










Serviços Personalizados
artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282versão On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.30 no.1 São Paulo jan./abr. 2020
http://dx.doi.org/10.7322/jhgd.v30.10086
ORIGINAL ARTICLE
Evidence-based Physiotherapy and Functionality in Adult and Pediatric patients with COVID-19
Evidências científicas sobre Fisioterapia e funcionalidade em pacientes com COVID-19 Adulto e Pediátrico
Cássio Magalhães da Silva e SilvaI; Aline do Nascimento AndradeII; Balbino NepomucenoIII; Daniel Salgado XavierIV; Eugênia LimaV; Iura GonzalezVI; Juliana Costa SantosI; Mateus Souza EsquivelVII; Michelli Christina Magalhães NovaisVIII; Paulo MagalhãesIX; Robson da Silva AlmeidaX; Vinícius Afonso GomesXI; Vitor Oliveira CarvalhoXII; Wiron Correia Lima FilhoXIII; Oséas Florêncio de Moura FilhoXIII; Mansueto Gomes NetoI
IPhysiotherapist. Federal University of Bahia - Department of Physiotherapy
IIPhysiotherapist. Physiotherapist at Ana Nery Hospital
IIIPhysiotherapist. Aliança Hospital
IVPhysiotherapist. Municipal Health Secretariat \ AM
VPhysiotherapist. Tereza de Lisieux Hospital
VIPhysiotherapist. Bahiana School of Medicine and Public Health
VIIPhysiotherapist. Respiratory and Cardiovascular Physiotherapy Nucleus
VIIIPhysiotherapist. Jorge Amado University Center
IXPhysiotherapist. University of Pernambuco - Physiotherapy;
XPhysiotherapist. Madre Thaís College
XIPhysiotherapist. Ruy Barbosa-Wyde College
XIIPhysiotherapist. Federal University of Sergipe
XIIIPhysiotherapist. Brazilian Physiotherapy Society
ABSTRACT
INTRODUCTION: The corona virus (2019-nCoV OR HCOV-19 or CoV2), has emerged in China as the main cause of viral pneumonia (COVID-19, Coronavirus Disease-19). : To provide evidence-based Physiotherapy and functionality in patients with adult and pediatric COVID-19
METHODS: This is an integrative literature review using the MedLine / PubMed databases, library of Latin American and Caribbean Literature in Health Sciences (LILACS) and Physiotherapy Evidence Database (PEDRo
RESULTS: Part of the patients with covid 19 show signs of respiratory deficiency with hypoxemia, with low severity in children. Impaired functionality is also expected
CONCLUSION: COVID-19 causes low pulmonary compliance and important changes in lung function with hypoxemia and cardiovascular repercussions. These changes lead to the need for Physiotherapy and the management of oxygen therapy and ventilatory support (invasive and non-invasive) for these patients
Keywords: Physiotherapy, International Classification of Functionality, Disability and Health, hypoxia.
Authors summary
Why was this study done?
In view of the pandemic that also affects Brazil, a large number of patients with COVID-19 may have an important Respiratory System Deficiency. The Physiotherapist is the professional who is at the forefront of the process of assessment, diagnosis and intervention of the respiratory function. For this reason, it is necessary to better understand the evolution and therapeutic process of these patients, in order to provide management with greater expertise and quality.
What did the researchers do and find?
We seek to gather information through an integrative bibliographic review, in several databases and guidelines of the World Health Organization on COVID-19, with a focus on respiratory, muscular function, and on the functionality of these patients. As the moment is still little known by COVID-19, in this material we highlight the current knowledge processes for the assessment, diagnosis and Physiotherapeutic interventions.
What do these findings mean?
These findings confirm the dynamics, care and service provision for the professional Physiotherapist in a hospital and intensive care unit, for new practices that integrate the necessary advances in the quality of care, safety and prevention of patients with Respiratory Deficiency by COVID-19.
INTRODUCTION
The coronavirus infection pneumonia epidemic broke out in late December 2019 in the city of Wuhan in China, and spread rapidly across the country and all the continents of the world. Discovered through entire genome sequencing, the pathogen was considered a new beta coronavirus genus, and the pathology was called a new coronavirus pneumonia, defined by the World Health Organization1-4.
Clinical conditions such as hypertension, respiratory, cardiovascular, and metabolic diseases seem to be important risk factors for the severity of covid-195. Age is also an important unmodifiable risk factor. Patients with a mean age of 47 years had a mortality rate of 3 to 5%, oxygen therapy was necessary in 42% of these patients, 5% were admitted to the ICU, 2.3% underwent invasive mechanical ventilation (IMV), and of these, 1.4% died6,7.
The coronavirus responsible for COVID-19, may have repercussions that go beyond the involvement of the respiratory system, harming several systems, including the cardiovascular system8. COVID-19 can trigger decompensation of the cardiovascular system, especially in people with previous disorders, such as heart failure and coronary artery disease. In addition, studies indicate the occurrence of acute myocarditis and severe acute respiratory syndrome (SARS), which favors systolic dysfunction and myocardial infarction8,9.
Among the various professionals involved in the physical recovery of the patient with COVID-19, the physiotherapist stands out not for treating the disease but for preventing and rehabilitating respiratory deficiencies and the functional limitations of the daily life activity10.
COVID-19 is a disease that causes deficiency of respiratory tract structures, leading to impaired breathing functions11. Not only, depending on the clinical severity presented, there may be impaired respiratory muscle function and exercise tolerance. Limitations, which make it difficult to carry out basic activities that involve the ability to move, affecting even routine tasks such as walking and performing self transfers12.
As the Physiotherapist is in charge of the care process for these patients, there is a need to better understand the functional repercussions of COVID-19 in order to think about the best approach to the patient, thus, the objective of this work is to evaluate scientific evidence about Physiotherapy and functionality in patients with adult and pediatric COVID-19.
METHODS
It is an integrative literature review using the MedLine/PubMed database, library of Latin American and Caribbean Literature in Health Sciences (LILACS) and Physiotherapy Evidence Database (PEDRo). The approach was through a methodology that provides the synthesis of knowledge and the incorporation of the applicability of results of significant studies in practice on the scientific evidence for the performance of Physiotherapy at COVID-19. The literature review was carried out in March and April of 2020.
Thus, this study investigates and presents the scientific evidence in Physiotherapy and functionality in COVID-19 that can guide Physiotherapists in their daily conduct with these respective patients with recommendations.
Search strategy
The electronic search was performed by well-trained researchers with experience in the subject of the articles. The search was performed in March 2020 with the combination of the following terms: First combination: Covid 19 and coronavirus and coronavirus (COVID-19) infection. Second Combination: Physiotherapy and Covid 19 and coronavirus and coronavirus (COVID-19) infection. Third combination: Cardiac Involvement and coronavirus (COVID-19) infection. Fourth combination: Diagnosis and treatment and prevention and Covid 19 and coronavirus. From this search, articles were selected for full reading that met the inclusion criteria for this review.
Eligibility criteria
Published studies in English or Portuguese about COVID-19 and aspects related to Physiotherapy, mechanical ventilation, oxygen therapy and cardiac alterations were included. Reviews, meta-analyzes, editorials, original articles and Consensus were also included.
Summary of data
The summary included the extraction of the following data: authors and year of publication of the evidence, instruments and/or assessment equipment, and effects of the Physiotherapeutic performance in patients with COVID-19, with a focus on functionality. Finally, the outcomes pertinent to the therapeutic intervention in COVID-19 in respiratory function were evaluated for the production of evidence.
RESULTS
Despite the scarcity of studies, Table 1 shows the evidence found on the Deficiency of Respiratory Function in COVID-1913-25.
The recommendations in Physiotherapy for patients with Respiratory and Cardiac Disability by COVID-19 follow in an appendix to this study. (Attachment 1)
DISCUSSION
COVID-19 may have cardiovascular and myocardial repercussions13,14, retrospective multicenter study using a database from Jin Yin-tan Hospital and Tongji Hospital in China, showed that 33% of deaths were caused by the association of heart and respiratory failure, with 7% of deaths caused exclusively by myocardial injury25.
There is an indication for a closed suction system to perform bronchial hygiene therapy, as well as an occlusive face mask and in the pre-oxygenation of these hypoxemic patients19, as these protocols protect health professionals from contamination.
Exhaled air is known to increase virus dispersion and subsequently the risk of nosocomial infection26 and spread of the virus12,16. Procedures that enhance the aerosolization and contamination of health professionals are not indicated, associated with the absence of a proven benefit in the treatment of refractory hypoxemic respiratory failure27.
Opportunistic airborne transmission generally occurs during aerosol-generating health procedures such as patient coughing and contact with surfaces27, why 1716 healthcare workers were infected with SARS-CoV-2 in a hospital in China28.
About 41% of all patients hospitalized with COVID-19 used oxygen therapy18. In the study performed during the SARS-COVID pandemic in 2002, administrative factors were identified for greater risk of an outbreak, including the O2 flow rate> 6L / min, considered as "high flow". In this study, the adoption of high O2 rates increased the chances of providing a viral outbreak by 2.42 times than the adoption of low flow. Thus, the adoption of high oxygen flows should be discouraged in the absence of the respiratory isolation bed29,30.
NIV procedures23 should be performed with personal protective equipment and in those patients who develop dyspnea, tachypnea and peripheral oxygen desaturation. NIV can be used in those places where access to invasive mechanical ventilation is possible. Studies recommend only the use of a helmet with a double limb circuit, as they can reduce the risk of airborne transmission21.
In children with COVID-19, symptoms12,15 are usually less severe. COVID-19 is a disease that causes deficiency of respiratory tract structures11, in addition to thinking that the control of the spread of infection leads to the restriction of children's participation.
Infant COVID-19 is characterized by respiratory failure requiring ventilatory support. Neonatal and pediatric physiotherapy plays a fundamental role in multidisciplinary care, acting in order to identify, elaborate and develop kinetic-functional diagnosis in cardiorespiratory disorders caused by viral infection, through anamnesis, physical evaluation and complementary exams. In addition to developing promotion, prevention, rehabilitation and recovery strategies for children with risk factors for the development of problems and determinants of the health-disease process, at different levels of health care.
It is worth noting that patients who fail oxygen therapy, NIV, or have a direct indication for invasive mechanical ventilation, should be intubated quickly, as the need for intubation and IMV is common during this outbreak31. The need for intubation vary from 2,3% 4%7,32,33, to 42% e 47%30,32, considering the studies available in the literature. With differing rates regarding the need for intubation, attention to the patient's characteristics, specific care and a careful evaluation are essential at this time. Additionally, patients using invasive ventilation should be isolated in a single room12 and it is important to pay close attention to their handling with professional protection21.
Scientific studies from professional experiences in other places that struggle to treat patients with COVID-1934, it appears that due to the unsatisfactory results, high failure rate, higher risk of spreading the virus, and unavailability of the appropriate interface (helmet), in In most Brazilian intensive care units, NIV should be rethought and indicated with greater evaluative and diagnostic precision, and should not be a first-line ventilatory strategy, intended for patients with SARS / COVID-19 and that can be extrapolated to the nasal cannula of high flow.
Patients with tachypnea (respiratory rate > 30 ipm), hypoxemia, Spo2 less than 93% at room air and a Ratio of arterial oxygen pressure and the inspired fraction of oxygen <300 mmHg33, with progressive worsening of the clinical picture and with the prospect of continuing to worsen, and undergoing no clinical improvement at conventional oxygen therapy (face mask up to 5 liters or mask with reservoir, non-reinaline, up to 10 L/min)21,33,35,36, orotracheal intubation22 should be performed which must be performed with an occlusive face mask (well adjusted to the patient's face) coupled to a mask valve bag24.
The need to carefully assess the physiological signs for indication of orotracheal intubation in asymptomatic hypoxic patients, referred to as silent hypoxemia24, is emphasized, since the emergency intubation procedure poses a risk of cross infection37.
CNAF21 can be used in respiratory deficiency due to severe hypoxemia as long as it presents a potential response in oxygenation in the first 30 minutes of therapy. The use of CNAF should preferably be used with patients in beds with a negative pressure room, in order to reduce the potential for contamination with the formation of aerosol. It is worth mentioning the need for the health care team to use individual protective equipment during the application of this therapy. To date, the literature does not provide a basis to support the routine use of CNAF for the treatment of patients with COVID-1920,38.
Patients evaluated and prescribed for Physiotherapy21, must always promote Physiotherapeutic adaptations with the guidelines of the "Crisis Unit" and approved by the Directors of the Institutes that manage patients with COVID-19, in the specific professional environment of each hospital.
CONCLUSION
COVID-19 causes low pulmonary compliance and important changes in lung function with hypoxemia and cardiovascular repercussions. These changes lead to the need for Physiotherapy and the management of oxygen therapy and ventilatory support (invasive and non-invasive) for these patients. The need for further updates to this document is anticipated as changes in functionality for Physiotherapy are better known.
