










Serviços Personalizados
artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282versão On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.29 no.3 São Paulo set./dez. 2019
http://dx.doi.org/10.7322/jhgd.v29.9533
ORIGINAL ARTICLE
Parent's perception of allergic or food-intolerant children in relation to disease
Suzely Adas Saliba MoimazI; Marcelo Augusto AmaralII; Aline Maria Malachini MiottoIII; Cléa Adas Saliba GarbinI; Tânia Adas SalibaIV
IDocente Titular do Programa de Pós-Graduação em Odontologia Preventiva e Social, Universidade Estadual Paulista (UNESP), Araçatuba (SP), Brasil
IIDoutor em Odontologia Preventiva e Social , Universidade Estadual Paulista (UNESP), Faculdade de Odontologia (FOA), Araçatuba (SP), Brasil. Docente do Centro Universitário de Maringá (UniCesumar), Maringá (PR), Brasil
IIIDocente Adjunta do Programa de Pós-Graduação em Ciência da Computação, Universidade Estadual de Maringá (UEM), Maringá (PR), Brasil
IVDocente Adjunta do Programa de Pós-Graduação em Odontologia Preventiva e Social, Universidade Estadual Paulista (UNESP), Araçatuba (SP), Brasil
ABSTRACT
INTRODUCTION: Cow´s milk protein allergy (CMPA) and lactose intolerance (LI) negatively affect the quality of life of patients and their families.
OBJECTIVE: To analyse the perception parents of children with CMPA or LI regarding aspects of health, emphasizing their oral health and the factors involved in the treatment of allergy/food intolerance
METHODS: Qualitative research employing focus groups, with a sample of 12 parents of children with CMPA or LI (two groups), including the participation of a researcher/moderator, an observer, and six participants in each group and a plan with guiding questions. Discourses were recorded and transcribed, and textual contents were processed in software IRAMUTEQ and analysed by the descendant hierarchical classification (DHC) technique, content analysis, and word cloud.
RESULTS: Six categories were derived from DHC-multivariate analysis: (1) children formula, (2) oral health, (3) nutritional aspects, (4) treatment, (5) disease´s stigma, and (6) health services. The thematic axes were derived from nutritional, assistance, and care categories. Reports of different oral diseases were given by parents regarding food allergy or intolerance in their children, such as frequent caries, teeth spots, pain, and sensitive teeth.
CONCLUSION: Parents´ perception of CMPA/LI in their children is affected by nutritional factors and the stigma caused by the disease, with special reference to the importance given to children´s oral health and reports about difficulties in the access to health services with multi-professional teams.
Keywords: qualitative analysis, milk hypersensitivity, lactose intolerance.
Authors summary
Why was this study done?
The present study aimed to analyse the perception of parents of children with cow's milk protein allergy or lactose intolerance regarding health aspects, emphasising their children's oral health and the factors involved in the treatment of allergy and food intolerance.
What did the researchers do and find?
A qualitative research was conducted using the focus group technique with a sample of 12 parents of children with cow's milk protein allergy or lactose intolerance. Through the multivariate analysis, six word categories were identified: (1) infant formulas, (2) oral health, (3) nutritional aspects, (4) treatment, (5) disease stigma, and (6) health services. From these, three thematic axes were identified: nutrition, attention, and assistance. The content analysis obtained reports of different oral diseases in their children, such as frequent caries, dental stains, pain, and sensitive teeth.
What do these findings mean?
This is the first national qualitative study based on the population of parents of children with cow's milk allergy or lactose intolerance and their relationship to oral health. The results allowed us to understand how parents face the disease, their experiences, and expectations regarding health services.
INTRODUCTION
Food allergy has increased significantly in developed countries, and it may have significant effects on people´s quality of life1. Currently, it affects 6%-8% of children and 2% of adults worldwide2,3. The seriousness of allergic reactions may range from slight to potentially fatal1,3. Cow´s milk protein allergy (CMPA) is the most common allergy in children4,5 and it may affect up to 4.9% of children less than three years old6.
As a rule, lactose intolerance (LI) prevalence varies worldwide. In northeastern Europe, close to the North Sea, it occurs in 5% of adults, with a lower prevalence in Denmark (4%), the UK (5%), and Sweden (1%-7%). There is an increasing rate in central-southern Europe, and close to 100% in Asia and the Middle East7. In Brazil, 43% of white and mixed-race adults have LI, with great frequency among Negroes and Japanese descendants8.
Allergies are often confused with food intolerances or non-immune adverse reactions such as LI, food poisoning, or caffeine intolerance9. The usual treatment of CMPA is the total and/or definitive exclusion of cow's milk from patients' diets. However, a restricted diet in a child who does not require it or who has LI can alter growth and quality of life and produce unnecessary costs10.
Several studies have shown that food allergies and hypersensitivity have psychosocial impacts and negatively affect the lifestyle of children, adolescents, and their families. This is because the disease is treated with food restrictions, and constant vigilance is required11,12.
Despite the importance of this issue, few qualitative studies have been conducted on CMPA. Several studies investigate allergy to peanuts and/or oleaginous fruits1,13,14. In Brazil, cow´s milk is one of the main allergy-causing foods. Milk exclusion is highly difficult due to its wide distribution in food products and its nutritional importance for children. Further, studies rarely deal with emotional problems related to food restrictions15.
