










Serviços Personalizados
artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282versão On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.30 no.2 São Paulo maio/ago. 2020
http://dx.doi.org/10.7322/jhgd.v30.10363
ORIGINAL
Abortion withdrawal of sexual violence pregnancy: the role of the sex offender
Renata Macedo Martins PimentelI; Jefferson DrezettII; Hugo Macedo JrIII; Solange AndreoniIV; Rebeca Souza e SilvaV
Ihttps://orcid.org/0000-0002-9523-4859
IIhttp://orcid.org/0000-0002-9966-8072
IIIhttps://orcid.org/0000-0003-4072-3636
IVhttps://orcid.org/0000-0003-4589-9876
Vhttps://orcid.org/0000-0001-7492-1708
ABSTRACT
INTRODUCTION: Unwanted pregnancy is a serious consequence for women who experience sexual violence. Although deciding on abortion is frequent in these cases, there is not much information on women who give up abortion in this circumstance
OBJECTIVE: To analyse the associated factors in abortion withdrawal of sexual violence pregnancy
METHODS: A cross-sectional epidemiological study with a convenience sample of adolescents and women with pregnancy due to sexual violence and requesting legal abortion between August 1994 and December 2012, at Hospital Pérola Byington, São Paulo, Brazil. Pregnant women who gave up abortion after receiving the procedure approval were included and, in another group, pregnant women who completed the abortion. The variables were selected from a digitized database and analyzed using SPSS 15.0 software. The outcome was abortion withdrawal. The study variables were age; low education level; gestational age; color/black ethnicity; not being united; declare religion; serious threat from the aggressor; known offender; and residence of the aggressor. Odds ratios with 95% confidence intervals were calculated. The analysis used Wald's chi-square test (χ2W) and logistic regression with variable of interest defined as the known aggressor. The research was approved by the Research Ethics Committee of the Federal University of São Paulo, Opinion No. 6767
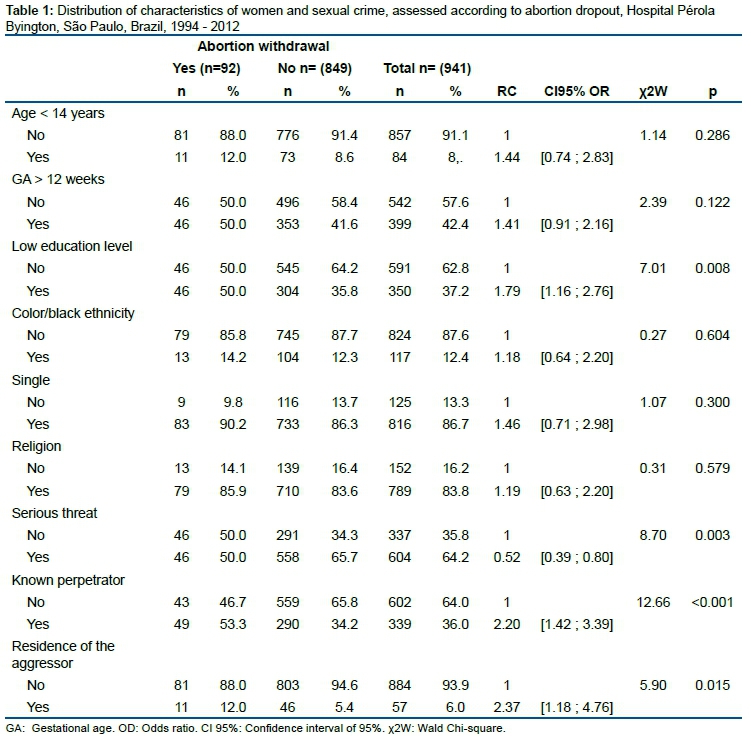
RESULTS: The study included 941 women, 849 (90.2%) who had an abortion and 92 (9.8%) who gave up after being approved. Age ranged from 10-46 years, mean 23.2 ± 7.9 years, gestational age 4-22 weeks, average 11.9 ± 4.5 weeks. Among those who gave up abortion, 12.0% were <14 years old; 50.0% had gestational age ≥ 13 weeks; 50.0% had low education; 14.2% were black; 90.2% single; 85.9% declared to have religion; 50.0% were threatened; 12.0% of the cases occurred at the perpetrator's residence and 53.3% of the victims were raped by known perpetrators. In logistic regression, the only significant variable was the known perpetrator, increasing the victim's chance of giving up abortion twice
CONCLUSION: The known sex offender has influenced the woman or adolescent's decision to give up legal abortion
Keywords: sex offenses, domestic violence, abused women, legal abortion, induced abortion.