Acknowledgments
Brazilian Society of Physiotherapy - BSP
REFERENCES
1.Bogoch II, Watts A, Thomas-Bachli A, Huber C, Kraemer MUG, Khan K. Potential for global spread of a novel coronavirus from China. J Travel Med. 2020; 27(2):taaa011. DOI: http://doi.org/10.1093/jtm/taaa011 [ Links ]
2.Lu R, Zhao X, Li J, Peihua N, Bo yang, Hoglong Hu, et al. Genomic characterization and epidemiology of 2019 novel coronavirus: implications for virus origins and receptor binding. Lancet. 2020; 395(10224):565-74. DOI: http://doi.org/10.1016/S0140-6736(20)30251-8 [ Links ]
3.National Health Committee of the People's Republic of China. Notice of the National Health Committee on the provisional naming of new coronavirus pneumonia. [cited 2020 Feb 12] Available from: http://www.nhc.gov.cn/mohwsbwstjxxzx/s2908/202002/f15dda000f6a46b2a1ea1377cd80434d.shtml [ Links ]
4.World Health Organization (WHO). WHO Director-General's remarks at the media briefing on 2019-nCoV on 11 February 2020. [cited 2020 Feb 12] Available from: https://www.who.int/dg/speeches/detail/who-director-general-s-remarks-at-the-media-briefing-on-2019-ncov-on-11-february-2020 [ Links ]
5.Yang J, Zheng Y, Gou X, Pu K, Chen Z, Guo Q, et al. Prevalence of comorbidities in the novel Wuhan coronavirus (COVID-19) infection: a systematic review and meta-analysis. Int J Infect Dis. 2020;S1201-9712(20)30136-3. DOI: http://doi.org/10.1016/j.ijid.2020.03.017 [ Links ]
6.World Health Organisation (WHO). Coronavirus disease 2019 (COVID-19) Situation Report, 46. [cited 2020 Feb 12] Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports [ Links ]
7.Guan W, Ni ZY, Hu Y, Liang L, Ou C, He J, et al. Clinical characteristics of Corona virus Disease 2019 in China. New Engl J Med. 2020. DOI: http://doi.org/10.1056/NEJMoa2002032 [ Links ]
8.Inciardi RM, Lupi L, Zaccone G, Italia L, Raffo M, Tomasoni D, et al. Cardiac Involvement in a Patient With Coronavirus Disease 2019 (COVID-19). Jama Cardiol. 2020. DOI: http://doi.org/10.1001/jamacardio.2020.1096 [ Links ]
9.Madjid M, Safavi-Naeini P, Solomon SD, Vardeny O. Potential Effects of Coronaviruses on the Cardiovascular System A Review. Jama Cardiol. 2020. DOI: http://doi.org/10.1001/jamacardio.2020.1286 [ Links ]
10.Bispo Júnior JP. Fisioterapia e saúde coletiva: Desafios e novas responsabilidades profissionais. Cienc Saude Coletiva. 2010;15(Supl.1):1627-36. DOI: https://doi.org/10.1590/S1413-812320100007000741 [ Links ]
11.Xia W, Shao J, Guo Y, Peng X, Li Z, Hu D. Clinical and CT features in pediatric patients with COVID-19 infection: Different points from adults. Pediatr Pulmonol. 2020. DOI: https://doi.org/10.1002/ppul.24718 [ Links ]
12.Guanghai WYZ, Jin Z, Jun Z, Fan J. Mitigate the effects of home confinement on children during the COVID-19 outbreak. Lancet. 2020;395(10228):945-7. DOI: https://doi.org/10.1016/S0140-6736(20)30547-X [ Links ]
13.Bouadma L, Lescure FX, Lucet JC, Yazdanpanah Y, Timsit JF. Severe SARS-CoV-2 infections: practical considerations and management strategy for intensivists. Intensive Care Med. 2020;46(4):579-82. DOI: https://doi.org/10.1007/s00134-020-05967-x [ Links ]
14.Xu Z, Shi L, Wang Y, Zhang J, Huang L, Zhang C, et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir Med. 2020;8(4):420-422. DOI: https://doi.org/110.1016/S2213-2600(20)30076-X [ Links ]
15.Cai J, Xu J, Lin D, Yang Z, Xu L, Qu Z, et al. A Case Series of children with 2019 novel coronavirus infection: clinical and epidemiological features. Clin Infect Dis. 2020: ciaa198. DOI: https://doi.org/10.1093/cid/ciaa198 [ Links ]
16.Shen K, Yang Y, Wang T, Zhao D, Jiang Y, Jin R, et al. Diagnosis, treatment, and prevention of 2019 novel coronavirus infection in children: experts' consensus statement. World J Pediatr. 2020. DOI: https://doi.org/10.1007/s12519-020-00343-7 [ Links ]
17.Respiratory care committee of Chinese Thoracic Society. Expert consensus on preventing nosocomial transmission during respiratory care for critically ill patients infected by 2019 novel coronavirus pneumonia. Zhonghua Jie He He Hu Xi Za Zhi. 2020;17(0):E020. DOI: https://doi.org/10.3760/cma.j.issn.1001-0939.2020.0020 [ Links ]
18.van den Boom W, Hoy M, Sankaran J, Liu M, Chahed H, Feng M, et al. The Search for Optimal Oxygen Saturation Targets in Critically Ill Patients: Observational Data From Large ICU Databases. Chest. 2020;157:566-73. DOI: https://doi.org/10.1016/j.chest.2019.09.015 [ Links ]
19.Alhazzani W, Møller MH, Arabi YM, Loeb M, Gong MN, Fan E, et al. Surviving Sepsis Campaign: Guidelines on the Management of Critically Ill Adults with Coronavirus Disease 2019 (COVID-19). Intensive Care Med. 2020. DOI: https://doi.org/10.1007/s00134-020-06022-5 [ Links ]
20.Thomas P, Baldwin C, Bissett B, Boden I, Gosselink R, Granger CL, et al. Physiotherapy management for COVID-19 in the acute hospital setting: clinical practice recommendations. J Physiother. 2020. DOI: https://doi.org/10.1016/j.jphys.2020.03.011 [ Links ]
21.Cheung JC, Ho LT, Cheng JV, Cham EYK, Lam KN. Staff safety during emergency airway management for COVID-19 in Hong Kong. Lancet Respir Med. 2020;8(4):e19. DOI: https://doi.org/10.1016/S2213-2600(20)30084-9 [ Links ]
22.Meng L, Qiu H, Wan L, Ai Y, Xue Z, Guo Q, et al. Intubation and Ventilation amid the COVID-19 Outbreak: Wuhan's Experience. Anesthesiology. 2020. DOI: https://doi.org/10.1097/ALN.0000000000003296 [ Links ]
23.Murthy S, Gomersall CD, Fowler RA. Care for Critically Ill Patients With COVID-19. JAMA. 2020. DOI: https://doi.org/10.1001/jama.2020.3633 [ Links ]
24.Wax RS, Christian MD. Practical recommendations for critical care and anesthesiology teams caring for novel coronavirus (2019-nCoV) patients. Can J Anaesth. 2020. DOI: https://doi.org/10.1007/s12630-020-01591-x [ Links ]
25.Brewster DJ, Chrimes NC, Do T, Fraser K, Groombridge C, Higgs A, et al. Consensus statement: Safe Airway Society principles of airway management and tracheal intubation specific to the COVID-19 adult patient group. Med J Aust. 2020. [ Links ]
26.Ruan Q, Yang K, Wang W, Jiang L, Song J. Clinical predictors of mortality due to COVID-19 based on an analysis of data of 150 patients from Wuhan, China. Intensive Care Med. 2020. DOI: https://doi.org/10.1007/s00134-020-05991-x [ Links ]
27.Simonds AK, Hanak A, Chatwin M, Hall A, Parker KH, Siggers JH, Dickinson RJ. Evaluation of droplet dispersion during non-invasive ventilation, oxygen therapy, nebuliser treatment and chest physiotherapy in clinical practice: implications for management of pandemic influenza and other airborne infections. Health Technol Assess 2010;14(46):131-72. DOI: https://doi.org/10.3310/hta14460-02 [ Links ]
28.Chen C, Zhao B. Makeshift hospitals for COVID-19 patients: where health-care workers and patients need sufficientventilation for more protection. J Hosp Infect. 2020: S0195-6701(20)30107-9. DOI: https://doi.org/10.1016/j.jhin.2020.03.008 [ Links ]
29.Christian MD, Loutfy M, McDonald C, Martinez KF, Ofner M, Wong T, et al. Possible SARS coronavirus transmission during cardiopulmonary resuscitation. Emerg Infect Dis. 2004;10(2):287-93. DOI: https://doi.org/10.3201/eid1002.030700 [ Links ]
30.Yu IT, Xie ZH, Tsoi KK, Chiu YL, Lok SW, Tang XP, et al. Why did outbreaks of severe acute respiratory syndrome occur in some hospital wards but not in others? Clin Infect Dis. 2007;44(8):1017-25. DOI: https://doi.org/10.1086/512819 [ Links ]
31.Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA 2020. DOI: https://doi.org/10.1001/jama.2020.1585 [ Links ]
32.Hui DS, Chow BK, Lo T, Ng SS, Ko FW, Gin T, et al. Exhaled air dispersion during noninvasive ventilation via helmets and a total facemask. Chest. 2015;147(5):1336-43. DOI: https://doi.org/10.1378/chest.14-1934 [ Links ]
33.Yang X, Yu Y, Xu J, Shu H, Xia J, Liu H, et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study. Lancet Respir Med. 2020:S2213-2600(20)30079-5. DOI: https://doi.org/10.1016/S2213-2600(20)30079-5 [ Links ]
34.Guan L, Zhou L, Zhang J, Peng W, Chen R. More awareness is needed for severe acute respiratory syndrome coronavirus 2019 transmission through exhaled air during non-invasive respiratory support: experience from China. Eur Respir J. 2020;55(3): 2000352. DOI: https://doi.org/10.1183/13993003.00352-2020 [ Links ]
35.Lazzerri M, Lanza A, Bellini R, Bellofiori A, Cecchetto S, Colombo A, et al. Respiratory Physiotherapy in patients with COVID-19 infection in acute setting: a Position paper of the Italian Association of Respiratory Physiotherapists (ARIR). Monaldi Arch Chest Dis. 2020; 90(1). DOI: https://doi.org/10.4081/monaldi.2020.1285 [ Links ]
36.Airway management of COVID-19 patients with severe pneumonia. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2020 Feb 26;55(4):E001. DOI: https://doi.org/10.3760/cma.j.issn.1673-0860.2020.04.001 [ Links ]
37.Xie J, Tong Z, Guan X, Du B, Qiu H, Slutsky AS. Critical care crisis and some recommendations during the COVID-19 epidemic in China. Intensive Care Med. 2020. DOI: https://doi.org/10.1007/s00134-020-05979-7 [ Links ]
38.Alhazzani W, Møller MH, Arabi YM, Loeb M, Gong MN, Fan E, et al. Sepsis Campaign: Guidelines on the Management of Critically Ill Adults with Coronavirus Disease 2019 (COVID-19). Intensive Cara Med. 2020. DOI: https://doi.org/10.1007/s00134-020-06022-5 [ Links ]
 Correspondence:
Correspondence:
cassiofisio2@yahoo.com.br
Manuscript received: March 2020
Manuscript accepted: March 2020
Version of record online: March 2020
Recomendations and Evidence:Physiotherapy in COVID-19 respiratory and heart disability
Elaboration
Dr. Cássio Magalhães da Silva e Silva
Physiotherapist. PhD in Interactive Processes of Organs and Systems - FUBA. Master in Human Development and Social Responsibility - FVC. Federal University of Bahia -UFBA - Physiotherapy Department.
Adult Physiotherapy Commission
Dr. Balbino Nepomuceno
Physiotherapist. Master in Medicine and Health at UFBA, PhD in Interactive Processes of Organs and Systems at UFBA. Founding partner Reative Specialized Physiotherapy. Physiotherapist at Aliança Hospital. Prohope Hospital / GFH; Partner - Coordinator of Agnus Dei Hospital.
Dr. Daniel Salgado Xavier
Physiotherapist. Doctor "honorius causa" in Oncological Physiotherapy by Logos University - Florida / USA and in Intensive Care by the Brazilian Association of Intensive Care. Doctor in Intensive Care by the Brazilian Institute of Intensive Care - IBRATI / SP PHD - Philosophy and Doctor in Physiotherapy. Health Secretariat - AM.
Drª. Iura Gonzalez
Physiotherapist. Master in Health Sciences by UFS, Doctor in Health Sciences by UFS, Bahiana School of Medicine and Public Health, Bahia Social University Center, Maurício de Nassau University Center, member of the Physiotherapy Research Group at UFBA.
Drª. Juliana Costa dos Santos
Fisioterapeuta. Doutoranda e Mestre em Processos Interativos dos Órgãos e Sistemas - UFBA. Docente da Universidade Federal da Bahia e da Faculdade Bahiana de Medicina e Saúde Pública. Especialista Fisioterapia em Cardiologia
Dr. Mateus Souza Esquivel
Physiotherapist. Post-Graduation in Physiotherapy in Intensive Care. Partner-Coordinator of the GNAP Respiratory and Cardiovascular Physiotherapy Nucleus.
Dr. Robson da Silva Almeida
Physiotherapist. Master in Health Sciences (UESC-BA). Specialist in traumato-orthopedics and cardiorespiratory. Coordinator of the Lato Senso Postgraduate Course in Traumato-Hospital Physiotherapy at FMT.
Dr. Vinícius Afonso Gomes
Physiotherapist. Master in Medicine and Human Health by Escola Bahiana de Medicine and Public Health. Specialist in cardiovascular physiotherapy by COFFITO. Professor at UNIFACS, UNIRUY and substitute professor at UFBA.
Dr. Victor Oliveira Carvalho
Physiotherapist. Post-doctor in Medical School of USP. PhD in Cardiology from the Medical School of USP. Professor at the Physiotherapy Department at the Federal University of Sergipe. Professor of the Postgraduate Program in Health Sciences at the Federal University of Sergipe.
Dr. Wiron Correia Lima Filho
Physiotherapist. Specialist in Cardiorespiratory Physiotherapy. Scientific Coordinator of the Brazilian Physiotherapy Society.
Pediatric Physiotherapy Commission
Drª. Aline do Nascimento Andrade
Physiotherapist. Master in Interactive Processes of organs and systems - UFBA. Physiotherapist at Ana Nery Hospital.
Dr. Paulo Magalhães
Physiotherapist. Doctor of Maternal and Child Health; Professor Adjunct to the Physiotherapy course at the University of Pernambuco; Permanent professor of the Stricto Sensu Graduate Program in Rehabilitation and Functional Performance, PPGRDF; Leader of the research group in Neonatal and Pediatric Physiotherapy, Baby Group.
Drª. Michelli Christina Magalhães Novais
Physiotherapist. PhD student in the Postgraduate Program in Interactive Processes of the Organ and Systems of the Federal University of Bahia (UFBA); Professor at the Jorge Amado University Center. Member of the Physiotherapy Research Group at UFBA.
