










Serviços Personalizados
artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282versão On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.30 no.1 São Paulo jan./abr. 2020
http://dx.doi.org/10.7322/jhgd.v30.9963
ORIGINAL ARTICLE
Nutritional profile of women assisted by the program of Family Health Strategy in Maranhão State, Brazil
Perfil nutricional de mulheres atendidas pela Estratégia Saúde da Família Maranhão, Brasil
Patricia Dore VieiraI,VIII; Maria Tereza Borges Araújo FrotaII,III; Elida Mara Braga RochaIII,VII; Sophia Cornbluth SzarfarcIII; Italla Maria Pinheiro BezerraVI; Viviane Gabriela NascimentoIV,V; Claudio LeoneI,IV; Luiz Carlos de AbreuI,IV
ILaboratório de Delineamento de Estudos e Escrita Científica da Faculdade de Medicina do ABC. Santo André, SP, Brasil
IIDepartamento de Nutrição, Universidade Federal do Maranhão, São Luiz, Maranhão
IIIDepartamento de Nutrição, Faculdade de Saúde Pública, Universidade de São Paulo, São Paulo, SP, Brasil
IVDepartamento de Saúde, Ciclos de Vida e Sociedade. Faculdade de Saúde Pública, Universidade de São Paulo, São Paulo, SP, Brasil
VProfessora Titular da Universidade Paulista - UNIP
VIEscola Superior de Ciências da Santa Casa de Misericórdia de Vitória, Vitória, Espírito Santo, Brasil
VIIFaculdade Juazeiro do Norte
VIIIFaculdade de Medicina Estácio de Juazeiro do Norte
ABSTRACT
INTRODUCTION: Inadequate diet, whether due to excess or insufficient calories and nutrients, results in health risk situations as well as inadequate nutritional profile. The presence of nutritional deficiencies is more visible in women and, therefore, is more likely to reflect the risks of such deficiencies. Knowing the profile of the nutritional status of the female population of Maranhão, Brazil, which provide evidence of the nutritional status of their families, may support the creation of specific actions to combat eating problems and, consequently, improve their health
OBJECTIVE: To evaluate the nutritional profile and its relationship with social determinants in a population of women attended by the program of Family Health Strategy in Maranhão
METHODS: Cross-sectional study with 989 women aged 15 to 49 years, carried out during July to September 2010. Socioeconomic data were collected through a questionnaire, in addition it was applied of the Brazilian Food Insecurity Scale to know the level of food insecurity. Body mass index (BMI) and hip and waist circumference measurements were obtained to verify the nutritional profile. The variables were analyzed for frequencies, distribution and central tendency. Bivariate analysis was performed as to the associations between socioeconomic variables and BMI. The Spearman correlation coefficient was used between the food safety score and the BMI, adopting a significance level of 5%. Multivariate linear regression analysis was performed
RESULTS: It was found a relationship between the BMI classification with some social determinants such as age, family income and food insecurity. There is a high prevalence of women at nutritional risk, especially for overweight and obesity, as well as the presence of thinness and short stature
CONCLUSION: Socioeconomic factors have a significant association with women's Body Mass Index indicating that there is an important relationship between age-matched maternal Body Mass Index and food insecurity
Keywords: women of reproductive age, body mass index, brazilian food insecurity scale, family health strategy.
Authors summary
Why was this study done?
The nutritional transition is a worldwide phenomenon that has led, even among populations of low socioeconomic status, significant increase in the prevalence of obesity and its consequences. This study aimed to know the nutritional status of women from Maranhão, assisted by the Family Health Strategy (FHS) program, aiming at proposals that are consistent with their social characteristics.
What did the researchers do and find?
The evaluation of the body mass index showed the presence of malnutrition occurs in Maranhão, Brazil, in an acceptable proportion according to the standard distribution proposed by World Health Organization (WHO). Overweight and obesity exist in a worrying proportion to demand the search for feasible interventions for this population studied. The association between the presence of overweight/obesity and subjective food insecurity assessed by the Brazilian Food Insecurity Scale (EBIA) suggests that habitual eating does not meet the nutritional needs of most people who are hungry and/or afraid of starvation.