Authors summary
Why was this study done?
Few research have documented the personal trajectories and decision-making processes of women who resort to legal abortion. Particular situation in cases of sexual violence is that of women who give up abortion, even after receiving care in the health service and having legally approved request. In this case, this study was developed in an attempt to know who these women are and what circumstances interfere or influence their decision.
What did the researchers do and find?
From primary data collected from patients enrolled in a referral hospital for the care of women and adolescents victims of sexual violence and legal termination of pregnancy, with the outcome variable analyzed as abortion, logistic regression was applied and the use of stepwise backward method observed that where only when the sex offender is typified as known explains the withdrawal of the procedure.
What do these findings mean?
The known sex offender was found to be associated with a two-fold greater chance of the woman giving up legal abortion. We assume that various elements can interact in this process from the proximity between the aggressor and the victim, such as threats, inhibition of women's initiative in the pursuit of their rights, or resistance to criminalize the known or relative. Demonstrating the need to improve public policies to protect women facing sexual violence by known perpetrators.
INTRODUCTION
Abortion has been typified as a crime in Brazil since 1940. In a few cases, abortion is well founded and legally supported, such as when pregnancy results from sexual violence; when there is a risk of death for the pregnant woman, as provided for in Article 128 of the law1; or in cases of anencephaly, according to a Supreme Court ruling in 20122.
Strongly restrictive abortion laws are often enforced in developing countries. However, in cases where abortion is legally permitted, the World Health Organisation recommends that these countries promote measures that increase women's access to safe and humane abortion health services3. Strengthening health services and public policies on abortion should be based on women's human rights and health needs and evidence, within a rigorous understanding of each country's social, cultural, political and economic context3.
Changes in this direction have been observed in Brazil in recent decades, although slowly and in the face of obstacles and resistance4. Public policies include the implementation in 1989 of health services organised to assist women who resort to legal abortion and the technical regulations of the Ministry of Health to guide managers and health professionals, published in 19991,4,5.
Although the country has a noticeably insufficient and centralised number of health services that perform legal abortion, some successful experiences have enabled the accretion of consistent knowledge about women who resort to legal abortion in cases of sexual violence6,7. Authors such as Pedroso (2010)8 and Blake et al. (2014)9 established the main characteristics and vulnerabilities of these women, who are predominantly single Catholic young people without much education. The unknown perpetrator is mentioned as the most frequent, threatening them with death to commit sexual crimes. Most women report sexual crimes to the police and undergo medical examination to identify and hold the perpetrator responsible8,9.
Debates and legislative changes on abortion should not be restricted to the criminal aspect but incorporate elements of education, culture and public health. This allows a better understanding of the reasons why women resort to abortion6. In situations of pregnancy resulting from sexual violence, the legitimate justification of women to seek abortion is recognised10. In this sense, few studies have documented the personal trajectories and decision-making processes of women who resort to legal abortion7.
Drezett et al. (2012)11, in a qualitative study with 43 Brazilian women, found different points of convergence for the choice of abortion. Women mainly pointed out their rejection of forced pregnancy, considered the situation as a serious violation of their right to choose maternity, and expressed intense fear of possible social and emotional consequences if they continued their pregnancy until termination11.
Despite this perceived violation of their human rights, some Brazilian women still cannot obtain a legal abortion due to technical impediments, even when accessing the few specialised services available8,9,12,13. Among these impediments, it is worth considering the role played by the sexual aggressor. When the aggressor is known to the victim, Blake et al. (2015)9 found that the search for abortion is delayed, often with advanced gestational age (≥ 23) weeks, impeding the procedure9. In cases of incest, Bessa et al. (2019)13 found that the related family abusers was less frequently related to legal abortion. A similar finding was reported by Pedroso (2010)8, who found a lower chance of abortion when the perpetrator was declared as known by young women8.
Intimate partner sexual violence should also be considered. In these cases, the data are less accurate and difficult to delimit, either by the diversity of classifications that define this aggression, by the naturalisation of violence as a "right" of the partner and "duty" of women in many cultures, or by the embarrassment of women to reveal this experience. In Brazil, intimate partner sexual violence affects between 10.1% and 14.3% of women; it is often severe and repeated, associated with other forms of violence14.
A particular situation in cases of sexual violence is that of women who give up abortion, even after receiving care in the health service and having a request legally approved. In these cases, not much is known about who these women are and what circumstances influence or interfere with their decision. Thus, the objective is to analyse the associated factors in abortion withdrawal of sexual violence pregnancy.