Drª. Eugenia Lima
Physiotherapist. Master in Interactive Processes for Organs and Systems; Professor Substitute at the Federal University of Bahia; Technical responsible for the Neonatal and Pediatric ICU of HTL-BA.
Scientific Reviewer:
Dr. Mansueto Gomes Neto
Physiotherapist. Master in Rehabilitation Sciences from the Federal University of Minas Gerais and PhD in Medicine and Health from the Federal University of Bahia. Adjunct Professor III of the Physiotherapy department and permanent professor of the Postgraduate Program in Medicine and Health and the Interactive Processes Program of the Organs and Systems at UFBA.
Dr. Oséas Florêncio de Moura Filho
Physiotherapist. Master in Intensive Care from the Brazilian Society of Intensive Care. President of the Brazilian Physiotherapy Society
Founded in 1998 in Fortaleza and having Dr. Vilalba Rita Colares Cruz Dourado as its first president, the Brazilian Physiotherapy Society (SBF) arose from the imperative will of a group of Brazilian Physiotherapists concerned with all the content of social, cultural and scientific demands of the profession .
SBF always in the forefront position SBF already in its embryonic phase debated themes such as Functional Kinesiological Diagnosis, Fee Reference, models of scientific development pertinent to the growth of Brazilian Physiotherapy, themes that would later become fundamental bases worldwide.
It is in this profile that the SBF has always raised two banners: clinical physiotherapy and full autonomy of the physiotherapist has supported all initiatives for the development of physiotherapy in Brazil. At this moment, as it could not be otherwise, we will propose in this paper a review based on evidence and recommendations from Physiotherapists specialized in the area of Respiratory Physiotherapy to propose recommendations on the Physiotherapist's performance in a hospital in the respiratory deficiencies caused by COVID-19.
We emphasize that this document should not be considered imperative, and adaptations must be made to the regional realities of Brazil associated with the contribution of the experience of other countries, in order to standardize decision making with a focus on mitigating preventable and treatable Acute Respiratory Deficiency events.
Considering the complexity and fragility of the affected patients, we recommend, whenever possible, consult Physiotherapists with experience and specialized training in Physiotherapy in highly complex patients and Respiratory Physiotherapy.
For the complexity and dimension of COVID 19 in the world since December 2019 and for the great commitment of the Unified Health System (SUS) in facing this new challenge. We physiotherapists professionals have gathered in this example some recommendations for the assessment, diagnosis and care of patients with Disabilities and or Limitation by COVID 19.
The term Disability and or Limitation was used extensively in this recommendation, as it is the Physiotherapeutic Diagnosis with a focus on changing a patient's function and activity respectively, based on the International Classification of Functionality, Disability and Health.
We incorporate and encourage the search for knowledge and evidence. This material contains science-based instruments for a better understanding of Brazilian and worldwide Physiotherapists in the construction of protocols and attention to the care of patients with COVID 19.
The pages of these recommendations were based on scientific evidence, expert opinion and peer-reviewed, in order to contribute in a simple way to the improvement of Physiotherapeutic care, mainly in its greatest aspect, which is the functional treatment of ventilation and oxygenation of patients.
ORGANIZATION
Brazilian Society of Physiotherapy (SBF)
Dr. Oséas Florêncio de Moura Filho - President of SBF
Dr. Luiz Jonas Marques Filho - Vice President of SBF
Dr. Wiron Correia Lima Filho - Scientific Coordinator of SBF
Dr. Karoline Ferreira - Regional Director
Dr. Adriano Sá Ferreira - Regional Director
Dr. Antônio Viana de Carvalho Júnior - Secretary Director
PREFACE
PRESENTATION
Corresponding author
Cássio Magalhães da Silva e Silva
https://orcid.org/0000-0002-9119-5418
Collegiate of Physiotherapy - Pavilhão de Aulas do Canela, room 106
Address: Avenida Reitor Miguel Calmon, 1105, Vale do Canela, Salvador - CEP: 40110 -902.
Email: cassiofisio2@yahoo.com.br
1. Physiotherapeutic Assessment and Diagnosis in Adult Patients with Respiratory Disabilities caused by COVID-19
Evidences: The epidemic of pneumonia due to infection with the new coronavirus (COVID-19) broke out in late December 2019, Wuhan, Hubei Province, China and spread rapidly across Brazil and the world. Discovered through entire genome sequencing, the pathogen was considered a new beta coronavirus genus, and the pathology was named new coronavirus pneumonia by the World Health Organization1-4.
Evidences: Comorbidities and chronic diseases, such as hypertension, diabetes and other deficiencies in the respiratory, cardiovascular and metabolic systems, can be risk factors for severe acute respiratory syndrome (SARS-CoV-2). The patients seem to have an average age of 47 years, 5% of which require admission to the ICU, 2.3% are submitted to invasive mechanical pulmonary ventilation (VPMI), and mortality around 1.4%.6,7.
PHYSIOTHERAPEUTIC EVALUATION
The evaluative aspects may be focused on the function changes caused by the clinical condition, so that, after this phase, provide the Physiotherapeutic Diagnosis as suggested in chart 1.
Recommendation 1: Ventilometry. CV, Vt and VE. CV is a variable that assesses the capacity to distend the thoracopulmonary system39,40. Values below 65 ml / kg indicate respiratory deficiency and less than 10 -15 ml / kg indicates severe respiratory deficiency. Vt is approximately 500ml or 7ml / kg of weight41,42.
Recommendation 2: Mechanical ventilator. Plateau pressure (Pplat) and Cst can be measured every 4 hours, after any change in Vt and positive end-expiratory pressure (PEEP), in the controlled volume mode12. Being Cst: 70-80 mL / cmH2O43 or 57-85 mL / cmH2O44.
Recommendation 3: In RT the structure presents consolidation, ground-glass lesion with peripheral distribution and lower zone bilaterally45. CT shows ground-glass opacity, interlobular septal consolidation and thickening46.
Recommendation 4: Monitoring pulse oximetry and arterial blood gases.
PaO2 \ FiO2 ratio, Oxygenation Index (IO) and SpO2 Saturation Index (IS) are preferred parameters for stratifying the severity of oxygenation in mechanically ventilated patients47.
IO= (FiO2 x Mean airway pressure x 100)/PaO2. IO ≥ 4 and < 8 (DR mild hypoxemic), IO ≥ 8 and < 16 (DR moderate hypoxemic), IO ≥ 16 (DR severe hypoxemic)47.
IS = (FiO2 x Mean airway pressure x 100) / SpO2. IS ≥ 5 and <7.5 (mild hypoxemic DR), IS ≥ 7.5 and <12.3 (moderate hypoxemic DR), IS ≥ 12.3 (severe hypoxemic DR)47.
PF = PaO2 \ FiO2. Mild hypoxemic DR 200 mmHg <PaO2 / FiO2 ≤ 300, Moderate 100 mmHg <PaO2 / FiO2 ≤200 mmHg and severe PaO2 / FiO2 ≤ 100 mmHg and PEEP 5 with PEEP 5 cmH2O48.
ROX index: Success indicator for high flow oxygen therapy, ROX index ≥ 9.2 is a predictor of success for high flow oxygen therapy49. ROX <3.85 received endotracheal intubation for invasive mechanical ventilation50.
Recommendation 5: Manovacuometry. The assessment of inspiratory muscle strength. Equation for predicted values in MIP men (cmH2O) = 155.3 - 0.80 (age) and MIP women (cmH2O) = 110.4 - 0.49 (age)51.
Recommendation 6: Peak Flow. Instrument for assessing proximal airway resistance and as an outcome for cough function. In normal cough, 2.3 ± 0.5 L of air are expelled at a flow rate of 360 to 1,200 L / min,52 160 L / min is the minimum required in adult patients to achieve effective cough53.
(*) ATTENTION: All quantitative assessment instruments are essential for the best functional understanding and diagnosis of patients; however, the use of these instruments must respect:
1) Control of the spread of the virus - A dialogue with the hospital infection control service is suggested.
2) The use of a barrier and bacteriostatic filter between the mask or the mouthpiece and the evaluation device.
3) The protection of the evaluation device to not be contaminated externally with droplets and aerosols.
4) Proper disinfection of the evaluation device after use with a suspected or confirmed patient of COVID-19.
5) Prefer using a mask for the evaluation and get it well adapted to the patient to avoid contamination.
Respiratory Physiotherapeutic interventions are potentially aerosol producers, therefore, Physiotherapists must promote the highest protection with personal protective equipment.
All assessment procedures must be discussed with the head of Physiotherapy for a more appropriate, safe and common-sense approach.
Recommendation 7: Step test. Evaluates cardiorespiratory and metabolic function during exercise to provide deficiency to exercise tolerance in addition to identifying the evolution of functionality and response to treatment54.
VO2máx ml.-1kg-1.min-1 = 0.2 x (stepping rhythm) + 1.33 x 1.8 x (step height in meters) x (stepping rhythm) + 3.554.
Recommendation 8: FSS - Functional Status Scale. This assessment of the activity of hospitalized patients created based on the contexts of Activities of Daily Living (ADL) and the ability to adapt behavior55. Total score is 35, we recommend using the International Classification of Functionality qualifier to define the severity level.
2. Physiotherapeutic Assessment and Diagnosis in Pediatric Patients with Respiratory Disabilities caused by COVID-19
Evidences: Epidemiological data showed a lower proportion of severe expression of COVID-19 in neonates and children, with rare cases of mortality. However, children with chronic lung diseases are the most likely to develop severe acute respiratory syndrome (SARS-CoV-2)56-58. The newest individual with COVID-19 was only 1 month old and the possibility of vertical transmission remains uncertain57-59.
PHYSIOTHERAPEUTIC EVALUATION
Recommendation 1: Evaluate the clinical and functional signs of COVID-19 Respiratory Deficiency: Temperature (common to fever), Cough (Common: Dry cough) and Respiratory rate with respiratory pattern (common to fatigue)60.
Recommendation 2: Investigate symptoms of Respiratory Deficiency due to upper airway infection: nasal congestion and runny nose60.
Recommendation 3: Investigate symptoms of Gastrointestinal Deficiency (uncommon), of which: nausea, vomiting, abdominal pain and diarrhea60.
Recommendation 4: Laboratory tests should be evaluated. Normal or reduced white blood cell count, elevated liver and muscle enzyme changes; high level of C-reactive protein, reduction of lymphocytes in the blood and smears in the throat, sputum, lower respiratory tract, secretions, feces and blood, etc. Positive for COVID-19 nucleic acids.
Recommendation 5: Evaluate the pulmonary structure by means of an image, as these patients may present images with a ground-glass pattern and pulmonary consolidation (severe and critical cases)16.
Evidences: Children with any of the symptoms listed below are considered a warning sign for hospitalization16,61,62,63:
- respiratory rate> 50 times / min for 2-12 months; > 40 times / min for 1-5 years; > 30 times / min in patients over 5 years (rule out the effects of fever and crying);
· persistent high fever for 3-5 days;
· lethargy or changes in the level of consciousness;
· hepatic cardiac enzymes, altered lactate;
· metabolic acidosis without a definite cause; chest image examination indicating infiltration, pleural effusion or rapid progression;
· extrapulmonary complications;
· infection associated with other viruses and / or bacteria.
Recommendation 6: If is suspected a COVID-19 contamination , both the child and his companion should receive a face mask and be placed in a separate area64.
Observation: The use of PPE must be mandatory for the team (mask, glove, protective glasses, cape), in addition to washing hands or using alcohol gel. Stethoscopes and thermometers should not be shared between patients.
PHYSIOTHERAPEUTIC DIAGNOSIS
Recommendation 1: For the diagnosis, the professional must pay attention to the following markers:
- Respiratory frequency (consider severe respiratory deficiency) - disregard effects produced by fever and crying:
· 50 ipm for 2-12 months;
· 40 ipm for 1-5 years old;
· 30 ipm for patients over 5 years.
· Peripheral oxygen saturation - (SpO2): between 92% to 97% - values below indicate hypoxia-like respiratory deficiency;
- Static and dynamic compliance, airway resistance - (indicate respiratory deficiency due to reduced compliance or impaired airway hygiene, respectively):
· RN: 5 ml/cm H2O ;
· 1 year old: 15 ml/cm H2O;
· 7 years old: 50 ml/cm H2O;
· Dynamic compliance: 10-20% less than static.
· Inspiratory and expiratory tidal volume - (Vt): 6 to 8ml / kg - values below indicate respiratory deficiency due to Vt reduction);
- Arterial blood gases: evaluation of PaO2 and PaCO2 (changes result in respiratory deficiency due to changes in gas exchange).
- Chest radiography and tomography (associate with pulmonary auscultation): respiratory failure due to alveolar collapse.
- Cough: It is not a parameter applicable to the entire population due to the wide variation in age and development of the respiratory muscular system, with greater assessable evidence of the inability to cough in neonates.
- Peak Flow: it is effort-dependent and therefore requires patient collaboration - not applicable to the entire population.
FINAL CONSIDERATIONS
There is a limitation of more accurate data on the pathophysiology of COVID-19 in children and neonates and researchers around the world are trying to understand the reasons that lead to relatively lower infection rates forthis population, when compared to adult individuals.
Another important aspect to consider is that the variability of weight and age for this population limits the standardization of assessment, so the age of each patient must be respected and adjustments must be made for each age group.
Younger children who cannot wear masks and more specific isolation measures must be taken. It should be discussed with the team of the Hospital Infection Control Commission (CCIH).
The physiotherapist professional must be equipped with PPE's suitable for the evaluation of the child and, on average, their performance can produce the spread of droplets and aerosols, and therefore must also provide the companion, when necessary, with appropriate PPE during the process.
The evaluation of the specialist is essential, since, through the respiratory functional diagnosis, the anticipation of care and early rehabilitation can lead to more favorable outcomes for this population.