What do these findings mean?
Effective strategies to aware the population that an adequate nutritional status is the best prevention against the occurrences of common chronic diseases among obese people. The cost of addressing these consequences for public spending at the three levels of health care and at the three levels of government cannot be neglected.
It is up to the public power to defend and protect the population in their human rights to adequate food and health, meeting the demand for a democratic, just and egalitarian society. Likewise, the State must ensure that public resources are available to all citizens regardless of their social and economic condition, allowing the welfare of all free from iniquities.
INTRODUCTION
The analysis of the nutritional status of the individual contributes to assess the extent to which their physiological nutrient needs are being met, in order to maintain the body's composition and functions, which results from the balance between nutrient intake and need1.
The world is currently living a moment of epidemiological and nutritional transition, progressively changing from a scenario in which malnutrition prevailed. Today, a scenario of overweight and obesity has prevailed.
In 2004, for the first time on the planet, the number of overweight people exceeded the number of malnourished, reaching about one billion overweight adults, of whom 300 million were obese2,3.
In Brazil, statistics indicate that 40% of adults are overweight and in almost all age groups there is an increased prevalence of obesity4.
This nutritional transition has had serious consequences over time, including in Brazil and even in less developed countries. Over the past fifty years, changes in diet quantity and quality have been observed, associated with changes in lifestyle, economic, social and demographic conditions, with negative repercussions on population health5,6.
In Brazil, the nutritional status of the population has been the subject of great attention in the field of public health and, as this context points out, its periodic assessment is particularly important, especially in populations of higher-risk areas, such as the state of Maranhão.
Located in Northeastern Brazil, Maranhão has a Human Development Index (HDI) of 0.69, which ranks it in the penultimate position among Brazilian states7. It is also the state with the largest proportion of socially excluded population, with a Social Exclusion Index (HEI) of 59.6%, the highest in the region8. The prevalence of population living in a situation of indigence more than doubles in relation to Brazil and 25.7% of its inhabitants are in extreme poverty9.
In this scenario, even considering the issues related to the quality of public actions in Primary Health Care, it is undeniable the importance that the program Family Health Strategy (FHS) assumes in the restructuring of the health system and organization of primary care10,11, as well as the Bolsa Familia is a conditional cash transfer program that benefits families in poverty and extreme poverty. This program should include dimensions such as the promotion of immediate poverty alleviation through the direct transfer of income to families, in addition to reinforcing the exercise of basic social rights in the areas of health and education, through the monitoring of conditionalities, which contributes to that families are able to break the cycle of poverty between generations in order to offer support for the development of families' capacities through the articulation with complementary training programs, job and income generation, literacy, among others12.
The aim of this study is to evaluate the nutritional status and its relationship with social determinants in the population of women attended by the Family Health Strategy program in the State of Maranhão, Brazil.
METHODS
This is a Cross-sectional study, with analysis of secondary data from the research project "Prevalence and Determinants of Anemia in Women and Children in the State of Maranhão", developed with the objective of evaluating the health and nutrition conditions of children under five and women of reproductive age in the state of Maranhão13.
In Maranhão, the FHS program started in 1994 in the municipality of São Luís, gradually expanding to 100% of its municipalities, reaching in 2012 a population coverage of around 81.2%14.
For the present study, there were selected the capital city of São Luis and five municipalities from each of the four state macroregions, and 40 families were surveyed in each one of them. The families included in the sample were randomly selected from the list of families attended by the FHS program in Maranhão14.
From this sample resulted 989 women aged 15 to 49 years. Data were collected from July to September 2010.
Standardized forms were used to collect data of socioeconomic conditions: place of residence, (urban and rural), family composition, maternal education, family income, access to benefits and governmental social programs such as family allowance and maternal age.
Household food security was also assessed using the Brazilian Food Insecurity Scale (EBIA)15.
Measurements of weight and height were collected from the participants to calculate their Body Mass Index (BMI) and classify their nutritional status.