In this context, the present study aimed to analyse the perception of parents of children with CMPA or LI regarding aspects of health, emphasising their oral health and the factors involved in the treatment of allergy/food intolerance.
METHODS
Study design, population, and data collection
This study consists of a qualitative research employing the focus group technique. Samples comprised 12 parents of children with CMPA or LI (10 females and 2 males) within the 22-47-year-old age bracket. Four had a history of food allergy. Participants were divided into two groups at different periods. Inclusion criteria were availability to participate in focus groups and good communication capacity, evaluated in a preliminary contact.
Data collection occurred in 2018 in a private school in a town in southern Brazil at night. The interview technique, with a duration of 40-60 minutes, was employed in the focus groups, with the participation of a researcher/moderator, an observer, and six fathers/mothers per group. Parents were selected after an exploratory analysis of the school, verification of children with CMPA or LI, and an invitation, sent through the school to 18 parents, to participate in the focus group at a pre-determined date by the research´s moderator/second author.
Several conditions were standardised for the focus groups. These included preparations of the interview room, with lights, ventilation, accommodation, and sufficient space; signs on the outside of the door: 'Meeting going on. Do not enter'; verification of a recorder (working conditions and volume); and welcoming participants. The following took place at the start of the meeting for each focus group: the researcher/moderator and observer welcomed the participants; the research´s aim and technique were explained; permission was asked to employ the recorder; the importance of speaking order for the group´s activities so that speeches would not be crossed was explained; the relevance of the participation of all participants was discussed; information was given on the duration of the meeting; participation was confirmed; and number tags for the preservation of participants' identity were distributed.
The focus group interview technique consists of the interaction between participants and researchers to understand the different social representations on a practice, fact, product, or service, through a discussion on specific topics16. The main researcher of this study conducted the interview by a topic plan to guide the discussion and capture the interviewees' point of view about the theme: Parents' perceptions of allergic or food-intolerant children in relation to disease. During the interview, free discussion occurred, although the conversation design was followed to keep the interview fine-tuned to the research aims. The interview was recorded on a digital recorder and ended at a saturation point when, after the collection of information with a certain number of participants, other interviews tended towards repetition of contents17.
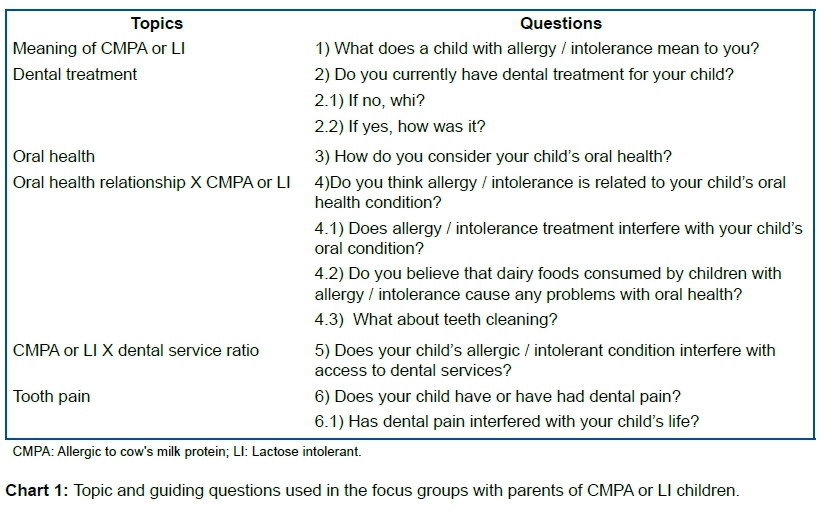
Six guiding questions and other complementary topics were applied to the focus groups (Chart 1). Recordings were fully transcribed one day after the sessions with the focus groups.
Processing and data analysis
The textual corpus of the focus groups was processed by IRAMUTEQ 0.7 for qualitative analysis and analysed by descendant hierarchical classification (DHC) and word cloud techniques. IRAMUTEQ (Interface de R pour les Analyses Multidimensionnelles de Textes et de Questionnaires), a free software based on programme R language, was employed, since it allowed processing and statistical analysis of several textual corpuses18,19.
The DHC technique, proposed by Reinert20 was used to obtain word classes from textual corpuses that, in a concomitant way, have similar meanings/vocabularies, but, at the same time, are different from the text segments of the other classes21. DHC organises the qualitative analysis of texts in a dendrogram, graphically representing classes and their possible relationships. The researcher tags the classes according to semantics, taking into account frequencies and Chi-square statistical tests (X2) provided by the software.
IRAMUTEQ underscores lexical worlds of full words with the same meaning nucleus. The dendrogram synthesises axes and underscores word classes. The latter require hermeneutical analysis to understand the text and the content production of meaning22.
An analytic model is built after the processing of textual content. It is composed of categories that correspond to word classes generated by IRAMUTEQ and DHC. Categories may be established prior to field work, during the exploratory phase of the research, or after data collection. In the current research, post-data-collection analytic categories were employed, since they were more specific, concrete, and according to lexical criteria13.