3. Recommendations for Physiotherapeutic Management in Patients with Metabolic and Heart Disabilities caused by COVID-19
Evidences: The coronavirus responsible for COVID-19 can have repercussions that go beyond lung involvement, damaging several systems, including the cardiovascular system65. COVID-19 can get the heart function decompensated, especially in those with previous impairments, such as heart failure and coronary artery disease. In addition, studies indicate the occurrence of acute myocarditis and severe acute respiratory syndrome (SARS-CoV-2), which favors systolic dysfunction and myocardial infarction9,65.
Evidences: In a retrospective multicenter study, 33% of deaths from COVID-19 showed a joint association between heart failure and respiratory failure, with 7% of deaths being precipitated by isolated myocardial injury26. In this same study, the presence of myocardial infiltration by interstitial mononuclear inflammatory cells was observed at autopsy, demonstrating the direct impact of the coronavirus on the myocardium14.
Evidences: In its severe presentation, COVID-19 can present several cardiovascular repercussions, making continuous monitoring and a multidisciplinary approach necessary in the care of this patient13. It is known that the integrity of aerobic physical performance is also associated with the integrity of the cardiovascular system. In addition, the physical weakness and the consequent disuse of the peripheral musculature means that the survivors of COVID-19 may present some impairment in physical performance. However, there is still no scientific data to support this scenario in COVID-19.
Recommendation 1: Among the various professionals involved in the physical recovery of patients with COVID-19, the role of the physiotherapist stands out, not for treating the disease but for preventing and rehabilitating the deficiencies and functional limitations caused by it66.
Recommendation 2: The physiotherapist must follow the main global recommendations for physical exercise in heart failure, from the perspective of the impacts caused by COVID-19 / SARS-CoV-2.
Recommendation 3: Physical exercise is contraindicated in cardiac deficiencies caused by myocarditis, myocardial infarction (before 24 to 48 hours), acute systemic infection, dyspnoea at rest, hypotension and severe complex ventricular arrhythmias67. In these cases, continuous respiratory monitoring and bed rest with an elevated headboard, passive mobilizations and biomechanical positioning in the bed with controlled energy expenditure are recommended67,68.
Recommendation 4: Before starting treatment, the physiotherapist must observe the reduction in serum levels of biochemical markers of cardiac injury such as CK-MB, myoglobin and troponins; in addition to certifying the absence of precordialgia and infra / supra unevenness of ST follow-up on the electrocardiogram69.
It should also be noted whether there are signs of improvement in the thickness of the cardiac wall and in the ejection fraction seen on transthoracic echocardiography, especially in cases of acute myocarditis68,67,70, as a form of cardiac functional evolution under the conditions described in recommendation26. The stability of the cardiovascular condition and beginning of exercises should always be discussed with the multiprofessional team.
Recommendation 5: The physiotherapist must pay attention to safety criteria70 to be observed before performing physical exercises on the critical patient. It is essential to observe the signs and symptoms of intolerance to effort by the physiotherapist and the patient, observation of the security and mobilization instruments is recommended71.
Recommendation 6: When performing exercises in patients with heart failure secondary to COVID-19, attention should be paid to the Frequency, Intensity, Type (or modality), Time (or duration) - Volume and Progression (FITT-VP) of the American College of Sports Medicine (ACMS), for post- infarction patients72.
Recommendation 7: The FREQUENCY of mobilization can be between 2 to 4 times a day for the first 3 days of hospitalization, with INTENSITY guided by the BORG effort subjective perception scale, not exceeding 13 (in the 6 to 20 scale) and the frequency heart rate, which should not exceed 20 beats per minute in relation to rest. Another important criterion to be considered is the use of exercises that require energy expenditure < 3 MET´s72. The exercise time can vary between 3 to 5 minutes, progressing according to tolerability; in TYPE, bed exercises that should evolve to walk according to the individuality of each patient. PROGRESSION must be performed when the duration reaches 10 to 15 minutes, as recommended by the heart rate and always taking into account the subjective perception of effort72.
Recommendation 8: As there are no studies available on rehabilitation in individuals with COVID-19, we suggest taking into account the routine and consistent protocols reported in the literature.
4. Recommendations for Physiotherapeutic Management in Patients with Respiratory Disabilities caused by COVID-19
Evidences: Patients with suspected or confirmed COVID-19 may have exudative consolidation, mucous hypersecretion and / or difficulty in clearing secretions20, and also present:
· Wet voice/wet speech20;
· SpO2 <90% with supplemental oxygen therapy at 5l / min20.
Recommendation 1: Secretion Removal Techniques (TRM) can be performed to ensure hygienic conditions and prevent contagion, and compliance with individual protection rules is essential20.
Recommendation 2: Directed cough20,73 should be performed in an isolated room with negative pressure, if the service does not have this isolation, a surgical marker should be used. The aim is to prevent secretion build-up and reduce ventilatory discomfort20,73.
Recommendation 3: Oscillating Positive Expiratory Pressure20 can be used in cooperative patients, with availability of the service and understanding of the tool by the patien73. The aim is to facilitate the removal of secretion and unblock the airways74,75.
Note: Most of the patients affected with COVID-19 do not have a productive cough or radiological alteration and have the ability to expectorate without assistance20.
EARLY MOBILIZATION
Evidences: In the ICU, severe muscle weakness is independently associated with prolonged mechanical ventilation, increased ICU stay, hospital stay and increased mortality76, with consequent decrease in quality of life and increase in mortality within 1 year after discharge from the ICU77. One of the factors favorable to the implementation of a systematic physical therapy intervention in patients with COVID -19, lies in the fact that intensive management, including prolonged mechanical ventilation, sedation and use of neuromuscular blockers, will significantly increase the risk of developing acquired muscle weakness in the ICU.
Recommendation 4: Exercises, mobilization and interventions for patients with Muscular Disabilities associated with COVID-19, in order to enable a functional return to the home. Therefore, it is essential to anticipate early physical therapy after the acute phase for rapid functional recovery76.
Recommendation 5: The physiotherapist should consider the complexity of the condition and understand that with the appearance of generalized muscle weakness, functionality will certainly be compromised depending on the greater or lesser degree of this condition, which should be measured quantitatively using recognized and validated assessment methods.
Recommendation 6: Muscle strength assessed according to the Medical Research Council (MRC)78 criteria (table 2) a total score below 48/60 designates FAUTI or significant weakness, and a total MRC score below 36/48 indicates severe weakness (table 3)79.
Recommendation 7: Dynamometry measures isometric muscle strength and can be used as a quick diagnostic test. The cut-off scores are: less than 11kg (IQR 10 - 40) in men and less than 7kg (IQR zero to 7.3) in women, which were considered indicative of ICUAW80.
The evaluation by the MRC scale and dynamometry are indicated for the conscious, cooperative and motivated patient81.
Evidences: Functional assessment is the basic and first element of any Physiotherapy program aimed at optimizing therapeutic interventions81. Currently we have several scales that quantify and qualify the functional status, it is imperative to respect the specificity of each unit.
· Physical Function in Intensive care Test scored (PFIT-s);
· Functional Status Score for the ICU (FSS-ICU);
· Surgical Intensive Care Unit Optimal Mobilization Score (SOMS);
· Chelsea Critical Care Physical Assessment Tool (CPAx);
· Intensive Care Unit Mobility Scale (IMS);
· Perme Intensive Care Unit Mobility Score (Perme Score);
· Manchester Mobility Scale (MMS).
Recommendation 8: Avoid using more generic scales that do not meet the specificities of the patient admitted to the ICU with Functional Disability.
Recommendation 9: Transfer sitting to standing. With the patient in the armchair, the need for help by one or two people is evaluated for him to stand up, the scores are from 0 to 3 (where 0 = does not perform the task even with the help of two people and 3 = performs the task). task without help).
Recommendation 10: Walking cadence. Maximum number of steps possible without time limit. The cadence values are evaluated from 0 to 3 (0 = no steps and 3 = over 80 steps / min).
Recommendation 11: Strength of knee extensors and shoulder flexors. In this stage, the Oxford scale is used to measure the degree of strength that goes from 0 to 5 (with 0 = no strength and 5 = normal muscle strength).
Recommendation 12: AAfter the evaluation, these values are added and there is a score of 0 to 12 or 0 to 10 (on the modified scale), where the lower the scores, the less function the patient has, or the more dependent he is and how much the greater the value of these scores, the greater the degree of functionality or independence we recommend using the international classification of functionality qualifier82 to define the severity level.W
Recommendation 13: All safety criteria and clinical status of the patient must be observed and the hemodynamic and respiratory organic reserves must be calculated before the prescription of the therapeutic intervention.
Recommendation 14: Use of FITT-VP as a reference for physical activity.
· F - Frequency in times per day, per week.
· I - Intensity between mild, moderate or severe activity, depending on some indicators, such as respiratory rate, heart rate and perceived effort.
· T - Duration time, as well as rest time between sets.
· T - Type or modality chosen: aerobic, muscular endurance, muscular strength or exclusively functional exercises.
· V - Volume: number of sessions or repetitions, intensity, type of exercise and time of rest between sets (total caloric expenditure in a given time).
· P - Progression, optimizing, in this way ,the gains obtained.
Recommendation 15: We recommend the use of Denehy83 protocol (table 4). This protocol is based on the PFIT scale, serving as a basis for the prescription of the Physiotherapy session.
Note: The use of this series of exercises scaled according to the patient's capacity can be used in any hospital environment. The formal indication is that the progression of this activity or protocol mentioned above reaches up to 60 minutes of execution, based on the criteria of FITT-VP. The therapeutic objective should always include the individual's functionality considering the DNPMN (functional neuropsychomotor development) in our therapy.
Recommendation 16: Perform progressive activities (table 5) and aiming at functionality. Representing the main functional activities based on the DNPMN and which should be included in any protocol adopted for early mobilization in patients with COVID-19.

Evidences: In children with COVID-19, symptoms are generally less severe than adults and are mainly with cough, fever, pharyngeal erythema and more rare, diarrhea, fatigue, rhinorrhea, vomiting and nasal congestion85.
Evidences: Few cases have been reported of babies confirmed with COVID-19 and have experienced mild illness16.
Evidences: 5% of children develop severe and critical symptoms that require hospitalization and intensive care11,33,86,87.
Evidences: Children are classified as severe pneumonia when they have:
· Increased respiratory rate: ≥ 70 i.p.m. (<1 year) and ≥ 50 i.p.m. (≥ 1 year) (after discarding the effects of fever and crying);
· Drop in Oxygen Saturation <92%;
· Increased ventilatory work with cyanosis and intermittent apnea;
· Disorders of consciousness: drowsiness, coma;
· Refusal of food or feeding difficulties, with signs of dehydration16.
Note: Respiratory failure that requires mechanical ventilation; shock; and / or failure of other organs fall into the Critical Cases class16.
Recommendation 1: The physiotherapist must act in order to identify, elaborate and develop a physiotherapeutic diagnosis in the deficiencies of the cardiorespiratory and musculoskeletal system caused by viral infection, through anamnesis, physical evaluation and complementary exams.
POSSIBLE REPERCUSSIONS OF COVID-19 IN PEDIATRICS, FROM THE PERSPECTIVE OF CIF MULTIFACTORIAL CONTEXT·
· COVID-19 is a disease that causes deficiency of respiratory tract structures, leading to impaired breathing functions11, such as respiratory rate, respiratory rate and depth of breathing.
· Not only, depending on the clinical severity presented, there may be impaired respiratory muscle function and exercise tolerance.
· Limitations, which make it difficult to carry out basic activities that involve the ability to move, affecting even routine tasks such as walking and performing self transfers.
· The control of the spread of infection leads to the restriction of participation, interfering with tasks such as recreation and leisure activities12.
Figure 1 shows some possible repercussions of COVID-19 in pediatrics, from the perspective of the ICF multifactorial context:
OVID-19 INFECTION PREVENTION STRATEGIES
Evidences: Children with COVID-19, even if asymptomatic, must remain in social isolation, an essential measure to prevent the spread of the virus88.
Recommendation 2: To prevent and control the spread of COVID-19, the following measures are recommended: wash your hands frequently with soap and water for at least 20 seconds; if there is no soap and water, use a hand sanitizer (which is 60% or more alcohol-based); keep children away from other sick people or keep them at home if they are sick; teach children to cough and sneeze on a tissue (make sure to throw it away after each use) or teach to cough and sneeze on the arm or elbow, not the hands; clean and disinfect the house as usual, using regular household sprays or cleaning cloths; avoid touching the face; teaching children to do the same; face masks only for people with COVID-19 symptoms, not for healthy people88.
PHYSIOTHERAPEUTIC TREATMENT IN MUSCULOSKELETAL SYSTEM DEFICIENCIES CAUSED BY COVID-19
Evidences: Immobilization can lead to respiratory deficiencies such as hypoventilation and cardiorespiratory deconditioning89.
Recommendation 3: Exercise and early mobilization are part of the Society of Critical Care Medicine Bundle, which aims to improve the quality of care provided to critically ill patients90.
Evidences: Early mobilization can reduce the time of mechanical ventilation and hospitalization89.
Recommendation4: Kinesiotherapy physiotherapy can be performed by virtual reality, promoting playful and attractive exercise for children, as long as attention is paid to the dissemination prevention measures87,88.
Recommendation 5: Progressive mobilization protocols can be adopted, based on conducts that encourage the maintenance of functionality89.
PHYSIOTHERAPEUTIC TREATMENT OF THE IMPAIRED RESPIRATORY SYSTEM CAUSED BY COVID-19
Secretion Removal Therapy
Evidences: According to the clinical classification for pediatric COVID-19, children with upper airway infection have nasal congestion16.
Recommendation 6: In conditions of nasal congestion and upper airway obstruction, secretion removal techniques (TRM) should be applied. Attention should be paid to the specific indications and contraindications, to the different ways of performing the techniques according to the age group91,92 and the use of PPE.
Figure 1: Possible repercussions of COVID-19 in pediatrics, from the perspective of the multifactorial context of the International Classification of Functionality, Disability and Health (CIF)82.
Flowchart: prepared by the authors based on the reference. CIF: International Classification of Functionality, Disability and Health. São Paulo: Edusp; 200382.