Nutritional status was classified according to the reference values for BMI proposed by the World Health Organization16.
The variables were analyzed for frequencies, distribution and central tendency. A bivariate analysis was performed regarding the associations between socioeconomic variables and BMI. The Spearman correlation coefficient between the food safety score and the women's BMI was also calculated. The level of significance adopted was 5%. At the end, the linear regression analysis of multiple variables was performed, including in the model all variables that in the bivariate analysis had values of p<0.20.
This research was developed according to Resolution CNS 466/12 of the National Health Council, approved by the Ethics Committee of the University of São Paulo, School of Public Health (No. 2191/10), with the formal consent of the institutions involved and the agreement with the person responsible for the services, as well as the signing of the Informed Consent Form by the studied population.
RESULTS
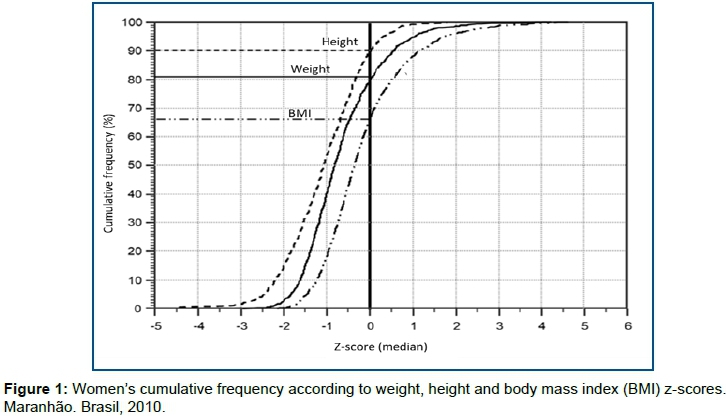
The total study sample consisted of 989 women, whose average age was 27.5 years (standard deviation (SD)=7.0), weight average 57.7kg (SD=11.6), height 1 .54m (SD=0.59m) and Body Mass Index of 24.3kg/m2 (sd=4.5) (Figure 1).
In Figure 1, it is observed that 90% of women were below the median height and 81% were below the median height. Regarding BMI, the proportion of women below the median was 67%.
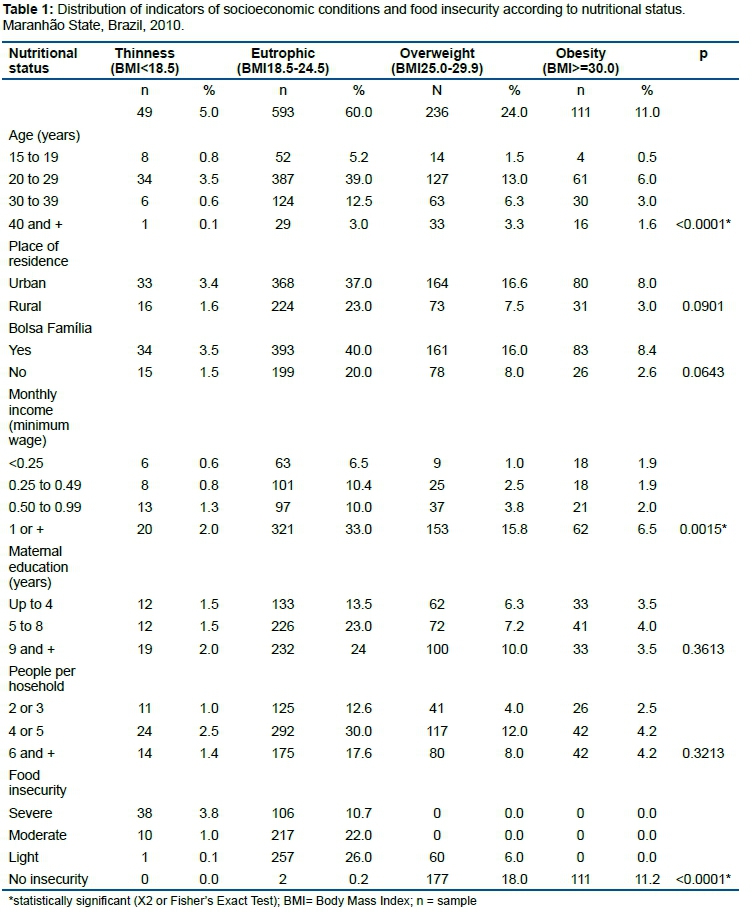
Regarding nutritional status, 60% (n = 593) of the women were eutrophic, 5% (n = 49) were thin, 24% (n = 236) and 11% (n = 111) overweight and obesity (Table 1).
