, restrictive or mixed ventilatory disorder10.
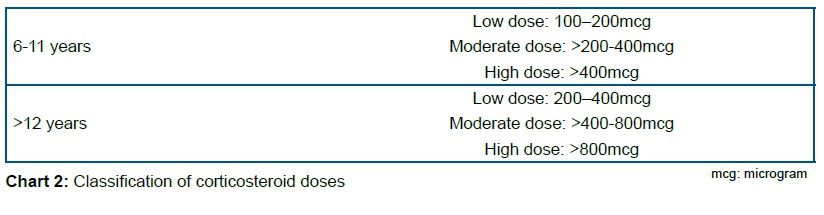
The medical records collected anthropometric characteristics (age, gender and body mass index - BMI) and the ongoing treatment. The daily dose of inhaled corticosteroid (IC) (budesonide or equivalent) was categorized as recommended by GINA 2017 (Chart 2)1.
Data analysis
Mean values and respective standard deviations were recorded for continuous variables with normal distribution. For continuous variables without normal distribution, the median values (minimum and maximum) were recorded. Categorical variables were described as absolute and percentage frequencies. The relationship between the degree of asthma control measured by GINA, the C-ACT/ACT and the FEV1 measurement was assessed by analysis of variance (ANOVA). The analyzes were conducted using SPSS version 20 software with a significance level of 5% as reference. To make the graphs we used the program R version 3.2.
Ethical aspects of research
This study was approved by the Research Ethics Committee (CEP) of HUAP - UFF on June 13, 2014 (CMM/HUAP No. 686.801 - CAEE: 31282314.2.0000.5243).
RESULTS
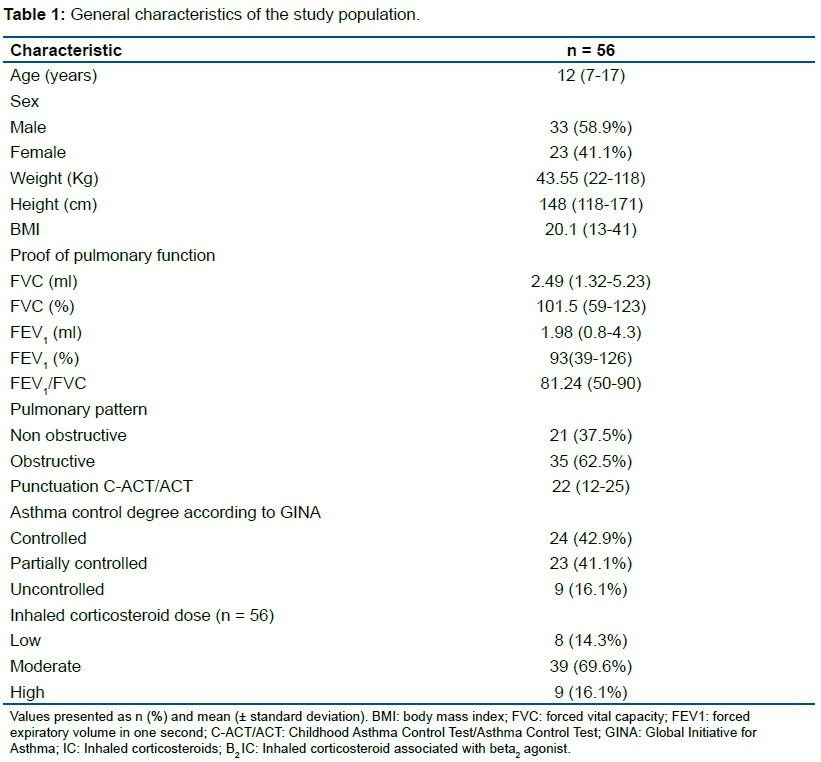
Fifty-six asthmatic children and adolescents on regular IC use, whether or not associated with LABA, were selected. The median age was 12 (7-17) years, with a predominance of males (58.9%). More than half (62.5%) of the children and adolescents evaluated presented obstructive pattern on spirometry. Table 1 shows the general characteristics of the studied population.