5. Recommendations for Physiotherapeutic Management in Pediatric Patients with Respiratory Disabilities caused by COVID-19
OXYGEN THERAPY AND NON-INVASIVE PULMONARY MECHANICAL VENTILATION
Recommendation 7: Retrograde rhinopharyngeal clearance (DRR) can be used to remove upper airway secretion.
Evidences: Children with COVID-19 with Severe Pneumonia (class 4) are suffering from Respiratory Deficiency, have hypoxemia and other symptoms16.
Recommendation 8: For class 4, TEM which require less energy expenditure, priority should be given to this, the use of the Thoracoabdominal Rebalancing (RTA) method seems to be advantageous91.
Evidences: The critical presentation (class 5) of the children's COVID-19 is characterized by respiratory failure with the need for ventilatory support16.
Recommendation 9: In critical conditions it is advisable to opt for secretion mobilization techniques that do not require the disconnection of the artificial airway, such as techniques for increasing tidal volume without disconnecting the ventilator, avoiding the release of aerosols and depressurizing the system.
Recommendation 10: To prevent the spread of the virus, the use of a closed suction system is indicated93, and this procedure should only be chosen to increase exergaming94 and virtual reality, promoting playful and attractive exercise for children, as long as attention is paid to measures to prevent dissemination87,88.
Evidences: It is important to highlight that most physical therapy interventions, especially with regard to MRI, have the potential to form aerosols24 and risk of contamination at work.
Recommendation 11: The choice of TRM must be evaluated on the real need for application, the procedures must be carried out with the appropriate personal protective equipment, and preferably in an environment with negative pressure respiratory isolation (IRPN)24,93. If the environment does not have IRPN, TRM should be performed with a closed door with the least possible circulation of professionals24.
Evidences: It is known that the newborn, under physiological conditions, has predominantly nasal breathing95. Obstructions in the upper airways cause rapid and progressive respiratory discomfort, manifesting with nose wing beats (BAN), chest runs and chest retractions that increase energy demand.
Evidences: Children affected by Respiratory Deficiency may have low levels of oxygenation, in this sense the continuous monitoring of peripheral oxygen saturation (SpO2) as a severity marker in this population is essential for the indication and administration of supplemental O234,96.
Recommendation 12: SpO2 should be maintained ≥ 90% in pediatric patients with Respiratory Deficiency due to previous Lung Diseases and ≥ 94% for those who do not have it.
Recommendation 13: The administration of supplemental oxygen should be offered preferably by a low- flow O2 catheter or low-flow mask with a reservoir when the child shows signs of respiratory distress and a drop in arterial O2 pressure (PaO2)30,97. (Table 6)
Evidences: Noninvasive mechanical pulmonary ventilation (NPMVP) is a resource frequently used in cases of hypoxemia and / or hypercapnia, and the subgroup of patients that seems to benefit most from NIPVM is that in which the PaO2 / FiO2 ratio (ratio between partial pressure of arterial blood oxygen and inspired oxygen fraction) is greater than 200 mmHg98.
Recommendation 14: VPMNI can be applied to normalize breathing and reduces the need for intubation, but it also significantly reduces the need for high doses of oxygen to achieve a normal level of oxygenation97,98.
Note: In order for VPMNI to be performed on children with COVID-19, it is necessary to guarantee the sealing of the interface during its application to avoid spraying the virus.
INVASIVE MECHANICAL PULMONARY VENTILATION
Figure 2 shows signs for the recognition of respiratory distress that are some of the indicators of the need for endotracheal intubation and invasive mechanical pulmonary ventilation (VPMI) for children with severe acute respiratory syndrome (SARS-CoV-2), as well as a suggestion for adjustments initial ventilation.
Source: Flowchart prepared by the authors based on the references: Pediatric Acute Lung Injury Consensus Conference Group. Pediatric acute respiratory distress syndrome: consensus recommendations from the Pediatric Acute Lung Injury Consensus Conference[J]. Pediatr Crit Care Med, 2015, 16(5): 428-439. Marraro GA, Spada C. Consideration of the Respiratory Support Strategy of Severe Acute Respiratory Failure Caused by SARS-CoV-2 Infection in Children. Zhongguo Dang Dai Er Ke Za Zhi. 2020 Mar;22(3):183-194.
THERAPEUTIC POSITIONING
Evidences: The prone position reduces the number of areas with Respiratory Deficiency due to Pulmonary Collapse in the dependent lung, promoting a homogenization of the pleural pressure gradient. This position can reduce the risk of barotrauma related to the need to apply manual recruitment maneuvers or increase the tidal volume to improve ventilation100.
Recommendation 15: It is suggested that children be positioned no more than 1-2 hours, three or four times a day since the start of VPMI. While the 12-hour duration of the prone position is suggested for the consolidated dependent lung areas of the patient treated for several days with invasive ventilatory support97.
Evidences: This intervention, according to the Pediatric Acute Lung Injury Consensus Conference (PALLIC), should not be used routinely, in all children with Respiratory Deficiency due to ARDS99. Thus, the prone position is perhaps a method of choice most suitable for the most serious cases of children with SARS-Cov-2.
VENTILATORY WEANING IN CHILDREN WITH SARS-COV-2
Evidences: When consulting the main literary databases (PUBMED, PEdro, SciELO...), the authors found no evidence about specific procedures and protocols for the weaning of children and babies with SARS-CoV-2.
Recommendation 16: Extubation should be brought forward as soon as the patient returns to a stable state and the initial resolution of Respiratory Deficiency due to Lung Disease, to avoid the deleterious effects of IMPV97.
Recommendation 17: If there is any doubt about the success of ventilatory weaning, it is suggested to keep the infant intubated to avoid the risk of reintubation.
Recommendation 18: Ventilatory weaning protocols should be strengthened, and include:
· Definition of weaning criteria;
· Reduction of ventilatory, sedative and control parameters;
· Interventions that favor weaning and extubation;
· Use of predictive indexes of weaning, including mechanics and lung volume according to the age group.
6. Oxygen therapy in Adults with Respiratory Disabilities due to COVID-19
Evidences: The use of oxygen therapy is an independent factor for increasing the chance of coronavirus spread101.
Recommendation 1: Aerosol-generating procedures should be avoided whenever possible, given the risk of contamination of the environment and staff.
Evidences: Hypoxemia is a frequent sign in patients with symptomatic symptoms102. In a recent Chinese study, two scores related to SpO2 and supplemental oxygen were proposed, reinforcing the importance of these data in patients with COVID-19103.
Recommendation 2: Patient on spontaneous ventilation with or without supplemental O2, isolated analysis of arterial oxygen pressure (PaO2), demands that the reference value be corrected for age. Corrected PaO2 = 109 (age x 0.43)104 with suggested use for this specific population102.
Evidences: In VPM, monitoring the PaO2 / FiO2 ratio is a usual severity marker105. In conditions where the PaO2 marker is not available, it is possible to use the SpO2 / FiO2 marker instead, with a cutoff ≤ 315, to suggest Respiratory Deficiency due to ARDS2.
Recommendation 3: All hospital units that assist the patient with COVID-19 must be equipped with at least pulse oximetry. As well as, disposable oxygen therapy systems must be available, such as: nasal cannula, nasal catheters, simple face mask and mask with reservoir bag.
Evidences: About 41% of all patients hospitalized with COVID-19 use oxygen therapy in the course of their treatment, this number rises to 70% among cases with very severe evolution18. In the SARS-COVID pandemic in 2002, O2 flow rates> 6L / min was a marker of increased outbreak risk. Adoption of high O2 rates increased the chance of a viral outbreak by 2.42 times compared to low flow adoption21,30.
Recommendation 4: The adoption of high oxygen flows should be discouraged in the absence of the respiratory isolation bed21,30.
Evidences: Hypoxemia in acute conditions, SpO2 ≤92%, may favor the dysfunction of organs and systems19. The excess supplemental oxygen causes complications such as respiratory system deficiency due to pulmonary absorption collapse and inflammatory cytokine production.
Recommendation 5: In patients with COVID-19, we suggest that supplemental oxygen be offered if SpO2 is less than ≤ 92%. On the other hand, we advise against patients with acute hypoxemic respiratory failure being treated with oxygen support for SpO2> 96%. The reasoning applies to the various O2 delivery devices.
Recommendation 6: The high flow nasal catheter (CNAF) can be used in severe hypoxemic insufficiency as long as it presents a potential response in oxygenation in the first 30 minutes of therapy30. Should limit the CNAF flow rate to levels not exceeding 30L / min to reduce the potential for viral transmission20.
Recommendation 7: The use of CNAF should preferably be used with patients in beds with a negative pressure room and with the use of individual protective equipment19,20.
Evidences: To date, the literature does not provide a basis to support the routine use of CNAF for the treatment of patients with COVID-19. The potential risk of aerosol dispersion is not practicable in the current state of the art.
Recommendation 8: Adults in emergency conditions such as: severe hypoventilation or respiratory arrest; severe dyspnoea; central cyanosis; circulatory shock; coma; convulsions. They must receive maneuvers to release the airways and oxygen therapy, start flow with oxygen at 5 L / min and titrate flow rates to reach the target SpO2 93%, during resuscitation. For children the target SpO2 is ≥94% during such procedure102.
Recommendation 9: The use of the mask-balloon resuscitator must have oxygen therapy guided by a SpO2 target ≥94%, with a flow rate starting at 5L / min, with rational titration aiming at providing adequate oxygenation of the patient, as well as minimizing the formation of aerosol during emergency procedures.
7. Noninvasive Mechanical Pulmonary Ventilation in Adults with Respiratory Disabilities caused by COVID-19
Evidences: Non-invasive positive pressure ventilation (NIPPV) can I increase contamination of healthcare workers106, even when applied by helmet(Helmet)107 with double branch circuit, filters and good sealing at the neck-helmet interface, as the jet of exhaled air can reach 92cm107 in distance. Additionally, the inappropriate application of NIPPV may delay the intubation process, and contribute to increased mortality109.
Evidences: NIPPV is associated with the absence of proven benefits in refractory hypoxemic respiratory deficiency28, in previous epidemics (H1N1 e MERS- COV)110,111, as well as in acute respiratory deficiencies secondary to acute respiratory distress syndrome (ARDS)112.
Evidences: COVID-19 shows that 14% of patients developed dyspnea, tachypnea, peripheral oxygen desaturation (SpO2) less than or equal to 93%, and deficient oxygenation index with a PaO2 / FiO2 ratio < 300 mmHg and / or SaO2 / FiO2 lower or equal to 315, in 48hrs113.
Evidences: NIPPV through an endotracheal tube is common in the midst of this outbreak, improving the clinical outcome114.
Evidences: The risk of transmitting acute respiratory infections to healthcare professionals, in procedures that generate aerosol, are three times higher during the use of NIPPV101.
Recommendation 1: Patients who benefit best from NIPPV are those in which the PaO2 / FiO2 ratio is greater than 200 mmHg98, despite the diagnosis of ARDS being associated with ineffective NIPPV115. However, the risk of spreading COVID-19 is greater, and therefore PPE is needed.
Recommendation 2: NIPPV can be used in those places where access to NIPPV is limited, or before patients have severe hypoxemic respiratory failure23. In this sense, the physiotherapist must ensure to perform any Physiotherapeutic conduct that:
1 - The procedures that generate aerosols are performed in a room with adequate ventilation (natural ventilation with an air flow of at least 160 L / s per patient)116 or in negative pressure rooms117;
2 - NIPPV procedures should be performed with PPE, such as professional mask PPE2 (N95), goggles for protecting the eye mucosa, long-sleeved, fluid-resistant apron, and clean gloves for protection21;
Recommendation 3: In specific situations, defined by the multiprofessional team, a response test to NIPPV, lasting "60 minutes" (we recommend up to 30 minutes), can be performed in patients with Respiratory System Deficiency by Hypoxemia who have mild respiratory distress (with a higher PaO2 / FiO2 ratio or equal to 200), immunosuppression present or cardiovascular problems118.
Recommendation 4: Avoid masks with ventilation holes, and add a filter between the mask and the ventilation valve to reduce viral transmission119.
Recommendation 5: The best option is to combine NIPPV with a dual circuit with an expiratory valve, combining a single circuit face mask with an integrated exhalation port instead of using ventilated masks120.
Recommendation 6: Antimicrobial and antiviral filters should always be installed27. Although some studies recommend changing filters every 48-72h, or before that, in cases of obstruction (water, blood or secretions), manufacturers recommend changing them every 24h to reduce infections121,122,123.
Recommendation 7: The helmet interface must be used with a double limb circuit to reduce the risk of airborne transmission32.
Recommendation 8: Dialogue with the team for endotracheal intubation if there is no response to NIPPV124.
Recommendation 9: For patients with suspected COVID-19 infection who receive long-term respiratory support at home (for example, patients with respiratory impairment due to chronic airflow obstruction), they should stay in a single, well-ventilated room to avoid the possibility of infecting their relatives125, and every care must be taken with respect to PPE.
Recommendation 10: In specific situations, in which there is an isolation room31, mask without rebreathing, negative pressure room, double circuit and barrier filter in the exhalation branch, a quick test can be performed if SpO2 < 93% and / or respiratory frequency (RF) > 24 ipm, already with oxygen therapy87.
Recommendation 11: The NIPPV pressures should be as low as possible to provide and provides a reduction in RF and the use of accessory muscles, with an improvement in SpO234, keeping it around 93%.
8. Invasive Mechanical Pulmonary Ventilation in Adults with Respiratory Disabilities caused by COVID-19: From Intubation to Weaning
Evidences: Patients with COVID-19 may have Respiratory Deficiency due to severe pneumonia, acute respiratory distress syndrome (ARDS), sepsis and septic shock102,126 and present hypoxemic acute respiratory failure or failure (SARS-CoV2 - severe acute respiratory syndrome caused by CoV2), requiring admission to the ICU in order to be addressed with ventilatory strategies24,31,126. Thus, the need for intubation and invasive mechanical pulmonary ventilation (VPMI) is common in the midst of this outbreak22 mainly due to the variation of 2.3% to 4%,7,87 and even higher values like, 42% and 47%31,126 in related studies.