Analysis of contents was also performed to interpret the textual corpus. This method is widely employed, since it provides an in-depth evaluation of the interviewee´s discourse, so that, after careful study, one may understand critically the meaning of the explicit, hidden, or obscure messages23. In the quantitative approach, the occurrences of the words present in the textual corpus were evaluated, and in the qualitative analysis, the terms of the categories were selected through the set of characteristics represented by the content analysis24.
Word cloud is a simpler method and features graphic representation due to word frequency. It easily allows visual identification by a figure generated by IRAMUTEQ25.
Ethical consideration
This study complies with the ethical requirements established by National Health Council Resolution 466/12, the Declaration of Helsinki, and the Nuremberg Code. Ethical approval was obtained by the Ethics in Research Committee of the University Centre of Maringá (UniCesumar), under protocol number 2.028.098/2017. All parents received information on the study´s aims and signed the Free Consent Term on their research participation.
RESULTS AND DISCUSSION
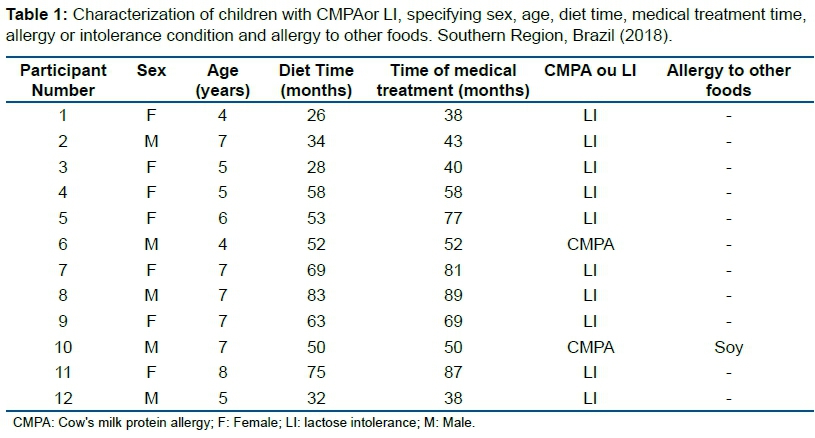
Regarding the profile of the participants' children, seven were females and five males. The mean age of the children with CMPA/LI was 5.9±1.3 years, at the time of research, varying between four and eight years. The period of diet exclusion or cow milk replacement averaged 51.9±18.9 months, and medical follow-up reached 60.2±19.5 months. Ten out of the 12 parents reported LI, and two reported CMPA. One child was even allergic to soybean-based food (Table 1).
Class/category characterisation
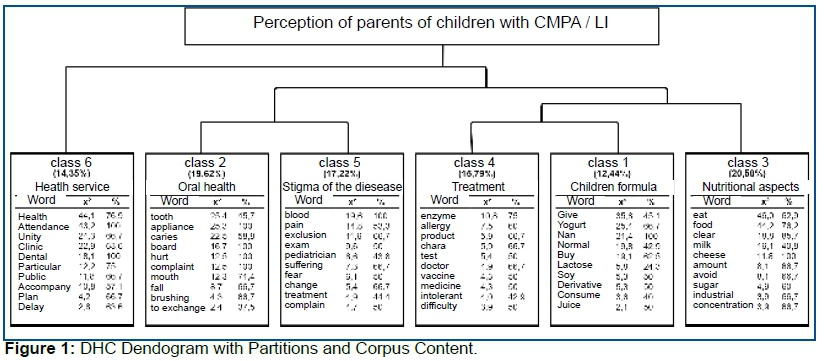
The analysis of the corpus 'Parents' perceptions of allergic or food intolerant children in relation to disease' derived from the focus groups' transcription shows 256 segments, of which 209 (81.64%) words were classified by DHC. It indicated the degree of similarity and distortion in the vocabulary of the six resultant classes: infant formula (class 1), oral health (class 2), nutritional aspects (class 3), treatment (class 4), disease stigma (class 5), and health services (class 6). The nutritional aspects class was predominant, characterised by the terms eat (X2=46.0), food (X2=44.2), and expensive (X2=18.8) (Figure 1).
DHC´s multivariate analysis identified six word classes as a whole. The Chi-square test indicates the degree of statistical significance of the words with the greatest frequency in each class. Statistical significance shows that certain terms tend to appear in a determined class, while a lack of meaning shows that terms were present in several groups. The greater the presence of a determined term, the more specific is the group. The greatest class was 3, with 20.58% of the textual corpus, followed by class 2 with 19.62%, class 5 with 17.22%, class 4 with 15.79%, and class 6 with 14.35%. Class 1 represented 12.44% of the total discourse. Classes 1, 3, and 4 and classes 2 and 5 derive from the same axis and thus have the greatest connection. The same is not true for the other axis, which includes class 6 alone (Figure 1).
From the extraction and partition of the six classes generated by the IRAMUTEQ software, the authors of this research identified three thematic axes: nutrition, attention, and care. Analysis of classes 1, 3, and 4 (48.81%) represents the axis with the highest representativeness rate in the textual corpus of focus groups and demonstrates the different types of infant formula used by food allergic/intolerant children, the meaning and difficulties generated by the exclusion of these foods in children´s diet, and the type of treatment that cow milk-replacement therapies represent for these children (nutrition axis).