Bivariate analysis (Table 1) showed a significant association between nutritional status and maternal age (p <0.0001), family income (p = 0.0015) and food insecurity (p <0.0001).
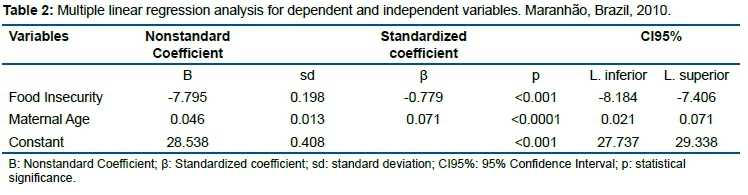
For the multivariate linear regression analysis, we selected the statistically significant characteristics in the bivariate (maternal age, family income and food insecurity) and also the variables: place of residence and family allowance benefit, for its epidemiological plausibility.
At the end of the multiple variable analysis, only maternal age and food insecurity remained significant.
In the multivariate regression analysis, a higher maternal age resulted as a risk factor for a higher BMI, coef.: 0.71 (p> 0.0001), while the condition of lower food insecurity resulted in a protective factor for lower BMI, coef.: -0.78 (p <0.0001) (Table 2).
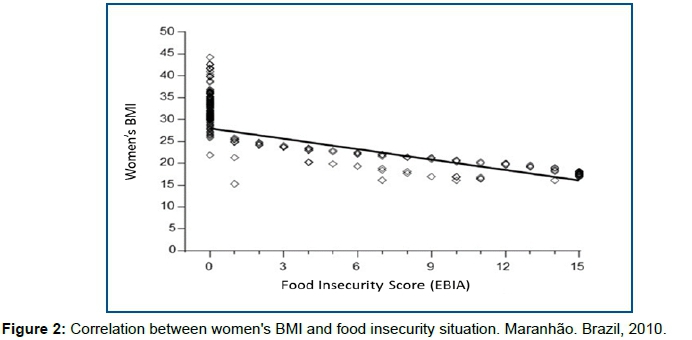
The Figure 2 illustrates a statistically significant inverse correlation between BMI in absolute value and food security, showing that the higher the food security at home, higher BMI values are observed among women, Pearson's coefficient: -0, 97 (p <0.0001).
DISCUSSION
Women's height measurements indicate that 40% of them must have shown linear growth during childhood and adolescence below normal as expected, as only one in ten had a height above the median of the reference population.
About 30% of women have probably lower weight than what is expected, as only 1/5 of them were overweight. However, is more than one malnutrition process in force, this represents a weight that is a consequence of the smaller stature that these women had, since the proportion of thinness observed from the BMI z-score is practically as expected from the reference distribution, ie about 2.5% of women with BMI z-score <-2.017.
BMI has the advantage of being easily obtained from standardization of getting weight and height measurements, besides it is related to causes of morbidity and mortality, in this case, especially in the extreme limits of its values18.
The distribution of the BMI z-score values shows that 1/3 of the women had a value above the median, which corroborates the previous hypothesis that they had a weight probably due to a shorter stature, which is very relevant. Among these, there is already a tendency towards a high prevalence of overweight and obesity.
This analysis, when done by the WHO classification based on absolute BMI values, indicates that one in four and one in ten women of the sample are already classified as overweight and obesity respectively.
The prevalence of thinness was 5.0% which is practically the same as described for the Northeast region where it reached 5.2%. According the National Demographic and Health Survey of Children and Women 200919 the proportions of overweight and obese women are also lower than the values reported in Northeast region as follows 41% overweight and 14.7% obese. The numbers are also lower to the ones reported by the Northeast Semi-Arid region where were found, 32.6 overweight and 16.1% obesity20.