OROTRACHEAL INTUBATION (IOT)
Evidences: Intubation and invasive mechanical ventilation may have been delayed in some patients and this may have had a negative impact on mortality22,127.
Recommendation 1: All patients in cardiopulmonary arrest (CRP) or with several non- pervious areas should be intubated. In other patients, the decision for IOT should be made based on the patient's functional assessment and clinical experience22, considering early intervention.
Recommendation 2: Intubation should be performed as soon as the patient has tachypnea (> 30 ipm), hypoxemia, Spo2 less than 93% in room air and a PaO2 / FiO2 ratio < 300 mmHg22. Also consider Orotracheal intubation in cases of progressive worsening of the clinical picture with no prospect of acute recovery, with no clinical and functional improvement to conventional oxygen therapy or high flow oxygen therapy or : Non-invasive positive pressure ventilation (NIPPV) in use within 1-2 hours20,22,35,73.
Recommendation 3: You need to be aware of the physiological signs of asymptomatic hypoxic patients referred to as silent hypoxemia37, to consider the need for intubation, avoiding an emergency procedure, as this poses a risk of cross-infection.
Evidences: It should be noted that, until now, for COVID-19, there is no scientific evidence to recommend one method over the other with regard to pre-oxygenation, and that the clinical guidelines and consensus disagree on these aspects25,128. The use of a mask valve bag (AMBÚ, or similar brand) is still questioned before intubation for pre-oxygenation due to the risk of generating aerosols and suggest that this method be avoided128.
Recommendation 4: Satisfactory pre-oxygenation must be performed before intubation, as already pointed out by guidelines and previous studies, in other health conditions129,130,131. A minimum of 5 minutes is recommended25.
Recommendation 5: The reservoir mask is not recommended for patients diagnosed with COVID-19 due to the risk of contamination25 should use an occlusive face mask (well adjusted to the patient's face) coupled to a mask valve bag (AMBÚ, or similar brand), connected to an oxygen source128.
Recommendation 6: The filter must be connected to the mask valve bag (between the mask or the endotracheal tube and the AMBÚ)25.
Recommendation 7: If the mask valve bag is used (most common in our country), a filter MUST be present. It is important to consider the use of AMBÚ if the pre-oxygenation method chosen by the team does not effectively improve the patient's oxygenation22.
Recommendation 8: Personal Protective Equipment (PPE) can prevent auscultation to help confirm correct tube placement25,132. In this sense, it is recommended132 a careful inspection of the bilateral movement of the chest, until the radiographic examination is performed (portable X-ray), since the use of PPE, at this moment, is essential22.
Recommendation 9: Capnometry, SpO2, skin color inspection, and clinical and functional assessment are useful for assessing successful intubation22.
Recommendation 10: The cuff cuff pressure must be maintained between 25 to 30 cmH2O (1 cmH2O = 0.098 kPa)17,35,73 and the cuffometer pressure gauge can be used routinely (every 6 to 8 hours)17.
VENTILATING THE PATIENT
Evidences: With attention focused mainly on increasing the number of beds and ventilators, an approach to patients similar to that used in severe ARDS has been used, that is, high expiratory pressure (PEEP) and prone positioning133. However, patients with respiratory failure caused by 2019-nCOV2, who are diagnosed based on the Berlin criteria for ARDS, may have an atypical form of the syndrome133. In fact, the main characteristics observed are the dissociation between relatively well preserved pulmonary mechanics and the severity of hypoxemia133.
Recommendation 11: Use the protective ventilatory strategy with a maximum tidal volume of 6 ml / Kg of predicted weight, plateau pressure limited to 28 - 30 cmH2O, driving pressure limited to 15 cmH2O, and target saturation of 88 to 93%. Hypercapnia must be tolerated (permissive hypercapnia), as well as acidosis (pH ≥ 7,20)7,17,21,24,134.
Recommendation 12: PEEP should be used in order to reduce driving pressure levels, as this parameter predicts mortality in RD due to ARDS135. Elevated PEEP in a poorly recruitable lung tends to result in severe hemodynamic impairment and fluid retention133. It should be noted that this should be individualized and should be titled based on clinical and functional evaluation, considering that atypical ARDS can be observed133.
Recommendation 13: The ventilatory modes most used in the studies are the conventional ones (PCV and VCV)22. The more contemporary modes, (such as double control), may be a possibility, but there is no scientific information about their use in COVID-19 patients.
Recommendation 14: AVOID disconnections of ventilator patients, as this results in air contamination (aerosols), loss of pressurization (PEEP) and can cause Respiratory System Deficiency due to collapse102.
Recommendation 15: Orotracheal tube clamping with straight Reynold or Kelly forceps should be performed when disconnection is necessary (for example to change the mechanical ventilator, change the Heat-moisture exchanger (HME) / High Efficiency Particulate Arrestance (HEPA) / HMEF, change the closed suction system)102.
Recommendation 16: All gas exhaled from the ventilator must be filtered in order to avoid air contamination and the spread of COVID-19. Therefore, it is recommended that the heat and humidity exchanger, HME (be used between the orotracheal tube and the combined circuit with HEPA (High Efficiency Particulate Arrestance), which must be placed between the circuit and the fan , in the expiratory branch. HMEF (with filtration efficiency greater than 99.9%) can replace the HME + HEPA combination, and must be placed between the tube and the circuit17. Do not use a heated humidification system (HH - heated humidification)17.
Recommendation 17: Regarding the use of VPMI equipment to ventilate two patients (Dual-Patient Ventilation), although there are already practical manuals for carrying out emergency cases, data on the effectiveness and / or losses of this strategy are not available.
VENTILATORY WEANING
Recommendation 18: Pressure support ventilation (PSV) mode is recommended for the implementation of a spontaneous breathing test (TRE). It is not recommended to use the T-piece to do the TRE17.
Recommendation 19: Using a T-piece or tracheostomy mask17.
Recommendation 20: Weaning protocols should be implemented, as well as, when possible, a sedation reduction protocol (daily awakening)102.
Recommendation 21: For extubation, the same precautions as intubation must be considered. You should be thinking about using appropriate sedation to avoid coughing and agitation22,136.
SPECIAL SITUATIONS
Evidences: In the patient infected with COVID-19, the need for resuscitation requires what the authors call ''Protected Code Blue'', a term created to distinguish the usual resuscitation from that which requires special procedures128,137.
Recommendation 22: Resuscitation should take place in an air isolation room, given the need for aerosol- generating procedures, staff should be kept to a minimum, and PPE must be used29.
Recommendation 23: It is suggested that the resuscitation cart be replaced by a cart containing the necessary devices, due to the difficulty of posterior cleaning29. Pay attention to the use of AMBU, it should be used with a filter17.
Recommendation 24: Transport and transfers of patients diagnosed with COVID on VPMI should be avoided17. If essential, preparations must be made before the transfer is carried out, and it is recommended that the condensate in the respiratory circuit be cleaned, as well as the patient's airway and oral cavity. The use of HMEF, must be maintained and sedation aims to promote comfort and prevent coughing17.
REFERENCES
39. Siqueira LTD. Impacto dos aspectos respiratórios e vocais na qualidade de vida do idoso. Dissertação (Mestrado) - Faculdade de Odontologia de Bauru, Universidade de São Paulo. Bauru: 2013. DOI: https://doi.org/10.11606/D.25.2013.tde-05062013-153747 [ Links ]
40. Fabron EMG, Sebastião LT, Oliveira GAG, Motonaga SM. Medidas da dinâmica respiratória em idosos participantes de grupos de terceira idade. Rev Cefac 2011;13(5):895-01. DOI: https://doi.org/10.1590/S1516-18462011005000034 [ Links ]
41. Scalan CL, Wilkins RK, Stoller J. Fundamentos da terapia respiratória de Egan. São Paulo: Manole, 2000. [ Links ]
42. Beardsell I, Bell S, Robinson S, Rumbold H, Hulbert D. MCEM Part A: MCQs. Londo: Royal Society of Medicine Press, 2009. [cited 2020 Apr 20] Available from: https://www.worldcat.org/title/mcem-part-a-mcqs/oclc/645632705 [ Links ]
43. Rajesh C, Todi S. ICU Protocols. A Step-wise Approach. Vol I. Second Edition. Springer, 2020. DOI: https://doi.org/10.1007/978-981-15-0898-1 [ Links ]
44. Lu Q, Rouby JJ. Measurement of pressure-volume curves in patients on mechanical ventilation: methods and significance. Crit Care. 2000;4(2):91-100. DOI: https://doi.org/10.1186/cc662 [ Links ]
45. Wong HYF, Lam HYS, Fong AH, Leung ST, Chin TWY, Lo CSY, et al. Frequency and Distribution of Chest Radiographic Findings in COVID-19 Positive Patients. Radiology. 2019;201160. DOI: https://doi.org/10.1148/radiol.2020201160 [ Links ]
46. Wu J, Wu X, Zeng W, Guo D, Fang Z, Chen L, et al. Chest CT findings in patients with corona virus disease 2019 and its relationship with clinical features. Invest Radiol. 2020;55(5):257-61. DOI: https://doi.org/10.1097/RLI.0000000000000670 [ Links ]
47. Silva C, Silva-Pinto A, Santos L, Tavares M, Sarmento A. From the emergency of a novel human virus to the global spread of a new disease. [cited 2020 Mar 03] Available from: https://ispup.up.pt/news/internal-news/from-the-emergency-of-a-novel-human-virus-to-the-global-spread-of-a-new-disease/906.html/ [ Links ]
48. World Health Organization (WHO). Clinical management of severe acute respiratory infection when Novel coronavirus (2019-nCoV) infection is suspected: Interim Guidance. [cited 2020 Jan 28] Available from: https://www.who.int/publications-detail/clinical-management-of-severe-acute-respiratory-infection-when-novel-coronavirus-(ncov)-infection-is-suspected [ Links ]
49. Rodriguez M, Thille AW, Boissier F, Veinstein A, Chatellier D, Robert R, et al. Predictors of successful separation from high-fow nasal oxygen therapy in patients with acute respiratory failure: a retrospective monocenter study. Intensive Care. 2019;9(1):101. DOI: https://doi.org/10.1186/s13613-019-0578-8 [ Links ]
50. Roca O, Caralt B, Messika J, Samper M, Sztrymf B, Hernández G, et al. An index combining respiratory rate and oxygenation to predict outcome of nasal high flow therapy. Am J Respir Care Med. 2019;119(11):1368-76. DOI: https://doi.org/10.1164/rccm.201803-0589OC [ Links ]