METHODS
Study design
This is a cross-sectional study with a convenience sample from primary data collected from patients enrolled at Hospital Pérola Byington, São Paulo, Brazil, between August 1994 and December 2012, with pregnancy resulting from sexual violence and requesting legal abortion. The Hospital Pérola Byington is the most important Brazilian reference institution for the care of women and adolescent victims of sexual violence and legal pregnancy termination.
Criteria for selection and inclusion of subjects
The study population consisted of adult pregnant women and pregnant adolescents of sexual violence, allocated in two groups. The first group included patients who gave up on abortion after receiving approval for the procedure. The second group included patients who had an abortion.
To characterise the sexual crime was considered the complaint of the patient or her legal representative in accordance with articles 213 and 217-A of the Brazilian criminal law, Law No. 12.015. Article 213 considers sexual violence to be unauthorised sexual contact imposed through violence or serious threat. Article 217-A typifies the sexual violence of vulnerable persons, including sexual acts against persons under 14 or against persons who cannot offer resistance or valid consent1. The request for termination of pregnancy is legally supported by Article 128 of the Brazilian criminal law, Law No. 2,8481.
Cases that were not approved for abortion were excluded, such as gestational age ≥ 23 weeks, pregnancy unrelated to sexual crime (prior or subsequent to sexual violence), false allegation of sexual crime and loss of follow-up.
Instruments and analysis of data
The variables selected for the study were extracted from a Microsoft Excel 2010 database and transferred to SPSS 15.0 software for analysis. The primary database was fed through a pre-coded form with consensus records of the team of physicians, social workers and psychologists of the Hospital Pérola Byington. The fill considered the narratives of the patient or her legal representative. The pre-coded sheets were reviewed at the end of each call and before typing. Each case included in the database was subjected to the consistency of information by a different reviewer than the one responsible for the typing, and divergences were corrected and consolidated before transfer to SPSS 15.0 software.
Statistical analysis
The outcome variable analysed was abortion dropout (1 = yes; 0 = no). The study variables considered were the pregnant woman's age (< 14 years = 1), gestational age (< 13 weeks = 1); low education (< 9 years of schooling); colour / black ethnicity = 1; not being united = 1; declared religion = 1; use of severe threat by the aggressor = 1; known offender = 1; residence of offender (indicated place of approach of victim = 1).
Odds ratios and respective 95% confidence intervals were calculated. Wald's chi-square tests (χ2W) and their statistical significance (p) were calculated. The adopted significance level was 5%. Logistic regression adjusted by analysis of the study variables with the variable of interest defined as the known aggressor = 1 was used. The analysis using likelihood ratio tests employed the stepwise backward method.
Ethical aspects
All cases included in the study received interdisciplinary care according to technical regulations of the Brazilian Ministry of Health5. The abortion evaluation and performance procedures fully complied with ethical-legal norms and current Brazilian legislation1.
Resolutions No. 196/1996 and No. 466/12 of the National Health Council (CNS) were respected concerning the ethical aspects inherent in conducting research involving human beings. The study did not incorporate any form of patient identification, ensuring confidentiality. The research was approved by the Research Ethics Committee of the Federal University of São Paulo, Opinion No. 6767 and CAAE No. 00957512.3.0000.5505, of March 9, 2012.
RESULTS
During the study period, 1,236 women and adolescents with pregnancy due to sexual violence and requesting legal abortion were identified in the primary database. We excluded 227 cases (18.4%) in which abortion was not approved by the institution and 68 cases (5.5%) due to loss of follow-up. The final sample for analysis consisted of 941 women, 849 (90.2%) of whom had had an abortion and 92 (9.8%) of whom withdrew from the procedure after approval.
Age ranged from 10 to 46 years, mean 23.2 ± 7.9 years, with gestational age ranging from 4 to 22 weeks, average 11.9 ± 4.5 weeks. Table 1 shows the distribution of the characteristics of women and adolescents and sexual crime, evaluated according to abortion withdrawal (Table 1).
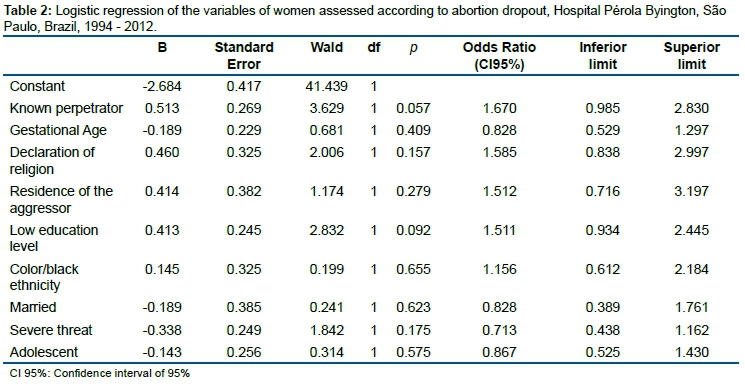
In the regression analysis, the relationship between the dependent variable and other independent variables is sought. The analysis using likelihood ratio tests used the stepwise backward method according to the following order: colour/black ethnicity (p = 0.655); united (p = 0.617); adolescent (p = 0.656); gestational age (0.402); residence of the author (p = 0.246); declared religion (0.194); threat (p = 0.157); and low education (p = 0.077) (Table 2).