Thus, the reality of the increase in overweight cases in women from Maranhão does not exactly reflect the reality of other regions of the country. This difference is probably explained by the pronounced poor income distribution in Maranhão5,21.
These distinct values, besides being justified by possible sample and methodological differences among the studies, may also be due to a slower evolution of the Nutritional Transition in the state of Maranhão, which makes it be in a initial stage of transition compared to the rest of the northeast region, as a consequence of the state's socioeconomic reality, which has about ¼ of the population in extreme poverty9,11,22,23.
Preliminary analysis of the data from the present study indicated a relationship between women's BMI classification and age, household income and food insecurity at home.
In this phase, BMI was not associated with: place of residence (urban or rural), family allowance, maternal education and number of people residing in the same household. Although classically cited as associated with nutritional status, their non-association in the present sample was probably due to the limited variation that these risk factors present in a population that can be considered homogeneously of low socioeconomic status.
Regarding the average BMI for family income, it is found that as family income decreases, there is a reduction in women's BMI level, similarly reported by other studies showing the influence mainly of income, maternal education and sanitation conditions on the risk of protein-energy malnutrition present in the Brazilian population21,24,25. Although Bolsa Família program did not present statistical significance in its relationship with BMI, more than 60% of families receive such benefit, which aims to improve family income and, therefore, can reduce the risk of food insecurity.
However, the final analysis of those same variables together by multivariate linear regression showed that only maternal age and food security/insecurity were associated with women's BMI.
The correlation between BMI and age, although not so high, is an expected phenomenon as age advances, as there are already data in the literature that point to a tendency to increase body weight with age26.
As might be expected, due to the risk of food deficiency at its various levels, it effectively results in lower energy consumption and, consequently, a lower risk of overweight. The converse also occurs, the greater the food security the greater the diversification of food items consumed, especially those showed in the media. Higher food insecurity is related to a tendency to lower BMI among women, while the opposite condition, ie food security, already shows a significant prevalence of overweight and obesity even in this population of low-income women.
In accordance with these results, the relationship between food insecurity and lower family income, low education, higher number of residents in the household, inadequate sanitation conditions, lack of employment and higher prevalence of nutritional risk among families in rural areas were evidenced. Regarding food intake, in addition to the quantitative restriction identified by the EBIA, Food Insecurity has also been related to a lower dietary quality, with lower consumption of protein-rich foods (belonging to the legume, milk and derivatives and meats and eggs) and regulators (fruits and vegetables), as well as higher omission of meals and glycemic27.
It is important to consider that these nutritional changes are present in families that are assisted by the FHS program, which suggests that the need for food orientation must be emphasized to better adapt it to the reality of the State of Maranhão.
The FHS program should include dimensions such as the promotion of immediate poverty alleviation through direct income transfer to families, as well as strengthening the exercise of basic social rights in the areas of health and education, through the monitoring of conditionalities, which contributes to that families can break the cycle of intergenerational poverty in order to support the development of families' capacities through articulation with complementary training, employment and income generation, literacy programs, among others12.
In parallel, it is essential that the actions developed aiming at income redistribution are reviewed, since they are key for changing this reality. At this time, actions aimed at preventing the increase in the prevalence of overweight and obesity in the population are also fundamental, as part of the necessary strategies to minimize or even avoid the already known health complications that result from these nutritional changes, such as chronic non communicable diseases28.
CONCLUSION
Compared to Brazil as a whole and even with the rest of the Northeast region, the state of Maranhão has a high prevalence of women at nutritional risk, especially for overweight and obesity, although there is the presence of thinness and short height, which characterizes a nutritional transition even at earlier stages
Socioeconomic factors have a significant association with women's Body Mass Index indicating that there is an important relationship between age-matched maternal Body Mass Index and food insecurity.