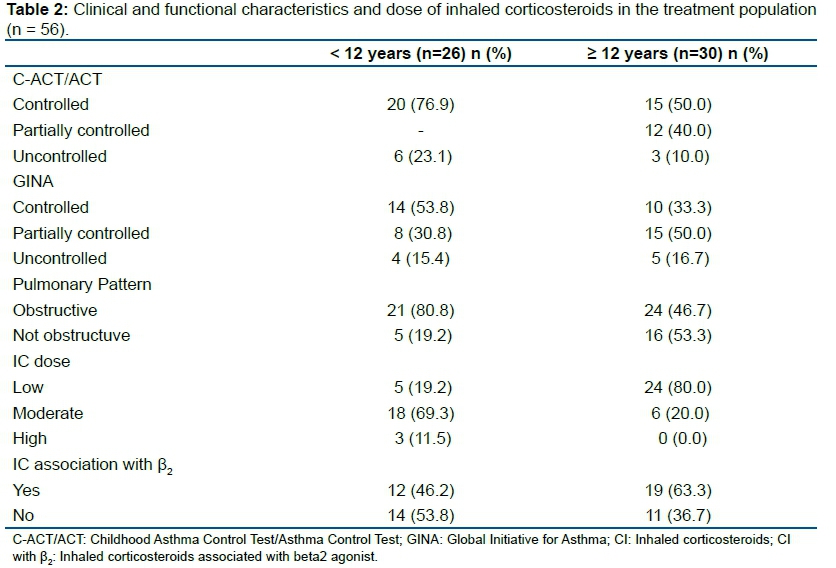
According to Table 2, controlled asthma was observed in 76.9% of patients <12 years and 50% in those older than 12 years according to C-ACT/ACT, and in 53.8% and 33.3%, respectively, according to GINA.
DISCUSSION
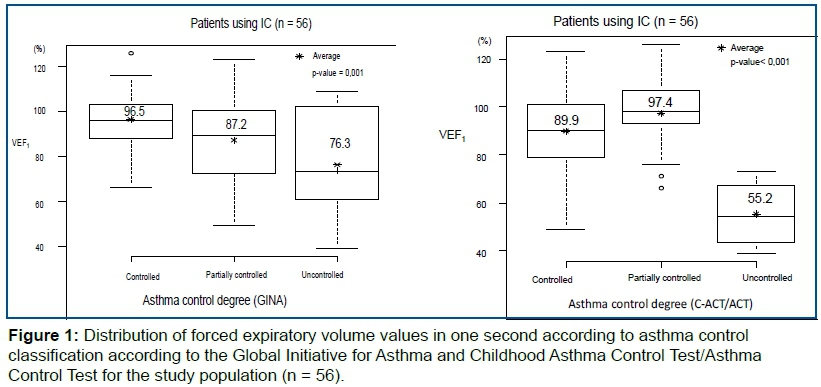
In this study, it was observed that in the children and adolescents studied there is an association between FEV1 values and clinical asthma control ratings, according to GINA, since FEV1 percentage values gradually decreased as the degree of Asthma control worsened. This association was also observed between FEV1 and C-ACT/ACT, in relation to controlled and uncontrolled asthma in the studied population.
When C-ACT/ACT results were compared to GINA results, it was observed that C-ACT/ACT categorized higher proportion of asthmatics as controlled, regardless of age group.
The frequency of children with OVD in this study was almost double among those under 12 years of age. The dose of IC used in patients under 12 years was moderate, while in patients over 12 years, the most frequent dose was low. Another finding was that most children under 12 years old did not use the association of IC with long-acting β2 agonist when compared to those older than 12 years old.
The Figure 1 reveals that there was a statistically significant association between FEV1 values and clinical asthma control ratings according to GINA (p-value = 0.001). This association was also observed between FEV1 and C-ACT/ACT (p-value <0.01), in relation to controlled and uncontrolled asthma in the studied population.
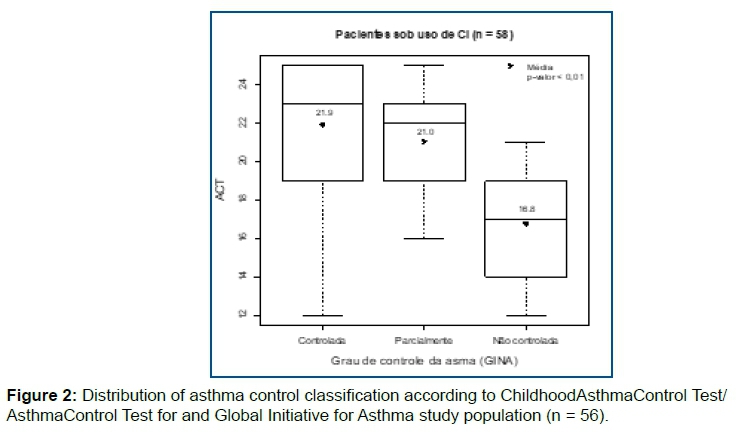
The Figure 2 shows the mean C-ACT/ACT score values according to the degree of asthma control according to GINA (p-value <0.01).