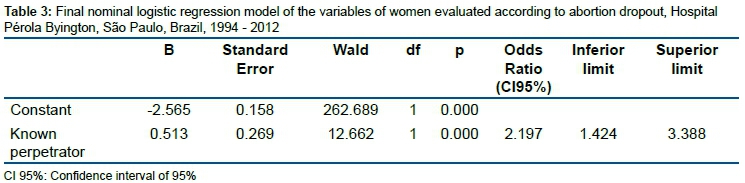
The final logistic regression model, where only when the sex offender is typified as known, explains the withdrawal of the procedure. In this case, the chance of the victim giving up on authorised abortion is about double the chance of giving up abortion if the sex offender is typified as unknown (Table 3).
DISCUSSION
Gender inequalities are the main foundation of violence against women. "Gender" refers to the set of relationships, attributes, roles, beliefs and attitudes that define the social and cultural meaning of men and women. Gender is one of the most important markers of gender inequality as it strongly permeates power relations15.
Sexual violence is an expression of gender violence and is considered a serious violation of women's human rights. It is a phenomenon of high prevalence and with major impact on women's health11. The World Health Organisation (WHO) considers sexual violence to be sexual acts attempted or completed without consent, imposed by the perpetrator through coercion or intimidation, the use of force or physical violence, threat, or psychological fear16.
Forced and unwanted pregnancies are one of the most complex and important consequences of sexual violence11. The outcome of these pregnancies is still poorly understood, and access to and safety of abortion largely depend on the laws in force in each country17. According to Holmes et al. (1996)18, half of women with pregnancy due to sexual violence resorted to legally induced abortion, while 32% accepted pregnancy18.
As with children and adolescents, young women of reproductive age are referred to as the age group with high prevalence of sexual violence. They are subject to forced and unwanted pregnancies when they do not use a contraceptive method that is independent of the perpetrator or when they are unaware or not of quick access to emergency contraception18-22. In this study, the final logistic regression model disproved the hypothesis that very young women under 14 would give up legal abortion because of their lower decision-making autonomy and possible family interference.
A significant number of Brazilian women resort to legal abortion after the twelfth week of pregnancy, possibly due to the emotional damage that limits women's initiatives or the difficulty of access to health services9,11,12. We reasonably believe that reaching the second trimester of pregnancy while facing strong social and family pressure against abortion could end as a factor in giving up pregnancy. However, this hypothesis was also refuted in this study.
Low education, defined as less than nine years of formal schooling, is a condition often found among women who experience sex crimes in large urban centers9,12,16,23,24. According to Souto et al. (2012)25, low education is even more frequent among intellectually disabled people who suffer sexual crimes25. In this study, poor education was found for half of women who dropped out of legal abortion and was significant in univariate analysis (p = 0.008). However, the hypothesis that women with low education gave up on abortion more often was not confirmed. In the final regression model, low education was not relevant, although it approached significance (p = 0.077 - OR: 1.501 [0.957 - 2.353]). We intend, in future more complex statistical analyses, to better assess the role of low education in giving up legal abortion.
According to data from the Brazilian Institute of Geography and Statistics (IBGE)26, the declaration of colour/ethnicity by the Brazilian population has been changing in recent decades. In the last census of 2010, 47.7% of people declared themselves white, while in previous surveys this information was 53.7% in 2010 and 62.2% in 1991, with similar figures for men and women26.
Research has pointed to the predominance of white colour/ethnicity among Brazilian women in situations of sexual violence, in similar percentages to the IBGE censuses9,12,27. However, the colour/black ethnicity statement in this study corresponded to 12.4% of the cases analysed, contrasting markedly with data from the Brazilian population. We believe this finding may be related to greater obstacles and difficulties for black women in accessing legal abortion.
Indeed, there is evidence that black Brazilian women are more vulnerable to violence and to develop preventable sexual and reproductive health problems. They also have unfavourable social indicators such as lower education, higher poverty, lower access to health services and higher unemployment4,26. However, in this study we did not find colour/ethnicity as a factor associated with giving up abortion.