Classes 2 and 5 (36.84%) show the relevance that parents give to prevention and to general oral health of allergic/intolerant children. These classes reveal what oral conditions represent for parents in the care of their children and the stigma and representation of this specific health condition to parents (attention axis). Class 6 (14.35%) refers to the behaviour and expectations of parents with regard to public or private health services available to CMPA/LI children. The classes demonstrate the dichotomy in marketological practice in the care of these patients (care axis). An interpretative analysis of speeches is provided in each identified category grouped from the application of the DHC technique in the textual corpus.
Interpretative analysis: perception of parents of children with CMPA/LI
Children formula
Infant formula was the least expressive category in the focus groups, with the most representative terms give, yogurt, Nan, normal, purchase, lactose, soy, derived, consume, and juice. The category detects possible food sources used by children with CMPA/LI to replace mother´s milk or cow milk. It also indicates the association between a consumption experience of food with lactose or cow milk protein and the many symptoms that CMPA/LI children had. Parents´ discourse may help understand the class contents and the context of its meanings:
The belly becomes swollen, with great pain in the stomach, a bad feeling throughout; this is very bad for the child and for us parents. We suffer without knowing how to give any help. Therefore, we buy food without lactose or with low lactose, so that they would not have such symptoms (LI 3).
As soon as my son was born, he had extensive diarrhea after breastfeeding. I started to perceive that my milk may be causing such disorder. Things worsened, and I visited the doctor, who suspected milk allergy. I started to use powdered soybean milk to feed my newly born child (CMPA 6).
In the case of my daughter, normal milk caused huge problems, such as headache, nauseas, and belly aches. All this was solved when cow milk was replaced by milk without lactose (LI 9).
Allergy to cow milk and soybean milk brought many difficulties during the first months after my son´s birth. He used to breastfeed and vomit, and he had fever and difficulties in breathing. Everything was solved when breastfeeding stopped and we stopped using cow or soybean milk. In fact, he is a case in severe food allergy (CMPA 10).
During the first years of life, mother´s milk and replacements, such as infant milk formula, are the infants´ main food sources. However, in the case of children with CMPA/LI, the process is different. In fact, parents experience several difficulties, doubts, sufferings, and changes to adapt themselves to the child´s special health issue.
In the case of the several doubts in the follow-up of children with CMPA/LI, Yonamine et al.15 insist that they are related to the disease´s diagnosis, treatment, and history. They reported a lack of understanding of the cause of the allergy, questionings of the existence of other treatment modes, and the replacement of cow milk by infant formula as the only therapy for these children.
Guidelines on the treatment of food allergy/intolerance should be clear and practical so that they help in the choice of the best infant formula and facilitate adhesion to the treatment. A basic guideline is reading food labels. This may be a difficult task due to the great number of synonymous terms, letter size, and Brazilian legislation26.
Oral health
The most representative terms in this category are tooth, brace, caries, plate, hurt, complaint, mouth, fall, brushing, and touch. One may underscore the importance of oral health reported by parents in the caring of children with food allergy/intolerance and discuss the problems caused by such health conditions. These may be analysed by the following discourses:
Due to intolerance to lactose, my son has weak and fragile teeth, with clefts; they are more sensitive than those of children who drink common milk. They do not need to use industrialised replacements (LI 2).
Since birth, my daughter had several caries and spots on her teeth. This made me uneasy, since brushing teeth every day failed to bring any results (LI 7).
I have two sons. The child with intolerance to lactose changed teeth differently from the other. Teeth delayed falling when compared to those of his brother´s. The two had the same care; however, the son who took normal milk lost the primary teeth some time after the other; I also had to take him more frequently to the dentist to pull out his teeth (LI 8).
Frequently my daughter´s teeth have caries, and she always complains of pain in the mouth. I cannot understand the reason for so many caries and the need of obturations. She is very young, and every six months I have to take her to the dentist (LI 9).
Parents of LI children offered perceptions of different oral problems, such as teeth fragility and sensitivity, caries, spots on the teeth, delayed change of teeth, and toothaches. These issues may have serious consequences during childhood and adolescence. They need periodic follow-up by the dentist every three to six months, depending on the child´s disease risks.
As a rule, children with CMPA/LI have an exclusion diet or cow milk reduction. They normally consume soybean-based food or other milk replacements, sometimes sweetened with sucrose27. It is also important that parents should be aware that this type of food may wear children´s teeth structure and cause demineralisation of the primary tooth enamel28.
Soybean-based food has been frequently employed by food allergic/intolerant people till the emergence of milk foods with lactose reduction. In fact, they have recently become highly popular among parents of children with these health conditions.
There is little information on the oral health of children with food allergy/intolerance. Few studies and research work deal with the relationship between tooth conditions and intolerance to lactose29,30.
Cagetti et al.29 studied the prevalence of caries in children aged six to eight years old and associated the ingestion of lactose-free milk to children with a high caries index. Thus, there are indications that the consumption of baby milk may cause tooth erosion31 demineralisation of deciduous tooth enamel28 and caries29,32. Further studies are recommended to evaluate different risks in children´s mouth diseases and the influence of these factors on quality of life.