Another important finding observed in this study was that the proportions of asthmatics classified as controlled were equivalent for both the C-ACT/ACT and the GINA questionnaire.
The results found in our study are similar to those of Fuhlbrigge et al.12, who concluded that FEV1 is associated with important clinical outcomes in children with asthma, such as symptoms, exacerbations and health care utilization. However, Vidal et al.13 in a study of 88 patients aged 12 to 17 years concluded that FEV1 would not be an adequate instrument to monitor asthma control in children, since most children with asthma have normal FEV1 values.
Corroborating our study, Yasunori et al.14 analyzed 258 asthmatic children aged 5-11 years and found a positive correlation between C-ACT score and FEV1. The same conclusion was seen in the study by Oliveira et al.8, which analyzed 105 asthmatic children aged 4 to 11 years with the objective of validating the Brazilian version of C-ACT. However, the opposite was observed by Piacentini et al.15 when analyzing 200 asthmatic children, with an average age of 8.9 years (± 2.8), with 143 of them being treated according to GINA guidelines and 47 without treatment. In those under treatment, there was no correlation between C-ACT score and FEV1 values. Poor perception of symptoms by patients and their families may explain this finding, as the Asthma Control Test is a self-applicable tool that considers only clinical parameters and not spirometric parameters such as FEV116,17.
There was agreement between the asthma control classifications according to GINA and C-ACT/ACT, regardless of age. Similar results were found by Somashekar et al.12, who evaluated 97 children aged 4-12 years. However, in the study by Koolen et al.18, evaluating 145 asthmatic children aged 4 to 18 years in order to compare GINA classification with C-ACT and ACT for the detection of uncontrolled asthma, it was observed that asthma was completely controlled in 14% of children and uncontrolled in 51% of them, according to the GINA proposal. If ACT and C-ACT were used, the proportions of "uncontrolled" patients would be different (33% and 17%, respectively). The authors suggested that the cutoff points commonly used for C-ACT and ACT underestimate the proportion of children with uncontrolled asthma as defined by the GINA.
In our study, all patients were on regular IC regardless of age. More than half of this population had OVD and controlled asthma according to the self-administered C-ACT/ACT questionnaire regarding their symptoms. However, our limitation in the study was the impossibility of measuring correct use and adherence to medications. Factors such as incorrect inhalation technique and poor adherence to treatment may be implicated for non-control of asthma in this group of symptomatic and OVD patients, despite training with inhalation devices and continuing clarification on the importance of regular medication use. practiced during consultations19. Another issue would be whether patients with severe asthma phenotypes, unresponsive or not responsive to regular IC use, could be part of the study sample20. Regarding the use of high doses of isolated IC to the detriment of the CI-LABA association, we face a major public health problem that is the difficulty of the government-assisted population to acquire the gold standard medication for their proposed treatment and the self-cost of these medications19.
CONCLUSION
The measurement of FEV1 is a useful component among the instruments for assessing clinical asthma control. Apparently, their result is related to the usual tests to evaluate asthma control: GINA and ACT/C-ACT.
REFERENCES
1.Globla Initiative for Asthma. Global Strategy for Asthma Management and Prevention: 2017 update. [cited 2017 May 19]. Available from: https://ginasthma.org/wp-content/uploads/2019/04/wmsGINA-2017-main-report-final_V2.pdf [ Links ]
2.Andrade CR, Chatkin JM, Camargos PAM. Avaliação do grau de controle clínico, espirométrico e da intensidade do processo inflamatório na asma. J. Pediatr. 2010;86(2):93-100. DOI: http://dx.doi.org/10.1590/S0021-75572010000200003 [ Links ]