Women living in large urban centres commonly declare themselves single at the time of sexual offence9,12,16,24,28. It is reasonable to suppose that this is due to the young age of these women. In this study, a similar situation was observed, with 86.7% of the women analysed declaring themselves single. However, this variable was not relevant in giving up legal abortion.
Clearly, the marital situation we encounter contrasts with the high prevalence of intimate partner violence among Brazilian women14. Ellsberg et al. (2008)15 warn that cultural issues can transform everyday violent events into something relatively acceptable or tolerable by women, hindering both their recognition and possible interventions15. For authors such as Drezett et al. (2012)11 and Souza and Adesse (2005)4 women in situations of sexual and domestic violence may feel that referral health services do not apply to them because the aggressor is their intimate partner4,11. Similarly, we question whether the intimate partner, as an aggressor, cannot exert an obstacle to denouncing and seeking women for their rights.
There is not much information about the role of religion in the outcome of pregnancy due to sexual violence, especially in Brazil. Pedroso's research (2010)8 shows that 78.3% of Brazilian women who have had abortions in cases of sexual crime declare themselves Catholic or evangelical, religions with inflexible and axiomatic positions against abortion, even in circumstances where abortion is permitted by law. For the author, the simple declaration of religion was not shown to impede the choice to have an abortion among the women studied8.
Contrary to our initial hypothesis, the declaration of religion as a factor in giving up legal abortion was not confirmed in this study. Of the women studied, 83.8% reported following a religion, similar to that observed by Pedroso (2010)8. However, the relationship between religion and abortion is complex and should be carefully analysed. Not much is known about the role of religion among women who resolutely do not allow abortion, even in cases of sexual violence, as they do not seek legal abortion.
The embarrassment of women by serious threat or psychological intimidation is considered the most frequent method used by the aggressor to consummate the sexual crime9,11-13. By not employing physical violence, the aggressor avoids producing any material evidence, helping to keep sexual violence hidden and reducing the chances of being identified29,30. Physical injuries are often more common among victims who offer resistance to the aggressor31. On the other hand, firearm threats can inhibit women's resistance, significantly reducing the occurrence of physical harm32.
Among Brazilian women who have experienced intimate partner sexual violence throughout their lives, Schraiber et al. (2007)14 reported that physical force was involved in between 71.8% and 82% of cases. Another 70% of women reported fear of refusal to have sex with their partner14. A similar situation was found in rural communities in Nepal, with 42% of married women admitting that their partner used violence to have sex33. A survey of young men from 70 communities in South Africa shows that 16% committed sexual acts against women and 8% admitted using violence during sexual intercourse28.
Our results found a higher frequency of serious threat both for women who underwent legal abortion (65.7%) and those who gave up the procedure. Although univariate analysis indicated significance (p = 0.003), in the final logistic regression model, the type of embarrassment was not associated with legal abortion withdrawal.
Intimate partner sexual violence stems from hierarchical gender norms that, by their very nature, usually occur in the domestic space. The same is true of sexual violence against children and adolescents, with most cases occurring at home by known and often related19,20,22,23,34. Private spaces are also the most frequent places to approach when victims have intellectual disabilities13. Even during pregnancy, a significant part of women experience different forms of gender-based violence in the home environment, especially those with lower education and low income35.
Ensslen et al. (2018)36 state that perpetrators who prefer to practice sexual violence at the victim's residence are a specific type of perpetrator, even when unknown to the woman36. In this study, we did not find the aggressor's residence as a factor for giving up legal abortion in the final regression model. For Wegnar (2015)37, many aggressors seek different arguments to justify sexual violence, which acts as a predictive factor for other violence37. In cases of intimate partner violence, gender inequalities are associated with justification by aggressors and greater blaming of victims38.
The role of the known or related sex offender is largely described by the dynamics of sexual violence. Zambon et al. (2012)20 found that the related aggressor increases the chance of violence becoming recurrent fourfold20. In cases of incestuous sexual abuse, Yildirim et al. (2014)39 found that sexual violence lasted for more than one year in one-third of cases39. Bessa et al. (2019)13 observed that in cases of pregnancy due to incest, the aggressor exerted an influence on the care path of adolescents, making access to health services difficult13. Among children, Vertamatti et al. (2018)34 found that a related or known perpetrator postponed disclosure and reporting of sexual abuse to the appropriate authorities34.
Martin et al. (2006)40 suggest that known sex offenders intimidate the victim and her family, creating barriers for the crime to be reported to the authorities40. In the same vein, Blake et al. (2015)9 found that when the sex offender was known and close to the victim, medical care was delayed, even when violence resulted in pregnancy9.