REFERENCES
1.Acuna K, Cruz T. Avaliação do estado nutricional de adultos e idosos e situação nutricional da população brasileira. Arq Bras Endocrinol Metab. 2004;48(3):345-61. DOI: http://dx.doi.org/10.1590/S0004-27302004000300004 [ Links ]
2.Organização Mundial de Saúde (OMS). Obesidade: prevenção e controle e epidemia global. Relatório da Consultoria da OMS. São Paulo: Roca, 2004. [ Links ]
3.World Health Organization. Obesity and overweight. [cited 2016 ago 21] Available from: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight [ Links ]
4.Monteiro CA, Moura EC, Conde WL, Popkin BM. Socioeconomic status and obesity in adult populations of developing countries: a review. Bull World Health Org. 2004; 82(12):940-6. [ Links ]
5.Batista Filho M, Rissin A. A transição nutricional no Brasil: tendências regionais e temporais. Cad Saúde Pública. 2003;19(Sup. 1): S181-91. DOI: http://dx.doi.org/10.1590/S0102-311X2003000700019 [ Links ]
6.Souza NP, Lira PIC, Fontbonne A, Pinto FCL, Cesse EAP. A (des)nutrição e o novo padrão epidemiológico em um contexto de desenvolvimento e desigualdades. Ciênc Saúde Coletiva. 2017;22(7):2257-66. DOI: https://doi.org/10.1590/1413-81232017227.03042017 [ Links ]
7.Comissão Econômica para a América Latina e o Caribe (CEPAL). Programa das Nações Unidas para o Desenvolvimento (PNUD). Organização Internacional do Trabalho (OIT). Emprego, desenvolvimento humano e trabalho decente: a experiência brasileira recente. Brasília: CEPAL/ PNUD/OIT, 2008. [ Links ]
8.Silva MO. Avaliando o Bolsa Família: unificação, focalização e impactos. São Paulo: Cortez, 2010. [ Links ]
9.Instituto Brasileiro de Geografia e Estatística (IBGE). Censo demográfico 2010: IBGE Estados: Maranhao (12° Recenseamento Geral do Brasil). [cited 2016 Nov 02] Available from: www.ibge.gov.br/home/.../censo2010/.../total_populacao_maranhao.pdf. [ Links ]
10.Brasil. Ministério da Saúde. Secretaria de Atenção a Saúde. Departamento de Atenção Básica. Política Nacional de atenção Básica (PNAB). Brasília: Ministério da Saúde, 2006. [ Links ]
11.Alves MTSSB, Batista RFL, Silva AAM, Coimbra LC. Atenção à saúde nos seis municípios mais população do Maranhão: os caminhos percorridos. In: Alves MTSSB, Sousa MPS, Coimbra LC. Atenção à Saúde do adulto e da criança no Maranhão. São Luis: EDUFMA, 2009; p.25-31. [ Links ]
12.Silva MOS. O Bolsa Família: problematizando questões centrais na política de transferência de renda no Brasil. Ciênc Saúde Coletiva. 2007;12(6):1429-39. DOI: http://dx.doi.org/10.1590/S1413-81232007000600006 [ Links ]
13.Frota MTBA, Szarfarc SC. Prevalência e fatores associados à anemia em mulheres e crianças no Maranhão. Tese (Doutorado) - Faculdade de Saúde Pública, Universidade de São Paulo. São Paulo: 2013. [ Links ]
14.Brasil. Ministério da Saúde. Secretaria de Atenção Básica. Departamento de Atenção Básica. Coordenação-geral da Política de Alimentação e Nutrição. Estratégias de promoção da alimentação saudável para o nível local. Relatório da Oficina de Trabalho do I Seminário sobre Política Nacional de Promoção da Saúde. Brasília: Ministério da Saúde, 2007. [ Links ]
15.Ruschel LF, Henn RL, Backes V, Melo P, Marques LAS, Olinto MTA. Insegurança alimentar e consumo alimentar inadequado em escolares da rede municipal de São Leopoldo, RS, Brasil. Ciênc Saúde Coletiva. 2016;21(7):2275-85. DOI: http://dx.doi.org/10.1590/1413-81232015217.00742015 [ Links ]