Nutritional aspects
The nutritional aspects category was highly prevalent in the focus groups, with the terms eat, food, expensive, milk, cheese, quantity, avoid, sugar, industrialised, and concentration. In this class, the parents of intolerant children with more time for treatment were those who contributed more effectively. One may also detect the importance that nutrition has for the families and their different approaches and perceptions. Parents´ self-evaluation may be verified by the feelings related to the feeding of their children, as the texts below evidence:
I think that intolerance totally changed my daughter´s life. She became different from other children. She may not eat what she likes and may eat foods recommended by nutritionists. They may not be found everywhere (LI 5).
Replaced products without lactose are more expensive than normal ones. Frequently the price is double, and I cannot afford to buy them; besides, they are not found everywhere (LI 7).
Besides being 30% more expensive, foods with low lactose are difficult to find. They may be found in big supermarkets and in mid-sized towns (LI 8).
The food of children with intolerance is similar to medicine for a sick person: either you restrict this type of food and replace it with another, or the child will not feel well. We have to avoid the worst or reduce its amount (LI 11).
The reports above underscore the importance of food for these children and corroborate the conclusions by Yonamine et al.15 who insisted on the need to learn to deal with such health conditions, for example, permitted or restricted food, food replacement, meal planning, and adhesion to treatment by children and their parents.
Follow-up by a nutritionist is relevant for food allergic/intolerant children. This aspect has been highlighted by Yonamine et al.15 as a difference in their treatment. The nutritionist provides food alternatives and facilitates diet constitution. In fact, family members revealed that obedience to the nutritionist is fundamental and that it is worthless to make a visit to the nutritionist without complying with the treatment.
Another frequent factor in the focus groups is the high cost of lactose-free food. In the case of many families, the continuation of treatment is highly impaired, since it has to be dealt with in a multidisciplinary way. Treatment involves expensive lactose-free foods or their derivates. Further, nutritionists in the multiprofessional team are greatly relevant, especially when dealing with patients with food allergy/intolerance, relatives (parents, uncles, and aunts), and caretakers (teachers and neighbours). Their task is not merely to provide alternative recipes but to instruct everyone responsible for the patient´s food15 including the possibility of choosing financially more available food replacements.
Treatment
DHC reveals that the terms that trigger the category were enzyme, allergy, product, behaviour, test, doctor, vaccine, medicine, intolerant, and difficulty. The category symbolises the vision that parents with children suffering from allergy/intolerance have of their care. It is more associated to the biological (medical) than the behavioural aspect (psychology).
Several extracts of their discourses reveal participants´ perception of 'treatment' and how it may affect care for their children:
Since my son has a high intolerance to lactose, I may abide with the problem using the enzyme lactase every day prior to his going to school; since he is still very small and shares lunch with other children, he feels less of the disease´s effects and symptoms (LI 2).
Cow´s milk protein in the food taken by my son is capable of causing his allergic state; when this occurs, I have to run to the doctor´s; this fact has brought great changes in our lives (CMPA 10).
Lactose from products consumed by my daughter causes different signs and symptoms in her body, ranging from a general malaise to changes in her behaviour, such as irritability and uncontrolled weeping. I cannot treat this sort of thing (LI 9).
Treatment is a highly complex thing. Several tests were performed and not even the physicians knew what my daughter had! I tried to give her nothing that contained milk; she took milk with low lactose, or enzyme at meals. However, it seems that no improvements occurred (LI 11).
Treatment against food allergy and intolerance is actually one of the most complex things to follow up in children in such conditions. Total and/or definitive exclusion of lactose in CMPA/LI diets depends on correct diagnosis and normally involves the use of milk replacements based on baby milk27.
Yonamine et al.15 reported that relatives of allergic children have several doubts about the treatment. They do not know whether the treatment may be related only to medicine or vaccine, or whether an exclusion diet may be another approach in the treatment of the disease. The health professional should maintain a strict bond with the family, establish mutual trust, and exchange two-way information routes, facilitating successful care of the patient with chronic disease33.
It is highly recommended that caretakers are informed on the natural history of CMPA and the possible development of milk tolerance. They should realise that the disease may not endure throughout the whole span of life and that treatment may be for a limited period. They should also be aware that religion and spirituality may provide comfort, hope, and resilience for the acceptance of the conditions caused by the disease within a period in the child's life33.
Stigma of the disease
The most representative terms in the category are blood, pain, exclusion, exam, pediatrician, suffering, fear, change, treatment, and complaint. One may surmise the difficulties that patients and parents have to cope with, coupled with the possibility of a discussion on the disease with regard to the life of these people, analysed in their own words:
The life of a person with milk intolerance brings much suffering to the child and those who care for her. My daughter complains a lot; she has pains when she consumes food with milk. She has to undergo allergy tests requested by her doctor (LI 1).
When we discovered the allergy of my son, great changes occurred in our lives. I had to stop working at the office to give attention to his needs. I feared he would die (CMPA 6).
Surviving with food allergy is difficult; the disease brings a lot of concern and fear of what would happen to one´s son. Everyday care on diet is a must. The greatest difficulty is that I am not always with him at all moments. Doubts abound (CMPA 10).
Since we were informed that my son had intolerance to lactose, my life is consumed by visiting the pediatrician and following his recommendations on food exclusion. It would have been easier if my son quit all-day school where he has various meals. Every day is a negative surprise (LI 12).