In line with this evidence, the final logistic regression model adopted in this study found that the involvement of known sex offenders made victims twice as likely to give up on legal abortion. However, the results of this study do not clarify the mechanisms by which this happens. We assume that various elements can interact in this process due to the proximity between the aggressor and the victim, such as threats, inhibition of women's initiative in the pursuit of their rights, or resistance to criminalise a partner, acquaintance or relative.
Brazilian public policies have advanced in the protection of women facing violence. Law No. 11,340 of 2006, known as the Lei Maria da Penha, establishes protective mechanisms and measures to curb domestic violence against women. In 2015, Law No. 13,104 made femicide aggravated by the crime of homicide. In the health field, Law No. 5,099 made it mandatory for health professionals to report sexual violence1.
Oshikata et al. (2011)24 have observed a significant increase in police participation in referring women who suffer sexual violence to referral health services. The authors believe that this increase is partly due to these legal measures24. A similar situation was found by Mutta and Yela (2017)12, who reported the perpetrator more frequently to the police and performed expert medical examinations among women who resorted to abortion due to pregnancy due to sexual violence12.
We consider that the documentary aspect, the relevant theme for public health and the number of subjects included represent strengths of this study. The findings may contribute to improving public policies for women in these circumstances, particularly those experiencing sexual violence by known perpetrators.
We seek to recognise the limitation of each study variable and present it to the reader, as recommended for observational studies by Strengthening the Reporting of Observational Studies in Epidemiology41. We call attention to the methodological limits of an investigation based on a convenience sample. Care is required when generalising the results of this study to other social and cultural contexts. Another potential limit is the inaccuracy of information on intimate partners as aggressors, admitting that it is difficult for women to disclose this information due to stigma, shame or guilt. The restriction of external validity of variables such as colour/ethnicity and religion should be considered due to the sociodemographic heterogeneity of other samples. We could not adequately interpret complex associations such as the role of religion and schooling as reasons for giving up abortion.
Thus, it is concluded that a known offender is associated with the withdrawal from legal abortion among women with pregnancy due to sexual violence. The mechanisms by which they exert this influence are unclear.
REFERENCES
1.Brasil. Ministério da Saúde. Secretaria de Atenção à Saúde. Departamento de Ações Pragmáticas Estratégicas. Juridical aspects of the attention to victims of sexual violence: questions and answers for health professionals. 2th ed. Brasília: Editora do Ministério da Saúde; 2011. 48p. [ Links ]
2.Brasil. Ministério da Saúde. Secretaria de Atenção à Saúde. Departamento de Ações Programáticas Estratégicas. Atenção às mulheres com gestação de anencéfalos: norma técnica. Brasília: Ministério da Saúde; 2014. 52p. [ Links ]
3.World Health Organization. Department of Reproductive Health and Research. Safe abortion: technical and policy guidance for health systems. 2nd ed. Uruguay: World Health Organization; 2012. 134p. [ Links ]
4.Souza CM, Adesse L. Violência sexual no Brasil: perspectivas e desafios. Brasília: Secretaria Especial de Políticas para Mulheres; 2005. 188p. [ Links ]
5.Brasil. Ministério da Saúde. Secretaria de Atenção à Saúde. Departamento de Ações Programáticas Estratégicas. Prevention and treatment of damages resulting from sexual violence against women and adolescents: technical standard. 3th ed. Brasília: Ministério da Saúde; 2012. 124p. [ Links ]
6.Madeiro AP, Rufino AC. Maus-tratos e discriminação na assistência ao aborto provocado: a percepção das mulheres em Teresina, Piauí, Brasil. Cienc Saude Coletiva. 2017,22(8):2771-80. http://dx.doi.org/10.1590/1413-81232017228.04252016. [ Links ]