16.Brasil. Ministério da Saúde. Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Protocolos do Sistema de Vigilância Alimentar e Nutricional - SISVAN na assistência à saúde. Brasília: Ministério da Saúde, 2008. [ Links ]
17.Frisancho AR. New norms of upper limb fat and muscle areas for assessment of nutritional status. Am J Clin Nutr. 1981;34(11):2540-5. DOI: http://dx.doi.org/10.1093/ajcn/34.11.2540 [ Links ]
18.Nascimento MM, Pereira LGD, Cordeiro PR, Araújo LMG. Comparison and agreement of criteria for the BMI classification of physically active elderly women living in the Backlands, semi-arid Region. J Hum Growth Dev. 2017;27(3):342-9 DOI: https://doi.org/10.7322/jhgd.128227 [ Links ]
19.Brasil. Ministério da Saúde. Centro Brasileiro de Análise e Planejamento. Pesquisa Nacional de Demografia e Saúde da Criança e da Mulher. PNDS 2006: Dimensões do processo reprodutivo e da saúde da criança. Brasília: ministério da Saúde, 2009. [ Links ]
20.Correia LL, Silveira DMI, Silva AC, Campos JS, Machado MMT, Rocha HAL, et al. Prevalência e determinantes de obesidade e sobrepeso em mulheres em idade reprodutiva residentes na região semiárida do Brasil. Ciênc Saúde Coletiva. 2011;16(1):133-45. DOI: http://dx.doi.org/10.1590/S1413-81232011000100017 [ Links ]
21.Linhares RS, Horta BL, Gigante DP, Dias-da-Costa JS, Olinto MTA. Distribuição de obesidade geral e abdominal em adultos de uma cidade no Sul do Brasil. Cad Saúde Pública. 2012;28(3):438-47. DOI: http://dx.doi.org/10.1590/S0102-311X2012000300004 [ Links ]
22.Popkin BM. The nutrition transition and obesity in the Developing World. J Nutr. 2001;131(3):871S-3. DOI: https://doi.org/10.1093/jn/131.3.871S [ Links ]
23.Popkin BM, Adair LS, Ng SW. Global nutrition transition and the pandemic of obesity in developing countries Nutr Rev. 2011;70(1):3-21. DOI: https://doi.org/10.1111/j.1753-4887.2011.00456.x [ Links ]
24.Batista Filho M, Rissin A. A transição nutricional no Brasil: tendências regionais e temporais. Cad Saúde Pública. 2003;19(Supl. 1):S181-91. DOI: http://dx.doi.org/10.1590/S0102-311X2003000700019 [ Links ]
25.Souza EB. Transição nutricional no Brasil: análise dos principais fatores. Cad UniFoA. 2010;5(13):49-53. [ Links ]
26.Peixoto MRG, Cordeiro MM, Ferreira VR, Cardoso CKS, Crispim PAA. Ganho de peso na vida adulta: preditor da hipertensão arterial?. Cad Saúde Coletiva. 2017;25(1):58-64. DOI: http://dx.doi.org/10.1590/1414-462X201700010023 [ Links ]
27.Almeida JA, Santos SA, Nascimento MAO, Oliveira JVC, Silva DG, Mendes-Netto RS. Fatores associados ao risco de insegurança alimentar e nutricional em famílias de assentamentos rurais. Ciênc Saúde Coletiva. 2017;22(2):479-88. DOI: http://dx.doi.org/10.1590/1413-81232017222.27102015 [ Links ]
28.Brasil. Ministério da Saúde. Secretaria de Atenção Básica. Departamento de Ações Programáticas Estratégicas. Relatório de gestão 2003 a 2006: Política Nacional de Atenção Integral a Saúde da mulher. Brasília: Ministério da Saúde, 2007. [ Links ]
 Correspondence:
Correspondence:
mariaterezafrota@gmail.com
Manuscript received: September 2019
Manuscript accepted: February 2020
Version of record online: March 2020


{kind=link}
{kind=link}
{kind=link}
{kind=link}