The parents of these allergic/intolerant children share perceptions of similar treatments with children suffering from other chronic diseases, such as sickle cell disease34. It is recommended that the experience of food allergy/intolerance should be seen within a wider family context, with special reference to coping with parents´ anxiety. Health services should better attend the psychological and social needs of the people affected by such health conditions35.
Several studies have shown that food allergies/intolerance negatively affect the lifestyle of patients and parents, especially females with a great number of crossed allergies, a great number of previous allergic reactions, or other associated atopic diseases. Health professionals have an important role in the improvement of the lifestyle of this population through information on the disease and nutritionally adequate replacements11,12.
Further, there is evidence that children with food allergies featuring anaphylaxis suffer more than those with other chronic diseases, such as rheumatism or insulin-dependent diabetes mellitus. This fact may be related to the constant fear of a possible anaphylactic reaction and death risk, generating high anxiety rates and stress for the patient and the family36.
Feeding is an important activity in human development and involves nutritional, medical, psychological, and commercial contexts. Feeding may present other meanings that depend on local culture and rituals. Besides, there is a dialogical relationship between the school and the community in coping with aspects involving healthy feeding37. They may pose great difficulty to allergic/intolerant people in the control of disease.
Health services
Health services are the last category of the focus groups, featuring representative terms such as health, attendance, unity, dentistry, clinical, private, public, follow-up, plan, and delay. Several situations are present within the parents' daily life for different analyses of the current assistance model, as the discourse of participants reveals:
My son has a health plan. In fact, his health is a priority. He has already had several allergic crises that required immediate hospitalisation! However, my husband, my other son, and I do not have a private health plan (CMPA 10).
I cannot afford paying a private health plan! When a crisis emerges, I take my daughter to the health clinic and wait for the pediatrician to attend her. The real problem is delay. Since she complains a lot due to pain, I cannot do all the blood tests punctually (LI 1).
The private health system only attends intolerance cases with a doctor and a nutritionist; my daughter also requires dentistry care, and I have to pay for this too (LI 7).
The follow-up that my daughter needs demands a total health service, with physicians, nutritionists, psychologists, and even dentists. Practically, this is not possible in any public or private health plan (LI 11).
Parents´ discourses and perceptions reveal the need for an integral health plan that guarantees access to priority groups, such as those suffering from chronic diseases and CMPA/LI. Multidisciplinary care should acknowledge caretakers as protagonists in the treatment of food allergy/intolerance and elaborate activities for the encouragement of the different health professionals involved in the care of these diseases38.
To construct a new health model that meets all the needs of CMPA or LI patients, it is important to consider the different ways that nutrition affects children and adolescents in different situations. Undernutrition persists in many countries, and overnutrition is a continuing challenge in others to ensure optimal nutrition for all children39. The multiprofessional follow-up of CMPA/IL children provides proper help and guidance to parents so that patients may improve their lifestyles within undesirable conditions and perceive that it is possible to have a better lifestyle15 with the disease.
Besides the characteristics listed above, health services for chronic systemic disease patients require a multidisciplinary approach, at both the prevention and therapy levels, and they should include professionals from different disciplines, from basic sciences to clinics, with individualised recommendations according to the comorbidity of each patient40.
Word cloud
Analysis of a word cloud within the corpus under analysis revealed that the most frequent nouns were milk and tooth. The most frequent verb was eat, followed by take. The most frequent adjectives were dentistry and intolerant (Figure 2). In fact, the most common words of the participants refer to the main topics dealt with in the thematic classes given throughout the current analysis.

This is the first national qualitative study based on the population of parents of CMPA or LI children and their relationship to oral health. The results allowed us to understand how parents face the disease, their experiences, and expectations regarding health services.
CONCLUSION
Parents´ perception of CMPA/LI children is greatly affected by nutritional factors and the stigma that the disease brings to the patients. The importance of monitoring the oral health of children was highlighted by parents; however, it is important to highlight difficulties in accessing health services with multiprofessional teams to deal with the health condition.
Acknowledgement
The authors thank CAPES for the financial support.