7.Menezes G, Aquino EML. Pesquisa sobre o abortamento no Brasil: avanços e desafios para o campo da saúde coletiva. Cad Saude Publica. 2009:25(sup 2):S193-S204. http://dx.doi.org/10.1590/S0102-311X2009001400002. [ Links ]
8.Pedroso D. Estudo de fatores relacionados ao abortamento previsto em lei em situação de violência sexual. [dissertação]. São Paulo: Universidade de Santo Amaro; 2010. [ Links ]
9.Blake MT, Drezett J, Machi GS, Pereira VX, Raimundo RD, Oliveira FR, et al.,,. Factors associated with the delay in seeking legal abortion for pregnancy resulting from rape. Int Arch Med. 2015;8(29). doi: 10.3823/1628. [ Links ]
10.Costa RG, Hardy E, Osis MJ, Faundes A. Decisão de abortar: processo e sentimentos envolvidos. Cad Saude Publica. 1995;11(1):97-105. http://dx.doi.org/10.1590/S0102-311X1995000100016. [ Links ]
11.Drezett J, Pedroso D, Vertamatti MA, Macedo-Junior H, Blake MT, Gebrim LH, et al.,,. Pregnancy resulting from sexual abuse: reasons alleged by Brazilian women for carrying out the abortion - pregnancy and violence. Health MED. 2012;6(3):819-25. [ Links ]
12.Mutta DS, Yela DA. Sociodemographic characteristics of women in a public hospital in Campinas who underwent legal abortion due to sexual violence: cross-sectional study. Sao Paulo Med J. 2017;135(4):363-8. [ Links ]
13.Bessa MM, Drezett J, Adami F, Araújo SDT, Bezerra IMP, Abreu LC. Characterization of adolescent pregnancy and legal abortion in situations involving incest or sexual violence by an unknown aggressor. Medicina. 2019;55(474):1-11. doi: 10.3390/medicina55080474. [ Links ]
14.Schraiber LB, D'Oliveira AFPL, França-Junior I, Diniz S, Portella AP, Ludermir AB, et al.,,. Prevalence of intimate partner violence against women in regions of Brazil. Rev Saude Publica. 2007;41(5):1-10. http://dx.doi.org/10.1590/S0034-89102007000500014. [ Links ]
15.Ellsberg M, Jansen HA, Heise L, Watts CH, Garcia-Moreno C. Intimate partner violence and women's physical and mental health in the WHO multi-country study on women's health and domestic violence: an observational study. Lancet. 2008;371(9619):1165-72. doi: 10.1016/S0140-6736(08)60522-X. [ Links ]
16.Krug EG, Dahlberg LL, Mercy JA, Zwi AB, Lozano R. World report on violence and health. Geneva: World Health Organization; 2002. 346p. [ Links ]
17.Lathrope A. Pregnancy resulting from rape. J Obstet Gynecol Neonatal Nurs.1998;27(1):25-31, 1998. doi: https://doi.org/10.1111/j.1552-6909.1998.tb02587.x. [ Links ]
18.Holmes MM, Resnick HS, Kilpatrick DG, Best CL. Rape-related pregnancy: estimates and descriptive characteristics from a national sample of women. Am J Obstet Gynecol. 1996;175(2):320-4. doi: https://doi.org/10.1016/S0002-9378(96)70141-2. [ Links ]
19.Blake MT, Drezett J, Vertamatti MA, Adami F, Valenti VE, Paiva AC, et al., Characteristics of sexual violence against adolescent girls and adult women. BMC Womens Health. 2014; 22(14):15. doi: 10.1186/1472-6874-14-15. [ Links ]
20.Zambon MP, Jacintho ACA, Medeiros MM, Guglielminetti R, Marmo DB. Domestic violence against children and adolescents: a challenge. Rev Assoc Med Bras. 2012;58(4):465-71. doi.org/10.1590/S0104-42302012000400018. [ Links ]
21.Madeiro A, Diniz D. Legal abortion services in Brazil - a national study. Ciêncsaúde coletiva. 2016;21(2):563-72. doi: 10.1590/1413-81232015212.10352015. [ Links ]
22.Sodipo OO, Adedokun A, Adejumo AO, Olibamoyo O. The pattern and characteristics of sexual assault perpetrators and survivors managed at a sexual assault referral centre in Lagos. Afr J Prim Health Care Fam Med. 2018;10(1):e1-e5. doi: 10.4102/phcfm.v10i1.1727. [ Links ]
23.Jewkes R. Intimate partner violence: causes and prevention. Lancet. 2002;359(9315):1423-9. doi: 10.1016/S0140-6736(02)08357-5. [ Links ]
24.Oshikata CT, Bedone AJ, Papa MSF, Santos GB, Pinheiro CD, Kalies AH. Características das mulehres violentadas sexualmente e da adesão ao seguimento ambulatorial: tendências observadas ao longo dos anos em serviço de referência em campinas, São Paulo, Brasil. Cad Saude Publica. 2011;27(4):701-13. doi: http://dx.doi.org/10.1590/S0102-311X2011000400009. [ Links ]