51. Neder JA, Andreoni S, Lerario MC, Nery LE. Reference values for lung function tests. II. Maximal respiratory pressures and voluntary ventilation. Braz J Med Biol Res. 1999;32(6):71. DOI: https://doi.org/10.1590/S0100-879X1999000600007 [ Links ]
52. Paula P. Correlação entre o pico do fluxo da tosse e os parâmetros clínicos e funcionais nas doenças neuromusculares. Dissertação (Mestrado) - Faculdade de Medicina da Universidade Federal de Minas Gerais. Belo Horizonte: 2010. [ Links ]
53. Matos L, Rabahi M. Manejo respiratório em doenças neuromusculares: revisão de literatura. Rev. Educ. Saúde. 2017;5(2):121-29. DOI: https://doi.org/10.29237/2358-9868.2017v5i2.p121-129 [ Links ]
54. American College of Sports Medicine. Diretrizes do ACSM para os testes de esforço e sua prescrição. 7 ed. Rio de Janeiro: Guanabara Koogan, 2007. [ Links ]
55. Pollack MM, Holubkov R, Funai T, Clark A, Moler F, Shanley T, et al. Relationship between the functional status scale and the pediatric overall performance category and pediatric cerebral performance category scales. JAMA Pediátrico. 2014;168(7):671-76. DOI: https://doi.org/10.1001/jamapediatrics.2013.5316 [ Links ]
56. Xia W, Shao J, Guo Y, Peng X, Li Z, Hu D. Clinical and CT features in pediatric patients with COVID-19 infection: different points from adults. Pediatric Pulmonol. 2020;55(5):1169-174. DOI: https://doi.org/10.1002/ppul.24718 [ Links ]
57. Zhu H, Wang L, Fang C, Pang S, Zhang L, Chang G, et al. Clinical analysis of 10 neonates born to mothers with 2019-nCoV pneumonia. Translat Pediatr. 2020; 9(1):51-60. DOI: https://doi.org/10.21037/tp.2020.02.06 [ Links ]
58. Wei M, Yuan J, Liu Y, Fuo T, Yu X, Zhang ZJ. Novel coronavirus infection in hospitalized infants under 1 year of age in China. JAMA. 2020. DOI: https://doi.org/10.1001/jama.2020.2131 [ Links ]
59. Zhu N, Zhang D, Wang W, Li X, Yang B, Song J, et al. A novel coronavirus from patients with pneumonia in China, 2019. N Engl J Med. 2020;382(8):727-33. DOI: https://doi.org/10.1056/NEJMoa2001017 [ Links ]
60. Lu Q, Shi Y. Coronavirus disease (COVID-19) and neonate: What neonatologist need to know. J Med Virol. 2020:92(6);564-67. DOI: https://doi.org/10.1002/jmv.25740 [ Links ]
61. Subspecialty Group of Respiratory Diseases, The Society of Pediatrics, Chinese Medical Association; Editorial Board, Chinese Journal of Pediatrics. Guidelines for management of community acquired pneumonia in children (the revised edition of 2013). Zhonghua Er Ke Za Zhi. 2013;51(10):745-52. [ Links ]
62. Harris M, Clark J, Coote N, Fletcher P, Harnden Um, McKean M, et al. British Thoracic Society guidelines for themanagement of community acquired pneumonia in children: update 2011. Thorax. 2011;6(suppl 2);ii1-23. DOI: https://doi.org/10.1136/thoraxjnl-2011-200598 [ Links ]
63. Bradley J, Byington CL, Shah SS, Alverson B, Carter ER, Harrison C, et al. The management of community-acquired pneumonia in infants and children older than 3 months of age: clinical practice guidelines by the Pediatric Infectious Diseases Society and the Infectious Diseases Society of America. Clin Infect Dis. 2011;53(7):e25-76. DOI: https://doi.org/10.1093/cid/cir531 [ Links ]
64. World Health Organization (WHO). WHO Statement Regarding Cluster of Pneumonia Cases in Wuhan, China. 2020. [cited 2020 Mar 31] Available from: https://www.who.int/health-topics/coronavirus [ Links ]
65. Inciardi RM, Lupi L, Zaccone G, Italia L, Raffo M, Tomasoni D, et al. Cardiac Involvement in a Patient With Coronavirus Disease 2019 (COVID-19). JAMA Cardiol, 2020. DOI: https://doi.org/10.1001/jamacardio.2020.1096 [ Links ]
66. Bispo Júnior JP. Fisioterapia e saúde coletiva: Desafios e novas responsabilidades profissionais. Cienc Saude Coletiva. 2010;15(Suppl. 1):1627-36. DOI: https://doi.org/10.1590/s1413-81232010000700074 [ Links ]
67. Herdy AH, López-Jiménez F, Terzic CP, Milani M, Stein R, Carvalho T, et al. Diretriz Sul-Americana de Prevenção e Reabilitação Cardiovascular. Soc Bras Cardiol. 2014;103(2 Supl. 1):1-31. [ Links ]
68. Rocha ARM, Martinez BP, Silva VZM, Forgiarini Junior LA. Early mobilization: Why, what for and how? Med Intensiva. 2017;41(7):429-36. DOI: https://doi.org/10.1016/j.medin.2016.10.003 [ Links ]
69. Bassan R, Pimenta L, Leães PE, Timerman A. I Diretriz de dor torácica na sala de emergência. Arq Bras Cardiol. 2002;79(Supl 2):1-22. DOI: https://doi.org/10.1590/S0066-782X2002001700001 [ Links ]
70. Stiller K. Safety issues that should be considered when mobilizing critically ill patients. Crit Care Clin. 2007;23(1):35-53. DOI: https://doi.org/10.1016/j.ccc.2006.11.005 [ Links ]
71. Stiller K, Phillips A. Safety aspects of mobilising acutely ill inpatients. Physiother Theory Pract. 2003;19(4):239-57. DOI: https://doi.org/10.1080/09593980390246751 [ Links ]
72. Diretrizes do ACMS para os testes de esforço e sua prescrição. 9 ed. Rio de Janeiro: 2016. [ Links ]
73. Zhonghua JHHHXZZ. Recommendations for respiratory rehabilitation of COVID-19 in adult. Chinese Association of Rehabilitation Medicine; Respiratory rehabilitation committee of Chinese Association of Rehabilitation Medicine; Cardiopulmonary rehabilitation Group of Chinese Society of Physicai Medicine and Rehabilitation. 2020;43(0):E029. DOI: https://doi.org/10.3760/cma.j.cn112147-20200228-00206 [ Links ]
74. Morsch ALBC, Amorim MM, Barbieri A, Santoro lL, Fernandes ALG. Influência da técnica de pressão expiratória positiva oscilante e da técnica de expiração forçada na contagem de células e quantidade do escarro induzido em portadores de asma ou doença pulmonar obstrutiva crônica. Bras Pneumol. 2008;34(12):1026-032. DOI: https://doi.org/10.1590/S1806-37132008001200007 [ Links ]
75. Tambascio J, Souza LT, Lisboa RM, Passarelli RC, Souza HC, Gastaldi AC. The influence of Flutter® VRP1 components on mucus transport of patients with bronchiectasis. Respir Med. 2011;105(9):1316-21. DOI: https://doi.org/10.1016/j.rmed.2011.04.017 [ Links ]
76. Latronico N, Bolton CF. Critical illness polyneuropathy and myopathy: a major cause of muscle weakness and paralysis. Lancet Neurol. 2011;10(10):931-41. DOI: https://doi.org//10.1016/S1474-4422(11)70178-8 [ Links ]
77. Needham DM, Wozniak AW, Hough CL, Morris PE, Dinglas VD, Jackson JC, et al. Risk factors for physical impairment after acute lung injury in a national, multicenter study. Am J Respir Crit Care Med. 2014;189(10):1214-24. DOI: https://doi.org/10.1164/rccm.201401-0158OC [ Links ]
78. Jonghe B, Sharshar T, Lefaucheur JP, Outin H. Critical illness neuromyopathy. Clin Pulm Med. 2005;12(2):90-6. DOI: https://doi.org/10.1097/01.cpm.0000156639.67261.19 [ Links ]
79. Hermans G, Clerckx B, Vanhullebusch T, Segers J, Vanpee G, Robbeets C, et al. Interobserver agreement of Medical Research Council sumscore and handgrip strength in the intensive care unit. Muscle Nerve. 2012;45(1):18-25. DOI: https://doi.org/10.1002/mus.22219 [ Links ]
80. Parry SM, Berney S, Granger CL, Dunlop DL, Murphy L, El-Ansary D, et al. A new two-tier strength assessment approach to the diagnosis of weakness in intensive care: an observational study. Crit Care. 2015;19:52. DOI: https://doi.org/10.1186/s13054-015-0780-5 [ Links ]
81. Vanpee G, Hermans G, Segers J, Gosselink R. Assessment of limb muscle strength in critically ill patients: a systematic review. Crit Care Med. 2014;42(3):701-11. DOI: https://doi.org/10.1097/CCM.0000000000000030 [ Links ]
82. Organização Mundial da Saúde (OMS) Classificação Internacional de Funcionalidade, Incapacidade e Saúde (CIF). São Paulo: Edusp; 2003. [ Links ]
83. Denehy L, Morton NA, Skinner EH, Edbrooke L, Haines K, Warrillow S, et al. A physical function test for use in the intensive care unit: validity, responsiveness, and predictive utility of the physical function ICU test (scored). Phys Ther. 2013;93(12):1636-45. DOI: https://doi.org/10.2522/ptj.20120310 [ Links ]
84. Franca EET, Ferrari F, Fernandes P, Cavalcanti R, Duarte A, Martinez BP, et al. Fisioterapia em pacientes críticos adultos: recomendações do Departamento de Fisioterapia da Associação de Medicina Intensiva Brasileira. Rev Bras Ter Intensiva. 2012;24(1):6-22. DOI: https://doi.org/10.1590/S0103-507X2012000100003 [ Links ]
85. Cai J, Xu J, Lin D, Yang Z, Xu L, Qu Z, et al. A Case Series of children with 2019 novel coronavirus infection: clinical and epidemiological features. Clin Infect Dis. 2020;pii:ciaa198. DOI: https://doi.org/10.1093/cid/ciaa198 [ Links ]
86. China CDC Weekly. The Epidemiological Characteristics of an Outbreak of 2019 Novel Coronavirus Diseases (COVID-19) in China. Zhonghua Liu Xing Bing Xue Za Zhi. 2020;41(2):145-51. DOI: https://doi.org/10.3760/cma.j.issn.0254-6450.2020.02.003 [ Links ]
87. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395(10223):497-06. DOI: https://doi.org/10.1016/S0140-6736(20)30183-5 [ Links ]
88. American Academy of Pediatrics. 2019 Novel Coronavirus (COVID-19). [cited 2020 Mar 31] Available from: https://www.healthychildren.org/English/health-issues/conditions/chest-lungs/Pages/2019-Novel-Coronavirus.aspx [ Links ]
89. Cameron S, Ball I, Cepinskas G, Choong K, Doherty TJ, Ellis CG, et al. Early mobilization in the critical care unit: A review of adult and pediatric literature. J Crit Care. 2015;30(4):664-72. DOI: https://doi.org/10.1016/j.jcrc.2015.03.032 [ Links ]
90. Stollings JL, Devlin JW, Lin JC, Pun BT, Byrum D, Barr J. Best Practices for Conducting Interprofessional Team Rounds to Facilitate Performance of the ICU Liberation (ABCDEF) Bundle. Crit Care Med. 2019;48(4):562-70. DOI: https://doi.org/10.1097/CCM.0000000000004197 [ Links ]
91. Oliveira MC, Ortiz Sobrinho C, Orsini M. Comparação entre o método Reequilíbrio Toracoabdominal e a fisioterapia respiratória convencional em recém-nascidos com taquipneia transitória: um ensaio clínico randomizado. Fisioter Bras. 2017;18(5):598-607. [ Links ]
92. Oliveira EAR, Gomes ELFD. Evidência científica das técnicas atuais e convencionais de fisioterapia respiratória em pediatria. Fisioter Bras. 2016;17(1):88-97. [ Links ]
93. Respiratory Care Committee of Chinese Thoracic Society. Expert consensus on preventing nosocomial transmission during respiratory care for critically ill patients infected by 2019 novel coronavirus pneumonia. Zhonghua Jie He He Hu Xi Za Zhi. 2020;17(0):E020. DOI: https://doi.org/10.3760/cma.j.issn.1001-0939.2020.0020 [ Links ]
94. Abdulsatar F, Walker RG, Timmons BW, Choong K. "Wii-Hab" in critically ill children: A pilot trial. J Pediatr Rehabil Med. 2013;6(4):193-204. DOI: https://doi.org/10.3233/PRM-130260 [ Links ]
95. Brasil. Ministério da Saúde. Secretaria de Atenção à Saúde. Departamento de Ações Programáticas Estratégicas. Atenção à Saúde do recém-nascido: guia para os profissionais de saúde. 2 ed. Volume 2. 2012; p.1-202. [ Links ]
96. Dong Y, Mo X, Hu Y, Qi X, Jiang F, Jiang Z, et al. Epidemiological Characteristics of 2143 Pediatric Patients With 2019 Coronavirus Disease in China. Pediatrics. 2020;16:pii:e20200702. DOI: https://doi.org/10.1542/peds.2020-0702 [ Links ]