Article supported by University Centre of Maringa - Institute of Science, Technology and Innovation - ICETI
REFERENCES
1.Antolín-Amérigo D, Manso L, Caminati M, de la Hoz Caballer B, Cerecedo I, Muriel A, et al. Quality of life in patients with food allergy. Clin Mol Allergy. 2016;14(4). DOI: http://dx.doi.org/10.1186/s12948-016-0041-4 [ Links ]
2.National Institute for Health and Clinical Excellence. Food allergy in children and young people: diagnosis and assessment of food allergy in children and young people in primary care and community settings. London: NICE; 2011. [ Links ]
3.Zhu J, Pouillot R, Kwegvir-Afful EK, Luccioli S, Gendel SM. A retrospective analysis of allergic reaction severities and minimal eliciting doses for peanut, milk, egg, and soy oral food challenges. Food Chem Toxicol. 2015;80:92-100. DOI: http://dx.doi.org/10.1016/j.fct.2015.02.023 [ Links ]
4.Luyt D, Ball H, Makwana N, Green MR, Bravin K, Nasser SM, et al. BSACI guideline for the diagnosis and management of cow's milk allergy. Clin Exp Allergy. 2014;44(5):642-72. DOI: http://dx.doi.org/10.1111/cea.12302 [ Links ]
5.Nosan G, Jakic M, Jager M, Paro-Panjan D. Prognostic accuracy of clinical signs and diagnostic tests in cow's milk allergy in newborns. Pediatr Neonatol. 2017;58(5):449-54. DOI: http://dx.doi.org/10.1016/j.pedneo.2016.09.009 [ Links ]
6.Fiocchi A, Brozek J, Schünemann H, Bahna SL, Berg A, Beyer K, et al. World Allergy Organization (WAO) diagnosis and rationale for action against cow's milk allergy (DRACMA) guidelines. Pediatr Allergy Immunol. 2010; 21 (Suppl 21):1-125. DOI: http://dx.doi.org/10.1111/j.1399-3038.2010.01068.x [ Links ]
7.Sahi T. Genetics and epidemiology of adult-type hypolactasia. Scand J Gastroenterol Suppl. 1994;202:7-20. DOI: http://dx.doi.org/10.3109/00365529409091740 [ Links ]
8.Mattar R, Mazo DFC. Intolerância à lactose: mudança de paradigmas com a biologia molecular. Rev Assoc Med Bras. 2010;56(2):230-6. DOI: http://dx.doi.org/10.1590/S0104-42302010000200025 [ Links ]
9.Mehta R. Allergy and asthma: food allergies. FP Essent. 2018;472:16-19. [ Links ]
10.Cordero RC, Prado SF, Bravo JP. Actualización en manejo de Alergia a la proteína de leche de vaca: fórmulas lácteas disponibles y otros brebajes. Rev Chil Pediatr. 2018;89(3):310-17. DOI: http://dx.doi.org/10.4067/S0370-41062018005000503 [ Links ]
11.Cummings AJ, Knibb RC, King RM, Lucas JS. The psychosocial impact of food allergy and food hypersensitivity in children, adolescents and their families: a review. Allergy. 2010;65(8):933-45. DOI: http://dx.doi.org/10.1111/j.1398-9995.2010.02342.x [ Links ]
12.Monks H, Gowland MH, MacKenzie H, ErlewynLajeunesse M, King R, Lucas JS, et al. How do teenagers manage their food allergies? Clin Exp Allergy. 2010;40(10):1533-40. DOI: http://dx.doi.org/10.1111/j.1365-2222.2010.03586.x [ Links ]
13.Bollinger ME, Dahlquist LM, Mudd K, Sonntag C, Dillinger L, McKenna K. The impact of food allergy on the daily activities of children and their families. Ann Allergy Asthma Immunol. 2006;96(3):415-21. DOI: http://dx.doi.org/10.1016/S1081-1206(10)60908-8 [ Links ]
14.MacKenzie H, Roberts G, van Laar D, Dean T. Teenagers' experiences of living with food hypersensitivity: a qualitative study. Pediatr Allergy Immunol. 2010;21(4 Pt 1):595-602. DOI: http://dx.doi.org/10.1111/j.1399-3038.2009.00938.x [ Links ]
15.Yonamine GH, Contim D, Castro APBM, Jacob CMA, Pastorino AC. Percepção dos familiares de pacientes com alergia ao leite de vaca em relação ao tratamento. J Hum Growth Dev. 2013;23(1):58-64. DOI: https://doi.org/10.7322/jhgd.50392 [ Links ]
16.Iervolino SA, Pelicioni MCF. A utilização do grupo focal como metodologia qualitativa na promoção da saúde. Rev Esc Enferm USP. 2001;35(2):115-21. DOI: http://dx.doi.org/10.1590/S0080-62342001000200004 [ Links ]
17.Turato ER. Tratado de metodologia da pesquisa clínico-qualitativa: construção teórico-epistemológica, discussão comparada e aplicação nas áreas de saúde e humanas. Petrópolis: Vozes, 2003. [ Links ]
18.Lebart L, Salem A. Statistique textuelle. Paris: DUNOP, 1994. [ Links ]
19.Ratinaud P. IRAMUTEQ: Interface de R pour les Analyses Multidimensionnelles de Textes et de Questionnaires. Un logiciel libre construit avec des logiciels libres. [cited 2017 May 19]. Available from: http://www.iramuteq.org/ [ Links ]
20.Reinert M. Alceste une méthodologie d'analyse des donnés textuelles et une application: Aurelia de Gerard de Nerval. Bull Methodol Sociol. 1990;26(1):24-54. DOI: http://dx.doi.org/10.1177/075910639002600103 [ Links ]