25.Souto RQ, Leite CCS, França ISX, Cavalcanti AL. Violência sexual contra mulheres portadoras de necessidades especiais: perfil da vítima e do agressor. Cogitare Enferm. 2012;17(1):72-7. doi: http://dx.doi.org/10.5380/ce.v17i1.26377. [ Links ]
26.Instituto Brasileiro de Geografia e Estatística (IBGE). Ministério do Planejamento, Desenvolvimento e Gestão. Síntese de indicadores sociais: uma análise das condições de vida da população brasileira 2016. Rio de Janeiro: Instituto Brasileiro de Geografia e Estatística; 2016. 141p. [ Links ]
27.Machado CL, Fernandes MAS, Osis MJD, Makuch MY. Gravidez após violência sexual: vivências de mulheres em busca da interrupção legal. Cad Saúde Pública. 2015;31(2):345-53. doi: http://dx.doi.org/10.1590/0102-311X00051714. [ Links ]
28.Jewkes R, Dunkle K, Koss MP, Levin JB, Nduna M, Jama N, et al., Rape perpetration by young, rural South African men: prevalence, patterns and riskfactors. Soc Sci Med. 2006;63(11):2949-61. [ Links ]
29.Vadysinghe AN, Dassanayaka PB, Sivasubramanium M, Senasinghe DPP, Samaranayake AN, Wickramasinghe WMMHP. A study on sexual violence inflicted on individuals with intellectual developmental disorder. Disabil Health J. 2017;10(3):451-4. doi: 10.1016/j.dhjo.2016.12.010. [ Links ]
30.Ramos CRA, Medicci VPG, Puccia MIR. Sexually abused women - social and demographic profile and health care procedure analysis at a referral center. Rev Inst Ciênc Saúde. 2009;27(1):22-7. [ Links ]
31.Atkeson BM, Calhoun KS, Morris KT. Victim resistance to rape: the relationship of previous victimization, demographics, and situational factors. Arch Sex Behav. 1989;18(6):497-507. [ Links ]
32.Reis JN, Martin CCS, Ferriani MGC. Female victims of sexual abuse: coercive methods and non-genital injuries. Cad Saude Publica. 2004;20(2):465-73. http://dx.doi.org/10.1590/S0102-311X2004000200014. [ Links ]
33.Lamichhane P, Puri M, Tamang J, Dulal B. Women's status and violence against young married women in rural Nepal. BMC Womens Health. 2011;11:19. doi: 10.1186/1472-6874-11-19. [ Links ]
34.Vertamatti MAF, Strufaldi R, Evans DP, Drezett J, Barbosa CP, Abreu LC. Factors associated with reporting delays and severity of childhood sexual abuse in São Paulo, Brazil. Psychology Health Med. 2018;1-10. doi: 10.1080/13548506.2018.1556397. [ Links ]
35.Chasweka R, Chimwaza A, Maluwa A. Isn't pregnancy supposed to be a joyful time? A cross-sectional study on the types of domestic violence women experience during pregnancy in Malawi. Malawi Med J. 2018;30(3):191-6. doi: 10.4314/mmj.v30i3.11. [ Links ]
36.Ensslen K, Beauregard E, Pedneault A. An Examination of the home-intruder sex offender. Int J Offender Ther Comp Criminol. 2018;62(14):4694-713. doi: 10.1177/0306624X18778450. [ Links ]
37.Wegner R, Abbey A, Pierce J, Pegram SE, Woerner J. Sexual assault perpetrators' justifications for their actions: relationships to rape supportive attitudes, incident characteristics, and future perpetration. Violence Against Women. 2015;21(8):1018-37. doi: 10.1177/1077801215589380. [ Links ]
38.Erickson KA, Jonnson M, Langille JI, Walsh Z. Victim gender, rater attitudes, and rater violence history influence perceptions of intimate partner violence. Violence Vict. 2017;1;32(3):533-44. doi: 10.1891/0886-6708.VV-D-15-00086. [ Links ]
39.Yildirim A, Ozer E, Bozkurt H, Ozsoy S, Enginyurt O, Evcuman D, et al., Evaluation of social and demographic characteristics of incest cases in a university hospital in Turkey. Med Sci Monit. 2014;20:693-7. doi: 10.12659/MSM.890361. [ Links ]
40.Martin SL, Ray N, Sotres-Alvarez D, Kupper LL, Moracco KE, Dickens PA, et al., Physical and sexual assault of women with disabilities. Violence Against Women. 2006;12(9):823-37. doi: https://doi.org/10.1177/1077801206292672. [ Links ]
41.The PLOS Medicine Editors. Observational studies: Getting clear about transparency. PLoS Med. 2014;11(8):e1001711. https://doi.org/10.1371/journal.pmed.1001711. [ Links ]
 Correspondence:
Correspondence:
re_pimentel1@hotmail.com
Manuscript received: July 2019
Manuscript accepted: November 2019
Version of record online: May 2020


{kind=link}
{kind=link}
{kind=link}