3.Sociedade Brasileira de Pneumologia e Tisiologia. Diretrizes da Sociedade Brasileira de Pneumologia e Tisiologia para o Manejo da Asma - 2012. J Bras Pneumol. 2012;38(suppl1):S1-46. [ Links ]
4.Demoly P, Paggiaro P, Plaza V, Bolge SC, Kannan H, Sohier B, et al. Prevalence of asthma control among adults in France, Germany, Italy, Spain and the UK. Eur Respir Rev. 2009;18(112):105-12. DOI: http://dx.doi.org/10.1183/09059180.00001209 [ Links ]
5.Paiva M, Martins P, Carvalho S, Chambel M, Matos A, Almeida I, et al. Avaliação do controlo da asma: Utilização de diferentes métodos. Rev Port Imunoalergologia. 2010;18(3):227-41. [ Links ]
6.National Asthma Education and Prevention. Practical guide for diagnosis and management of asthma. 1997; p.5. [ Links ]
7.Zangirolami-Raimundo J, Echeimberg JO, Leone C.Research methodology topics: Cross-sectional studies. J Hum Growth Dev. 2018;28(3):356-60. DOI: http://dx.doi.org/10.7322/jhgd.152198 [ Links ]
8.Oliveira SG, Sarria EE, Roncada C, Stein RT, Pitrez PM, Mattiello R. Validation of the Brazilian version of the childhood asthma control test (c-ACT). Pediatr Pulmonol. 2016;51(4):358-63. DOI: http://dx.doi.org/10.1002/ppul.23318 [ Links ]
9.Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A, et al. Standardization of spirometry. Eur Respir J. 2005;26(2):319-38. DOI: http://dx.doi.org/10.1183/09031936.05.00034805 [ Links ]
10.Pellegrino R, Viegi G, Brusasco V, Crapo RO, Burgos F, Casaburi R, et al. Interpretative strategies for lung function tests. Eur Respir J. 2005;26(5):948-6. DOI:http://dx.doi.org/10.1183/09031936.05.00035205 [ Links ]
11.Somashekar AR, Ramakrishnan KG. Evaluation of Asthma Control in Children Using Childhood-Asthma Control Test (C-ACT) and Asthma Therapy Assessment Questionnaire (ATAQ). Indian Pediatr. 2017;54(9):746-8. DOI: http://dx.doi.org/10.1007/s13312-017-1167-2 [ Links ]
12.Fuhlbrigge AL, Weiss ST, Kuntz KM, Paltiel AD; CAMP Research Group. Forced expiratory volume in 1 second percentage improves the classification of severity among children with asthma. Pediatrics. 2006;118(2):346-56. DOI: http://dx.doi.org/10.1542/peds.2005-2962 [ Links ]
13.Vidal AG, Escobar AMC, Medina MER. Correlación y concordancia entre instrumentos de controldel asma enniños. Rev Chil Enferm Respir. 2012;28(1):29-34. DOI: http://dx.doi.org/10.4067/S0717-73482012000100005 [ Links ]
14.Ito Y, Adachi Y, Itazawa T, Okabe Y, Adachi YS, Higuchi O, et al. Association between the results of the childhood asthma control test and objective parameters in asthmatic children. J Asthma. 2011;48(10):1076-80. DOI: http://dx.doi.org/10.3109/02770903.2011.629356 [ Links ]
15.Piacentini GL, Peroni DG, Bodini A, Bonafiglia E, Rigotti E, Baraldi E, et al. Childhood Asthma Control Test and airway inflammation evaluation in asthmatic children. Allergy. 2009;64(12):1753-7. DOI: http://dx.doi.org/10.1111/j.1398-9995.2009.02068.x [ Links ]
16.Parente AAAI, March MFP, Evangelista LA, Cunha AL. Percepção da dispneia na crise asmática pediátrica pelos pacientes e responsáveis. J. Pediatr. 2011;87(6):541-6. http://dx.doi.org/10.2223/JPED.2144 [ Links ]
17.Aragão LJL, Coriolano-Marinus MWL, Sette GCS, Raposo MCF, Britto MCA, Lima LS. Qualidade de vida na asma brônquica - a concordância das percepções das crianças, adolescentes e seus pais. Rev Paul Pediatr. 2012;30(1):13-20. http://dx.doi.org/10.1590/S0103-05822012000100003 [ Links ]
18.Koolen BB, Pijnenburg MWH, Brackel HJL, Landstra AM, van den Berg NJ, Merkus PJFM, et al. Comparing Global Initiative for Asthma (GINA) criteria with the Childhood Asthma Control Test (C-ACT) and Asthma Control Test (ACT). Eur Respir J. 2011;38(3):561-6. DOI: http://dx.doi.org/10.1183/09031936.00173710 [ Links ]
19.Dalcin PTR, Grutcki DM, Laporte PP, Lima PB, Viana VP, Konzen GL, et al. Impacto de uma intervenção educacional de curta duração sobre a adesão ao tratamento e controle da asma. J Bras Pneumol. 2011;37(1):19-27. http://dx.doi.org/10.1590/S1806-37132011000100005 [ Links ]
20.Campos HS. Asma grave. J Bras Med. 2015;103(2):13-21. [ Links ]
 Correspondence:
Correspondence:
karladtf@hotmail.com
Manuscript received: September 2018
Manuscript accepted: August 2019
Version of record online: October 2019


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}