97. Marraro GA, Spada C. Consideration of the respiratory support strategy of severe acute respiratory failure caused by SARS-CoV-2 infection in children. Chin J Contemp Pediatr. 2020;22(3):183-94. DOI: https://doi.org/10.7499/j.issn.1008-8830.2020.03.002 [ Links ]
98. Zhan Q, Sun B, Wang C. Early Use of Noninvasive Positive Pressure Ventilation for Acute Lung Injury: A Multicenter Randomized Controlled Trial. Crit Care Med. 2012;40(2):455-460. DOI: https://doi.org/10.1097/CCM.0b013e318232d75e [ Links ]
99. Pediatric Acute Lung Injury Consensus Conference Group. Pediatric Acute Respiratory Distress Syndrome: Consensus Recommendations from the Pediatric Acute Lung Injury Consensus Conference. Pediatr Crit Care Med. 2015;16(5):428-39. DOI: https://doi.org/10.1097/PCC.0000000000000350 [ Links ]
100. Curley MA, Thompson JE AJ. The effects of early and repeated prone positioning in pediatric patients with acute lung injury. Chest. 2000;118(1):156-63. DOI: https://doi.org/10.1378/chest.118.1.156 [ Links ]
101. Tran K, Cimon K, Severn M, Pessoa-Silva CL, Conly J. Aerosol generating procedures and risk of transmission of acute respiratory infections to healthcare workers: a systematic review. PLoS One. 2012;7:e35797. DOI: https://doi.org/10.1371/journal.pone.0035797 [ Links ]
102. Word Health Organization (WHO). Clinical management of severe acute respiratory infection (SARI) when COVID-19 disease is suspected. Interim guidance 13 March 2020. [cited 2020 Mar 31] Available from: https://www.who.int/docs/default-source/coronaviruse/clinical-management-of-novel-cov.pdf [ Links ]
103. Liao X, Wang B, Kan Y. Novel coronavirus infection during the 2019-2020 epidemic: preparing intensive care units - the experience in Sichuan Province, China. Intensive Care Med. 2020;46:357-60. DOI: https://doi.org/10.1007/s00134-020-05954-2 [ Links ]
104. Sorbini CA, Grassi V, Solinas E, Muiesan G. Arterial oxygen tension in relation to age in healthy subjects. Respiration. 1968;25(1):3-13. DOI: https://doi.org/10.1159/000192549 [ Links ]
105. Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, Fan E, et al. Acute respiratory distress syndrome: the Berlin Definition. JAMA. 2012; 307(23):2526-33. DOI: https://doi.org/10.1001/jama.2012.5669 [ Links ]
106. Fowler RA, Guest CB, Lapinsky SE, Sibbald WJ, Louie M, Tang P, et al. Transmission of Severe Acute Respiratory Syndrome during Intubation and Mechanical Ventilation. Am J Respir Crit Care Med. 2004;169(11):1198-202. DOI: https://doi.org/10.1164/rccm.200305715OC [ Links ]
107. Xiao Z, Li Y, Chen R, Li S, Zhong S, Zhong N. A retrospective study of 78 patients with severe acute respiratory syndrome. Chin Med J (Engl). 2003;116(6):805-10. [ Links ]
108. Hui DS, Chow BK, Lo T, Ng SS, Ko FW, Gin T, Chan MTV. Exhaled Air Dispersion During Noninvasive Ventilation via Helmets and a Total Facemask. Chest. 2015;147(5):1336-43. DOI: https://doi.org/10.1378/chest.14-1934 [ Links ]
109. Hraiech S, Alingrin J, Dizier S, Brunet J, Forel JM, La Scola B, et al. Time to intubation is associated with outcome in patients with community-acquired pneumonia. PLoS One. 2013;8(9):e74937. DOI: https://doi.org/10.1371/journal.pone.0074937 [ Links ]
110. Xu XP, Zhang XC, Hu SL, Xu JY, Xie JF, Liu SQ, et al. Noninvasive Ventilation in Acute Hypoxemic Nonhypercapnic Respiratory Failure: A Systematic Review and Meta-Analysis. Critical care medicine. 2017;45(7):e727-e733. DOI: https://doi.org/10.1097/CCM.0000000000002361 [ Links ]
111. Alraddadi BM, Qushmaq I, Al-Hameed FM, Mandourah Y, Almekhlafi GA, Jose J, et al. Noninvasive ventilation in critically ill patients with the Middle East respiratory syndrome. Influenza Other Respir Viruses. 2019;13(4):382-90. DOI: https://doi.org/10.1111/irv.12635 [ Links ]
112. Agarwal R, Aggarwal AN, Gupta D. Role of Noninvasive Ventilation in Acute Lung Injury/Acute Respiratory Distress Syndrome: A Proportion Meta-analysis. Resp Care. 2010;55(12):1653-60. [ Links ]
113. Meng L, Qiu H, Wan L, Ai Y, Xue Z, Guo Q, et al. Intubation and Ventilation amid the COVID-19 Outbreak: Wuhan's Experience. Anesthesiology. 2020. DOI: https://doi.org/10.1097/ALN.0000000000003296 [ Links ]
114. Arabi YM, Arifi AA, Balkhy HH, Najm H, Aldawood AS, Ghabashi A, et al. Clinical Course and Outcomes of Critically Ill Patients With Middle East Respiratory Syndrome Coronavirus Infection. Ann Intern Med. 2014;160(6):389-97. DOI: https://doi.org/10.7326/M13-2486 [ Links ]
115. Antonelli M, Conti G, Moro ML, Esquinas A, Gonzalez-Diaz G, Confalonieri M. et al. Predictors of failure of noninvasive positive pressure ventilation in patients with acute hypoxemic respiratory failure: A multi-center study. Intensive Care Med. 2001;27(11):1718-28. DOI: https://doi.org/10.1007/s00134-001-1114-4 [ Links ]
116. Atkinson J, Chartier Y, Pessoa-Silva CK, Jensen P, Li Y, Seto WH. Natural ventilation for infection control in health-care settings. Geneva: World Health Organization, 2009. [ Links ]
117. World Health Organization (WHO). Infection Prevention and Control during Health Care when Novel Coronavirus (nCoV) Infection is Suspected. [cited 2020 Mar 31] Available from: https://www.who.int/publications-detail/infection-prevention-and-control-during-health-care-when-novel-coronavirus-(ncov)-infection-is-suspected-20200125 [ Links ]
118. Hui DS. Influenza A/H5N1 infection: other treatment options and issues. Respirology. 2008;13(suppl 1):S22-6. DOI: https://doi.org/10.1111/j.1440-1843.2008.01250.x [ Links ]
119. Conti G, Larrsson A, Nava S, Navalesi P. On the role of non-invasive ventilation (NIV) to treat patients during the H1N1 influenza pandemic. [cited 2020 Mar 31] Available from: http://dev.ersnet.org/uploads/Document/63/WEBCHEMIN54101258624143.pdf [ Links ]
120. Hui DS, Hall SD, Chan MTV, Chow BK, Tsou JY, Joynt GM, et al. Noninvasive positive-pressure ventilation: An experimental model to assess air and particle dispersion. Chest. 2006;130(3):730-40. DOI: https://doi.org/10.1378/chest.130.3.730 [ Links ]
121. Ricard JD, Markowicz P, Djedaini K, Mier L, Coste F, Dreyfuss D. Bedside evaluation of efficient airway humidification during mechanical ventilation of the critically ill. Chest. 1999;115(6):1646-52. DOI: https://doi.org/10.1378/chest.115.6.1646 [ Links ]
122. Davis KJr, Evans SL, Campbell RS, Johannigman JA, Luchette FA, Porembka DT, et al. Prolonged use of heat and moisture exchangers does not affect device efficiency or frequency rate of nosocomial pneumonia. Crit Care Med. 2000;28(5):1412-28. DOI: https://doi.org/10.1097/00003246-200005000-00026 [ Links ]
123. Boisson C, Viviand X, Arnaud S, Thomachot L, Miliani Y, Martin C. Changing a hydrophobic heat and moisture exchanger after 48 hours rather than 24 hours: a clinical and microbiological evaluation. Intensive Care Med 1999;25(11):1237-43. DOI: https://doi.org/10.1007/s001340051051 [ Links ]
124. Patel BK, Wolfe KS, Pohlman AS, Hall JB, Kress JP. Effect of Noninvasive Ventilation Delivered by Helmet vs Face Mask on the Rate of Endotracheal Intubation in Patients With Acute Respiratory Distress Syndrome: A Randomized Clinical Trial. JAMA. 2016;315(22):2435-41. DOI: https://doi.org/10.1001/jama.2016.6338 [ Links ]
125. Chan JFW, Yuan S, Kok KH, KKW To, Chu H, Yang J, et al. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person to-person transmission: a study of a family cluster. Lancet. 2020;395(10223)::514-23. DOI: https://doi.org/10.1016/S0140-6736(20)30154-9 [ Links ]
126. Yang X, Yu Y, Xu J, Shu H, Xia J, Liu H, et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: A single-centered, retrospective, observational study. Lancet Respir Med. 2020. DOI: https://doi.org/10.1016/S2213-2600(20)30079-5 [ Links ]
127. Zuo M, Huang Y, Ma W, Xue Z, Zhang J, Gong Y, et al. Chinese Society of Anesthesiology Task Force on Airway Management: Expert recommendations for tracheal intubation in critically ill patients with noval coronavirus disease 2019. Chin Med Sci J. 2020. DOI: https://doi.org/10.24920/003724 [ Links ]
128. Wax R, Christian MD. Practical recommendations for critical care and anesthesiology teams caring for novel coronavirus (2019-nCoV) patients. Can J Anaesth. 2020. DOI: https://doi.org/10.1007/s12630-020-01591-x [ Links ]
129. Higgs A, McGrath B, Goddard C, Rangasami J, Suntharalingam G, Gale R, et al. Guidelines for the management of tracheal intubation in critically ill adults. Br J Anaesth. 2018;120(2):323-5252. DOI: https://doi.org/10.1016/j.bja.2017.10.021 [ Links ]
130. Cabrini L, Pallanch O, Pieri M, Zangrillo A. Preoxygenation for tracheal intubation in critically ill patients: one technique does not fit all. J Thorac Dis. 2019;(Suppl 9):S1299-S1303. DOI: https://doi.org/10.21037/jtd.2019.04.67 [ Links ]
131. Frerk C, Mitchell V, McNarry A, Mendonca C, Bhagrath R, Patel A, et al. Difficult Airway Society 2015 guidelines for management of unanticipated difficult intubation in adults. Br J Anaesth. 2015;115(6):827-48. DOI: https://doi.org/10.1093/bja/aev371 [ Links ]
132. Gottlieb M, Holladay D, Burns K, Nakitende D, Bailitz J. Ultrasound for airway management: an evidence-based review for the emergency clinician. Am J Emerg Med. 2019;S0735-6757:30816-2. DOI: https://doi.org/10.1016/j.ajem.2019.12.019 [ Links ]
133. Gattinoni L, Coppola S, Cressooni M, Busana M, Rossi S, Chiumello D. Covid-19 Does Not Lead to a "Typical" Acute Respiratory Distress Syndrome. Am J Respir Crit Care Med. 2020. DOI: https://doi.org/10.1164/rccm.202003-0817LE [ Links ]
134. Fan E, Brodie D, Slutsky A. Acute respiratory distress syndrome: advances in diagnosis and treatment. JAMA. 2018;319(7):698-710. DOI: https://doi.org/10.1001/jama.2017.21907 [ Links ]
135. Amato MBP, Meade MO, Slutsky AS, Brochard L, Costa ELV, Schoenfeld DA, et al. Driving pressure and survival in the acute respiratory distress syndrome. N Engl J Med. 2015;372:747-55. DOI: https://doi.org/10.1056/NEJMsa1410639 [ Links ]
136. Venkatesan T, Korula G. A comparative study between the effects of 4% endotracheal tube cuff lignocaine and 1.5mg/kg intravenous lignocaine on coughing and hemodynamics during extubation in neurosurgical patients: A randomized controlled double-blind trial. J Neurosurg Anesthesiol. 2006;18(4):230-4. DOI: https://doi.org/10.1097/00008506-200610000-00002 [ Links ]
137. Abrahamson SD, Canzian S, Brunet F. Using simulation for training and to change protocol during the outbreak of severe acute respiratory syndrome. Crit Care. 2005; 10:R3. DOI: https://doi.org/10.1186/cc3916 [ Links ]


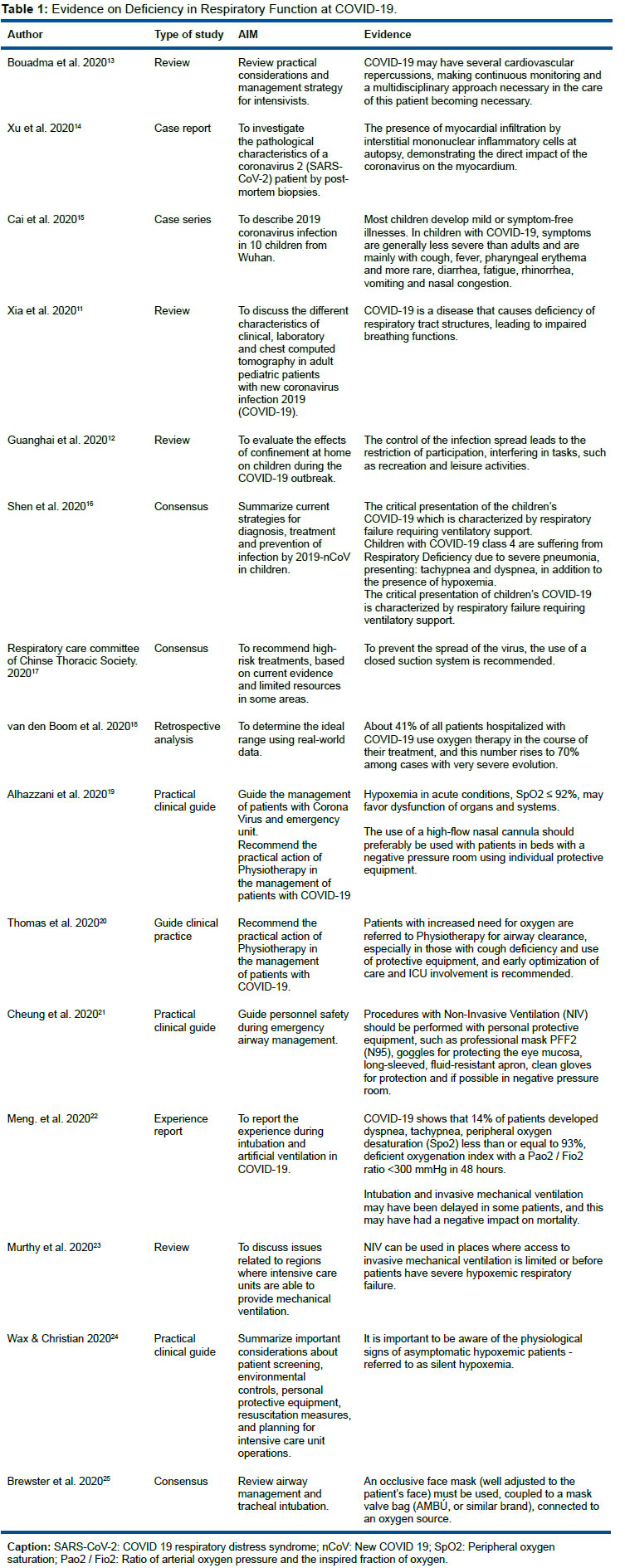{kind=link}
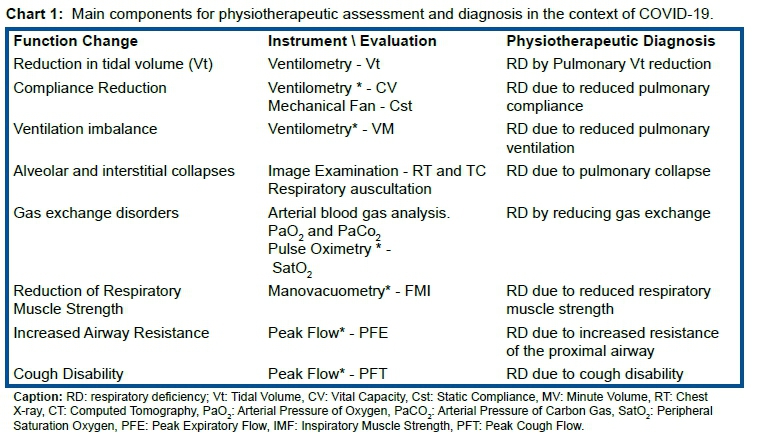{kind=link}
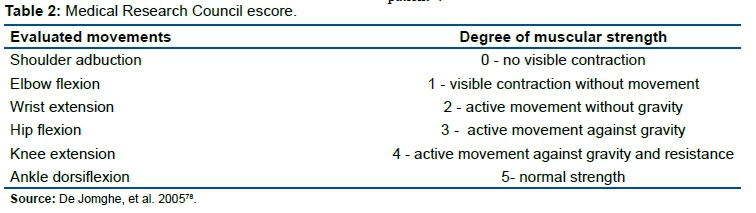{kind=link}
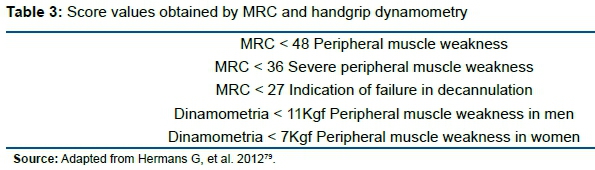{kind=link}
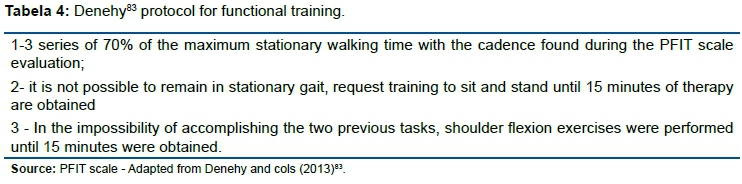{kind=link}
{kind=link}
{kind=link}
{kind=link}