21.Queiroz AAFLN, Sousa AFL. Fórum PrEP: um debate on-line sobre uso da profilaxia pré-exposição no Brasil. Cad Saúde Pública. 2017;33(11):e00112516. DOI: http://dx.doi.org/10.1590/0102-311x00112516 [ Links ]
22.Shimizu HE, Cruz MS, Bretas Júnior N, Schierholt SR, Ramalho WM, Ramos MC, et al. O protagonismo dos Conselhos de Secretários Municipais no processo de governança regional. Cien Saude Coletiv. 2017;22(4):1131-40. DOI: http://dx.doi.org/10.1590/1413-81232017224.28232016 [ Links ]
23.Campos CJG, Turato ER. Análise de conteúdo em pesquisas que utilizam metodologia clínico-qualitativa: aplicação e perspectivas. Rev Latino-Am Enfermagem. 2009;17(2):259-64. DOI: http://dx.doi.org/10.1590/S0104-11692009000200019 [ Links ]
24.Bardin L. Análise de conteúdo. São Paulo: Edições 70, 2011. [ Links ]
25.Camargo BV, Justo AM. IRAMUTEQ: um software gratuito para análise de dados textuais. Temas Psicol. 2013;21(2):513-18. DOI: http://dx.doi.org/10.9788/TP2013.2-16 [ Links ]
26.Binsfeld BL, Pastorino AC, Castro APBM, Yonamine GH, Gushken AKF, Jacob CMA. Conhecimento da rotulagem de produtos industrializados por familiares de pacientes com alergia a leite de vaca. Rev Paul Pediatr. 2009;27(3):296-302. DOI: http://dx.doi.org/10.1590/S0103-05822009000300010 [ Links ]
27.Mofidi S. Nutritional management of pediatric food hypersensitivity. Pediatrics. 2003;111(6):1645-53. [ Links ]
28.Mazer Papa AM, Tabchoury CP, Del Bel Cury AA, Tenuta LM, Arthur RA, Cury JA. Effect of milk and soy-based infant formulas on in situ demineralization of human primary enamel. Pediatr Dent. 2010;32(1):35-40. [ Links ]
29.Cagetti MG, Congiu G, Cocco F, Meloni G, Sale S, Campus G. Are distinctive risk indicators associated with different stages of caries in children? A cross-sectional study. BMC Public Health. 2016;16(1):1213. DOI: http://dx.doi.org/10.1186/s12889-016-3865-4 [ Links ]
30.Carvalho CAP, Nicodemo CAZ, Mercadante DCF, Carvalho FS, Buzalaf, MAR, Sales-Peres SHC. Dental fluorosis in the primary dentition and intake of manufactured soy-based foods with fluoride. Clin Nutr. 2013;32(3):432-37. DOI: http://dx.doi.org/10.1016/j.clnu.2012.09.006 [ Links ]
31.Torres CP, Chinelatti MA, Gomes-Silva JM, Rizóli FA, Oliveira MAHM, Palma-Dibb RG, et al. Surface and subsurface erosion of primary enamel by acid beverages over time. Braz Dent J. 2010;21(4):337-45. DOI: http://dx.doi.org/10.1590/s0103-64402010000400009 [ Links ]
32.Moimaz SAS, Amaral MA, Garbin CAS, Saliba TA, Saliba O. Caries in children with lactose intolerance and cow's milk protein allergy. Braz Oral Res. 2018;32:e91. DOI: http://dx.doi.org/10.1590/1807-3107bor-2018.vol32.0091 [ Links ]
33.Edmonds-Myles S, Tamborlane WV, Grey M. Perception of the impact of type 1 diabetes on low-income families. Diabetes Educ. 2010;36(2):318-25. DOI: http://dx.doi.org/10.1177/0145721709349219 [ Links ]
34.Luna A, Gomes M, Granville-Garcia A, Menezes V. Perception of treatment needs and use of dental services for children and adolescents with sickle cell disease. Oral Health Prev Dent. 2018;16(1):51-7. DOI: http://dx.doi.org/10.3290/j.ohpd.a39817 [ Links ]
35.Rouf K, White L, Evans K. A qualitative investigation into the maternal experience of having a young child with severe food allergy. Clin Child Psychol Psychiatry. 2011;17(1):49-64. DOI: http://dx.doi.org/10.1177/1359104511415636 [ Links ]
36.Teufel M, Biedermann T, Rapps N, Hausteiner C, Henningsen P, Enck P, et al. Psychological burden of food allergy. World J Gastroenterol. 2007;13(25):3456-65. DOI: http://dx.doi.org/10.3748/wjg.v13.i25.3456 [ Links ]
37.Freitas MCS, Minayo MCS, Ramos LB, Fontes GV, Santos LA, Souza EC, et al. Escola: lugar de estudar e de comer. Cienc Saude Coletiva. 2013;18(4):979-85. DOI: http://dx.doi.org/10.1590/S1413-81232013000400010 [ Links ]
38.Alanne S, Laitinen K, Soderlund R, Paavilainen E. Mothers' perceptions of factors affecting their abilities to care for infants with allergy. J Clin Nurs. 2011;21(1-2):170-9. DOI: http://dx.doi.org/10.1111/j.1365-2702.2010.03587.x [ Links ]
39.Hodge A. Challenges in child and adolescent nutrition. Public Health Nutr. 2019;22(1):1-2. DOI: https://doi.org/10.1017/S1368980018003646 [ Links ]
40.Bischoff SC, Boirie Y, Cederholm T, Chourdakis M, Cuerda C, Delzenne NM, et al. Towards a multidisciplinary approach to understand and manage obesity and related diseases. Clin Nutr. 2017;36(4):917-38. DOI: http://dx.doi.org/10.1016/j.clnu.2016.11.007 [ Links ]
 Correspondence:
Correspondence:
sasaliba@foa.unesp.br
Manuscript received: September 2018
Manuscript accepted: August 2019
Version of record online: October 2019


{kind=link}
{kind=link}
{kind=link}